
Abstract
Healthcare facilities are among the most expensive buildings to construct, maintain, and operate. How building design can best support healthcare services, staff, and patients is important to consider. In this narrative review, we outline why the healthcare environment matters and describe areas of research focus and current built environment evidence that supports healthcare in general and stroke care in particular. Ward configuration, corridor design, and staff station placements can all impact care provision, staff and patient behavior. Contrary to many new ward design approaches, single-bed rooms are neither uniformly favored, nor strongly evidence-based, for people with stroke. Green spaces are important both for staff (helping to reduce stress and errors), patients and relatives, although access to, and awareness of, these and other communal spaces is often poor. Built environment research specific to stroke is limited but increasing, and we highlight emerging collaborative multistakeholder partnerships (Living Labs) contributing to this evidence base. We believe that involving engaged and informed clinicians in design and research will help shape better hospitals of the future.
Introduction
Imagine (re-)designing the very hospital you work in. What would you design differently? What would you change, to benefit you, your patients, and their families? What evidence might help guide those design decisions?
Healthcare facilities are among the most expensive buildings to construct, maintain, and operate. 1 Once built, hospitals remain in service for decades and are difficult to modify. With stakes this high, considering how building design best supports healthcare services is important. In this narrative review, we outline why the built environment matters, with particular focus on stroke care. We also discuss challenges inherent in designing healthcare environments, undertaking research and evaluating completed architecture.
The planning and design process for new healthcare environments is incredibly complex, but, in general, it occurs in three overlapping stages: (1) the planning stage in which the healthcare provider describes the users’ needs, model of care, and clinical program in a functional brief that summarizes the requirements for the new hospital; (2) the design stage in which these requirements are interpreted by architects to develop an initial concept which is then refined to a more detailed design; and (3) the delivery stage in which the building is constructed. The extent to which hospital staff and patients are included at each stage of this process can vary significantly between projects. 2
Healthcare professionals have long advocated for design features thought to benefit health and well-being, such as natural light, ventilation, and space between patients—for example, the circular hospital design proposed by the physician Antoine Petit 3 and long “Nightingale wards” proposed by Florence Nightingale. 4 Hospital design is now informed by a process termed “evidence-based design” (EBD), in which research evidence is used alongside other considerations such as the healthcare context, budget, and architects’ experience, to inform the design of the healthcare built environment.5,6 In this context, the “healthcare built environment” encompasses: (1) the physical construction (layout, room dimensions, doors and window placement, outdoor and community access, etc.), (2) ambient features (noise, air quality, light, temperature, etc.), and (3) interior design (furniture, signage, equipment, artwork, etc.). 7 Analogous to evidence-based clinical practice, hospitals designed following best research evidence garnered from EBD processes have better safety, patient outcomes, staff retention, and operation costs.8,9 The Center for Health Design, established in 1993 to advance EBD, now maintains a repository of over 5,000 articles on healthcare design (https://www.healthdesign.org).
The field is growing; however, many healthcare contexts, including stroke, have a limited built environment evidence base. 10 Establishing geographically organized stroke units has been an important focus 11 ; however, these studies rarely address specifics of the built environment, and we know little about optimal stroke unit design. Stroke clinical guidelines rarely mention the built environment nor provide guidance on how the environment might best support care. There are currently no stroke care-specific building standards, nor standardized checklists to evaluate the quality of these environments. 12
Why is the built environment neglected? Clinicians may identify as knowing less about how the environment might influence patient care or staff well-being. They may also feel uninformed about the design process and how to contribute their clinical expertise to influence decision-making. To begin to address these gaps, our objectives for this review were: (1) to introduce readers to healthcare built environment research and (2) to highlight evidence that underpins acute, subacute, or rehabilitation stroke care facility design. This review is in three parts:
Overview of healthcare built environment research; Stroke care built environment evidence; and Planning and design of new healthcare environments: Challenges and opportunities.
We include research from recent, relevant systematic reviews, other evidence summaries, and selected qualitative and mixed-methods research focusing on healthcare environments and design. Healthcare environments are complex and context-specific, with many interdependent variables that can rarely be isolated. This complex system does not readily lend itself to highly controlled experimental research designs in real-life settings. 13 Qualitative methods, such as case studies and pre- and post-occupancy evaluations (before and after a redesign or redevelopment), are common. With research still developing, heterogeneity exists in research designs, outcomes, environments, populations, and theoretical frameworks employed. 14 Hence, robust summary evidence derived from meta-analyses is lacking.
Healthcare built environment research
Research is dominated by studies conducted in acute environments such as emergency, surgery, and intensive care units (ICUs) (Figure 1).6,15,16 Older people, including those in dementia care, are frequently studied post-acute populations.
17
The volume of built environment research conducted in different healthcare settings. Circle size indicates the number of published research articles based on systematic literature review in preparation
18
and articles listed in the Centre for Healthcare Design research repository. Pink circles represent all built environment research, and the dark gray circles indicate stroke-specific research. (The aerial sketch in this image has been adapted with permission from Architectus + HDR.)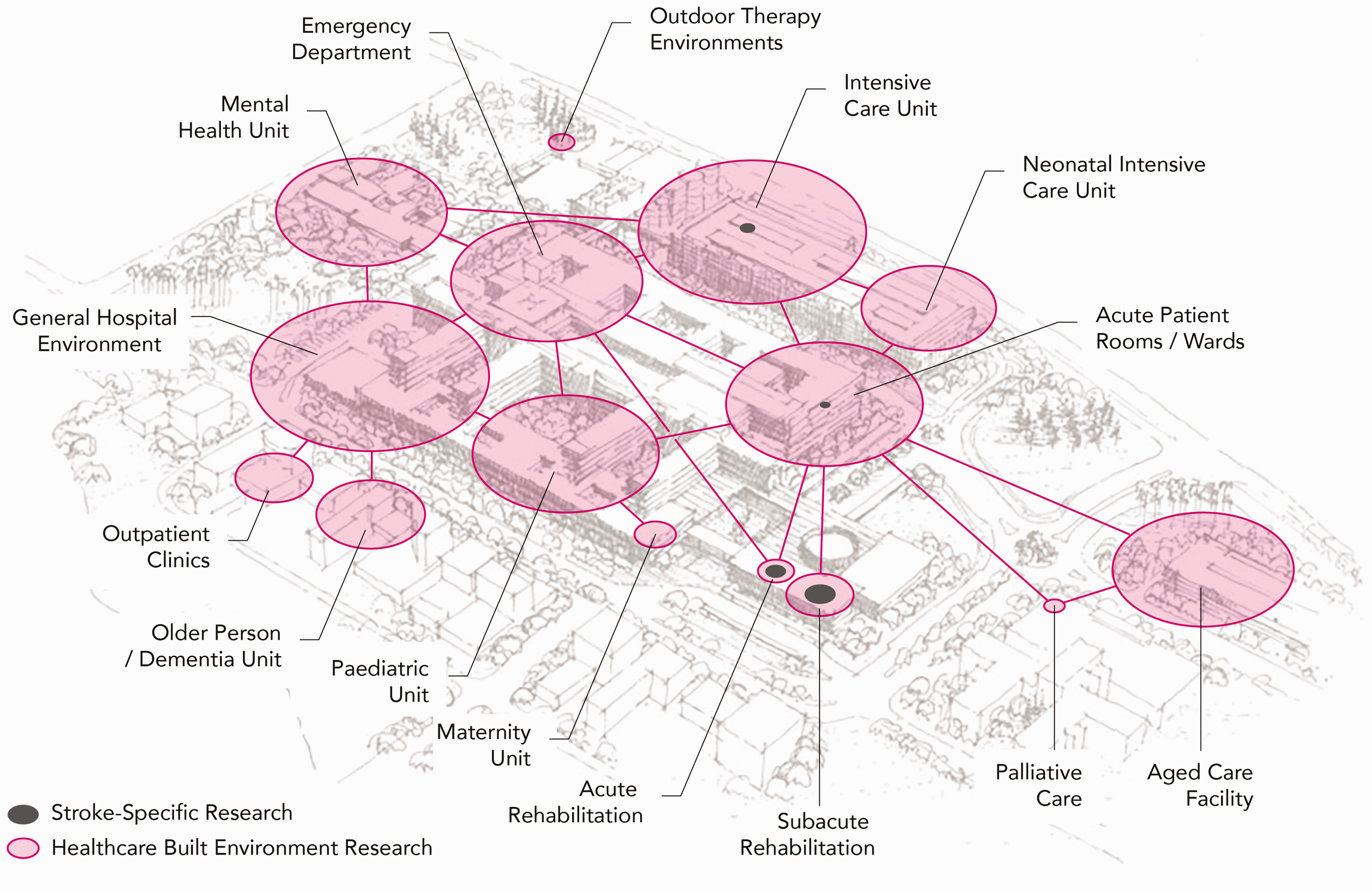
In this section, we introduce three topics relevant to most healthcare contexts: (1) design of internal spaces; (2) outdoor spaces; and (3) ambient features including light, noise, and air quality (with particular focus on infection control).
Internal spaces
The design of internal spaces, such as ward configuration, corridor design, and nurse station placements (centralized vs. decentralized), can influence patient visibility, safety, teamwork, distances staff walk in a shift, and time spent providing direct care to patients. 10 For example, open-plan, larger convex spaces can lead to greater patient visibility, and corridor width impacts staff circulation, informal communication, and teamwork. 19 In ICU, designs with centralized nurse stations and visibility of most patient rooms from that location are increasingly being replaced with decentralized nurses’ stations, arguably without strong evidence. 19 In emergency departments, with similar critical visibility requirements for teamwork and patient monitoring, some authors argue that physically separated zones or “pods” are neither efficient nor safe. 20 Decentralized nursing stations can lead to more patient room visits by staff.21,22 This highlights current uncertainties.
The layout of hospital spaces and line of sight influences patient and visitor orientation and their ability to find their way around (“wayfinding”). 23 Signs, information boards, and “landmarks” (artwork, furniture, views, etc.) are typical wayfinding elements.24,25 Inadequate wayfinding leads to delays in accessing services or finding people or places, associated stress, and higher staff burden as they provide directions for lost individuals. 25 While some standards exist, wayfinding is often not optimized in healthcare. 26
The proportion of single versus multiple(two or more)-bed rooms is a prominent ward design consideration. There is evidence that single rooms can support staff/patient communication, privacy, infection control, and noise reduction, but they are also associated with patient isolation and increased falls risk. 27 This evidence is, however, of mixed quality, limited to certain populations, with neutral and/or contrary results. 27 A higher proportion of single rooms generally results in longer corridors, longer staff walking distances, perceived decrease in patient visibility due to compromised sightlines, and higher construction and cleaning costs. 28 The inherent trade-offs will be different in every healthcare context. Less controversial is location of sinks and hand sanitizers; highly visible and standardized positioning promotes more consistent use.29,30
Outdoor spaces
Hospital gardens were historically commonplace 31 ; however, less priority has been given to green space over time. Access to the outdoors and time in nature has been linked to stress reduction, improved physical symptoms, and emotional well-being in many healthcare settings. 32 Views of nature have been linked to reduced length of stay. 33 Good hospital garden design principles include creating opportunities for exercise, exploration, socialization, and to engage with and escape in nature. 32 Surprisingly, patients and visitors are often not aware of hospital gardens, and proactive approaches to increasing patient and family use of gardens have been recommended. 34 Usually conceptualized as spaces for patients and visitors, staff are often their primary users. 32 Outdoor spaces can be restorative for hospital staff, helping to reduce stress and improve attention, which may improve patient care and staff retention. 35
Ambient features
Ambient features, such as light and noise, can impact patient well-being and comfort, sleep, and communication with staff.36,37 Light and noise also impact staff well-being and attention 38 and contribute to medication errors and other safety concerns. 39
Air quality is important for both comfort and infection control. Infection control is particularly prioritized in acute environments and is receiving deserved attention in the COVID-19 pandemic. A recent review of COVID-19 transmission showed that spatial configuration can affect patient density and thereby transmission. 40 Optimized systems for heating, ventilation, and air conditioning (HVAC) can filter microparticles such as viruses. Different HVAC systems also affect humidity, airflow velocities, air pressure—all important for exposure to active aerosols. Window ventilation, daylight, and electric UV light are recommended to aid disinfecting surfaces and use of surface materials that affect pathogen survival. 40
Stroke care built environment evidence
In this section, we outline how the built environment can influence important outcomes such as: (1) evidence-based stroke care, including rehabilitation; (2) efficiency of stroke care, staff processes, and communication; and (3) patient safety and well-being. The evidence-base specific to stroke care is small.
41
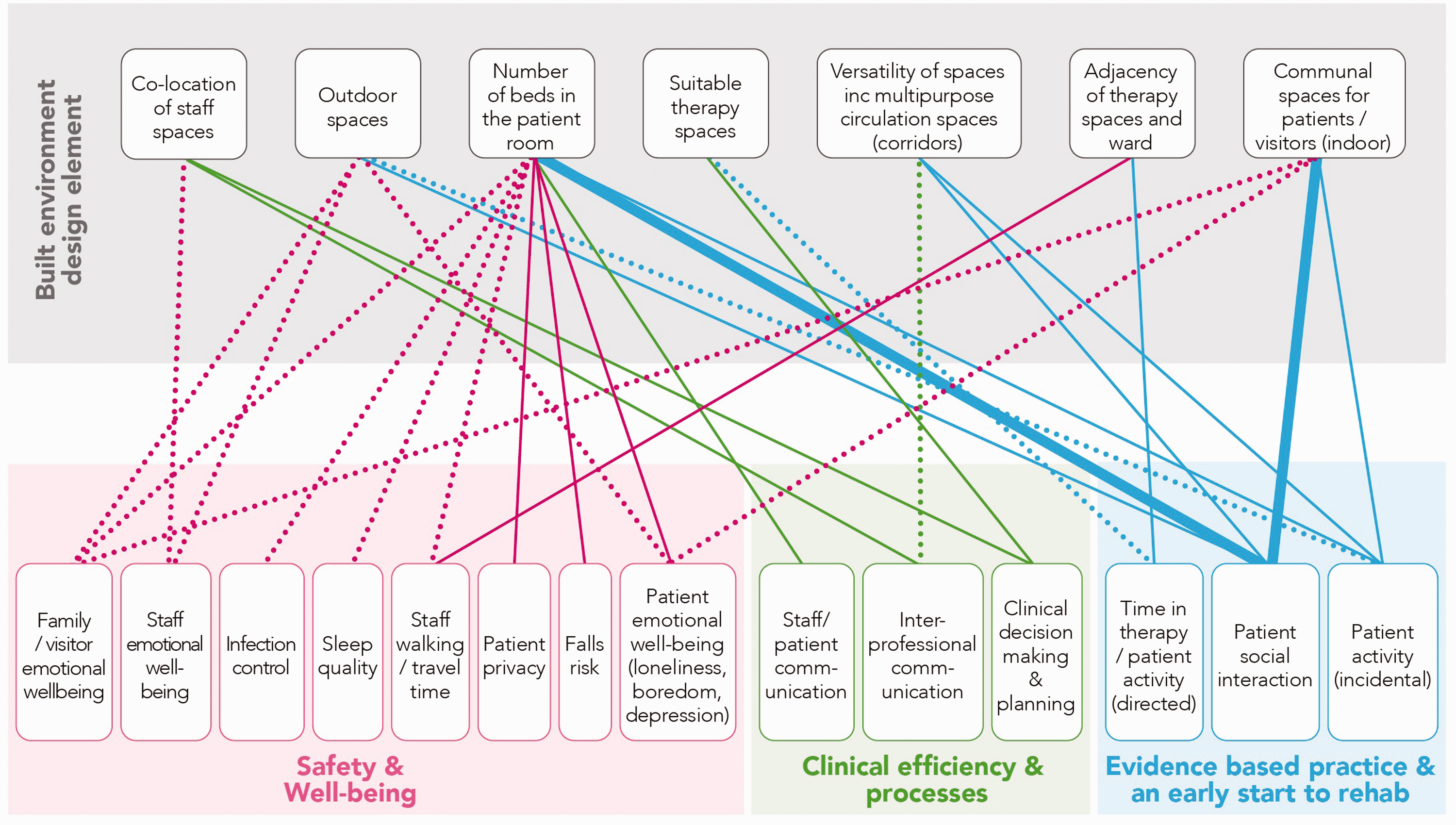
In Figure 2, we summarize the design features and how they may influence a range of outcomes including patient and staff behavior. This should be considered illustrative rather than exhaustive. Where possible, we draw directly from stroke or brain injury-specific evidence, supplementing evidence from other populations where relevant.
A summary of the evidence specific to stroke care environments. Dotted lines = a hypothesis, garnered from research in other populations; thin lines = limited evidence, < 3 studies; thick lines = moderate evidence, ≥ 3 studies, based on systematic literature review.
41
Evidence-based practice including rehabilitation
We found no stroke-specific research to underpin built environment recommendations for optimal delivery of either time-critical acute stroke treatments or evidence-based care, including rehabilitation. Guidelines recommend early commencement of both structured and incidental physical, cognitive, and social activity for all stroke patients,42,43 although recommended levels vary. Patients in both acute and subacute environments spend most of their day alone and inactive in their bedroom.44,45 While we can hypothesize that providing “draw-them-out” features on a ward may improve activity and engagement, evidence is limited. These features may include green spaces and indoor communal (social) spaces. Unfortunately, communal spaces, when present, often appear to be underutilized in both acute 46 and rehabilitation environments. 47 Many factors may influence whether patients use communal spaces, including not knowing they exist or where to find them, difficulty accessing them without help, or feeling they don’t have permission to use them. 48 In a Norwegian study across 11 stroke units with communal areas, patients were more active and spent less time in their bedroom in units where meals were served in the communal area. 49 Providing resources (games, music, books) in personalized activity packs and in communal spaces (“environmental enrichment”), with the aim to improve physical, social, and cognitive activity, has recently been tested in acute and subacute settings with mixed results.50–52 Importantly, this approach relies on staff to encourage use and engagement, rather than embedding activity opportunities into the building itself. Hallways and circulation spaces are generally underrecognized as providing spaces for incidental activity and interaction. 53
There is limited stroke-specific research about the value or harm of single- versus multiple-bed rooms. A higher proportion of single rooms may be associated with lower levels of patient activity in acute stroke.54,55 A systematic review of single- versus multiple-bed rooms in older people and those with neurological disorders found potential benefits (e.g. infection control, patient satisfaction) and harms (e.g. falls, isolation) with single rooms. 56 In rehabilitation facilities with a high proportion of single rooms, patients emphasize the importance of communal areas. 57 Further work is needed to identify and test how modifications to layout and communal and circulations spaces could enhance patient engagement, activity, and optimal care provision.
Efficiency of care, staff processes, and communication
Interprofessional communication and teamwork between physicians, nurses, and allied health professionals supports best practice stroke care. 11 Shared staff spaces support team communication and collaboration, enabling better understanding of patient needs, and greater knowledge about other team roles.58,59
Therapy spaces are often discrete locations (e.g. gym, occupational therapy rooms), rather than being holistic, context-based environments that reflect the connectivity and continuity necessary for rehabilitation and transition beyond discharge.60,61 Separation of clinical and therapy spaces can impact staff travel time, patient practice and activity, and even clinical decision-making. For example, Blennerhassett et al. 47 found that patients spent less time engaged in physical activity and more time in corridors when the ward was located further from the gym, on a separate floor. This also impacted wheelchair use and patient travel time. 47 Inaccessible therapy spaces can also change therapists’ intervention choices. 62
Safety and well-being
Falls are common after stroke, 63 yet the relationship between the built environment and falls is largely unexplored. The presence of a fellow patient (multiple-bed room) may help reduce falls, especially for older patients with neurological injury.56,64 Roommates play an important role in monitoring the physical and mental health of others in stroke rehabilitation. 48 Stroke patients often experience loneliness when in hospital,65,66 and some patients will choose a shared room over the privacy of a single room. 57 Sleep is important for recovery. Unsurprisingly, visual and aural privacy is less in multiple-bed rooms. However, noise traveling between corridors and bedrooms and lack of dedicated staff spaces for confidential conversations are also important. 48
Planning and design of new healthcare environments: Challenges and opportunities
Healthcare environments research and design is a multistakeholder endeavor involving government, healthcare providers, managers, clinical staff, patients, architects, quantity surveyors, construction companies, building managers, etc. This collaborative process can be challenging,67,68 considering interdisciplinary differences in knowledge and approaches. 69 The complexity of hospital procurement and the fact that design and construction processes are foreign to many healthcare professionals adds further challenge. Clinicians often do not understand what the “user group” consultation process is supposed to achieve, and their involvement may be inconsistent throughout the design process, which limits their contribution to the process and ability to influence decisions. 67 While collaboration between architects and healthcare professionals is not new, 70 limited evidence informs current consultation processes.67,71 High-quality healthcare environments are produced when shared decision-making and collaboration happens across healthcare, construction, and architecture to create designs based on evidence and end-users’ perspectives. 69
A number of research approaches are suggested to facilitate this collaboration, including participatory design, co-design, and Living Labs.2,72,73 Over many years, our team has built partnerships between healthcare environment practitioners, clinicians, researchers, and people living with stroke, which have served to create a common understanding of the barriers and opportunities for redesigning and optimizing stroke care environments. With the creation of the Neuroscience Optimized Virtual Living Lab (NOVELL) for stroke rehabilitation redesign (www.novellredesign.com), we are working to develop new models for stakeholder engagement and research, and to contribute new evidence to stroke rehabilitation design.
In addition to collaboration challenges, research is infrequently embedded in the planning and design of new healthcare environments, and leaders in EBD have long called for appropriately funded, transparent, and freely available evaluations of completed buildings.74–76 Given the cost of constructing and running healthcare buildings, the absence, or non-disclosure, of evaluations to determine whether desired outcomes were met is concerning.77,78 Hospital design and construction is underpinned by technical and generic building guidelines and standards that differ within and between countries. The degree to which these standards are “evidence-informed” varies. In stakeholder consultations, understanding what is evidence-based and what is open to change can be difficult. Design innovation is essential if hospital buildings are to respond to new healthcare models or processes. For example, the recent COVID-19 induced surge in utilization of telehealth and other e-health technologies for rehabilitation, other treatment, and communication with people with stroke has implications for healthcare design, increasing demand for spaces for videoconferencing, equipment storage, and potential changes to waiting rooms and on-site consultation spaces.79,80 Future design considerations for stroke recovery should also extend to the home environment. 81
Conclusion
The built environment matters. It can impact healthcare delivery and patient and staff outcomes. An evidence base is growing in some areas of healthcare design, while others require significant further research. The potential for both hospital and health services design innovation is strong. By continuing to build this evidence base, EBD can complement architectural processes to deliver high-performing healthcare assets. Involving engaged and informed clinicians in built environment design and research will help shape hospitals of the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NOVELL is funded by the Felton Bequest and the University of Melbourne. Julie Bernhardt is funded by an NHMRC Research Fellowship (1154904). The Florey Institute of Neuroscience and Mental Health acknowledges support from the Victorian government and in particular funding from the Operational Infrastructure Support Grant.