
Abstract
Background
Stroke Coach is a lifestyle coaching telehealth program to improve self-management of stroke risk factors.
Aims
To examine the efficacy of Stroke Coach on lifestyle behavior and risk factor control among community-living stroke survivors within one-year post stroke.
Methods
Participants were randomized to Stroke Coach or an attention control Memory Training group. Lifestyle behavior was measured using the Health Promoting Lifestyle Profile II. Secondary outcomes included specific behavioral and cardiometabolic risk factors, health-related quality of life (HRQoL), cognitive status, and depressive symptoms. Measurements were taken at baseline, post-intervention (6 months), and retention (12 month). Linear mixed-effects models were used to test the study hypotheses (p < 0.05). All analyses were intention-to-treat.
Results
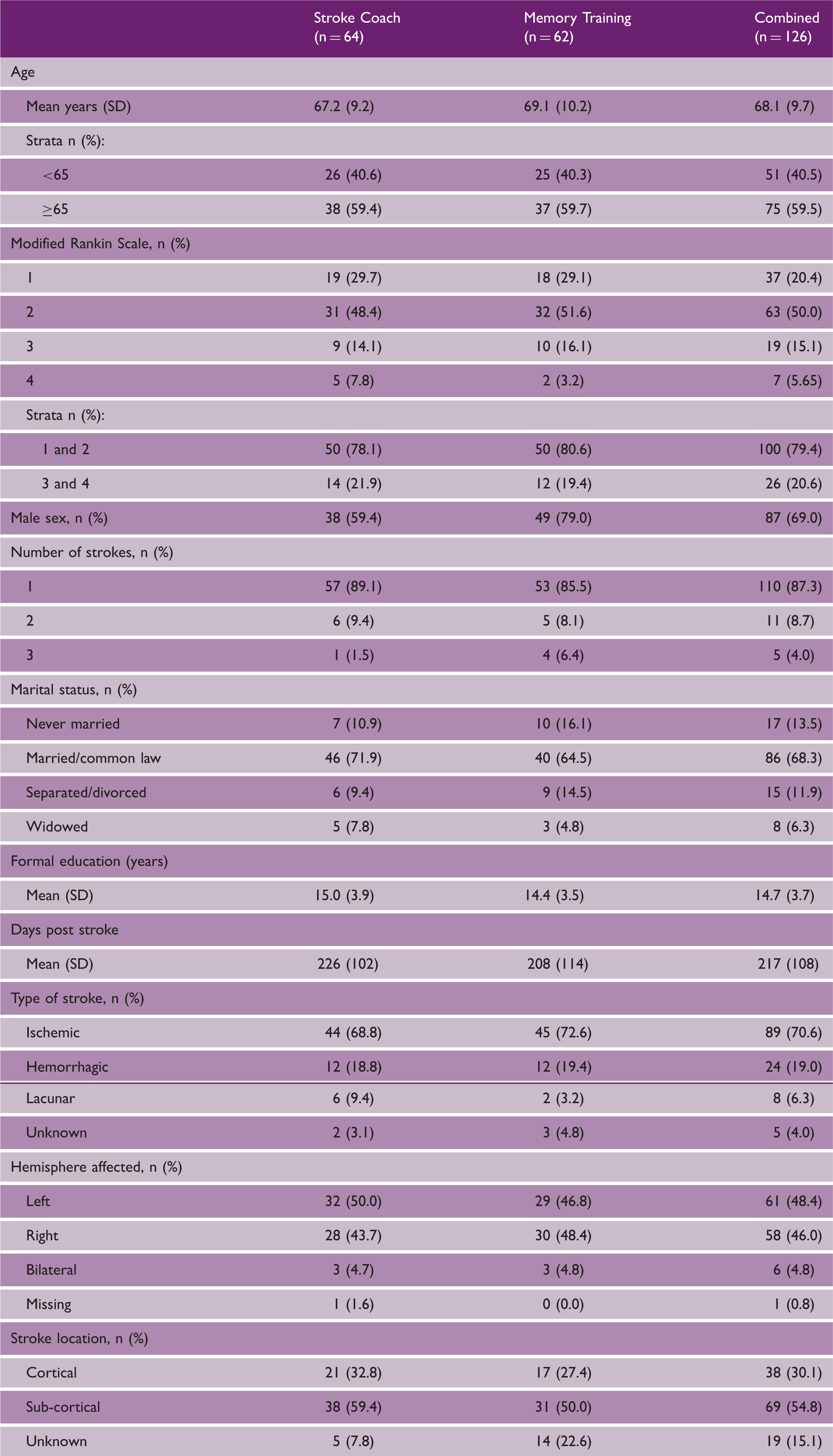
The mean age of the Stroke Coach (n = 64) and Memory Training (n = 62) groups was 67.2 and 69.1 years, respectively. The majority of participants (n = 100) had mild stroke (modified Rankin Scale = 1 or 2), were active, with controlled blood pressure (mean = 129/79 mmHg) at baseline. At post-intervention, there were no significant differences in lifestyle (b = −2.87; 95%CI − 8.03 to 2.29; p = 0.28). Glucose control, as measured by HbA1c (b = 0.17; 95%CI 0.17 to 0.32; p = 0.03), and HRQoL, measured using SF-36 Physical Component Summary (b = −3.05; 95%CI −5.88 to −0.21; p = 0.04), were significantly improved in Stroke Coach compared to Memory Training, and the improvements were maintained at retention.
Conclusion
Stroke Coach did not improve lifestyle behavior; however, there were improvements to HbA1c and HRQoL among community-living stroke survivors with mild stroke-related disability. (ClinicalTrials.gov identifier: NCT02207023)
Introduction
Stroke has considerable long-term consequences, notably deficits in motor and sensory function, communication, and cognition. These deficits pose serious barriers for stroke survivors to effectively manage their health. Unfortunately, post-discharge care remains underdeveloped for stroke survivors1,2 and stroke survivors are observed to have high rates of secondary cerebrovascular events. 3 There is a need for the development and investigation of innovative secondary prevention health services for stroke survivors.
We developed the Stroke Coach, a novel telehealth intervention to promote healthy lifestyle behaviors after stroke.4,5 Stroke Coach was developed using Intervention Mapping as a guiding framework to ensure the intervention was theoretically guided and comprised of evidence-based behavior change techniques. 6 Social Cognitive Theory was the underlying premise for behavior change, while Control Theory methods were directed towards sustaining the changes to ensure long-term health benefits. Furthermore, Stroke Coach is based on evidence that improvements to lifestyle can improve cardiometabolic risk,7,8 and that the delivery of health services using technology to stroke survivors is feasible and acceptable. 9 Stroke Coach resources and manuals are available at www.neurorehab.ubc.ca.
Aims and hypotheses
We hypothesized that individuals who participate in Stroke Coach would experience greater improvements in lifestyle behavior than individuals in an attention-controlled Memory Training Program. We also examined the effects of Stroke Coach on individual behavioral and cardiometabolic stroke risk factors, quality of life, and health outcomes.
Methods
Study design and participants
In this multi-site, single-blinded (assessors) randomized controlled trial we recruited from acute, rehabilitation, and outpatient stroke units from four regional hospitals in British Columbia, Canada. We used multiple recruitment strategies, including in-person recruitment by clinicians and research coordinators and mailouts. Participants were community-living individuals, ≥50 years of age, within one-year post-stroke, with a modified Rankin Scale (mRS) 10 score of 1 to 4, and telephone access. The University of British Columbia Clinical Research Ethics Board approved the study (H13-03353), and all participants provided informed consent. This study’s protocol is reported in detail elsewhere. 5 Appendix A documents our reporting of the study according to the consolidated standards of reporting trials (CONSORT) guidelines. 11
Baseline evaluation (T1 = 0 months)
Sociodemographic and stroke information were collected using a self-report form.
Primary outcome
Lifestyle behavior was measured using the 52-item Health Promoting Lifestyle Profile II (HPLPII). 12 We determined 50 participants per group would have 85% power to detect a group mean difference of 12 points13,14 on the HPLPII (alpha = 0.05). We recruited 126 participants to adjust for a potential 20% dropout.
Secondary outcomes
Health-related quality of life (HRQoL) was measured using the Physical and Mental Component Summaries of the Medical Outcomes Study: Short Form-36. 15 Depressive symptoms and cognitive function were assessed using the Center for Epidemiologic Studies Depression Scale 16 and Montreal Cognitive Assessment, 17 respectively.
Walking physical activity averaged over four days was measured using the StepWatch Activity Monitor. 18 Daily grams of fat consumption, medication adherence, and body composition were measured using the Canadian version of the SmartDiet Questionnaire, 19 Morisky Medication Adherence Scale,a,20 and body mass index, respectively. Blood pressure measurements 21 were taken using a digital blood pressure monitor. Glycated hemoglobin (HbA1c), fasting glucose, high- and low-density lipoprotein, C-reactive protein, and homocysteine were measured using standard outpatient blood laboratory services.
Randomization and interventions
Participants were randomized 1:1 using a blocked (two and four) randomization computer algorithm (www.randomize.net). Concealed randomization was stratified by age (<65 and ≥65 years), and stroke severity (mRS scores 1–2 and 3–4). Randomization was completed by a researcher who was not involved with data collection or delivering the intervention.
Stroke Coach
Over six months, participants received seven 30- to 60-min telephone sessions on a one-to-one basis (and five 5- to 10-min ‘check-in’ calls) with a trained lifestyle coach. Participants also received a self-management manual, a self-monitoring kit, and a health report card (adapted from Wister et al. 22 ) with grades ranging from A (good control) to F (poor control) on their behavioral and cardiometabolic stroke risk factors. The development of Stroke Coach is reported in detail elsewhere. 4
Memory Training
Participants received: (1) memory coaching at the same schedule and frequency of telephone calls as Stroke Coach; (2) a memory training manual consisting of seven lesson plans, homework, and cognitive exercises; and (3) an agenda to schedule appointments and make reminder notes.
Coaches in both programs were health professionals (e.g. physical therapists) or research assistants with graduate level training (e.g. Masters of Science), and experience working with individuals with stroke.
Post-intervention and retention evaluations (T2, T3)
Outcomes collected at T1 were collected at T2 and T3. Participants also completed an exit satisfaction survey at T2 to explore their experience in Stroke Coach.
Statistical analyses
Descriptive statistics characterized the sample. Between group differences were estimated using linear mixed effects models, with a random effect for each subject. An interaction term between time and group was included in each model. Time was included as a categorical variable, with T2 as the referent category. Baseline measures were included in all models. The relationship between baseline characteristics and attrition was assessed using logistic regression. The R software package, Linear Mixed-Effects Models using Eigen and S4, was used for all analyses at an alpha of 0.05. 23
Results
A total of 126 participants were recruited between August 2014 and November 2018 with the final measurement session in February 2020; 831 individuals who had a stroke within the last 12 months were provided with study information (either via mailout or in-person); 295 of these individuals made contact with the research team, of which 75 were ineligible. Of the 219 that were eligible, 93 declined to participate (38 were not interested, 31 lost contact with the research team, 14 were too busy, 9 had issues attending in-person assessments, and 1 only wanted to participate in one of the programs and not the other), as shown in Figure 1. Sixty-four participants were randomized to Stroke Coach.
CONSORT flow diagram of study participants.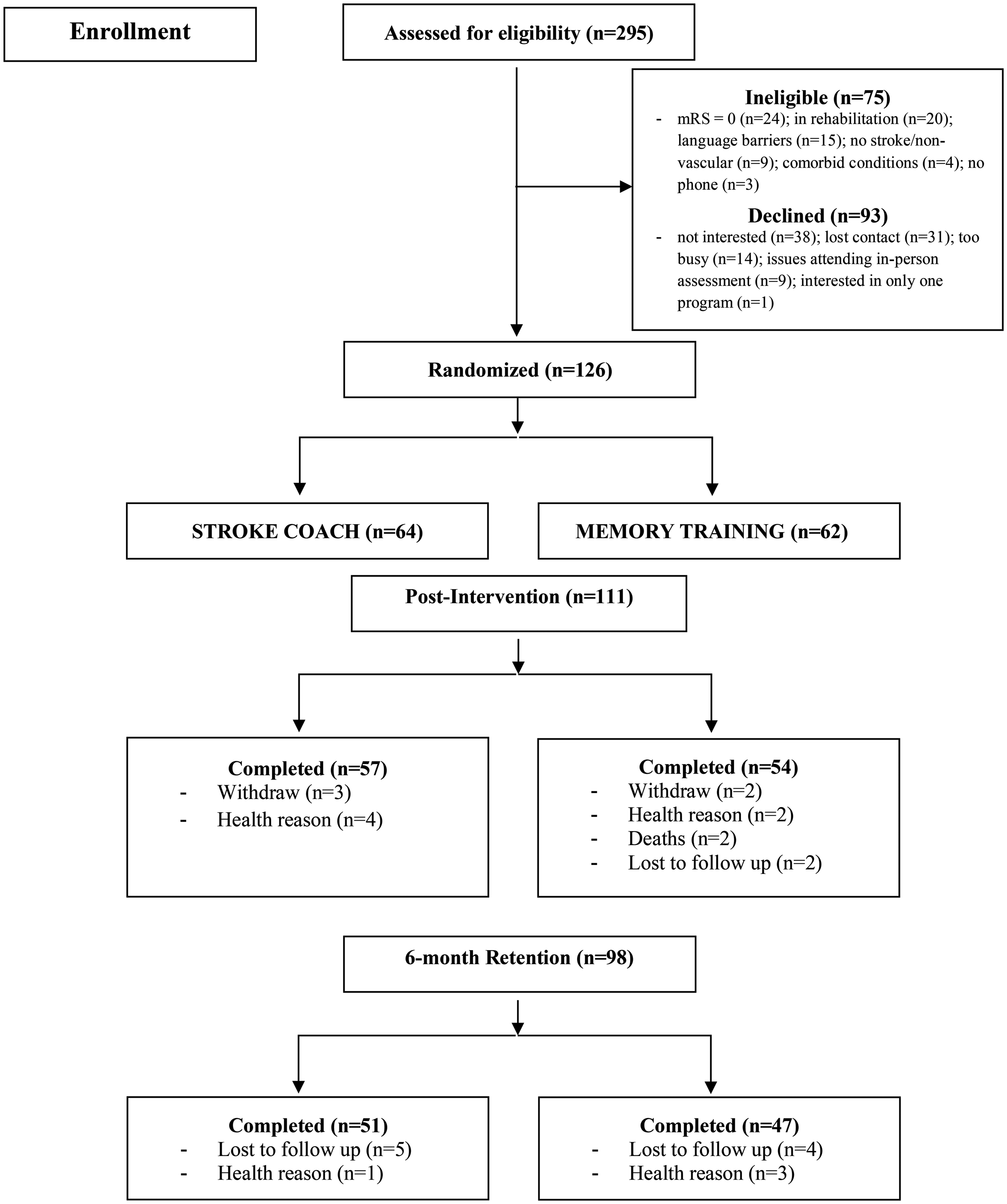
Participant demographics and clinical characteristics.
Descriptive statistics (mean (SD)) of study outcomes at all timepoints.
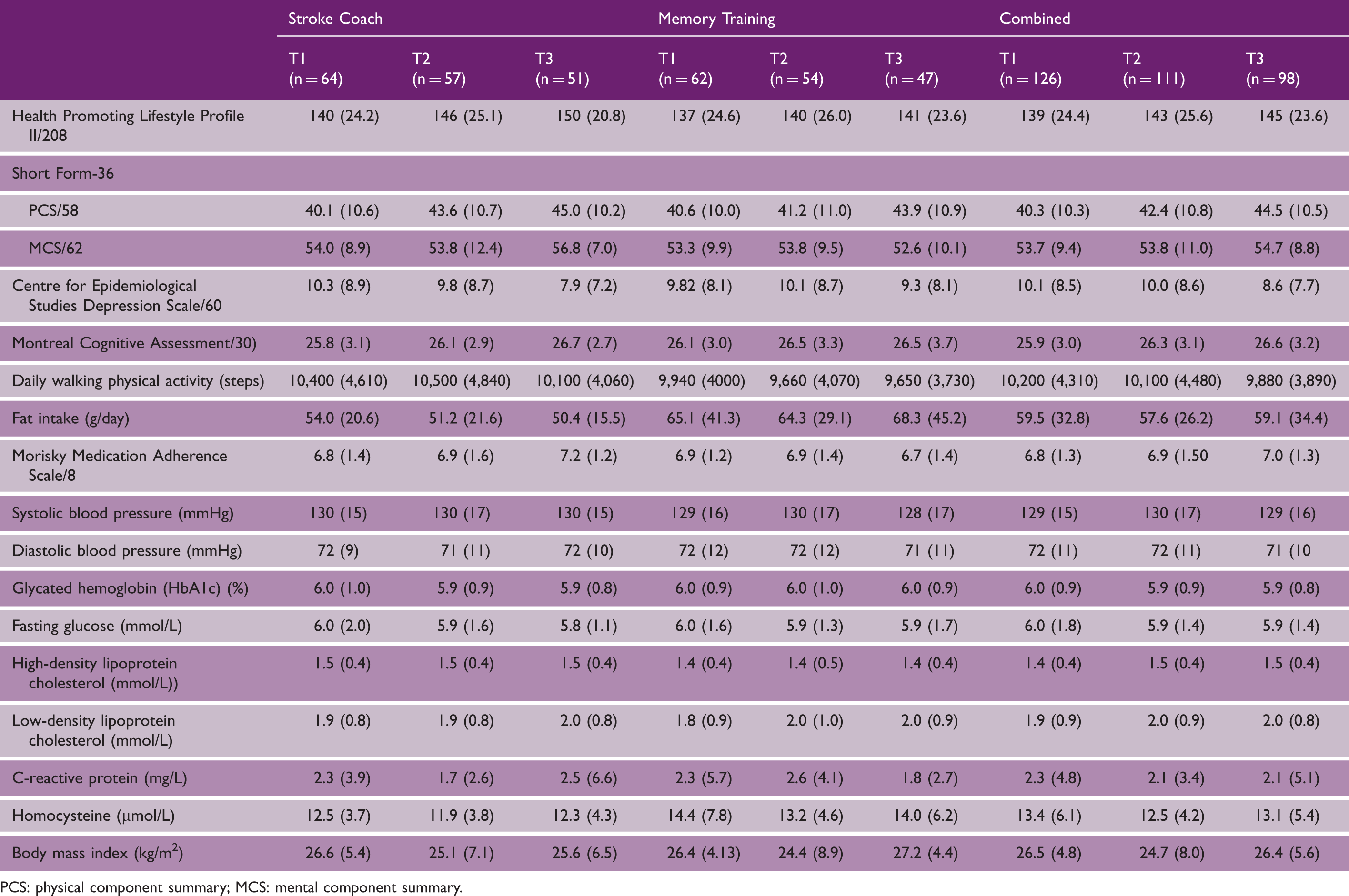
PCS: physical component summary; MCS: mental component summary.
There was an overall attrition rate of 20% in Stroke Coach and 24% in Memory Training (p = 0.67). Figure 1 presents the flow of participants through the study stages. Our logistic regression analyses indicated no systematic differences between those retained and those not completing the study protocol.
Protocol adherence
Of the 57 participants completing Stroke Coach, 56 completed all coaching sessions and 55 completed all check-in sessions. Of the 54 participants completing Memory Training, 52 completed all sessions and 46 completed all check-in sessions. Participants completed Stroke Coach in a mean of 188.7 days (SD = 30.2 days) and Memory Training in 188.0 days (SD = 52.5 days) (p = 0.93).
Post-intervention follow-up (T2 and T3)
Primary outcome
Linear mixed effects models for the statistically significant primary and secondary outcomes.
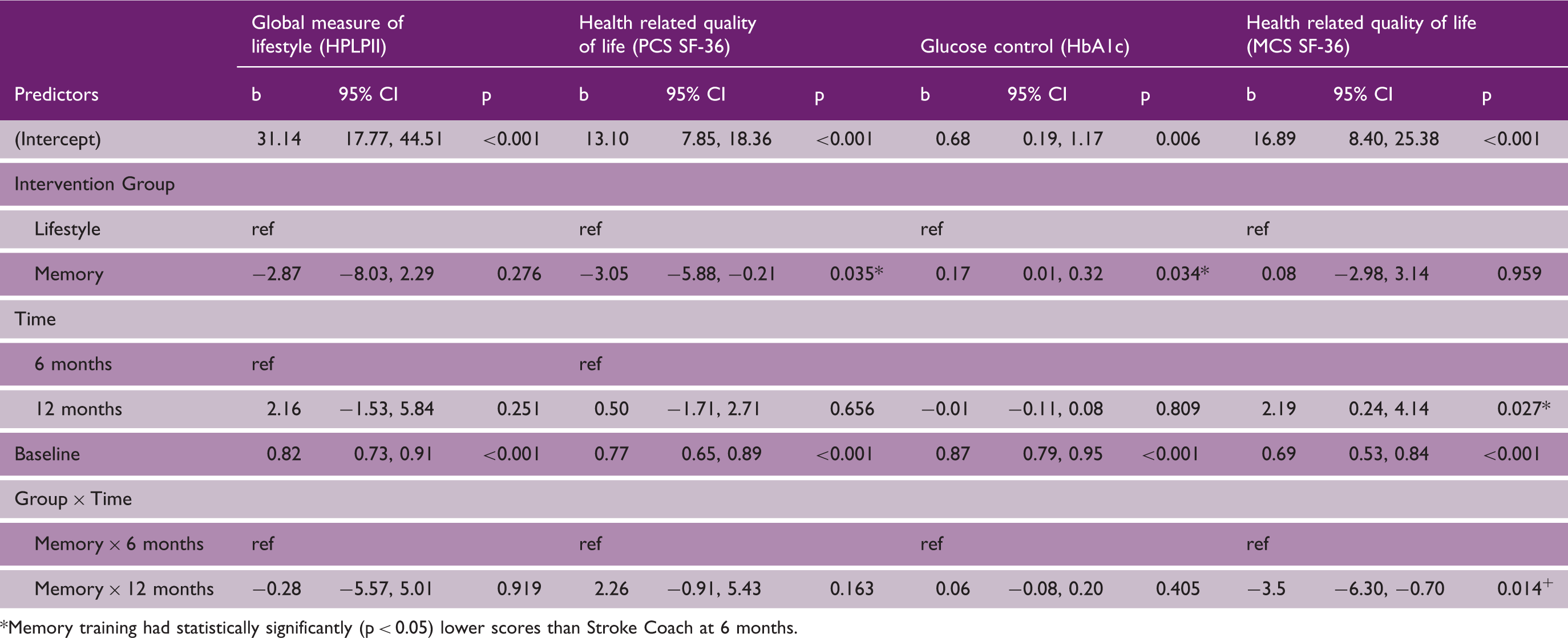
Memory training had statistically significantly (p < 0.05) lower scores than Stroke Coach at 6 months.
Secondary outcomes
Both HRQoL (Physical Component Summary) (b = −3.05; 95%CI −5.88 to −0.21; p = 0.04) and HbA1c (b = 0.17; 95%CI 0.17 to 0.32; p = 0.03) had significant differences between Stroke Coach and Memory Training at T2, as shown in Table 3. These effects were maintained over time. Stroke Coach also had a statistically significant increase in HRQoL (Mental Component Summary) between 6 and 12 months (p = 0.027) that was also significantly greater than Memory Training (p = 0.014).
No other outcomes had significant between-group differences; however, fat consumption reduced by 4 g per day in Stroke Coach and increased by roughly 3 g per day in Memory Training at T3. Appendix B presents the mixed effect models of the secondary outcomes.
Exit satisfaction survey
Results from the exit satisfaction survey.
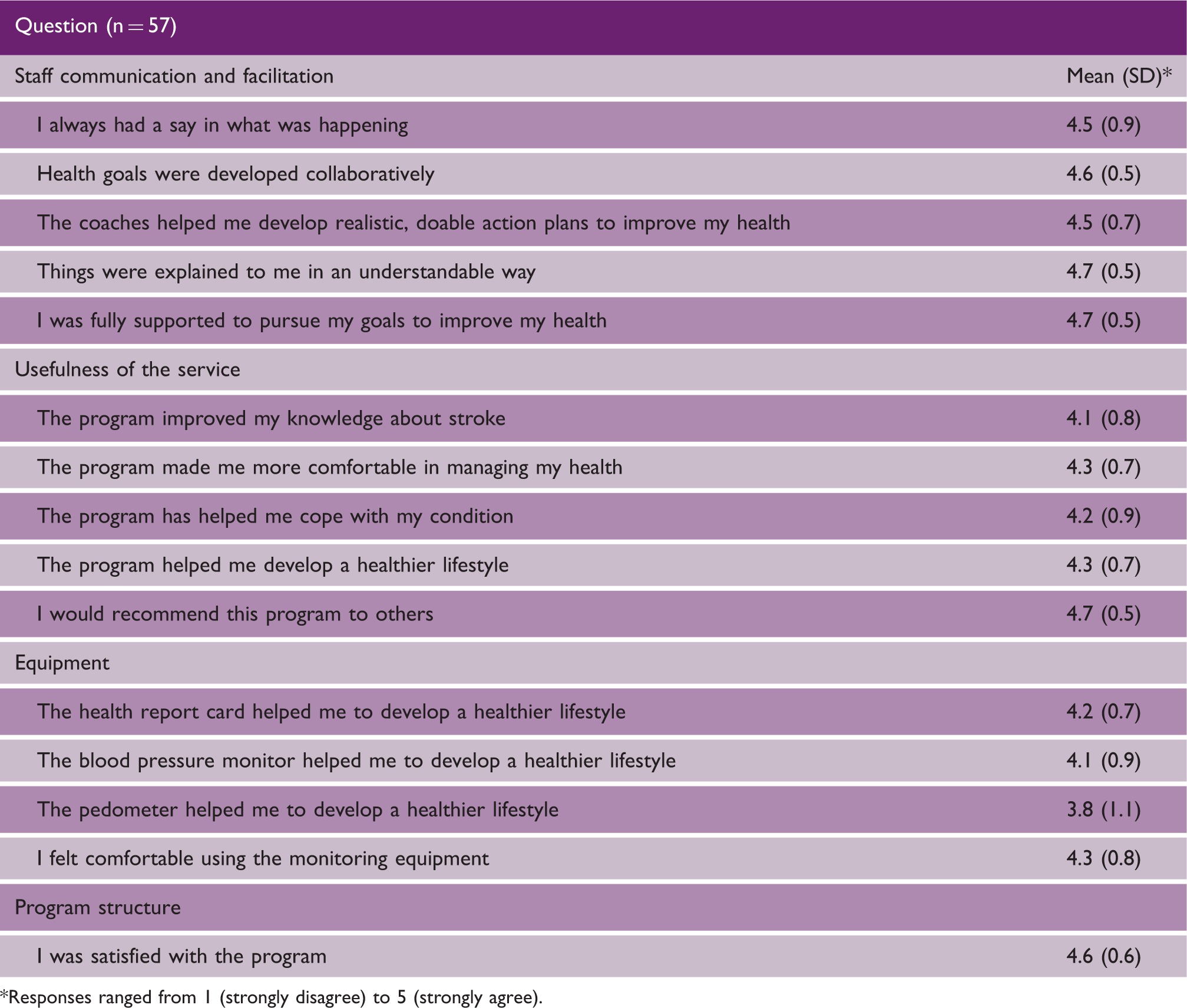
Responses ranged from 1 (strongly disagree) to 5 (strongly agree).
When asked about “dislikes,” participants reflected on the use of their telephone to receive the coaching program. Participants stated, “Speaker phone wasn’t clear,” and that, “…it’s difficult to express through the telephone.” Others stated that sometimes the sessions were too short, while others discussed the focus of the program. One participant suggested expanding the focus to include functional limitations after stroke, and others indicated that because they had healthy lifestyles the program might have had limited utility.
Discussion
We examined the efficacy of lifestyle coaching on secondary stroke prevention indicators. Our results suggest that lifestyle coaching does not improve lifestyle behavior, but does statistically significantly improve HRQoL and HbA1c.
In stroke, coaching has been used primarily to improve functioning and physical capacity,24,25 with unsuccessful results. Our study is one of the first to examine lifestyle coaching for self-management of stroke risk factors and secondary prevention. It also addresses recent calls for the investigation of coaching for behavioral modification in stroke survivors. 26 Unfortunately, our results parallels existing evidence in that coaching did not improve our primary outcome, this time however focusing on lifestyle behavior. A plausible explanation for this observation is that our sample reported healthy behaviors at baseline, and thus there may have been little room for improvement.
Stroke Coach, however, did result in important changes in the secondary outcomes of HRQoL and HbA1c. These findings support existing research examining self-management programs on HRQoL among stroke survivors. Authors of a Cochrane review that meta-analyzed results from six studies concluded that self-management programs improve HRQoL in people with stroke. 27 While similarities exist, evidence from the Cochrane review is from studies examining self-management programs aimed towards functional and physical recovery. Thus, our results are unique in that Stroke Coach is specifically aimed to improve lifestyle behaviors.
Our results of a statistically significant effect at lowering HbA1c compared to the attention-control group has important implications, especially when considering that a 1 percentage point decrease in HbA1c is associated with 18% decrease in overall cardiovascular risk and 17% decrease for risk of stroke. 28 While our findings are consistent with coaching research in the broader chronic disease literature, 29 they differ from a Cochrane review which found no improvements in HbA1c from the control comparators for improving modifiable risk factor control for secondary prevention after stroke. 30 The interventions included for review, however, differed from Stroke Coach in that they were not client-centered and did not involve aspects of lifestyle coaching, goal setting, action planning or self-monitoring. 30 More recently, Towfighi et al. examined the Healthy Eating and Lifestyle After Stroke program, and also reported no difference in HbA1c between groups. 31 Although this program included similar components to Stroke Coach, it was delivered in a group format and lacked the individualized coaching that our study participants appreciated. Furthermore, our finding may also be explained by the reduced fat consumption by individuals in Stroke Coach compared to Memory Training, considering evidence of an association between fat consumption and HbA1c. 32
Limitations
Our study was comprised primarily of participants who were mildly affected by stroke and had high levels of activity. In addition, the group mean systolic blood pressure was within guideline recommendations, 33 suggesting that the cardiovascular risk for this group was not high, and this may have limited the potential for improvements. The self-report nature of our primary outcome may have been affected by social desirability. Similarly, our outcomes may have been influenced by assessor bias, as we did not perform an assessment of unblinding. Finally, our small sample size may have missed an effect due to chance; similarly, the differences in HRQoL and HbA1c may have been due to the open nature of the study and chance.
Conclusion
Stroke Coach did not improve lifestyle behavior compared to an attention matched control intervention. Lifestyle coaching however appears to improve HRQoL and glucose control among community-living stroke survivors with mild stroke-related disability.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930211017699 - Supplemental material for Telehealth coaching to improve self-management for secondary prevention after stroke: A randomized controlled trial of Stroke Coach
Supplemental material, sj-pdf-1-wso-10.1177_17474930211017699 for Telehealth coaching to improve self-management for secondary prevention after stroke: A randomized controlled trial of Stroke Coach by Brodie M Sakakibara, Scott A Lear, Susan I Barr, Charlie H Goldsmith, Amy Schneeberg, Noah D Silverberg, Jennifer Yao and Janice J Eng in International Journal of Stroke
Footnotes
Authors’ contributions
BMS, JJE: conception and design, drafting of the manuscript, critical review of the manuscript; SAL, SIB, CHG, AS, NDS, JY: critical review of the manuscript. All authors approved final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by: Canadian Institutes of Health Research Postdoctoral Fellowship (BMS) and Operating Grant (FND-143340); Michael Smith Foundation for Health Research Postdoctoral Fellowship (BMS) and Senior Scholar Award (JJE); Canada Research Chair Program (JJE); Pfizer/Heart and Stroke Foundation Chair in Cardiovascular Prevention Research at St. Paul’s Hospital (SAL); Michael Smith Foundation for Health Research Health Professional Investigator Award (NDS); and the Heart and Stroke Foundation Canadian Partnership for Stroke Recovery Operating Grant.
Notes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.