
Abstract
Background
Treatment with intravenous alteplase for eligible patients with acute ischemic stroke is underused, with variation in treatment rates across the UK. This study sought to elucidate factors influencing variation in clinicians’ decision-making about this thrombolytic treatment.
Methods
A discrete choice experiment using hypothetical patient vignettes framed around areas of clinical uncertainty was conducted with UK-based clinicians. Mixed logit regression analyses were conducted on the data.
Results
A total of 138 clinicians completed the discrete choice experiment. Seven patient factors were individually predictive of increased likelihood of immediately offering IV alteplase (compared to reference levels in brackets): stroke onset time 2 h 30 min [50 min]; pre-stroke dependency mRS 3 [mRS 4]; systolic blood pressure 185 mm/Hg [140 mm/Hg]; stroke severity scores of NIHSS 5 without aphasia, NIHSS 14 and NIHSS 23 [NIHSS 2 without aphasia]; age 85 [68]; Afro-Caribbean [white]. Factors predictive of withholding treatment with IV alteplase were: age 95 [68]; stroke onset time of 4 h 15 min [50 min]; severe dementia [no memory problems]; SBP 200 mm/Hg [140 mm/Hg]. Three clinician-related factors were predictive of an increased likelihood of offering IV alteplase (perceived robustness of the evidence for IV alteplase; thrombolyzing more patients in the past 12 months; and high discomfort with uncertainty) and one with a decreased likelihood (high clinician comfort with treating patients outside the licensing criteria).
Conclusions
Both patient- and clinician-related factors have a major influence on the use of alteplase to treat patients with acute ischemic stroke. Clinicians’ views of the evidence, comfort with uncertainty and treating patients outside the license criteria are important factors to address in programs that seek to reduce variation in care quality regarding treatment with IV alteplase. Further research is needed to further understand the differences in clinical decision-making about treating patients with acute ischemic stroke with IV alteplase.
Keywords
Introduction
Stroke remains a leading cause of death and disability. 1 Thrombolysis with recombinant tissue plasminogen activator (intravenous (IV) alteplase) is a cost-effective treatment for acute ischemic stroke that reduces stroke-related disability, but unwarranted variation exists in UK thrombolysis rates 2 despite a strong evidence base3,4 reflected in the National Stroke Strategy, 5 National Institute for Health and Care Excellence (NICE) guidelines, 6 and treatment licensing criteria. 7 Since the expansion of 24/7 hyper-acute stroke services, organizational factors seem less likely to explain this variation, which may be accounted for by variation in clinical decision-making, based on interpretation and understanding of clinical factors, and on characteristics of the individual decision-makers (such as experience, attitude towards risk). The study aimed to elucidate patient and clinician factors that influence clinicians’ decision-making about the offer of IV alteplase to patients with acute ischemic stroke.
Clinical decision-making about IV alteplase is complex. The time limited window for treatment (maximum 4.5 h since symptom onset) and the many clinical factors that might influence the balance between the risk and benefit for individual patients factor into this high stakes decision. 8 Earlier treatment is associated with better outcomes, yet there is a small but significant risk of adverse outcomes, mainly due to treatment-related symptomatic intracranial hemorrhage (sICH). 9 Decision-making is further complicated by uncertainty in research evidence, typically where high-quality data from randomized controlled trials do not exist regarding the suitability of certain patients for treatment with IV alteplase. 10
In order to understand the variation in treatment rates, 2 the lack of expert consensus on several treatment exclusion criteria, 11 and on-going debates regarding the efficacy of IV alteplase,12,13 a research method is required that reflects decision-making in practice. 14 A discrete choice experiment (DCE) facilitates the investigation of multiple factors in a decision and is therefore appropriate for exploring this complex decision. This method enables the nuances of decision-making to be understood by providing insights not easily captured using more traditional research methods, such as interviews or observation. DCEs have been increasingly adopted to examine healthcare decision-making, including stroke rehabilitation. 15 Through a novel DCE approach, this study aimed to elucidate the factors influencing and contributing to variation in clinicians’ decision-making about treating patients with acute ischemic stroke with IV alteplase, with a focus on areas of clinical uncertainty and borderline cases.
Methods
Study design
The DCE development process consisted of five iterative stages, informed by current good practice recommendations.16–18 Through expert design and pilot testing,
19
hypothetical patient vignettes mimicked the clinical decision and required a binary response (offer IV alteplase or not). Supplementary Tables 1 and 2 describe factors and levels included in the study and their accompanying definitions. Optional free text boxes were included after each vignette for participants to comment on their decision-making, assisting with interpretation of findings (further design information and qualitative results methods can be found online as Supplementary material). A blocked design allowed a subset of vignettes to be presented to each participant to avoid overburdening participants (Figure 1).
Sample patient vignette.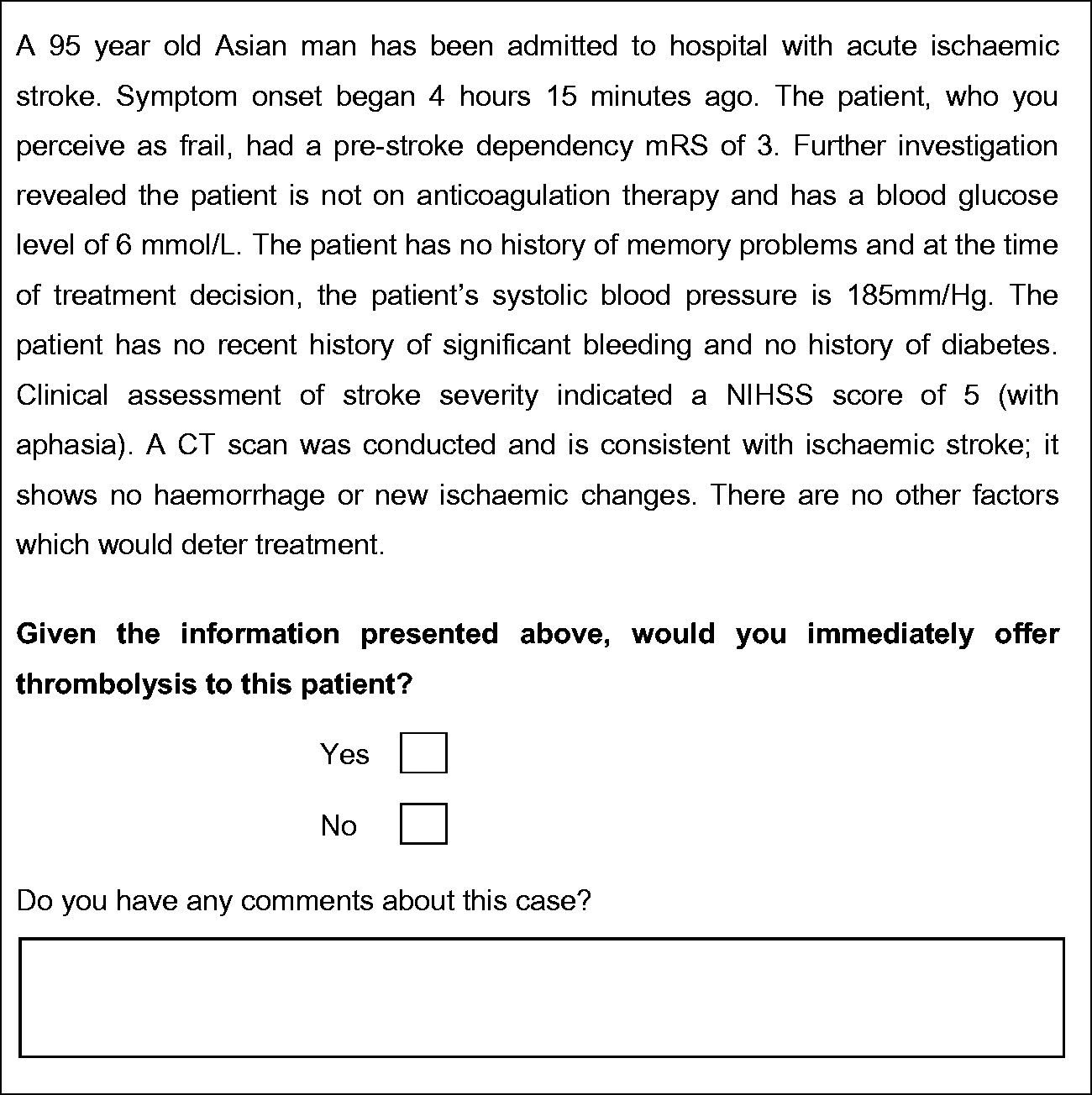
An online survey also included questions and measurement scales to collect information on clinician characteristics that were hypothesized to influence decision-making, including demography and level of experience. A scale was developed to gauge the institutional culture with respect to thrombolysis (“Institutional Culture Scale,” see Supplementary Table 3). The risk-taking sub-scale of the Jackson Personality Inventory (JPI) 20 and the Physician Reaction to Uncertainty Scale 21 were also employed.
Clinicians were asked to state how recent their last thrombolysis decision was, and how many stroke patients they had treated with IV alteplase and how many were harmed as a result, in the past 12 months. Six-point Likert scales were used to assess the impact of clinicians’ level of comfort treating a patient outside the licensing criteria and their views on the strength of the evidence base.
Ethical approval was obtained from Newcastle University Research Ethics Committee (reference: 00720/2013).
Recruitment
UK clinicians who were involved in decision-making regarding the offer of IV alteplase for patients with acute ischemic stroke were recruited via newsletters and emails sent through relevant professional associations, including the British Association of Stroke Physicians, Society for Acute Medicine, College of Emergency Medicine, British Geriatrics Society, and Association of British Neurologists. An invitation to participate was also sent to UK Safe Implementation of Treatments in Stroke (SITS) coordinators and information about the study was included on the Sentinel Stroke National Audit Programme (SSNAP) website. A screening question was first provided to participants ensuring they were involved in the “final decision-making” about thrombolysis. The survey was live for six months from September 2014.
Statistical analysis
Data were analyzed in STATA IC13. 22 Mixed logit regression (mixlogit) analyses were conducted to facilitate the examination of heterogeneity amongst respondents. The intercept (alternative specific constant; ASC) and model parameters were assumed to be random and normally distributed. A positive coefficient for a level of a factor in the mixlogit models, compared with the reference level of the factor, represents a driver of a decision to offer treatment with IV alteplase, whereas a negative coefficient represents an inhibiting influence on decisions to offer this treatment (i.e. more likely not to offer treatment). Significance was set at a P-value of <0.05, and the odds ratios (95% confidence intervals) were calculated to show magnitude/precision of effects in the regression models: patient-related factors (model 1) and both patient and clinician-related factors (model 2). Implausible combinations (e.g. pre-stroke dependency of mRS 1 and severe dementia) were omitted from the regression models. In addition, to control for the effects of block design, seven dummy variables were included in the analyses (comparing each design block to block 1).
Results
Sample characteristics
Characteristics of sample (N = 138)

Reliability analyses were conducted on the scales employed in the survey and showed good to high reliability across scales (Supplementary material).
There was overall general preference not to offer IV alteplase to patients described in the hypothetical vignettes, with 1103 decisions (68.6%) not to offer treatment with IV alteplase compared to 504 decisions to offer the treatment (31.4%).
DCE regression results
Model 1 – Patient-related factors (Supplementary Table 4)
Compared to their reference categories (in brackets), four patient factors were statistically significant predictors of decisions not to offer treatment with IV alteplase: patient age of 95 [68]; time since stroke symptom onset 4 h 15 min [50 min]; patients with severe dementia [no history of memory problems]; and systolic blood pressure (SBP) of 200 mm/Hg [140 mm/Hg].
There were eight statistically significant predictors of decisions to offer (compared to reference levels in brackets): patient age of 85 years [68]; Afro-Caribbean ethnicity [white]; time since stroke symptom onset of 2 h 30 min [50 min]; pre-stroke dependency score of mRS 3 [mRS 4]; and SBP of 185 mm/Hg [140 mm/Hg]. Compared with the stroke severity reference category of the National Institutes of Health Stroke Scale 25 (NIHSS) score of 2 without aphasia, respondents were significantly more likely to offer thrombolysis to patients with scores of NIHSS 5 without aphasia, NIHSS 14 and NIHSS 23.
The standard deviation for the ASC was statistically significant suggesting considerable heterogeneity among respondents in decision-making. There was also substantial heterogeneity on several of the random effects coefficients, with nine standard deviations significant, indicating the variation between participants in their IV alteplase decisions as a function of differing levels of patient-related factors.
Model 2 – Patient-related and clinician factors (Supplementary Table 5)
Model 2 added seven clinician characteristics to the patient-related factors: respondents’ perception of the effectiveness and safety of treating acute ischemic stroke patients with IV alteplase; physician reaction to uncertainty scale; clinicians’ attitude towards risk; estimated number of patients harmed by IV alteplase in the past 12 months and days since a patient was harmed; estimated number of patients treated with IV alteplase in the past 12 months; and comfort treating patients outside licensing criteria.
The standard deviation for the ASC for Model 2 was also statistically significant, which indicates the presence of considerable heterogeneity among respondents regarding their decisions about treating patients with IV alteplase. There was considerable heterogeneity for the random effects coefficients (i.e. the levels of patient factors), with the standard deviations of 17 factor levels emerging as statistically significant. All the statistically significant patient factor predictors from Model 1 remained significant in Model 2, but two additional patient factors became statistically significant predictors of decisions to offer treatment with IV alteplase: moderate dementia; and NIHSS 5 with aphasia.
Respondents’ were significantly more likely to offer treatment of IV alteplase when they perceived the evidence base for this treatment to be robust; had treated a high number of patients in the past 12 months; and reported a higher level of discomfort with uncertainty. Clinicians who reported being comfortable treating patients outside the licensing criteria were significantly less likely to offer thrombolysis.
Comparison of the Akaike and Bayesian information criteria established that Model 2 was a better fit for these data than Model 1.
The predicted probabilities of offering IV alteplase for patients with acute ischemic stroke based on Model 1 are presented in Supplementary Table 6.
Discussion
This is the first DCE to explore patient and clinician factors that influence the decision to offer IV alteplase (thrombolysis) to treat patients with acute ischemic stroke, with a particular focus on areas of uncertainty and borderline cases. For the vignettes included in this study, analysis revealed an aggregate level preference not to offer this treatment, which was expected given that the vignettes were designed to explore decisions related to the “gray” areas of the licensing and evidence base for treatment.
Levels of seven different patient-related factors (patient age, patient ethnicity, stroke symptom onset time, pre-stroke dependency, systolic blood pressure, stroke severity [NIHSS] 25 ; and pre-stroke cognitive status) and four different clinician-related “psychosocial” factors (perception of the evidence for the effectiveness and safety of IV alteplase, number of patients treated in the past 12 months, comfort with uncertainty, and comfort with treating patients outside the licensing criteria) were significant predictors of the treatment decision.
Patients aged 95 were significantly less likely to be offered treatment compared with patients aged 68. However, respondents were significantly more likely to treat 85 year olds compared with patients aged 68. The benefits of thrombolysis for older patients in terms of reduction in disability are at least as great as younger patients, despite an increased risk of symptomatic intracranial hemorrhage. This may also reflect the acceptance of a high profile clinical trial and case–control study data that reports benefit for patients aged >80, in particular for those with onset to treatment time of <3 h.3,4 It is feasible that a social desirability effect explains this latter finding; respondents may be over-compensating (pro-actively recommending a positive decision) to avoid denying treatment based on age. It appears that clinicians are not disinclined to treat older patients, but less likely to treat the very old (∼95). This may reflect the upper limit of data from IST-3 or clinical experience (there are few patients who have been treated in this age range in routine practice). SITS data indicate that only approximately 10% of treated patients were older than 80 26 and national audit data suggest that only 2.5% of the total number of patients who received IV alteplase between April 2010 and November 2011 were older than 90 years. 27
Consistent with evidence of increased benefit with earlier treatment, 4 we identified a statistically significant decreased likelihood of offering treatment to patients who could be treated at 4 h 15 min compared to 50 min from symptom onset. However, clinicians were significantly more likely to treat patients at 2 h 30 min relative to 50 min. This unexpected finding suggests that some clinicians rarely see patients this soon after onset or that clinicians might observe cases presenting early for a short while, particularly if there are factors which create high uncertainty; for instance in mild stroke, when a patient’s symptoms are rapidly improving, to see if symptoms may resolve (per licensing guidelines 7 ), or to give blood pressure time to stabilize or to take more readings before making a final decision.28,29 This is in contrast to research which confirms that earlier treatment is associated with substantially more favorable outcomes, 9 particularly when treatment occurs within the “golden hour” (<60 min from symptom onset). 29
Respondents were significantly more likely to offer IV alteplase to patients with moderate or severe stroke and not offer IV alteplase to patients with mild stroke. These findings are likely to reflect the lack of data and/or uncertainty around the risk/benefit ratio of treatment of minor stroke and the otherwise poor outcomes for untreated patients with severe strokes. There was significant heterogeneity among respondents on the influence of NIHSS 2 with aphasia and NIHSS 5 without aphasia, implying that clinicians differ in their thresholds for treatment of minor stroke and may consider the gains in quality of life for individual patients with isolated language deficits differently.
Compared to white patients, Afro-Caribbean patients were significantly more likely to be offered treatment, though there was no effect for Asian ethnicity. The explanation for this finding is unclear.
Patients with pre-stroke dependency of mRS 3 were more likely to be offered treatment than those with mRS 4. We would have expected that respondents would be more willing to treat patients with mRS 1 compared to mRS 4, but this did not emerge. However, the failure of this to reach significance may be due to an imbalance between the levels of pre-stroke dependency across vignettes in the study, where mRS 1 vignettes were significantly underrepresented.
Patients presenting with severe dementia were significantly less likely to be offered IV alteplase in Models 1 and 2, although in Model 2, clinicians were more likely to offer treatment to those with moderate dementia (compared to patients with no memory problems). This is difficult to explain but may be due to an attempt to preserve a patients’ independence when there is already a low probability that this might be retained. Inspection of the standard deviations reveals significant variation between respondents on the influence of both moderate and severe dementia on decision-making. This may show that clinicians are weighing up the pros and cons of treatment with reference to individual patient characteristics that are not part of the licensing criteria, although it may also reflect perceptions that dementia reduces likelihood of clinical benefit or is associated with an increased risk of adverse effects. However, current evidence suggests there is no increased risk of adverse effects from IV alteplase in patients with dementia. 30
Four of the seven clinician factors emerged as significant. There was a significant association found between the respondents’ perception of the evidence base and the offer of treatment with IV alteplase. Greater discomfort with uncertainty was associated with increased likelihood of offering IV alteplase. This may indicate a preference for action over inaction in instances of high uncertainty, or what may be termed commission bias when observed consistently. 31 Commission bias is defined as the tendency towards action/intervention rather than inaction. 31 Given the high scores observed on the Institutional Culture Scale in the study (indicating a strong culture of administering IV alteplase to patients with acute ischemic stroke in respondents’ institutions), clinicians may worry more about decisions not to treat and, therefore, those with higher levels of discomfort with uncertainty may be more willing to provide this treatment, if it is perceived as the dominant or favored position among colleagues. The results also indicated that clinicians who reported being more comfortable treating patients outside the licensing criteria were less likely to offer treatment in the current study; we do not have an explanation for this finding.
Finally, there was a significant positive association between clinicians’ experience of administering IV alteplase and the likelihood of offering the treatment in the current study. This may indicate that familiarity with administration of the treatment (and positive outcomes) increases the likelihood of future use and has important practical implications for how clinicians are supported when they begin involvement in decision-making. 32 Alternatively, it may simply represent that those more likely to offer treatment in the DCE are more likely to offer treatment in practice, and therefore have higher reported treatment rates.
A key strength of this study was our ability to account for both observed heterogeneity among respondents (via inclusion of clinician factors in the model) as well as unobserved variation (via the estimation of random parameters for the alternative specific constant and factor levels) using the mixed logit regression. Our research offers an important contribution towards a deeper understanding of the factors influencing the decision to offer IV alteplase to patients, in particular factors that influence decisions for patients who fall within the licensing criteria “gray” zone. However, a limitation of the study was the potential for response bias, given we cannot be certain about the absolute number of eligible clinicians who received the invitation to participate.
There were a number of results in this study that were unexpected, for example, respondents were more likely to offer IV alteplase to patients presenting with a stroke onset time of 2 h 30 min compared to 50 min. We do not have clear explanations for these findings without undertaking additional data collection. There are at least three issues to consider:
Technical: as a reflection of the degree of clinical uncertainty being examined by the vignettes, the responses did not contain enough positive responses for some factor levels to fully explore interactions between different factors/levels. A larger cohort or number of vignettes would have enabled greater certainty about the dependency between different factor levels and factors. A replication of the current study using a broader range of factor levels (e.g. for pre-stroke dependency) and including vignettes, where there is likely to be clear consensus about whether or not to offer IV alteplase would help to clarify the results observed in this study. Overcorrection: Respondents may have used their responses to emphasize a particular point which had been recently highlighted by clinical or research developments (e.g. evidence to support treatment of patients >80 years old), or to avoid a perception of bias against certain demographic groups. Diagnostic uncertainty: The decision to treat patients with IV alteplase involves a high degree of confidence that ischemic stroke is the cause of the acute symptoms. Despite assurance that only patients with acute ischemic stroke were being described in the vignettes, respondents may have been influenced by their clinical experience with stroke mimics. For instance, this may explain the apparent greater enthusiasm to treat at 2 h 30 min rather than 50 min, as respondents may have been concerned that the former could resolve and be a transient ischemic attack (TIA) rather than stroke. This may be a training issue which should be addressed.
Training for the assessment and treatment of patients with acute ischemic stroke should address the impact of the influence of clinician factors on decision-making, impart cognitive de-biasing strategies to optimize and support decision-making, and should ensure clinicians develop practical learning and self-efficacy in the administration of IV alteplase to eligible patients early in training to maximize appropriate treatment utilization. The use of patient vignettes as choice scenarios which focus on the “gray” areas in decision-making are useful in generating discussion and revealing differences in individual-level clinical decision-making. Future DCEs could feed back information to participants about their decision-making relative to other experienced colleagues, and inform reflective practice and professional development. High-quality clinical studies are also required to inform “gray areas” of decision-making and address current gaps in the evidence base; in particular, those patient factors (e.g. moderate and severe dementia) which resulted in significant heterogeneity in decision-making among participants in the current study. Future research could apply this method to make between-country comparisons of IV alteplase decision-making and should investigate additional factors beyond those included in this study. National stroke audit programs should consider including additional patient variables, such as pre-stroke cognitive status, in data collection strategies, as this could further illuminate variances in decision-making about the offer of IV alteplase.
Footnotes
Acknowledgments
We would like to express our sincere thanks to Jan Fuller for her excellent administrative support. We are also grateful to the members of the project advisory group for their constructive advice throughout the study development process. The views and opinions expressed herein are those of the authors and are not necessarily those of the HS&DR Programme, NIHR, NHS or the Department of Health. The NIHR had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Authors’ contribution
ADB, RGT, GAF, DF, LT, EL, HR, MR and CP were involved in study design, interpretation of results and drafting of this manuscript. SS and JT were involved in critique of the project, interpretation of results, and drafting of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DF, GAF, HR, and RGT have been involved in the development of COMPASS, a decision aid to support thrombolysis decision making and risk communication, which may be made commercially available, including covering the costs of technical maintenance and updating of the information content. HR is President of the British Association of Stroke Physicians and a member of the Intercollegiate Stroke Working Party. GAF's previous institution has received research grants from Boehringer Ingelheim (manufacturer of alteplase), and honoraria from Lundbeck for stroke-related activities. GAF has also received personal remuneration for educational and advisory work from Boehringer Ingelheim and Lundbeck. GAF is supported by an NIHR Senior Investigator award. ADB, LT, MR, SS, JT and EL, have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Health Research Health Services and Delivery Research Programme (12/5001/45).
Disclaimer
This report presents independent research commissioned by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the Health Services & Delivery Research programme or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.