
Abstract
Qualitative researchers working with trauma-exposed populations face predictable emotional risks, yet higher education policy frameworks rarely address researcher well-being as an institutional responsibility. This article introduces empathic strain—the cumulative impact of sustained engagement with distressing narratives without structured organizational care—as a critical but under-recognized occupational hazard in academia. Drawing on 4 workshops with 34 postgraduate students and interviews with 17 experienced trauma researchers, the study develops a three-phase, trauma-informed model for embedding emotional risk management into research governance. The framework spans planning/grounding; engagement/regulation; integration/reconnection phase combining individual strategies with systemic measures such as mandatory trauma-awareness training, integration of well-being assessments into ethics review, structured debriefing protocols, and access to trauma-informed counseling. Findings reveal that the prevailing reliance on individual resilience discourses perpetuates burnout, disengagement, and attrition, while institutional silence constitutes a form of structural neglect. The proposed model reframes researcher care as a core ethical and policy obligation, aligning with occupational safety principles and advancing debates on academic labor, ethics, and sustainability. By positioning emotional well-being as integral to research integrity, this article offers higher education institutions a scalable, governance-aligned pathway to creating ethically robust, humane, and sustainable research cultures.
Keywords
Introduction
For years, my work as an ethnographer has immersed me in the narratives of violence survivors and their experiences of war rape, forced displacement, and generational trauma. While I was aware of the risks of secondary trauma, I—like many in my field—assumed that professional awareness alone would be sufficient protection. It was not. Over time, the cumulative exposure to such emotionally charged narratives led to exhaustion, detachment, and a persistent sense of disconnection. This personal experience, echoed in the accounts of many academic collegues and students, became the impetus for the several engagements: I undertook specialized training to complement the traditional methods of ethnographic research with trauma-informed principles, and soon after began facilitating research ethics workshops for graduate students and colleagues, preparing for emotionally demanding research.
Based on this initial motivation, I conducted empirical inquiry that enabled me to draft and pilot a model for trauma-informed researcher care, which is presented in the scope of this paper. As a hybrid conceptual–empirical contribution, it is grounded in an interdisciplinary literature review, supported by the insights from interviews with experienced researchers and workshops with postgraduate students, and informed by my own research practice over the last decade. Built upon my past trainings, consulting practice, and initiatives I have facilitated, and inspired by other conceptual frameworks such as the one proposed by Kumar and Cavallaro (2018), the model introduced in this paper integrates interventions on both individual and institutional levels, and is structured around three phases of dealing with potential trauma impact: planning/grounding; engagement/regulation; integration/reconnection.
The following sections present a trauma-informed framework for supporting researcher well-being, drawing on three sources: (1) the existing literature on trauma exposure in non-clinical research; (2) qualitative data from interactive workshops and semi-structured interviews; and (3) critical reflections shaped by my own long-term engagement with trauma-sensitive research.
Central to this study is the concept of empathic strain: a gradual, cumulative emotional toll that emerges not necessarily from direct trauma or single exposure during witnessing, but from prolonged engagement with others’ suffering in the absence of structured institutional care. While secondary trauma and vicarious trauma have been widely used to describe the psychological impact of witnessing or absorbing others’ trauma, these terms originate primarily from clinical, caregiving, and therapeutic contexts, and typically imply a diagnostic or clinical condition with symptoms that may mirror those of post-traumatic stress disorder (PTSD). In contrast, empathic strain is a more flexible and context-sensitive term that better captures the particular experience researchers have with the narratives and research participants they engage with. With this term, I aim to avoid pathologizing the researcher’s experience, and instead emphasizing the relational and emotional labor involved in bearing witness, building trust, and holding space for research participants. With this, I want to focus on researcher wellbeing not solely a matter of individual resilience but a reflection of institutional design: when universities and funding bodies externalize responsibility for emotional labor, they reproduce structural neglect. The proposed Holistic Care Model is intended as potential institutional framework to deal with emphatic strain on personal but mostly on institutional level.
Impact of trauma and well-being in emotionally demanding research
Over the past two decades, the psychological risks of emotionally demanding research have become increasingly visible in academic research across disciplines such as anthropology, oral history, and ethnography (Liamputtong, 2007; Taylor, 2019; Vincett, 2018; Winfield, 2022). Scholars conducting research in contexts where individuals live with the experience of collective trauma or where communities are routinely exposed to violence, loss, and systemic injustice, yet despite their emotional proximity to such stories, they remain largely unsupported by institutional structures, often relying on informal peer support or personal resilience strategies (Berger, 2021; Moncur, 2013; Reyes-Foster and Lester, 2019). While caregiving professions such as social work and clinical psychology have developed trauma-informed approaches to mitigate emotional burnout and secondary trauma (Badger et al 2008; Bride, 2004; Cunningham, 2003; Coetzee and Laschinger, 2018), researchers in social sciences and humanities are often left without equivalent safeguards. The dominant narrative still frames self-care as a personal responsibility (Al-Najdi et al., 2025; McAuliffe et al., 2022) rather than a shared ethical commitment. In the previous literature, scholars have identified and explain the landscape of trauma impact on researchers under diverse definitions and key terms:
- Secondary traumatic stress (C. Branson and Bixby Radu, 2018; Figley, 1995), describing the emergence of PTSD-like symptoms (e.g. hypervigilance, sleep disturbance, avoidance) following indirect exposure to trauma through interviews or testimonies;
- Vicarious trauma (Pearlman and Saakvitne, 1995), when a deeper, long-term shift in the researcher’s worldview is recorded, often involving also disrupted assumptions about safety, trust, and justice;
- Burnout (Maslach and Leiter, 2016) for emotional exhaustion and decreased professional efficacy caused by chronic overwork or unprocessed stress;
- Empathic strain (Rager, 2005; TEMPO, 2021) as a gradually accumulating emotional toll marked by fatigue, detachment, and erosion of compassion, especially in contexts lacking institutional support.
From individual coping to institutional ethics of care
While the before mentioned terms differ in defining their source of stress, temporal pattern, psychological manifestation, and institutional context or support, their application often overlaps in practice, and they are sometimes used interchangeably. However, in this text, I deliberately move away from the commonly used terms to avoid reinforcing a pathologizing or medicalized understanding of researchers’ emotional experiences as individual only (Tend, 2023). The application of empathic strain as here is organizational: the cumulative emotional exhaustion and reflexive disturbance that arise from sustained empathic engagement with others’ suffering during and due to the job/professional assignment. Unlike the broader notion of ‘emotional toll’, which can equally include frustration, fatigue, or stress, empathic strain specifically denotes the relational dimension of emotional distress: it emerges when researchers identify with participants’ pain and absorb fragments of their affective experience. The term thus captures the porous boundary between witnessing and internalizing trauma, without pathologising the researcher’s response through clinical labels such as PTSD or secondary trauma. Empathic strain is most likely to occur under conditions of prolonged exposure to narratives of violence or suffering; when empathy is heightened by shared identities or moral resonance between researcher and participant; and especially when (or because) institutional containment structures (supervision, debriefing, peer dialog) are absent. It may also emerge belatedly, during data analysis or teaching, when the emotional residue of encounters resurfaces in reflective work. Although empathic strain emerges from shared exposure to human suffering, its intensity and meaning are shaped by researchers’ own positionality, related to their race, gender, class, nationality, age, and migration status, for instance. Researchers who share structural vulnerabilities with participants may experience amplified emotional resonance and diminished institutional protection (Nuttman-Shwartz, 2016); conversely, those perceived as privileged outsiders may confront guilt, moral conflict, or resistance. Institutions themselves are not neutral in this process: their bureaucratic, financial, and cultural structures often protect some bodies and identities more effectively than others. Access to counseling, supervisory care, or workload adjustments may depend on contract type, citizenship status, or departmental culture, leaving contingent, racialized, or migrant scholars disproportionately exposed. Any institutional framework must recognize that researchers’ wellbeing is situated rather than universal (Hummel and El Kurd, 2023) and that the established asymmetries should not prevent ensuring protective mechanisms also for those most structurally vulnerable within the academic system.
Empathy remains a double-edged quality in qualitative research: it is a condition for ethical listening and trust-building, yet it also dissolves protective distance. Empathic strain, therefore, is not a failure of professionalism but a by-product of ethical attunement. Recognizing this paradox reinforces the need for collective and institutional frameworks of care rather than individual self-blame. The Holistic Care Model reconceptualizes empathy management as a collective ethical responsibility. It links individual affect to institutional culture through three interdependent levels of care (personal, peer, and structural), each requiring different forms of recognition, resource allocation, and accountability.
The model presented here engages with critiques of wellness discourse in academia, where self-care is presented as a personal solution to structural neglect (Mattheis, 2025; Pearce, 2020). As Miller (2022) and Pakenham (2015) have argued, true resilience emerges not from individualized wellness routines alone, but from shared responsibility, trauma-informed systems, and value-consistent care embedded within institutional culture. A trauma-informed research model must therefore go beyond offering tools for individual coping; it must interrogate the very conditions that make such tools necessary in the first place. Despite growing awareness, institutional responses remain inconsistent. While isolated programs or workshops on emotional safety do exist, they are rarely integrated into research ethics protocols, mentorship training, or data collection preparation (van der Merwe and Hunt, 2019). This disjuncture reinforces the assumption that emotional risk is a matter of personal vulnerability rather than a legitimate professional concern. As a result, most of the researchers start to address their well-being needs only when the burnout, disengagement, or even withdrawal from the data collecting process become undeniable in disrupting research process and/or daily life activities. As institutions do not acknowledge the structural nature of poorly addressed care and wellness demands among researchers, but rather frame such challenges within ‘personal responsibility related to individual choices in research, as well as campaigns individualizing mental health and well-being’ (p. 6), this article argues for a shift from reactive, individualized wellness rhetoric, to proactive, trauma-informed institutional responsibility. The following sections introduce the methodology used to develop and refine the model, and examine how both early-career and experienced researchers navigate and reflect on the emotional toll of trauma-exposed research.
Methodology: Multimodal approach and ethical foundations
Study design and timeline
This study employed a multimodal qualitative design to explore how researchers experience and manage the emotional toll of emotionally demanding work. The study was conducted between February and October 2023 and was approved by an Institutional Review Board (UPF, CIREP Ethics Compliance Certificate, no.281). A Data Protection Impact Assessment (DPIA) was also completed to ensure confidentiality and ethical handling of participant data (Liamputtong, 2007).
Participants and sampling
The research was conducted with two groups of participants. The first group consisted of 34 postgraduate students enrolled in a professional social work program, preparing for data collection in high-risk environments (e.g. refugee shelters, substance abuse centers). Of these, 29 identified as women and 5 as men, ranging in age from 22 to 35. All contributed their input on the topic during a combined workshop and focus group process.
The second group comprised 17 experienced researchers from various disciplines who had previously conducted trauma-related qualitative research. This group included 11 women and 6 men, aged 33–61, from disciplines such as anthropology (7), oral history (4), social psychology (2), sociology (2), and ethnography (2). Their research focused on contexts involving political violence, genocide, forced displacement, and gender-based trauma. While most were based in central Western Europe, several had conducted fieldwork in Latin America, the Balkans, and the Middle East. All participants were selected through purposive sampling (Bernard, 2002; Creswell and Plano, 2011) based on their ability to critically reflect on emotional challenges in research. All participants received detailed information about the study and signed informed consent forms, which were translated into their native languages when applicable.
Workshop design with postgraduate students
Four 3-hour workshops were facilitated by the author at a private college in a central European country, between March and May 2023. These sessions introduced trauma-informed principles, emotional risk awareness, and adaptive self-care strategies tailored to qualitative research. Students were encouraged to share anticipated emotional challenges in their upcoming fieldwork and to critically evaluate the preparatory tools provided by the facilitator. These tools included excerpts from existing trauma-informed care frameworks used in humanitarian training, modified worksheets from Kumar and Cavallaro’s (2018) self-care planning model, and custom reflection prompts developed by the author based on prior ethics teaching. The workshop sessions were audio-recorded (with consent), and detailed field notes were taken by a co-facilitator. Students completed anonymous reflective questionnaires at the end of each session, commenting on which strategies felt useful, irrelevant, or burdensome. Their feedback informed iterative refinements to the trauma-informed care model presented in this paper.
Interviews with experienced researchers
Seventeen researchers participated in one-on-one, 70–90 minute-long interviews conducted by the author between June and August 2023. The interviews were semi-structured and guided by a protocol that included questions about prior field research experiences, emotional risk management, support systems, and reflections on institutional responses (Spradley, 1979). Participants were also introduced to a pilot version of the trauma-informed model and invited to reflect on its relevance, feasibility, and potential gaps. While the model was not implemented in a formal longitudinal study, several participants described applying aspects of it retrospectively to their past research or integrating the proposed strategies into their current supervisory roles. Their reflections informed the language, structure, and practical recommendations of the revised model.
Data analysis
All transcripts were anonymized and thematically coded using a hybrid deductive-inductive framework. Preliminary codes were drawn from literature on secondary trauma, self-care, and researcher well-being (e.g. Figley, 1995; Kumar and Cavallaro, 2018; Pearlman and Saakvitne, 1995), while emergent codes were developed iteratively through review of transcripts and field notes. Themes included anticipatory anxiety, emotional disconnection, institutional silence, self-blame, peer validation, and resilience practices. Coding was cross-checked by a research assistant familiar with qualitative trauma research to strengthen inter-rater reliability.
Limitations
This study relied on retrospective reflections from experienced researchers and anticipatory reflections from students. No direct measurement of psychological impact was conducted, and the model’s effects remain exploratory rather than empirically tested. Participant self-selection may also have favored individuals who were more attuned to emotional risk or who held strong opinions about institutional support. However, the depth and consistency of responses across participants suggest shared patterns that merit institutional consideration (Guest et al., 2006). This study does not claim generalizability, but rather aims to identify critical gaps and provide a practical starting point for broader policy and training development.
Results: Iterative care model for researcher well-being
The proposed model draws inspiration from the conceptual framework developed by Kumar and Cavallaro (2018), which served as the foundation during the initial brainstorming sessions. It provided a structured lens to examine the dynamic interplay between a researcher’s emotional responses and the research process, emphasizing their mutual influence. Although the model is presented in three phases for analytical clarity, these should not be understood as sequential or time-bound. Emotional strain fluctuates and may resurface long after data collection concludes. The framework thus functions as a cyclical and iterative care continuum, recognizing that preparation, coping, and recovery overlap and often re-emerge throughout the research process. Central to the new model is the recognition of both institutional and individual responsibilities in fostering researcher well-being, and its organization across three key phases: planning/grounding; engagement/regulation; integration/reconnection. To operationalize these principles, the model was structured into core phases, strategies, and activities designed to guide researchers in mitigating trauma exposure. It was iteratively developed through brainstorming sessions in interactive workshops, where participants collaboratively shaped its form. Beyond its theoretical foundation, the model was also tested in practice: research participants applied its structured phases and strategies in their daily work, systematically following its stages and later reporting back on its efficacy. Their reflections, detailing what proved effective and what required further adaptation, informed the refinement of the model.
In the next section, the specific phases and strategies will be presented in detail, alongside participant feedback on their practical implementation in preparation for the emotionally demanding research. Rather than measuring outcomes, this study captures how researchers evaluated the model’s relevance and shared concrete suggestions for strengthening it (Figure 1).
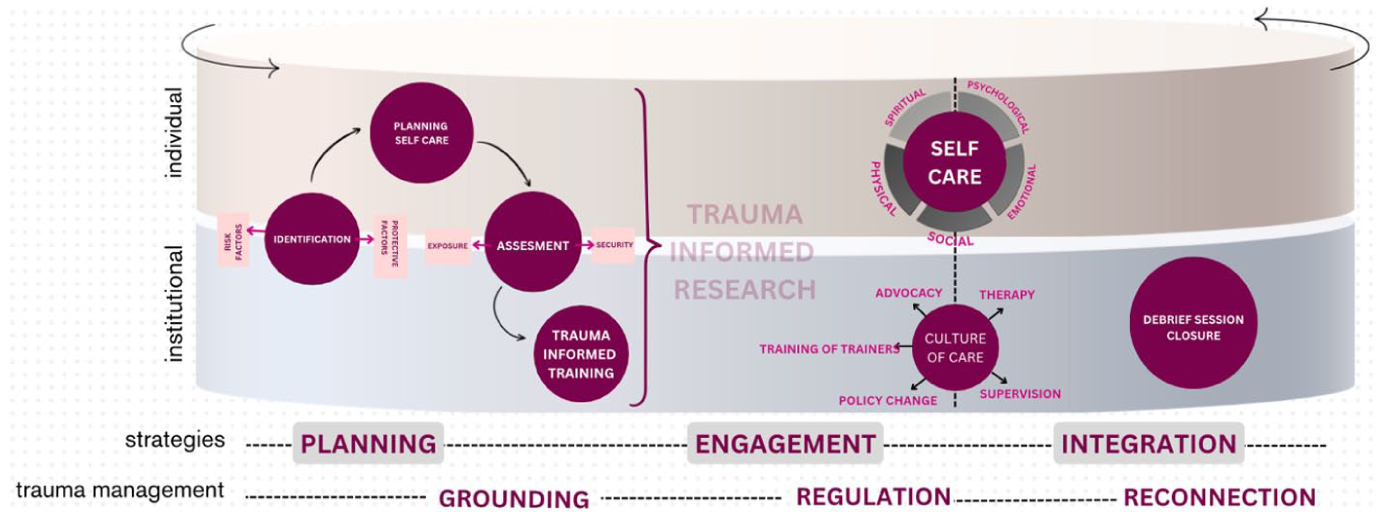
Iterative, circular process of holistic care; strategies before, during and after data collection, on individual and institutional level (see Appendix 1 for the enlarged photo).
Phase 1: Planning/grounding
Participants consistently emphasized the importance of anticipatory emotional preparedness. Already recognizing risk was seen as transformative, allowing them to better understand their vulnerabilities and develop coping strategies: ‘Adopting this model helped me recognize my personal trauma and initiate a healing process that made me feel more at peace during the research process’. (R, student)
Among the 34 students, 27 (79%) reported that prior to the workshops, they had received no formal training on the emotional risks of trauma-sensitive research. Many expressed surprise at how rarely emotional resilience was discussed in their graduate education. One student remarked: ‘We talk about ethical clearance and consent forms, but nobody talks about what to do when you can’t sleep after an interview’. (I, student) Researchers similarly described entering fieldwork unprepared for its emotional toll. An oral historian who had worked in post-conflict contexts shared: ‘I was trained to manage bias and narrative, not grief. I wish someone had warned me how much it stays with you’. (S, researcher). Across interviews, the following strategies before starting data collection emerged as most valuable:
Identification of risk and protective factors
Researchers must identify their emotional thresholds, past experiences, and positionality (gender, age, economic status etc.) before starting data collection. The potential for empathic strain varies across individual and institutional factors. At the individual level, vulnerability increases with prior trauma exposure, deep emotional connection to the research topic, high empathy, or pre-existing mental health conditions such as anxiety, depression, or PTSD. Institutional responses must recognize that exposure risks are unevenly distributed. Early-career, racialized, precariously employed, or migrant researchers often operate without the same safety nets as senior or majority-group colleagues and design equity-based approach: targeted mentoring and counseling for minoritised researchers; inclusive ethics-review panels reflecting demographic diversity; and transparent workload adjustments acknowledging compounded vulnerabilities. Embedding intersectionality within researcher-care governance ensures that wellbeing is not treated as an individual privilege but as an institutional right. Institutions can contribute to risk when they fail to provide trauma-informed training, perpetuate stigma around emotional distress, or lack structured support services, leaving researchers without the necessary resources to manage emotional challenges effectively.
For most researchers (14/17), recognizing risk was transformative, allowing them to better understand their vulnerabilities and develop coping strategies. One participant reflected: ‘Adopting this model helped me recognize my personal trauma and initiate a healing process that made me feel more at peace during the research process’. (L, researcher)
Assessment of exposure and security factors
Sometimes, resources or protocols may exist, but researchers are unaware of them unless they actively seek them out. By conducting a structured assessment, individuals and institutions can identify security and exposure levels not only beforehand, but also during and after data collection, in order to facilitate tailored support strategies. Figure 2 displays collected ideas in assessing administrative assistance, physical safety, and access to resources in order to improve/provide high security level. Those can be defined also by assessing exposure level and nature of the research process (its frequency, extent, and environmental conditions). Qualitative data from both student and senior researcher groups points out how persistent concerns about physical safety directly amplifies emotional distress. A participant working in a politically unstable environment describes how their continuous alertness blurred the boundary between professional vigilance and psychological hypervigilance: ‘I find myself scanning my surroundings, instead of focusing what I am hearing’ (K, researcher). They report how logistical challenges such us unreliable transport and ambiguous permissions trigger bodily tensions such as, for example, headache long before emotional exhaustion sets in. Such anticipatory anxiety therefore depletes their empathic capacity, and makes it harder to deliver quality performance during the interview. Physical insecurity that sustains the body in survival mode, magnifies emphatic strain, that is, preventing the mind from achieving emotional regulation or reflective distance.
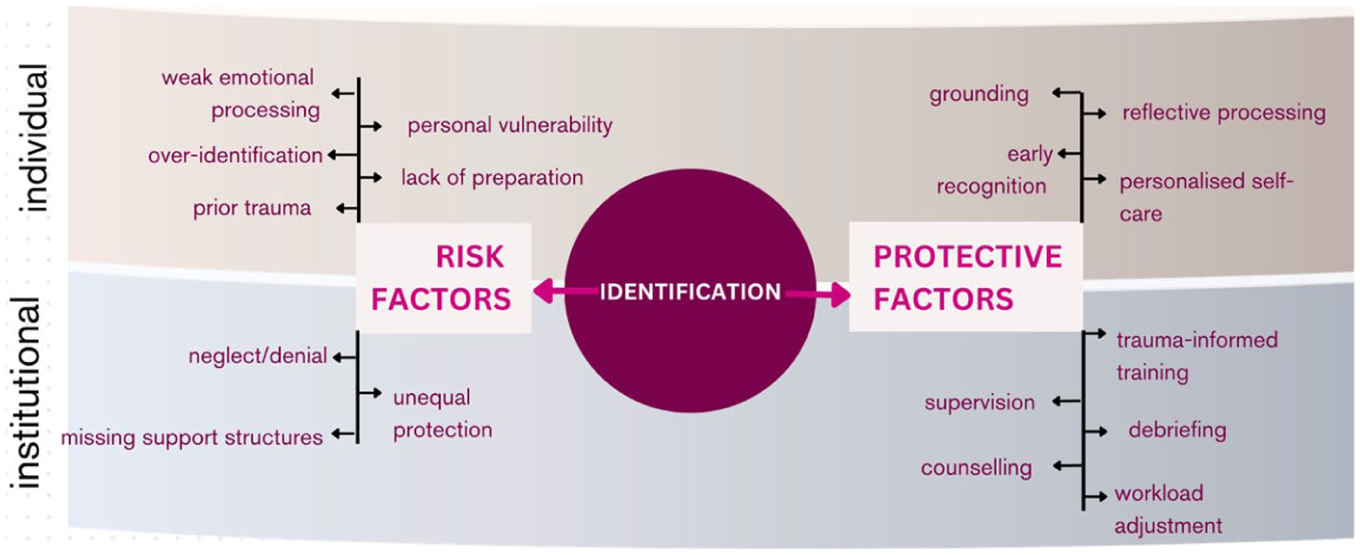
Identification of risk/protective factors on individual/institutional levels, details.
Commitment to self-care
Often, one begins with a list of actions, yet an intentional and ongoing commitment plan emphasizes that self-care is only effective when paired with consistency and adaptability. The commitment list can be proposed individually, and here I present (see Figure 3) seven strategies that outline how to integrate self-care into daily life. These were proposed during group work in the workshop. This section reminds us that self-care is not a one-time action but a practice that must be nurtured with intention. In addition, model focus on the ‘self-care’ and ‘well-being practices’ that directly address exposure-related emotional strain (reflection, supervision, ethical dialog, and institutional scaffolding) rather than general wellness behaviors. This distinction ensures conceptual coherence while acknowledging that general wellbeing contributes indirectly to resilience. In trauma-exposed work (e.g. emotionally demanding research, education, documentation), it is not enough to know what to do; we must also commit to doing it regularly, adapt as circumstances shift, and treat self-care as part of professional ethics, not as a luxury.

Assessment security/exposure factors on individual/institutional level, details.
In the discussion, several researchers emphasized the importance of institutionally promoted training on the impact of trauma prior to any data collection. Such training is essential to equip researchers with the skills to recognize, respond to, and mitigate the effects of working with distressing material or vulnerable populations. This responsibility must be upheld at the institutional level, as it ensures consistent ethical standards, protects the well-being of personnel, and fosters a safer, more supportive environment for both researchers and the communities they engage with. However, one researcher voiced a concern, shared by others in the room, that an overemphasis on trauma risks might discourage students or create anticipatory fear.
‘After the training, I became fixated on potential dangers and how my interlocutors’ trauma might haunt me and my family. But during the interview, I felt crushed—yet afterward, I experienced deep gratitude for my own life, family, and work. I feel focusing only on escaping trauma put me at risk of seeing nothing but trauma’. (A, researcher)
Institutions should operationalize the anticipatory dimension of researcher care through formal preparation and shared accountability mechanisms. Prior to project initiation, departments can introduce risk-assessment templates that include emotional, ethical, and safety dimensions alongside conventional logistical planning. Ethics committees could require a short ‘researcher wellbeing statement’ specifying anticipated affective risks and proposed containment strategies (supervision, peer groups, reflective journaling). Supervisors and principal investigators should be mandated to hold structured ‘pre-exposure briefings’, jointly identifying potential emotional triggers, boundary challenges, and available institutional supports. Funding agencies can allow time and budget for such preparatory work under ‘researcher safety and wellbeing’.
Phase 2: Engagement/regulation
Once data collection process begins, researchers must balance the ethical responsibility of protecting participants with the need to safeguard their own emotional well-being. A trauma-informed approach recognizes that self-care is not separate from ethics, but rather a fundamental aspect of responsible and sustainable research. While empathy is crucial for building trust with participants, it differs from sympathy, which can lead to emotional over-identification and increased vulnerability to empathic strain (Kisling, 2020). In qualitative research, where scholars engage deeply with narratives of suffering, the process is not merely intellectual but also emotional and psychological (Beckett, 2019). Although some assume that an ethical commitment to participant protection is sufficient to shield researchers from distress, evidence suggests otherwise. Researchers with heightened trauma awareness (of both their own experiences and those of their participants) are better equipped to regulate their responses and avoid internalizing suffering (Dickson-Swift et al., 2008; Rager, 2005; van der Merwe and Hunt, 2019). This awareness enables deeper empathy without slipping into over-identification (Jenkins and Baird, 2002; Pearlman and Saakvitne, 1995).
Participants in the workshops agreed that one of the most effective ways to mitigate the psychological toll of trauma exposure is through structured emotional processing. One researcher noted how common it is to carry unresolved emotions from one interview to the next, often unaware of the cumulative emotional burden. Without intentional reflection, this buildup can lead to burnout, compassion fatigue, or secondary trauma. Practices such as journaling, voice memos, or debriefing sessions were mentioned as helpful in identifying early signs of distress and supporting proactive coping. Writing down thoughts immediately after interviews was seen as particularly useful for recognizing emotional patterns and adjusting accordingly. Yet, maintaining a consistent self-care routine proved difficult. While activities like running contributed to general well-being, they did not necessarily help with trauma processing. Others found that an excessive focus on self-care created anxiety: turning it into another obligation rather than a tool for resilience. Despite their best intentions, one post-graduate student, with first time field work experience, mentioned struggling to implement routines and feeling guilty for not adhering to their plans.
‘I made a great plan. But once fieldwork started, balancing research with my personal responsibilities became overwhelming. Instead of helping, my self-care plan just made me feel guilty for not keeping up with it’. (M, student) ‘I had in mind to meditate every morning. But the first morning I opened my phone in bed, and there was an email—I spent 40 minutes answering it. And then I never came back to do this meditation’. (L, student)
One student mentioned feeling ‘obligated’ to engage in socially endorsed self-care routines (such as yoga or meditation) even when those practices did not resonate with them.
‘I tried yoga for weeks because I thought it was what I ‘’should’ do to take care of myself. But I hated every second of it. I realized I was forcing myself into something that didn’t actually help me relax’. (S, student)
Such reflections underscore the importance of personalizing self-care. Training programs should move away from universal checklists and instead emphasize that sustainable self-care must align with individual preferences, values, dynamics, and realities. It also almost necessarily includes self-compassion, that is, extending kindness toward oneself, allowing researchers to what Kristin Neff (2003) calls ‘balanced awareness’, acknowledging distress without over-identifying with it. Unlike conventional self-care frameworks that can become another task to ‘succeed at’, self-compassion offers a non-evaluative stance that softens the pressure to perform wellness. It encourages researchers to honor their emotional limits as a form of integrity, not deficiency. This is particularly important in trauma-exposed work, where researchers often experience guilt: both survivor guilt when returning from the field and guilt when they fail to implement ideal self-care routines (Bistricky et al., 2025). Interventions like Compassion-Focused Therapy (Gilbert, 2009) and Mindful Self-Compassion training (Germer and Neff, 2019) have shown measurable improvements in psychological well-being across diverse professional groups.
Trauma research often involves intimate, vulnerable exchanges. While empathy builds trust, researchers must carefully navigate the line between engagement and emotional over-identification. Participants were generally familiar with grounding techniques, and four reported using deep breathing before and after interviews to reset. Among other small rituals, listening to music, taking a walk, or engaging in light conversation were mentioned as ways to maintain psychological separation between work and personal life. These intentional acts helped prevent emotional overload and preserved a clear distinction between the researcher’s role and their inner world. Still, individual strategies alone are not enough. Early-career researchers in the group (6) reported feeling isolated in managing the emotional weight of their work. Academia’s emphasis on intellectual output often sidelines emotional well-being, making it difficult to speak openly about psychological strain. This silence intensifies distress and hinders recognition of when support is needed. Participants noted the value of peer validation, simply hearing someone say, ‘I’ve felt that too’, helped normalize their emotional responses. Regular peer check-ins, debriefings with supervisors, and informal support networks were described as crucial spaces for collective processing. However, without institutional recognition of the emotional labor embedded in trauma research, the burden of care continues to fall unfairly on individual researchers. Institutions must treat emotional well-being as a core ethical concern and incorporate it into trauma-informed research practices that shape not only how researchers engage with participants, but also how they sustain themselves in emotionally demanding work. During engagement, departments can provide real-time peer supervision groups and Human Resources units and student-support services can maintain on-call counseling hotlines for those conducting fieldwork abroad, ensuring confidential professional support. Research centers might appoint a wellbeing liaison or trauma-informed mentor who coordinates responses to acute distress. Supervisors should receive training in affective supervision so that regular progress meetings include discussion of emotional load as a legitimate research variable.
Phase 3: Integration/reconnection
The impact of trauma exposure often becomes most visible in the post-data collection phase. During the process, researchers are immersed in conducting interviews, analyzing data, and meeting deadlines, usually succeeding to maintain a level of intellectual detachment from the emotional weight of their work. However, as data collection slows and the focus shifts to writing and reflection, previously suppressed emotions begin to surface. Researchers in this study almost collectively agreed that they have experienced feeling unexpectedly drained, struggling with motivation, or experiencing physical symptoms such as sleep disturbances, headaches, and chronic fatigue. Even those who anticipated emotional challenges found that the stories they encountered lingered long after the research was completed. These experiences underscore the need for structured emotional management beyond data collection phase, ensuring that self-care and trauma processing remain integral throughout the research lifecycle.
A key challenge during this phase is distinguishing between normal exhaustion and signs of deeper emotional distress. While fatigue is an expected outcome of intensive work, symptoms such as emotional numbness, heightened anxiety, or detachment from personal relationships may signal secondary trauma or compassion fatigue. One participant described experiencing intrusive thoughts about suffering they were recording; another one struggled to regain a sense of purpose after data collection during the fieldwork, finding it difficult to transition back into daily life. In response, the group proposed structured reflection as an essential strategy. Writing journals or reflective memos helped researchers articulate and externalize their experiences, transforming abstract emotions into something tangible and manageable. One participant found particular value in debriefing sessions, where emotional responses could be acknowledged and validated.
Participants also emphasized the importance of reconnecting with activities that brought joy or a sense of normalcy, such as creative hobbies, spending time outdoors, or engaging in social interactions unrelated to research. Others turned to uplifting content—books, films, or music—as a way to counterbalance the emotional intensity of their work. As in previous stages, frustration over the lack of institutional support persisted in the post-research period. None of the institutions where the participating researchers worked offered structured debriefing sessions or trauma-informed mental health services tailored to those engaging with distressing content. Researchers were left to manage the emotional aftermath on their own. The prevailing academic culture of self-reliance discourages open conversations about emotional strain, reinforcing the perception that acknowledging distress is a sign of weakness.
To address this gap, institutions must recognize the post-research phase as a critical period requiring structured support. Incorporating debriefing sessions into research training, providing access to trauma-informed counseling, and allowing for flexible workloads after emotionally demanding research are essential steps toward fostering researcher well-being. While these changes require a cultural shift within academia, they are foundational to sustaining ethical and humane research practices.
Prioritizing personal well-being can sometimes feel at odds with the needs of participants or the communities being studied. This tension is particularly pronounced in non-Western or humanitarian contexts, where researchers may experience guilt or discomfort when taking time for self-care in the midst of others’ suffering. One participant reflected on this internal conflict: ‘I witnessed so much hardship, and then went back to a hotel with clean sheets and warm food. I couldn’t reconcile that gap—it felt wrong to take care of myself’. (S, researcher)
Balancing researcher well-being with ethical responsibility requires ongoing self-reflection and adaptation. Trauma-informed research must not only incorporate self-care but also critically examine how researchers’ positionality, power, and privilege influence their ethical decision-making. While some researchers found this self-awareness empowering, others felt it deepened their emotional entanglement with participants, making it more difficult to maintain emotional boundaries. However, developing resilience in trauma-sensitive research is not about emotional detachment; rather, it is about learning how to navigate emotional intensity in sustainable and compassionate ways. At an individual level, participants suggested that self-care practices in this final phase should be seen as a continuation of those adopted earlier, though often involving different forms. It became clear, however, that self-care is frequently only taken seriously once symptoms of emotional strain emerge—a pattern that was also observed among members of this very group. However, participants also strongly emphasized the need for institutional involvement. One participant proposed that researchers with prior experience in trauma-sensitive work be included in a pool of future trainers to help guide and support others through training activities proposed in Phase 1. Beyond training, other key recommendations included advocacy, policy reform, therapy, and ongoing supervision.
Importantly, the group agreed that such support mechanisms, necessary to cultivate a supportive research culture, should not be delayed until after exposure to/engagement in emotionally demanding research but initiated before or at the start of the research process. Those currently engaged in therapy collectively stressed that therapy should be recognized as a legitimate and integral part of the research role, not treated as a private or personal investment. As for the institutions in the post-data collecting process, they should formalize debriefing sessions, led by trained facilitators to process residual emotions and ethical dilemmas. Workload and contract policies should recognize emotional labor as part of research effort, allowing for compensatory leave or reduced teaching immediately after demanding projects. Graduate programs could integrate re-entry seminars or reflective writing retreats supporting both intellectual synthesis and emotional integration. Funding bodies might authorize ‘recovery time’ within grants, acknowledging that ethical research includes adequate decompression. Ultimately, a broader policy shift is needed across institutions to acknowledge the significance of emotional well-being and to provide the necessary support structures and services to sustain ethical and responsible research practice.
Guiding principles
To organize the range of responses to empathic strain, the paper distinguishes three interdependent levels of care:
(1) Individual practices that foster emotional regulation and boundary-setting;
(2) Peer and collective practices that sustain community support (e.g. reflective groups, supervision circles); and
(3) Institutional responsibilities that provide structural containment and accountability.
The Holistic Care Model integrates these levels as a continuum rather than a hierarchy, recognizing that personal wellbeing strategies are insufficient without peer infrastructures and institutional recognition.
From individual resilience to institutional accountability
Across both student and experienced researcher cohorts, the findings demonstrate that empathic strain is not an exception but a predictable outcome, particularly in research environments where emotional labor is normalized, self-care is treated as a private concern, and institutional safeguards are absent. This paper advances a holistic prevention model spanning different phases of research (before, during, and after) and calls for a shift from individual coping to institutional responsibility.
Unlike most ethical checklists, which primarily focus on protecting participants’ psychological safety and dignity, often overlooking any toll on researchers themselves (Griffin et al., 2003; Hummel and El Kurd, 2021), the model presented here foregrounds researcher well-being as an equally essential ethical consideration. The proposed Holistic Care Model supports researchers, by integrating both physical and emotional safety, distinguishing it from purely psychological approaches. Through structured preparation, sustained supervision, and post-research recovery, the model emphasizes that researchers’ safety must be understood holistically. Physical insecurity in fragile or conflict-affected settings directly undermines emotional stability, compounding empathic strain and diminishing the quality of ethical judgment. Despite the known risks, participants reported a persistent lack of institutional involvement, including minimal trauma training, inadequate access to mental health services, and the absence of structured debriefing sessions. This gap reflects what Smith and Freyd (2014) term ‘institutional betrayal’—when institutions neglect foreseeable harm to their members while claiming to uphold ethical standards in other areas (Mattheis and Kingdon, 2021). The consequences are both ethical and pragmatic. Emotional strain contributes to burnout, disengagement, diminished productivity, and weakened student supervision. Bassett-Cameron (2023) includes testimonies from researchers affirming that vicarious and secondary trauma have become serious workplace hazards (pp. 11–15). As with other high-risk professions, this highlights the urgent need for research institutions to treat emotional exposure as an occupational hazard, not an individual shortcoming. Well-being must be understood not as ancillary to performance, but as a prerequisite for sustainable professional engagement (Miller, 2022; Pakenham, 2015). One researcher expressed a desire for clearer institutional standards, pointing to occupational safety models from other sectors and underscoring the need for academia to adopt frameworks akin to OSHA. 1
To move from recognition to responsibility, I propose five concrete steps that universities and research institutions can implement:
(1) Mandatory trauma-informed training for researchers working on sensitive or emotionally demanding topics.
(2) Integration of researcher well-being assessments into ethics review protocols, ensuring emotional risks are evaluated alongside participant safety.
(3) Structured emotional debriefing sessions as a standard component of project closure procedures.
(4) Guaranteed access to trauma-informed mental health professionals, available throughout the research process.
(5) Training for supervisors to recognize and respond appropriately to signs of emotional distress among their mentees or team members.
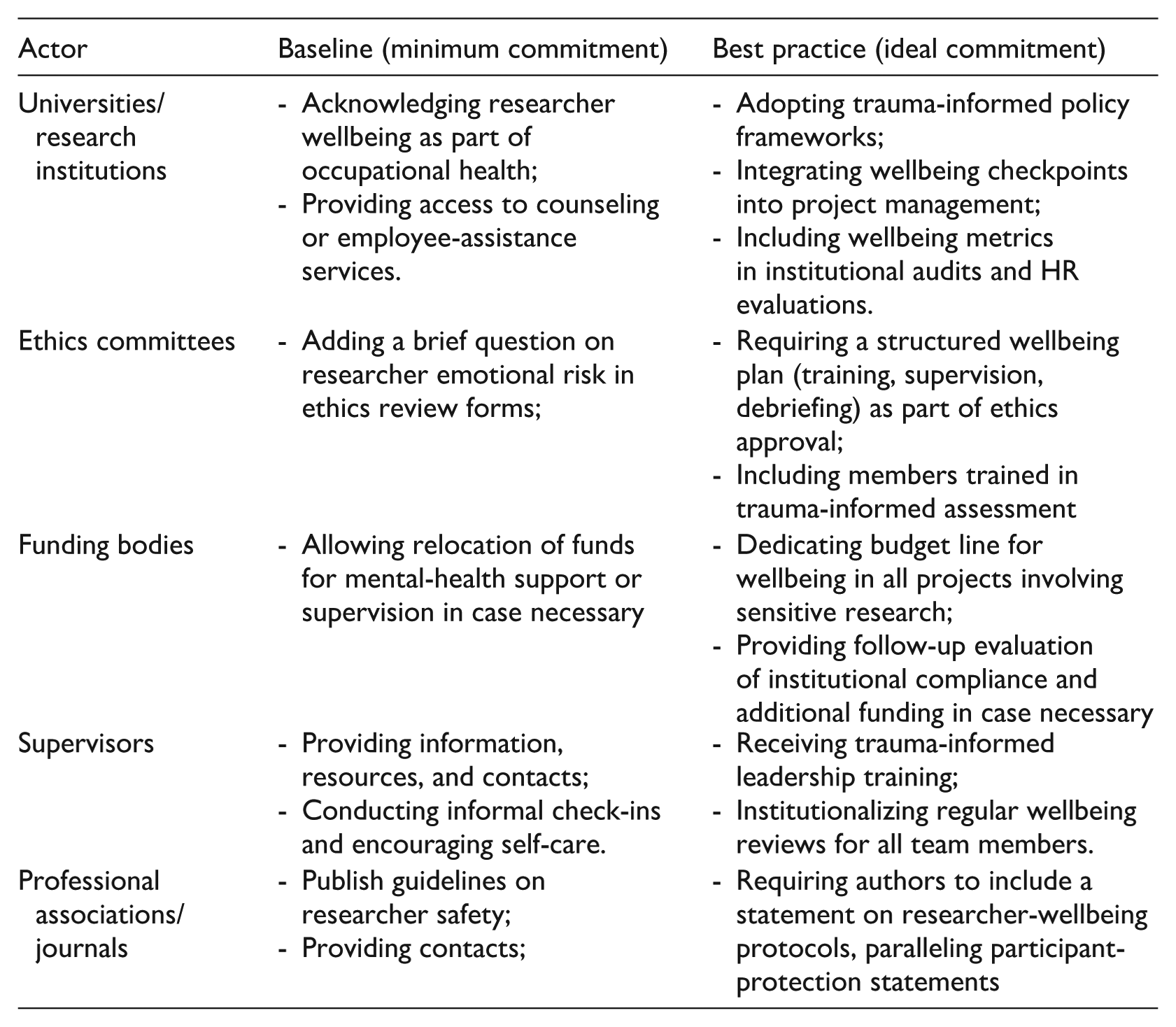
While the preceding recommendations outline broad principles, implementing them requires coordinated action across multiple levels of the research ecosystem. Empathic strain is sustained not only by individual overexposure but by structural fragmentation: when universities, ethics committees, and funding bodies each assume that another actor carries responsibility for researcher wellbeing. The table below specifies complementary responsibilities and minimum versus ideal commitments.
To avoid the self-care discourse that risks placing the burden of emotional regulation on the researcher rather than on institutions, Schulz et al. (2023), drawing on feminist ethics of care, propose relational and collaborative forms of ‘community care’ through collectives, peer networks, and shared reflective spaces. These peer-based communities of care represent an important bridge between individual coping and institutional accountability: they provide informal yet vital infrastructures of emotional support that can sustain researchers when formal structures are absent or inadequate. Within the model proposed here, such peer practices occupy the meso-level of researcher care, complementing individual resilience strategies and institutional responsibilities rather than substituting either.
From empathic strain to empathic gain
While this paper has focused on risk, participants also described empathic gain—a quiet, positive outcome of trauma-sensitive research when adequately supported. Unlike idealized resilience, empathic gain refers to deeper emotional insight, renewed purpose, and personal growth that emerge through care, reflection, and meaningful connection (Goldenberg, 2002). This does not happen by accident. It requires emotional scaffolding: structures, mentorship, and space to metabolize distress into learning. It aligns with concepts from positive psychology (Seligman, 2019), post-traumatic growth (Tedeschi and Calhoun, 1996), and value-consistent self-care (Miller, 2022; Pakenham, 2015), which suggest that confronting trauma need not result in depletion, but can also foster clarity, empathy, and meaning, if the right scaffolding is in place.
Future research and model evaluation
This model offers both a practical tool and a normative proposition. It lays out how institutions can reduce harm, but more importantly, it asserts that these actions are ethical imperatives. Emotional resilience does not grow from isolated self-care: it emerges from cultures that name emotional labor, make space for it, and reject the conflation of professionalism with silence. True resilience, that it can be called also ethical sustainability depends on institutions recognizing that researcher well-being is not a sign of personal fortitude, but a reflection of collective integrity. While this study provides an exploratory foundation rather than a validated intervention, the model’s effectiveness remains to be empirically tested. Future research could therefore build on this work by:
(1) Evaluating the impact of the model when implemented in full (e.g. in graduate programs or fieldwork preparation);
(2) Identifying which components are most protective for different groups (e.g. early-career vs senior researchers).
(3) Examining how institutional policies evolve when emotional labor is formally recognized as an occupational risk.
(4) Investigating how values-based self-care interacts with researcher positionality, privilege, and exposure.
The proposed framework is not confined to conventional notions of ‘the field’. Emotional and moral exposure can occur during online research, analysis of distressing narratives, or work with vulnerable populations in researchers’ own communities. Institutions should therefore adopt trauma-informed policies that recognize these diverse exposure contexts. This requires shifting from a spatial to an affective understanding of fieldwork, where risk and responsibility are linked to content and context rather than location. In practice, this entails extending access to supervision, counseling, and reflective spaces to all researchers engaging with potentially distressing materials, not only those formally ‘in the field’. Adjustments to the model would therefore be semantic rather than structural: its cyclical continuum of care remains valid, but its entry points multiply according to researchers’ exposure type.
Conclusion: Embedding emotional integrity into research culture
This paper began in response to a silence: my own, and that of many colleagues around the emotional aftershocks of concluding the emotionally demanding research. It ends with an invitation: to build a research culture where care is not heroic, but habitual; where trauma-informed practice is not remedial, but foundational; and where the ethical treatment of researchers is as robust and non-negotiable as that of participants. Research grounded in human vulnerability demands structures that also protect those who carry that vulnerability on their shoulders.
Institutions must move beyond rhetorical commitments. Trauma-informed policies must be enacted. Supervisors must learn to mentor emotional complexity. Ethics committees must assess researcher well-being with the same seriousness as participant safety. And most critically, institutions must stop rewarding silent endurance as proof of professional strength. As one participant noted, ‘The more we are told to handle it ourselves, the easier it is for institutions to stay quiet’. (S, researcher). Emotional integrity is not a luxury but a condition for sustainable, ethical research. Support for researcher well-being should not be a personal achievement but a collective standard. When research cultures honor the emotional labor of their members, both knowledge and those who produce it are allowed to thrive.
Footnotes
Appendix
Ethical considerations
This study received ethics approval from the Institutional Committee for Ethical Review of Projects (CIREP) at Universitat Pompeu Fabra, Barcelona, Spain, on 22 February 2023 (reference number: 281; approval code: X2020005313). The study is part of the bigger project titled ‘Enhancing the potential to provide reproductive health support to traumatized refugee mothers through community developed mobile app’, and the approval was received for all research conducted within this study between 2021–2023. All procedures complied with the ethical standards of the committee and with the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all participants prior to data collection. In cases where written consent was not feasible, verbal informed consent was obtained and formally recorded in accordance with the approved protocol.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the Horizon 2020 research and innovation programme under the Marie Sklodowska Curie grant agreement no 945380.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.