
Abstract
The Tak Province Community Ethics Advisory Board (T-CAB), established in January 2009, provides advice on health research (e.g., malaria, tuberculosis) conducted by the Shoklo Malaria Research Unit (SMRU) along the Thai-Myanmar border. As of June 2025, it comprises 19 members, aged between 25 and 60, of Karen and Burmese ethnicities. They advise health researchers on issues such as informed consent procedures and participant compensation amounts. They also provide direct input on research priorities, study design and procedures, and review participant-facing materials, including information sheets, and interview guides for qualitative studies. This paper presents reflections and lessons learnt over the past 10 years.
Introduction
The Shoklo Malaria Research Unit (SMRU), part of the Mahidol Oxford Tropical Medicine Research Unit (MORU) network, provides humanitarian health services along the Thai-Myanmar border, primarily serving Karen and Burmese migrants. Alongside health provision, SMRU conducts health research that addresses local health challenges, including malaria, tuberculosis, and maternal and child health.
Historical and persistent ethnic conflicts in this area compromise access to healthcare for communities in the region (Davis et al., 2015). Due to uncertain legal status, unstable employment and language barriers, many individuals living on the Thai-Myanmar border face significant challenges in accessing healthcare (Khirikoekkong et al., 2023a).
SMRU has a comprehensive community engagement programme. At its core is the long-running Tak Province Community Ethics Advisory Board (T-CAB; Cheah et al., 2010; Maung Lwin et al., 2014). Community Advisory Boards (CABs) comprised of community members or variants, are the most widely documented structures for supporting community engagement (World Health Organization, 2020).
The T-CAB was established in January 2009. From its establishment to June 2025, the T-CAB has conducted 100 in-person meetings, and over 155 topics have been discussed. The group actively makes efforts to include both younger and older members of the communities. In June 2025, the T-CAB comprised 19 members, 8 men, and 11 women aged between 25 and 60, from Karen and Burmese ethnic groups. Members include government and civil servants, healthcare workers, local leaders, non-governmental organisation (NGO) workers, farmers, and local business owners, from both sides of the Thai-Myanmar border.
The T-CAB meets regularly in-person, and meetings are facilitated by experienced coordinators from SMRU and supported by translators due to the multiple languages used at the border (Thai, Karen, Burmese, and English). Additionally, many informal meetings have been held to address ad hoc issues. Meetings typically take place on Saturday mornings, when members are available to attend. Members are compensated for their time (equivalent to a day’s wages) and reimbursed for transport if needed. Meetings usually start with members sharing general news and health-related issues from their villages or townships. This is followed by discussions of one or two planned research studies or health programmes. Occasionally, results of completed studies are shared with the members. Meetings conclude with a social lunch among T-CAB members and researchers.
As part of ongoing capacity-building efforts, T-CAB members have regular training sessions. Training topics vary according to members’ expressed interests. Topics have previously included general topics such as leadership, public speaking, and research ethics. Health and disease specific topics have also been included, for example, malaria, tuberculosis, filariasis and family planning. In addition to structured training sessions, field trips to laboratories and clinics have been arranged to augment participants’ comprehension, involvement, and engagement.
The group’s insights significantly influence our understanding of community context and inform our approach to our health services and research conducted at SMRU sites, highlighting their critical role in shaping research, in ways that are responsive to community concerns while ensuring that community’s voices are heard. In fact, SMRU researchers are encouraged to consult the group at the study inception phase, before protocol submission.
Although the facilitators are SMRU staff, the T-CAB operates independently, with a rotating chair selected from among its members. Potential conflicts of interest are minimised, as T-CAB members are not involved in study implementation or data analysis.
In this paper, we report our evaluation, reflections, and lessons learnt on engaging with the T-CAB. Here, ‘we’ refers to the research and engagement team involved in conducting the evaluation.
Methodology
We employed a mixed-methods approach. We used a qualitative approach with the T-CAB members, self-administered questionnaires (SAQs) with researchers and staff, reviewed meeting minutes, and held an evaluation workshop.
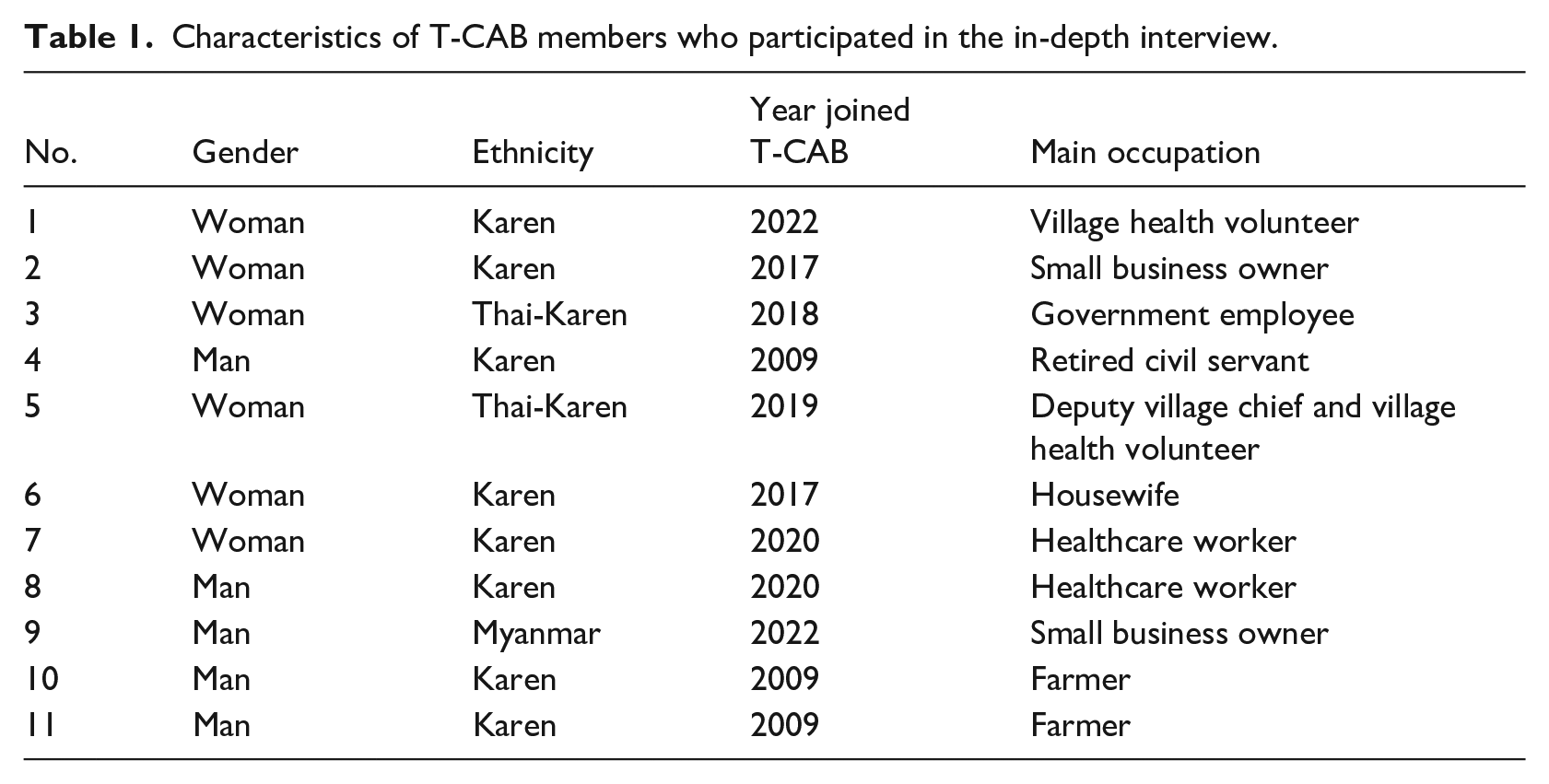
We conducted 11 in-depth interviews (IDIs) with T-CAB members between August 2023 and October 2023. Members were asked to reflect on their participation since they joined the T-CAB. Their characteristics are as shown in Table 1.
Characteristics of T-CAB members who participated in the in-depth interview.
We used online self-administered questionnaires (SAQs) to collect data from local and international researchers, doctors, and healthcare staff who engaged with T-CAB between July 2016 and June 2024. From this group, a total of 18 complete responses were obtained. The SAQs collected insights into the respondents’ experiences and perceptions regarding their engagement with T-CAB. Apart from demographic information (gender, job level, academic status at time of engagement), the SAQs asked respondents about how often and in what capacities they interacted with T-CAB, the perceptions of key benefits alongside any challenges encountered from their engagement, and how T-CAB influenced their work professionally. The questionnaires also assessed the willingness to participate in future T-CAB meetings, prompted respondents to provide suggestions for improving T-CAB’s facilitation and organisation, as well as strategies to enhance its impact and promote its work within and outside SMRU. Lastly, it asked for any additional feedback or suggestions, including logistical issues (e.g., meeting times, languages, and formats). Responses were collected in both structured (quantitative) and open-ended (qualitative) formats.
Additionally, we reviewed minutes from 68 T-CAB meetings in the preceding 10 years, that is, between July 2016 and June 2025, during which a total of 133 topics were discussed. It validated the mixed-methods findings, especially in T-CAB’s functions and its influence in research practices, supporting the core themes presented in our results and discussion. Only nine meetings took place in 2020 and 2021 due to nationwide travel restrictions and border closures implemented to prevent the spread of COVID-19.
Finally, we hosted an evaluation workshop with all T-CAB members in February 2024. In the workshop, we discussed the findings from the T-CAB interviews, SAQs, meeting minutes, and asked for additional feedback. This was important to include views from members who were not able to participate in the IDI.
Data management and analysis for the qualitative data were conducted using NVivo software. All survey forms were treated with confidentiality, with access restricted to authorised study team members. Descriptive inputs from the surveys were entered into NVivo for data management and coding. Data were coded based on emerging themes, and thematic and narrative analyses were conducted by the study team until data saturation was reached. Analysis commenced as soon as all expected responses were acquired.
Ethics approval for the in-depth interviews and SAQs was obtained in June 2023, covering the period from June 2023 to June 2024.
Results
Perspectives of T-CAB members
The impact of the T-CAB
Our consultation with the T-CAB has resulted in improvements in the value, ethics and practicality of our studies and health programmes.
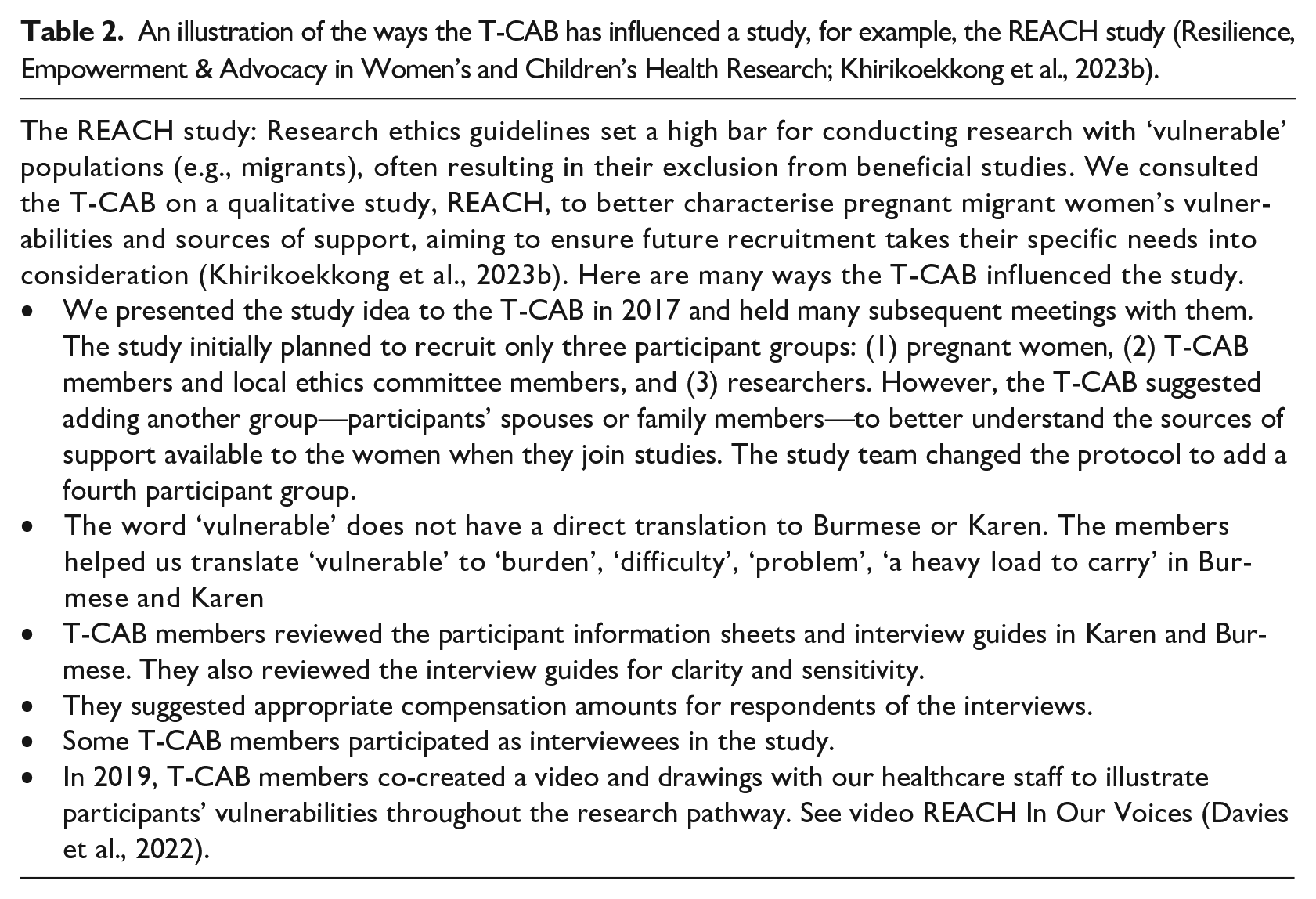
Firstly, members provide advice on issues common across studies such as informed consent, the amount to compensate participants, and reimbursement for transport costs. Secondly, members provide input directly in study design and procedures, and advocate for patient safety, for example, in procedures, or while travelling to the study site. Thirdly, they review participant-facing materials such as educational posters, information sheets, survey questions, and interview guides for qualitative studies. Finally, in some social science research, they are participants or respondents. Table 2 provides an illustration of the many ways the T-CAB improved a social science study.
An illustration of the ways the T-CAB has influenced a study, for example, the REACH study (Resilience, Empowerment & Advocacy in Women’s and Children’s Health Research; Khirikoekkong et al., 2023b).
Commitment and perceived role of members
It was clear from the interviews and evaluation workshop that most members are committed to their role. In fact, three members have been serving since the establishment of the T-CAB in 2009.
Most members saw their role as helping with healthcare access. They said that they frequently advised community members on where to seek care when they are ill. Members saw themselves as a bridge between researchers and healthcare providers, and the community. They said that they advised researchers on the ethical and practical aspects of studies. Some issues they raise are broad, while others are more specific, such as questions in a questionnaire designed to seek community opinion.
‘After the meeting, we go back to our area and share information [on health and research] with others.’ (woman, member since 2020)
Benefits to members and community
Members said that they see the T-CAB as a place to learn. They enjoy learning about their own health and passing on the information to their community members via their own networks or through their roles in the community. They enjoyed visiting our laboratories, as they were able to learn what happens to the blood samples collected as part of research studies.
They also enjoyed exchanging information with each other on general topics, for example, situation along the border, which could be related to safety or crops, because members are from different areas along the Thai-Myanmar border and may not be familiar with other places. Therefore, this is an opportunity to expand their network through meeting others and sharing interests.
Members appreciate that their opinions are sought and acted upon. Despite not having medical background or qualifications, they appreciate that they are given opportunities to reflect their views, provide suggestions, and be part of some studies which they would not have such opportunity elsewhere.
Challenges
Although members are keen to contribute and attend meetings, they mentioned that they faced many challenges, including travel to meeting location, often SMRU office, see Figure 1. Some members travel from the Myanmar side of the border, and some do not have required travel documents and fear being stopped by the police, as there are permanent checkpoints along travel route to meeting location. Figure 1, a map of the Thai-Myanmar border region, illustrates that members generally reside mainly in three districts, including Mae Ramat, Mae Sot, and Phop Phra.
‘We do not have [legal] documents. We fear for our safety if we have to travel . . . sometimes the police check early in the morning. We are afraid of that.’ (man, member since 2020)
Meetings usually discuss complex research studies on topics such as malaria and tuberculosis, including clinical trials, social science studies, and healthcare screenings. Members often lack the medical and scientific knowledge to fully understand these concepts, and researchers may struggle to communicate in accessible lay language. Multilingual meetings add translation challenges, especially with scientific jargon. Some members have noted difficulties in understanding the content and find it challenging to provide advice.

Map of the Thai-Myanmar border region.
Members see their main role as providing input on how to improve healthcare and healthcare access, but less on clinical research. This may be because SMRU is primarily seen as a healthcare provider, known to the community as the ‘fever clinic’ or the antenatal care clinic. SMRU conducts research alongside the provision of humanitarian aid and healthcare, but this constitutes only 10% of our work and informs our healthcare provision.
All meetings must be held in-person. Online meetings are not feasible for our context, as became apparent during the COVID-19 restrictions. Reasons include that members live in areas with unstable or no internet connection, are not equipped with devices, and some are unfamiliar with online meeting platforms.
Suggestions for improvement
Members suggested that more training on research ethics should be conducted. This would help them to better understand the ethical considerations involved in research and enable them to contribute more effectively to discussions and decision-making processes.
There was also a suggestion to recruit more young members. Bringing in younger individuals could bring fresh perspectives and new energy to the T-CAB, as well as ensure the continuity and sustainability of the group in the long term.
Perspectives from researchers and staff from engaging with the T-CAB
A total of 18 respondents (13 women and 5 men) from a range of professional roles (e.g., researchers, clinicians, programme staff, and public engagement practitioners) completed the SAQs during the period of the ethics approval (between June 2023 and June 2024). They were from different levels of seniority, with two identified as senior researchers, six as mid-career researchers, and five as junior researchers. There were five respondents who reported to have attended T-CAB meeting once, six attended between two and five times, four attended between five and ten times, and two attended the meeting more than ten times. Some researchers presented more than one study or project to the T-CAB.
Perceived benefits and how feedback from T-CAB influenced research
The responses indicate that T-CAB greatly contributes to enhancing research ethics, making it more responsive to community needs and context appropriate, with 14 responses confirming that T-CAB had influenced their work. They expressed that the feedback had helped enhance research design, introduced new perspectives for study, reviewed participant-facing materials, and strengthened research ethics. Based on feedback from T-CAB, some researchers modified certain aspects of their study design or materials. Additionally, presenting the research to the T-CAB reminded them to think about research application to community. It also promoted openness and respect between researchers and community members and became an opportunity to discuss study in lay terms, which is more relatable and could lead to discussions that would not take place in other research contexts. Only one said that it had no effect on their work, while three others were not sure or could not tell how it had affected them.
Challenges encountered
There are some areas considered by respondents to be areas for improvement. Language barrier, in terms of the researchers’ ability to present clearly, and the availability and quality of translation during the presentation, were observed. Some respondents felt that T-CAB members found it difficult to fully participate in giving recommendations when academic terms or technical terms were used, especially when the meeting is lengthy and rushed by time-constraints.
Suggestions for improving facilitation, organisation, and impact
Respondents proposed several areas for improvement. These included sharing translated materials in advance, simplifying technical content, and allowing more time for discussion. Many emphasised the importance of continued training particularly in ethical review, research communication and facilitation techniques. A few suggested that the roles and responsibilities of T-CAB could be made clearer and more structured to further enhance its effectiveness.
For suggestions for increasing T-CAB’s impact included creating a dedicated website section or social media presence, formally acknowledging T-CAB contributions in research outputs, and incorporating T-CAB into staff induction. Some respondents also recommended involving T-CAB more actively throughout the research process, not just during proposal development. When asked if they would be willing to engage with T-CAB again in the future, 14 respondents said they wanted to keep being involved, while the other 4 were not sure. No respondents chose to answer ‘No’ indicating a generally positive perspective towards continued engagement.
The responses showed that T-CAB is well-respected, and inputs from them are considerably important and impactful, especially at SMRU. Even though this engagement is perceived positively and beneficial, the challenges observed and reported in the responses showed that facilitation, translation support, and researcher preparation could be improved to enhance accessibility and understanding.
Discussion and conclusions
This paper highlights the crucial role of the T-CAB in ensuring our research and health programmes are ethical, relevant, and beneficial to the communities we serve. The T-CAB’s consistency and longevity have established trust, which enables members to provide honest feedback. While the T-CAB does not function as an ethics committee, it complements their role by offering community perspectives. It serves as a platform for community members to interact with experts, facilitating learning and advocacy. Members see themselves not as community representatives but as a bridge between the community and researchers, advocating for the community’s needs and concerns. This has not changed since the creation of the T-CAB (Cheah et al., 2010).
To our knowledge, the T-CAB is one of the longest-running CABs providing input on health research, and we have one of the most extensive records of any CAB proceedings. One limitation of this paper was the response rate to the SAQs emailed to researchers and staff who had engaged with the T-CAB. Despite several attempts to encourage participation, the response rate remained lower than expected. We were cognizant of questionnaire fatigue. SAQs administered outside the ethics approval period were excluded from the analysis.
Due to the success of the T-CAB, five more advisory groups have been established throughout the MORU network, involving hill tribe members, ethnic groups, and young people (Ean et al., 2024; Perrone et al., 2024; Osterrieder et al., 2025). Burdens and challenges are actively mitigated, and suggestions from T-CAB members and researchers are incorporated whenever possible. Additionally, we are involving T-CAB members in setting research priorities in the future, ensuring their input shapes the direction of our research.
Footnotes
Acknowledgements
This work represents a long-standing collaboration and partnership. We are grateful to all past and present members of the T-CAB for their dedication and invaluable input. We also extend our sincere thanks to the researchers and staff who participated in this evaluation. The essential contributions of the engagement facilitators and translators are gratefully acknowledged. We thank Myo Chit Min for producing ![]() . And finally, this work is built on the strong trust and partnership of the migrant communities along the Thai-Myanmar border, to whom we express our deepest gratitude.
. And finally, this work is built on the strong trust and partnership of the migrant communities along the Thai-Myanmar border, to whom we express our deepest gratitude.
Ethical Considerations
Ethics approvals were granted by two committees: the Faculty of Tropical Medicine Ethics Committee (FTM EC, reference: MUTM 2023-035-01) on 22 June 2023, and the Oxford Tropical Research Ethics Committee (OxTREC, Reference: 515-23), on 19 April 2023. An amendment to align the submitted documents with those approved by FTM EC was subsequently approved by OxTREC on 28 June 2023. A key ethical consideration is the decision, made in consultation with participants, to recognise the public-facing role of T-CAB and its collaboration with SMRU. T-CAB members operate as public advocates for their community. The members are proud of their role, having provided specific informed consent to be identified, viewing it as a model of community engagement. To balance this transparency with individual protection, specific ages were removed from demographic data, and all quotes remain unattributed to individual members. This strategy honours their dedication and voluntary service in this advocate role.
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
All participants provided written informed consent for publication prior to participating, under the confidentiality section.
Author Contributions
FN, PYC and BH provide overall support for and oversight of the T-CAB. PYC, KML and FN set up the T-CAB in 2009. Over the years, PT, LK, KML, NK, PYC have been facilitators of the T-CAB. NK and PT conducted the interviews. PYC and AO wrote the first draft of the paper. NK, SA and AO led the overall evaluation initiative. All authors read and approved the final manuscript. PYC is the guarantor of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in whole by the Wellcome Trust [220111/Z/20/Z, 222870/Z/21/Z, 228141/Z/23/Z].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this publication are not publicly available due to ethical and legal reasons, including participant anonymity but are available from the MORU Data Access Committee on reasonable request. A data access agreement will be put in place prior to data transfer.
Open Practices
For the purpose of Open Access, the authors have applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.