
Abstract
The Global Code of Conduct for Research in Resource-Poor Settings (GCC) aims to stop the export of unethical research practices from higher to lower income settings. Launched in 2018, the GCC was immediately adopted by European Commission funding streams for application in research that is situated in lower and lower-middle income countries. Other institutions soon followed suit. This article reports on the application of the GCC in two of the first UK-funded projects to implement this new code, one situated in India and one in Pakistan. Through systematic ethics evaluation of both projects, the practical application of the GCC in real-world environments was tested. The findings of this ethics evaluation suggest that while there are challenges for implementation, application of the GCC can promote equity in international research collaborations.
Keywords
Introduction
As the world faces ‘a global health crisis unlike any in the 75-year history of the United Nations’ (United Nations (UN), 2020), it is evident that national-level actions to address the coronavirus pandemic are no match for the global scale and complexity of the crisis. Never before has it been so apparent that international cooperative efforts are needed to ‘[e]nsure healthy lives and promote wellbeing for all at all ages’ (United Nations (UN), n.d.). While the coronavirus pandemic has brought the need and potential benefits of international research collaborations into sharp focus, the necessity of cooperative efforts to address global challenges has long been recognised (Godoy-Ruiz et al., 2016; OECD, 2014).
In recognition of the potential benefits of international collaborative research, many funding streams actively promote and/or require cooperative efforts. In the United Kingdom (UK), for example, the UK Research and Innovation, Global Challenges Research Fund (UKRI/GCRF) has invested heavily in research partnerships for ‘sustainable solutions to help make the world safer, healthier and more prosperous’ (UKRI, 2022). This trend is particularly evident in health research, where collaborations are viewed as essential for addressing global health disparities and to build research capacity in low- and middle-income countries (LMICs) (Kerasidou, 2019).
The coronavirus pandemic has also served to highlight extreme global health disparities with low-income and marginalised communities bearing the biggest impact thus amplifying existing inequities (Ivers and Walton, 2020). People living in LMICs experience significant hindrances to accessing public health measures that are needed to prevent the infection from spreading due to over-crowding, poor housing conditions and poor sanitation. Additionally, the global economic downturn has put millions of people in LMICs at significant risk of increasing or developing food insecurity (Shadmi et al., 2020). While collaborative research cannot offer a panacea for global health disparities, it should be noted that research collaborations between high-income countries (HICs) and LMIC groups are normally set against a backdrop of inequities. These inequities generate power imbalances between HIC and LMIC partners (Bradley, 2017) which researchers must recognise and take steps to address. International research ventures should help to reduce inequities, not reinforce them.
To help ensure equity in research, the European Union funded the work of a large, international consortium entitled TRUST (GCC, 2021), to develop a new ethics code, The Global Code of Conduct for Research in Resource-Poor Settings (GCC). The GCC consists of 23 clearly articulated articles (GCC, n.d.) that aim to help funders, researchers, communities and individuals to recognise and address potential ethical pitfalls. It is underpinned by the moral values of fairness, respect, care and honesty. During the development of the GCC, these values were identified by the TRUST consortium as being essential for equitable research partnerships (Chatfield et al., 2016). Launched in 2018, the GCC was immediately adopted by the European Commission as mandatory for projects conducted in lower or lower-middle income countries for their major funding streams. Other institutions soon followed suit, including the University of Central Lancashire (UCLan), the host UK university for the two projects examined in this article.
Following adoption by UCLan, implementation of the GCC became mandatory for ethics approval of projects situated in an LMIC. While the GCC is now applied in more than 40 countries (Schroeder et al., 2020), there has been little evaluation of its applicability and relevance in different cultural settings. This article aims to address a gap in understanding how/whether the GCC can be helpful for reducing inequity in research collaborations in two different cultural settings.
The article reports on application of the GCC in two of the first UK-funded projects to implement this new code, one situated in India (IMPROVISE) and one in Pakistan (BiZiFED2). Through systematic ethics evaluation of both projects, we 1 examined compliance with the GCC, from retrospective, ongoing and prospective viewpoints. The primary aim of these evaluations was to facilitate critical reflection upon practical application of the GCC in two real-world environments. It was anticipated that this information will aid understanding of the value of the GCC and the challenges for implementation in these settings.
The choice of these two environments is significant; while there was extensive input from research ethicists in India during the development of the GCC, there was no input from Pakistan. Indeed, there was little input from any Muslim countries or communities. Consequently, we hope that this evaluation might also offer some insight into where further research might be needed on the application of the GCC in Muslim countries.
The two projects: IMPROVISE and BiZiFED2
Both the IMPROVISE and BiZiFED2 projects include teams from UCLan, UK, which was one of the first universities to adopt the GCC for application in all collaborative projects that are situated in LMICs.
IMPROVISE in India
IMPROVIng Stroke CarE in India (IMPROVISE) is a Global Health Research Group (GHRG) focussing on addressing priorities in stroke care in India via high quality research (from 2017 and ongoing at the time of writing). Stroke is the fourth leading cause of death and the fifth leading cause of disability in India (Directorate General of Health Services: Ministry of Health and Family Welfare, 2019). People typically suffer a first stroke at a much younger age than in higher income countries (Jones et al., 2022), leading to a significant socio-economic burden (Dalal, 2006).
IMPROVISE GHRG has worked in partnership across the UK, Australia and India. There have been three key stages, to:
(1) agree research priorities using co-developed criteria including elements of stroke unit care that will benefit as many people as possible, and which are affordable and achievable in Indian healthcare settings,
(2) conduct robust feasibility studies on these priorities at three centres in India and
(3) develop a longer-term, sustainable, programme of stroke research and service development.
Significant improvements in stroke outcomes have been achieved through organised stroke unit care, which is suitable for all patients, reducing mortality and morbidity (Langhorne and Ramachandra, 2020). However, it is not known what components of the stroke unit interventions are effective, although swallowing and hydration, and neurological and physiological monitoring are thought to be key elements for improving stroke care. These elements were identified as priorities for evaluation in the IMPROVISE project and ‘care bundles’ for evaluation were co-developed with stakeholders in India around these elements of care.
BiZiFED in Pakistan
BiZiFED2 (Biofortification with Zinc and Iron for Eliminating Deficiency 2) (Lowe et al., 2020) was a collaborative research programme involving partners from the UK and Pakistan (2019–March 2022). It aimed to investigate whether biofortification of crops could offer a cost-effective and sustainable strategy for reducing zinc and iron deficiencies in rural populations Micronutrient deficiencies are a global public health problem, with the greatest burden occurring in LMICs and in Pakistan, over 40% of women are zinc deficient and over 20% have iron deficiency anaemia (Ohly et al., 2019). Biofortification is a process by which the nutritional quality of food crops is improved through plant breeding techniques and/or the addition of nutrient-rich fertilisers. BiZiFED2 was funded by the Biological and Biotechnology Research Council through the GCRF in the UK. The programme had three main components. The first component comprised a randomised controlled effectiveness study to assess the impact of consuming biofortified flour on zinc and iron status. The participants included adolescent girls and children living in a low-resource community in north-western Pakistan. The second component focussed on understanding wheat growing conditions in Pakistan and supporting farmers to improve the yield and grain quality of biofortified wheat. The third component focussed on promotion of the sustainable production and consumption of biofortified wheat in Pakistan (UKRI, 2019).
BiZiFED2 brought together a consortium of academic partners from the UK and Pakistan, plus a charitable body (the Abaseen Foundation), that had been working with UCLan to help improve the lives of those who live in one of the poorest and most deprived areas of Pakistan for over 20 years.
Methods
The methodological approach for these evaluations falls broadly within the domain of empirical ethics (Molewijk and Frith, 2009) as it involves the collection and analysis of ‘ethically relevant’ empirical data (DuBois, 2009). The data can be collected via a wide variety of means, by the empirical ethicist, or other researchers, as long as the data is relevant to ethical analysis of the phenomena or intervention in question. The approach taken to data collection differed for each project and is outlined below. The approach taken to data analysis was the same for each of the two projects. All data was qualitative and was analysed deductively using a framework developed from the 4 values and the 23 articles of the GCC. In other words, the data was first sorted in terms of relevance to the values of fairness, respect, care, and honesty and then further analysed in terms of compliance (or otherwise) with the relevant GCC articles.
IMPROVISE data collection
For the evaluation, 13 representatives from IMPROVISE were invited to discuss their experiences and opinions about a range of topics that were directly relevant to the requirements of the GCC. To ensure breadth of perspective, representatives were included from the host institution in the UK, partner institutions in the UK, Australia and India, and field workers in India. Table 1 provides an overview of the contributors’ roles in IMPROVISE.
Overview of the contributors’ roles in IMPROVISE.
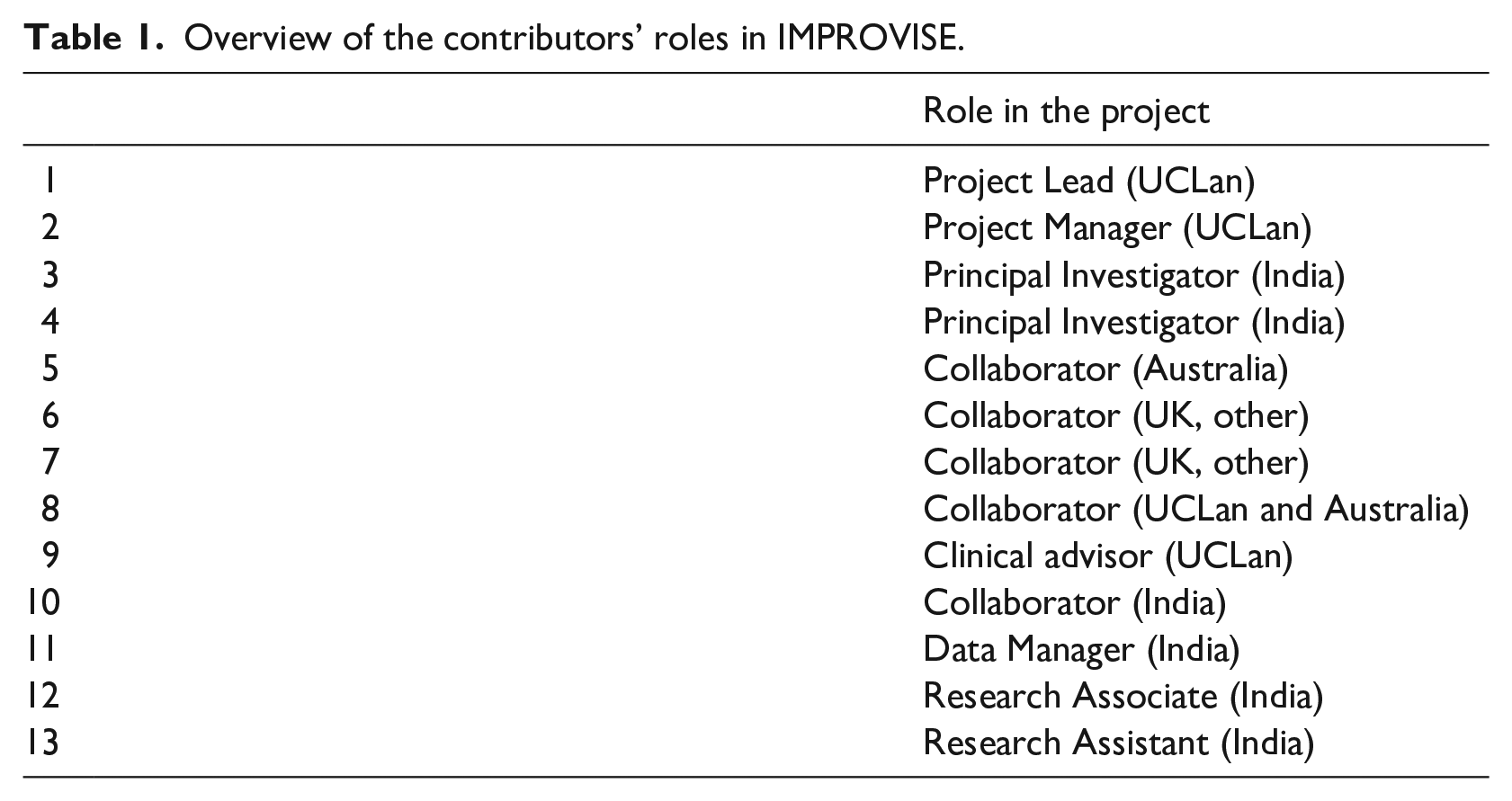
The one-to-one consultations and the evaluation were conducted by an empirical ethicist, external to the project, who was also involved in the development of the GCC. Questions referred to past experience (e.g. How did you go about seeking ethics approval?), ongoing experience (e.g. How are members of the local community engaged in the project (other than as participants)?), and future plans (e.g. What are the plans for publication and dissemination of findings?). This qualitative data was collected during the period January–February 2020.
BiZiFED2 data collection
This evaluation employed a participatory approach which involved consultation with different groups of stakeholders to gather their experiences and opinions about implementation of the GCC in BiZiFED2 specifically, as well as more broadly (aligning with beliefs and values) in Pakistan. The stakeholders included:
Project staff in Pakistan (early-stage researchers and senior researchers involved in the BiIZiFED2 project including the Project Director, Project Manager, nutritionist, field workers and other project staff). Six persons were involved via individual consultations and 12 via group consultation.
Research ethics committee (REC) members at Khyber Medical University (KMU) in Peshawar (18 persons).
Trustees of the Abaseen Foundation in the UK and in Pakistan (five persons).
In total, 41 people contributed through either group consultations, individual consultations or both. Questions varied according to the target groups, but all were designed to help reveal information relevant to analysis of the ethical components of the study. Additionally, REC members were asked to comment upon the relevance and suitability of the GCC in Pakistan as well as implementation in the BiZiFED2 study. The questions were devised by a team that included a researcher in Pakistan who had not previously been involved with the BiZiFED2 study. Data from the stakeholders in Pakistan was collected by the local researcher. Consultations with four UK-based AF trustees and the staff workshop were conducted by a member of the UK-based project team. The qualitative data was collected during the period February–July 2020. The original project design included consultations with participant families and community elders, but this was altered due to coronavirus restrictions. Group consultations occurred prior to the implementation of restrictions. One to one consultations during the pandemic were conducted online.
Findings and ethics analysis
Given the high volume of data generated for the two projects, it is not possible to detail all findings in this article. Rather, we focus here upon the most striking findings and challenging issues. The findings are organised by the four moral values that underpin the GCC namely, fairness, respect, care and honesty with selected illustrative quotes from contributors. To avoid association between persons and individual quotes, the quotes are attributed in a general manner only (for instance, senior project staff, project staff, field worker etc.).
Fairness
Fairness has a number of interpretations, but the most relevant for collaborative research ethics is fairness in exchange (Schroeder and Pogge, 2009). Of fundamental importance is that the research has relevance and potential benefits for the community or environment in which it is situated.
Local relevance and benefits
Both IMPROVISE and BiZiFED2 were designed with the intention of yielding local benefits (improved stroke care and improved zinc and iron status) but good intentions alone are not sufficient for determination of local relevance (Schroeder et al., 2019a, 2019b). Both projects determined the means by which benefits were going to be achieved through discussions with local teams. For instance, in the first stages of the IMPROVISE project, the research team worked in partnership with local teams to agree research priorities and care bundles that were acceptable, affordable and achievable in these settings: ‘When we designed it together, we modified according to the local situation particularly the diet consistency and all – those things are very good’ (Senior project staff member, India).
Dietary considerations were also important for BiZiFED2 where wheat flour is used every day to make chapattis. Hence, biofortification of the wheat that is grown locally has the potential to offer sustainable benefits to the communities and relevance of the project was tested with both local partners and members of the community: ‘Local partners agreed that this research is highly relevant because of the high prevalence of zinc and iron deficiencies (and related health problems) among women and children in Pakistan’ (Project staff member, Pakistan).
Additionally, both teams anticipate benefits for the local communities that extend beyond the more focussed aims of the projects. In India: ‘Even when this project is finished, there will be a huge number of people involved in the project who will understand and be more educated for further projects in their own fields with or without us for the future’ (Project staff member, UCLan).
And in Pakistan, there is potential for broader wellbeing benefits as borne out by the experience of a member of the project team who works closely with the community: ‘I am frequently asked on different occasions about the importance of balanced diet, iron and zinc, its rich food sources to increase its intake’ (Field worker, Pakistan).
Community involvement
For equitable partnerships, involvement of the local community should be continued throughout the implementation of the research project, but this can be difficult to achieve in its entirety, especially where there is no existing community engagement.
Such was the case for IMPROVISE. Representatives from local communities and potential participants were not involved in the early planning stages of IMPROVISE, largely because this is the first study that the UCLan team were involved in India. However, engagement was built into the study at later stages. For instance, at the time of this evaluation, one patient and public involvement meeting had been held at each of the three study sites. Amongst other things, these meetings highlighted the need to make adjustments for cultural differences for effective community engagement.
Trust between partners can take a lot of time and effort to develop; existing relationships between the collaborators in BiZiFED2 and the local communities provided a firm foundation for transparent and equitable partnerships. Many activities were designed to engage with the local communities: ‘We involved the whole community through public meetings, banners display, leaflets distribution and information sheets. We met the eligible and non-eligible 2 groups and have sought their inputs and feedback’ (Senior project staff member, Pakistan).
In particular, with the Jirga (committee of respected village elders): ‘It also guided us to establish a local supervisory body of the elders to oversee the project from the community point of view. We involved all the members at all the stages of the project implementation and adjusted the project activities in light of the community feedback’ (Senior project staff member, Pakistan).
However, in Pakistan, there are challenges to working with female research participants in this community because of the existing patriarchal infrastructure and systems (Tabassum, 2016) which mean that direct consultation with them was limited.
Local researchers
As well as local community involvement, it is essential that local researchers are employed meaningfully in the project conceptualisation and implementation. For IMPROVISE, at the higher level, meaningful inclusion of local researchers has been evident from the planning stages and throughout, but at ground level, there have been challenges for full and meaningful involvement of local researchers. Initially, there was some confusion around skills levels and equivalence between the UK and India. While this was not anticipated, the project team responded quickly and effectively engaged in intensive training and capacity building to ensure that the UK team had a better understanding of the local context, and local researchers were equipped with the relevant skills for their assigned roles.
BiZiFED2 has 35 members of staff in Pakistan including nutritionists, laboratory technicians, community health workers and research assistants. Capacity building was built into the project from the start.
Respect
Respect requires acceptance that people’s customs and cultures may be different from one’s own, and that behaviour should not cause offence. It means that one may need to accept a decision or a way of approaching a matter, even if one disagrees. Researchers should not enter a new environment ‘blind’; groundwork will be needed when working in different cultural settings to ensure that researchers respond appropriately to specific cultural sensitivities (Tindana et al., 2007).
In this regard, the support of the Abaseen Foundation was invaluable for respectful implementation in BiZiFED2 because they already had established links within the local community: ‘We have had to get involved in this aspect of the project because we (AF) are part of the community’ (Abaseen Foundation Trustee).
Nevertheless, some aspects of the study protocol required adjustment in response to local preferences. The BiZiFED2 project staff identified many examples of modifications to the study design. For instance, adolescent girls were always accompanied either by their mothers or female community workers; proper purdah 3 and separate waiting areas were provided for the female staff to keep interaction with males to a minimum. Additionally, BiZiFED2 staff showed respect for local dress customs by covering themselves appropriately to comply with the traditions of the community being visited.
However, even when researchers take steps to respect traditions, operationalising research in regions where there are well-embedded sensitivities (like gender roles) can lead to unforeseen issues: ‘A couple of times patients have refused to give blood samples to the male lab workers owing to the cultural norms’ (Field worker, Pakistan).
Further, work in a community where values and traditions challenge one’s own can be complex as noted by an interviewee from the UK: ‘The Jirga operates at one level in the community and it’s all men. The younger women and girls are not part of the decision-making process. Not sure if we could learn some lessons, but it is a big cultural challenge of working in this community’ (Abaseen Foundation Trustee).
Local ethics approval
Ensuring respect for cultural norms is one of the reasons why local ethics review should be sought for collaborative ventures, even if ethics approval has already been obtained in the high-income setting. Additionally, local ethics approval can ensure local relevance of the research and respect for local research ethics requirements. For the IMPROVISE project, this has proven to be the most challenging of all the GCC requirements.
IMPROVISE is located at three different sites in India so approval was sought from three different research ethics committees (RECs) in India prior to approval from the UCLan REC. Challenges included:
Each of the RECs had slightly different processes for ethics approval.
Membership of the individual RECs changed over time, meaning that those who reviewed amendments might not be the same persons as those who set the conditions. Additionally, they sometimes set new conditions.
The RECs all set different conditions, but the protocol had to be the same at each site. Consequently, amendments had to satisfy conditions set by all three RECs.
Ultimately, the challenges meant that ethics approval took far longer than anticipated and implementation of the project was delayed by 12 months.
For BiZiFED2, ethics approval was sought in parallel from both UCLan and KMU research ethics committees. The KMU application was modelled on the UCLan system but adapted for the local context. A challenge for approval arose when members of the UCLan REC requested compliance with UK norms for health and safety. While ideally, there should be equivalence in ethics standards to avoid double standards, direct translation into the local context is not always possible. Consequently, ethics approval from UCLan involved in-depth discussion with the committee to ensure that, within the local context, BiZiFED2 adhered to the ‘spirit’ of the guidance.
Care
Researchers who take good care combine several elements. For instance, they care about research participants, in the sense that they are valued as persons (not simply research ‘subjects’); they take care to safeguard the welfare of those who contribute to their research or might suffer as a result of it; and they are diligent in their work.
Informed consent procedures
When working with diverse communities, informed consent procedures must be tailored (in terms of language, literacy, education levels etc.) to achieve genuine understanding.
The IMPROVISE team took great care to tailor informed consent procedures to local requirements, but significant challenges remained that were largely due to the health status of potential participants who have suffered a stroke (e.g. people who were unable to engage with a standard informed consent procedure). In addition, some confusion about the nature of the intervention and the high levels of illiteracy have undoubtedly had an impact. These high levels of illiteracy meant that many potential participants relied upon a family member or other person to read and explain the study information. Research assistants reported more caution observed from those who have low levels of literacy: ‘They get scared. Are you going to test my husband? Are you going to test my wife?’ (Project staff member, India).
Some adjustments that would be made in the UK (e.g. the use of an aphasia-friendly information sheet) were not used in India and differences in understanding/interpretation of the consent process were highlighted when information sheets were adjusted at one of the sites without consultation with project partners.
The BiZiFED2 team also took care to tailor informed consent procedures to local requirements where literacy levels were low amongst the female research participants: ‘The female staff of the project introduced the programme with each family and also in groups wherever they find the opportunity’ (Project staff member, Pakistan).
When seeking consent from individuals, research assistants read information sheets aloud and were able to take questions from the potential participants. In spite of these efforts, some challenges for achieving genuine understanding were observed as was illustrated by the residual confusion amongst the population around the need for biological samples. The randomised controlled trial component of BiZiFED2 involved the collection of blood and hair samples from 500 adolescent girls. While informed consent was sought from the girls and the heads of the household for access to these biological materials, it is unclear whether there was full understanding of what they were needed for: ‘Community is very happy with the flour and free check-up provided to them but in the same time they are much confused about blood and hair samples, . . . is very hard to understand, they ask the same questions again and again’ (Field worker, Pakistan).
Furthermore, while the notion of respect for individual autonomy is paramount in most western cultures, in many parts of the world some type of community approval and/or permission for participation may also be required in addition to individual consent. For BiZiFED2 this entailed approval and permission from the Jirga and consent from the male heads of household as well as individual consent from the female participants.
Complaints procedures
The implementation of accessible complaints procedures is a requisite for ethical research. An effective complaints procedure can give voice to those who participate in research, offering a channel for raising concerns that might otherwise remain unheard, both during and after a study. Significantly, complaints mechanisms offer a means of revealing lapses and failures in ethical conduct thereby providing opportunities for enhancing ethical compliance in research.
Nevertheless, clear procedures for truly accessible complaints mechanisms are extremely rare in research projects. Often, such procedures simply consist of contact details on an information sheet which is of little use to people who are illiterate and/or have no means of contacting this person. It is further complicated when working in cultures (like India or Pakistan) where there can be a reluctance to make complaints.
In India, there was confusion about the feedback/complaints mechanism for IMPROVISE suggesting that this had not been fully explored by all partners at the outset of the research. There was also acknowledgement that people may feel reluctant to complain.
In common with most research, BiZiFED2 provided contact details on the study information sheet and: ‘.. . . that contact confirmed that she has received some calls from community members asking questions. However, she felt she was not necessarily the best contact as her first language is Urdu’ (Project staff member, Pakistan).
Hence, it can be assumed that neither the IMPROVISE nor the BiZiFED2 project had a truly accessible complaints mechanism in place.
Safety of persons involved
Efforts to safeguard welfare should extend to all who are involved in a project including the participants, the local community and the research staff. This can pose distinct challenges when research projects are situated in turbulent regions or when there is some misunderstanding or resistance towards the research.
For IMPROVISE, while some dangers were acknowledged, all overseas visitors to the research sites described appropriate actions for ensuring their health and safety. These included liaison with local partners for pre-travel briefings, advanced booking of transport and hotels, and advice about drinking water etc.
The situation appears to have been more challenging in Pakistan. Female members of the research team in Pakistan encountered some extremely worrying situations whilst conducting fieldwork: ‘We (the team of Community A) faced several tragedies in BiZiFED Project. We were abused by community and one of our community workers got beaten by community females that you people are running and implementing here foreign agenda 4 ’ (Field worker, Pakistan).
‘Female members of the field team experienced intimidation from local children throwing stones, so they have subsequently been accompanied by a security guard’ (Field worker, Pakistan).
The BiZiFED2 team took swift action to prevent further incidents: ‘We have also hired Local Male Community Workers in both areas and utilising their relationships with the communities and also the good offices of the other local male staff’ (Project staff member, Pakistan).
Honesty
The value of honesty has broad scope in the context of global research ethics. For instance, while it is obviously unacceptable to lie, it is equally unacceptable to omit important information from an informed consent process. Most prominently, the duties of honesty are vital for research integrity which include issues such as credit for contributions, manipulation of data or misappropriation of research funds.
Understanding among collaborators
For collaborative ventures that involve teams of workers, it is important that there is openness and transparency about roles, responsibilities, benefits and credits that might be associated with the research.
IMPROVISE experienced some challenges for this requirement in the early stages of the project. Some of the researchers did not fully understand what their roles entailed, but significant efforts have been made to address this, particularly in relation to capacity building and being available for support. However, there appears to have been clarity from the beginning about the expectation for equitable participation: ‘Yeah, we have a publication plan and for every task there is a plan. We have equal participation in all areas of the project’ (Senior project staff member, India). The overall impression from the contributors is of an open and supportive environment.
In BiZiFED2, rather than being ‘driven’ by the overseas (UK) researchers, a participatory approach has been adopted that entailed a leading role for the Abaseen Foundation. This has helped greatly to ensure understanding of roles and responsibilities among collaborators.
Clear information
The value of honesty also requires that all information about the research project is presented as clearly as possible so that understanding can be ensured.
Care has been taken by the IMPROVISE team to ensure that potential participants understand the purpose of the study and what it entails. In spite of these efforts, there was evidence of misunderstandings. For instance: ‘There was one particular meeting we had in Delhi, which was organised by the local centre, and patients and their families came along. . . .What we wanted was their views and their experiences of the illness and the effects of that on their life and beyond. Whereas, what they expected, when they came to the meeting, to actually have some sort of treatment or some sort of benefit from that meeting’ (Project staff member, UCLan).
However, such misunderstandings do not appear to be related to concealed or incomplete information. Similarly, in BiZiFED2, examples of misunderstanding by those involved (for instance, around the use of blood and hair samples) do not appear to be associated with any deficiencies in honesty or lack of openess.
Discussion
Ethics evaluation of ongoing or completed research projects is currently the exception rather than the norm as ethics review is almost solely prospective in nature (Dawson et al., 2019). On site monitoring of research projects has been suggested as an effective method for ensuring ethics compliance during a project (Ochieng et al., 2013) with involvement of the REC which granted prospective ethics approval. This type of ethics evaluation can include routine visits or random spot-checks to study sites to observe research procedures, review study documentation and possibly conduct interviews with participants and relevant research staff (Apau Bediako and Kaposy, 2020). However, on site monitoring is difficult to implement, not least because ‘on-site monitoring adds yet another resource-related issue to already stretched research ethics committees’ (Shafiq et al., 2021: 51). Further, while this type of evaluation can undoubtedly yield benefits, for instance, by helping to ensure that good clinical practice standards are maintained (Shetty et al., 2019) and safeguarding public trust in research (Ochieng et al., 2013), ‘the focus is very likely to be on completing reports rather than critical reflection, engaged discussion, and an increased sensitivity towards all aspects of relevance to ethical judgement’ (Dawson et al., 2019: 3).
The in-depth ethics evaluation of the two studies described in this paper is novel because it broadens the scope of research ethics assessment beyond the norm. It is also novel because we sought to facilitate critical reflection upon whether the application of the GCC can help to achieve equity in research collaborations situated in India and Pakistan. Both the IMPROVISE and BiZiFED2 projects were designed with the GCC in mind with the express intention of developing and supporting equitable research projects in India and Pakistan. Overall, the ethics evaluation has revealed that compliance with the GCC is possible and beneficial in these environments but certain specific challenges and insights were revealed.
In India, there are many factors that could lead to inequities and exploitation in research. For instance, high levels of poverty, unemployment, and malnutrition (Bageshwar, 2021) as well as illiteracy, which is disproportionately high in rural areas (Bhatia, 2013). Similarly, in Pakistan there are high levels of illiteracy, especially amongst females (Khan, 2008), as well as local challenges including poverty, joblessness, tension on the eastern and western borders, and political and economic instability (Khan et al., 2012). Set against these backdrops, achieving equity in international research collaborations can be extremely challenging.
For ensuring local relevance of research, meaningful involvement of the local communities and researchers, and sensitivity to local norms is essential. It is clear that this is aided when there are existing relationships to build upon, as was the case for BiZiFED2. The benefits of community engagement in all types of research are now widely acknowledged and numerous publications describe many potential benefits such as increasing trust, increasing community understanding and acceptance of the studies; enhancing researchers’ ability to understand and address community priorities; improving logistics and running of studies; strengthening the quality of the information that is collected; ensuring culturally sensitive communications and research approaches; and enhancing opportunities for capacity building (Bassler et al., 2008; Cook, 2008; Dunn, 2011). Of course, this is more challenging for research teams that do not have existing relationships with the local communities. Relationships take time to establish, but this should not deter teams from implementing measures that promote meaningful engagement. This was demonstrated by the IMPROVISE team, who developed relationships over the course of the project, that had the potential to yield many benefits for the current project as well as laying the foundation for future collaborations.
Double ethics approval, that is, approval from both HIC and LMIC institutions should be sought whenever possible. 5 HIC approval is not sufficient for assessment of compliance with local norms and requirements; local ethics approval can ensure relevance of the research and respect for norms in a manner that is not possible for RECs in partner HIC institutions. However, this posed problems for both projects, and for IMPROVISE, resulted in a significant delay to the start of the project. IMPROVISE is a complex project, conducted at three sites in India. Seeking approval from two RECs is difficult enough; seeking approval from four RECs (three sites in India plus UCLan in the UK) is a massive undertaking.
In recognition of this complexity, the Indian Council of Medical Research has developed draft guidelines for centralised ethics review of studies that are undertaken at multiple sites (Indian Council of Medical Research, 2019). The guidance describes the process for a common ethics review ‘so that research can proceed expeditiously without compromising ethical principles and ensuring protection for human research participants’ (p. 3). However, the precise processes for operationalising all aspects of these guidelines remains unclear.
Where there are multiple countries involved, due consideration needs to be given to where to apply first (LMIC or HIC RECs) and how best to relieve burden upon LMIC RECs. If HIC RECs are familiar with the GCC, as they are at UCLan, they can check for compliance, as best they can, from their remote viewpoints. Additionally, if sufficient community engagement has been undertaken, the application should already reflect many of the cultural norms in the target community. In this situation, initial approval from the HIC REC might prove the least burdensome option for the LMIC RECs who can then start their processes using information put together for the HIC REC. However, if the HIC researchers or REC members do not have experience of the research context, there is potential to embed problems during the ethics approval process that will then need to be resolved by the LMIC RECs. This is neither fair nor respectful. A viable alternative might be for the HIC and LMIC partners to draft the applications for all RECs in tandem, making sure that differing perspectives are discussed with REC members and harmonised as much as possible before an application is submitted to any REC. Hopefully, issues remaining after that should be smaller and more easily resolved.
The value of care demands that there is no lowering of standards for collaborative research projects that are located in resource-limited areas. It is imperative that researchers from high income locations do not take advantage of weak regulatory mechanisms to employ practices that would not be acceptable in their home countries. But this is not always straightforward. For instance, legal requirements for data protection in the EU are very high when compared with those in India and Pakistan, and most other LMICs. The application of equivalent data protection standards in LMICs can be fraught with difficulties and full implementation is challenging without the necessary resources, skills and infrastructure. Nevertheless, many LMICs are currently in the process of adopting data protection policies. In Pakistan, a draft of the proposed new Personal Data Protection Bill 2020 is open for consultation (Ministry of Information Technology and Telecommunication (MIT&T), 2020). In India, where data protection requirements were previously governed by diverse regulations, there is also a new bill pending. After 2 years of deliberations, The Data Protection Bill 2019 (Lok Sabha, 2019) was submitted by the Joint Parliamentary Committee to the Indian Parliament in December 2021.
Care for the safety and wellbeing of participants and project staff in Pakistan can be impacted by a number of factors including instability in the region, resistance to research and particular cultural aspects. These are often unpredictable. Risk management plans for helping to ensure safety of researchers can be put in place but ultimately, may not be sufficient. Consideration of how to adequately ensure the wellbeing of research staff is largely neglected in contemporary ethics discourse and amendments must be made to current ethical standards (Steinert et al., 2021).
Neither IMPROVISE nor BiZiFED2 had established truly accessible complaints/feedback mechanisms. This is not uncommon. There are many factors that act as barriers for complaints about research activities in LMICs, for instance cultural norms that preclude complaining, illiteracy of research participants and communication (language) difficulties, inability to access the means by which to file a complaint or fear of stigmatisation from loss of confidentiality or anonymity. Given these barriers, a simple email or telephone contact on an information sheet does not constitute an acceptable complaints mechanism. There is no ‘one size fits all’ solution for development of an accessible complaints procedure. Procedures must have sufficient inbuilt flexibility to suit the population who will be affected. This means that, for each unique situation, researchers will need to work with stakeholders to co-create effective strategies that take into account (at least) the circumstances, situation and culture, and the individuals to be recruited to the study (Chatfield et al., 2018).
Lastly, through this evaluation, we hoped to explore the relevance/suitability of the GCC in Pakistan. This was considered important because the GCC had not previously been deliberated in this environment where Muslim beliefs and values are central to the comprehension of ethics (Jafarey and Moazam, 2010), and bioethical deliberation is inseparable from Islam (Pratt et al., 2014). Our evaluation of the GCC implementation in BiZiFED2 indicated some distinct challenges for members of the BiZiFED2 team. For instance, in Pakistan, as in many other Muslim countries, gender inequality is deeply embedded (Khalid, 2018). Most women, aside from a minority in urban areas, inhabit a male dominated society where they are excluded from decision-making (Bukhari et al., 2019). Working in a location where cultural norms and traditions are different to the researchers’ own can be difficult but these challenges are not unique to Pakistan. They are to be expected in international, collaborative research projects and one of the reasons why the GCC is needed.
Overall, feedback from REC members in Pakistan was positive and indicated agreement with both the 4 values (fairness, respect, care, honesty) and the 23 articles of the GCC. However, there was one particular issue that requires further attention. It was noted that there are references in the GCC requirement for taking care to avoid stigmatisation, that may contradict the requirement for being respectful to cultural sensitivities 6 : ‘These examples and the language used would not be appropriate in Pakistan and may cause resistance from people to using the code. Need to come up with more relevant examples or just translate without examples’ (REC member, Pakistan).
Conclusion and recommendations
Our ethics evaluations of IMPROVISE and BiZiFED2 suggest that measures taken to implement the GCC have helped to promote equity in these international research collaborations through actions to facilitate community engagement, respect for local customs and processes, tailored informed consent and double ethics review. Importantly, the act of implementation has helped to reveal what aids and what hinders the building of equitable partnerships.
These factors aid compliance with the GCC thereby promoting equitable partnerships:
Existing collaborative links between the institutions and communities involved in the project.
Significant investment in local staff and capacity building for all.
Respectful responsiveness to challenges as they arise.
An explicit intention and collaborative effort to benefit the local community.
Careful consideration about how double ethics approval should be undertaken to help relieve burden upon LMIC RECs without compromising ethics procedures and requirements at the local level.
Development of a formal complaints and feedback mechanism that is culturally appropriate and accessible to all stakeholders (participants and researchers).
Development of procedures for ensuring understanding of the research aims and processes.
These challenges need to be noted:
When working in new environments, researchers need to be aware that specific cultural sensitivities may clash with their own ethical norms. This must be handled carefully and strategies for navigation of potential dilemmas developed.
Equivalence in legal and governance standards (for instance, data protection and employment law) may be difficult to achieve in full due the different national frameworks and laws. Careful planning, negotiation and capacity building for all partners may be required to ensure that there is a mutual agreement regarding what constitutes ‘best practice’ and that systems and procedures are harmonised as much as practically possible without imposing significant burdens.
In some countries, certain populations tend to have limited access to formal education (like females in Pakistan and rural populations in India). Greater care than expected may be needed to achieve genuine understanding when working with these populations.
Safeguarding of research participants and staff can be challenged in unpredictable ways. Risk management procedures should be developed collaboratively with local communities and be supported by an effective complaints/feedback mechanism.
It is too soon to claim that application of the GCC has helped to achieve equity in international research collaborations, but our analysis from two country studies suggests that it can certainly help to promote equity. Furthermore, as the LMIC and HIC researchers in our projects have learned, there are practical steps that can be taken to overcome challenges and make ongoing improvements.
Footnotes
Acknowledgements
We would like to thank all the contributors in India, Pakistan and the UK for their valuable assistance with these evaluations including members of the BiZiFED2 research team in Pakistan, the Abaseen Foundation Trustees (UK) and members of the Board of Governors (Pakistan); and members of the NIHR Global Health Research Group on IMPROVIng Stroke CarE in India.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author (Chatfield) is Editor in Chief of Research Ethics. Chatfield was not involved in editorial review or processing of the manuscript. It was subjected to peer review in the normal manner and underwent two rounds of revisions before acceptance.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]()
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The BiZiFED2 project was funded by Biotechnology and Biological Sciences Research Council (BBSRC) Global Challenges Research Fund (GCRF), Foundation Awards for Global Agriculture and Food Systems Research, grant number BB/P02338X/1. The exploration of the ethics code reported in this paper was funded by Research England QR Global Challenges Research Fund, awarded to UCLan.
The IMPROVISE project was commissioned by the National Institute for Health Research (NIHR) Global Health Research Group on Improving Stroke Care in India, University of Central Lancashire (16/137/16) using UK aid from the UK Government. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethics approval
Ethical approval for the BiZiFED2 study was provided by the STEMH and HEALTH Ethics Review Panels at the University of Central Lancashire (STEMH 1014 and HEALTH 0100) and by the Research Ethics Committee at Khyber Medical University.
Ethical approval for the IMPROVISE study was provided by the STEMH Ethics Review Panel at the University of Central Lancashire (STEMH 939). Additionally, the protocol was reviewed favourably by the HMSC – Indian Council of Medical Research and Science, The George Institute Ethics Committee, The George Institute for Global Health, New Delhi, Technology, Engineering, Medicine and Health Ethics Committee, and the ethics committees in the individual hospitals.