
Abstract
This study aimed to explore experiences and practices of key research team members in obtaining informed consent for pharmacogenetics research and to identify the approaches used for enhancing understanding during the consenting process. Data collection involved 15 qualitative, in-depth interviews with key researchers who were involved in obtaining informed consent from HIV infected individuals in Uganda for participation in pharmacogenetic clinical trials. The study explored two prominent themes: approaches used to convey information and enhance research participants’ understanding and challenges faced during the consenting process. Several barriers and facilitators for obtaining consent were identified. Innovative and potentially effective consenting strategies were identified in this study that should be studied and independently verified.
Background
Treatment of HIV/AIDS with antiretroviral therapy has drastically increased life expectancy for infected African populations, transforming a once highly fatal disease into a long-term condition (Ross et al., 2015). Anti-retroviral therapy is a life-long treatment and associated with a wide range of adverse drug reactions. The need for optimizing therapeutic responses and preventing adverse drug reactions has led to the growth of pharmacogenetic testing. Pharmacogenetic testing involves the “analysis of genes associated with drug targets, metabolism and other relevant pathways to predict drug effectiveness and/or likelihood of an adverse response for a given drug” (Haga and Mills, 2016: 1595). Host genetic variability has been shown to play a role in both antiretroviral drugs bioavailability and adverse effects susceptibility (Mayne et al., 2017). Pharmacogenetics is a relatively new field of research in Uganda and this means that very little is known about it, especially by laypersons from which research participants are usually drawn. Consequently, to facilitate adequate understanding of information that is provided to research participants during the process of obtaining consent, there is a need for innovative and effective approaches to participant education. The consenting process not only provides participants with relevant information to facilitate informed and voluntary decision-making, but also prepares them for receiving the findings of testing and enhances the likelihood of understanding the test results (Haga and Mills, 2016). Further, among other things such as respect for individuals’ autonomy and self-determination, an effective informed consent process is fundamental for avoiding the exploitation of research participants.
As the technologies used in the search for improved treatment and care for people living with HIV (such as pharmacogenetics research) are evolving, a unique set of ethical, legal, and social issues (ELSIs) are arising that require further exploration to ensure adequate protection of research participants, communities, and researchers (Adebamowo et al., 2018; Akinyemi et al., 2018; Eisenhauer et al., 2019; Mulder et al., 2017; Zhong et al., 2017). Navigating these unique ELSIs calls for a more robust consenting process beyond that which is employed in more familiar types of research. However, there is limited empirical research from sub-Saharan Africa regarding consent for genetics research (Haga and Mills, 2016; Tekola et al., 2009; Tindana et al., 2012). Empirical research suggests that researchers encounter several challenges in practice when obtaining consent from potential research participants, particularly in low resource settings (Tindana et al., 2006, 2012). There are concerns about research participants’ ability to understand the concepts of genetics research, sample storage for future use, and the potential risk of stigma or exploitation of study communities (Adebamowo et al., 2018; Marshall, 2004). This has partly been attributed to low literacy (Krosin et al., 2006), difficulties in translating scientific terms into local languages (Adebamowo et al., 2018), and difficulties with processing large amounts of information in a time-limited setting (Corneli et al., 2012). Literature has indicated that therapeutic misconception, whereby research participants believe that the research is being conducted primarily for their own benefit rather than for creating generalizable knowledge or the benefit of future patients, also poses a problem in some settings (Appelbaum et al., 2002; Dehority, 2021; Thong et al., 2016). A number of studies reveal poor understanding of genetics research by participants in resource-limited settings (Chokshi et al., 2007; Corneli et al., 2012; Marsh et al., 2010; Marshall et al., 2006; Masiye et al., 2017; Ogunrin et al., 2019; Tindana et al., 2012; Traore et al., 2015). Thus, since adequate comprehension of information is required for informed consent to be valid, it is imperative to inquire into how participants’ comprehension is being verified or can be enhanced by researchers. It is the responsibility of the researchers to ensure that the information is adequately understood by the participants. In an effort to fulfill this responsibility, researchers have come up with various innovative approaches for enhancing participant comprehension of study information, including enhanced written information, use of flyers and booklets (Falagas et al., 2009); multimedia tools and technologies such as audio-visual resources (Henry et al., 2009); oral information including altered counseling or dialog (Ellis, 2017) and face to face discussions (Sundberg et al., 2017); and the provision of quizzes that give immediate feedback (Bollinger et al., 2012; Sarkar et al., 2010).
The increase of genetics and genomics research in Uganda has led to some lurking concerns among researchers that participants continue to encounter challenges in understanding the information for informed consent, especially for complex genetic terminologies and concepts. Furthermore, from our experience we have noted that most technical terms have no direct translation and are thus difficult to explain in local languages. By exploring researchers’ experiences and practices in obtaining consent for pharmacogenetics research in Uganda, this study aimed to identify best and innovative practices for enhancing study participants’ comprehension of study information, and areas that may need further research and discussion. Though this topic is not new, it warrants further exploration in these settings because diverse cultures, beliefs, and value systems have a significant bearing on informed consent processes, particularly for genetics research (Adebamowo et al., 2018; Marshall, 2004). Results from this study may contribute to the development of a contextualized informed consent process that better enhances comprehension of consent for genetics research.
Methods
We adopted a qualitative research approach (Butterfield, 1989; Mays and Pope, 2000) that employed in-depth interviews to gain understanding of the experiences and practices of key research team members in obtaining informed consent for genetic testing in five ongoing pharmacogenetics clinical trials among HIV infected individuals. The study was conducted at the Infectious Diseases Institute (IDI) at Makerere University, Uganda from February to June 2018. The IDI is one of the leading HIV research organizations in Uganda and conducts a wide range of research including clinical trials, observational studies, diagnostic studies, genetics research, and also supports graduate research. The IDI supports nine HIV Care and Treatment Centers in Kampala, the Capital City. The key informants comprised of 15 research-team members who played a key role in informed consent processes in their respective studies. Key informants were purposively selected as follows: nurses (5), a nurse counselor, medical officers (6), and principal investigators in genetics research (3). Participants were selected and contacted directly because of their vast experience and expertise in obtaining informed consent for pharmacogenetics research. All research team members approached accepted the invitation to participate in the study. Data was collected using an interview guide that was developed by the authors and piloted on three graduate students who were excluded from the study. The interview guide explored researchers’ experiences and practices in obtaining consent for pharmacogenetics research, particularly with regard to research participant understanding of study information. All interviews were conducted by ME, NS, and one research assistant. At the time of the study, NS was a graduate student pursuing a Master of Health Sciences in Bioethics under direct supervision of ME, IC, and SN. The corresponding author (ME) is a bioethicist. The authors had a well-established relationship with all interviewees because they were all research team members affiliated to Makerere University. On average, interviews lasted between 45 and 60 minutes. All interviews were conducted in private offices at IDI.
Data analysis
All interviews were conducted in English, audio recorded, and transcribed verbatim. Field notes were also taken during the interviews. Debriefing meetings were held by the research team at the end of each interview to agree on the different perspectives that had been taken. Transcripts were not returned to interviewees for verification because of time constraints. Four of the authors (NS, KMD, NJ, and TA) developed a codebook and coding framework; disagreements were resolved via consensus. All transcripts were imported into NVivo 10 Software (2014) to manage and organize the data. Transcripts were then coded by three researchers (ME, NS, and TA). Data analysis and interpretation was conducted continuously throughout the study by three researchers (ME, NS, and OJ) using a thematic approach (Braun and Clarke, 2006; Fereday and Muir-Cochrane, 2006). The first step of the analysis involved reading all transcripts to familiarize, mark, and memo the data. We then performed open line-by-line coding to generate the first set of codes. The codebook was refined to identify themes in relation to participants’ practices in obtaining informed consent. Themes were supported by representative quotes.
Ethical considerations
This research was reviewed and approved by the Makerere University School of Biomedical Sciences Higher Degrees and Research Ethics Committee (SBS-524) and the Uganda National Council for Science and Technology (HS 199ES). Written informed consent was obtained from all participants prior to interview. All participants were assured of confidentiality.
Results
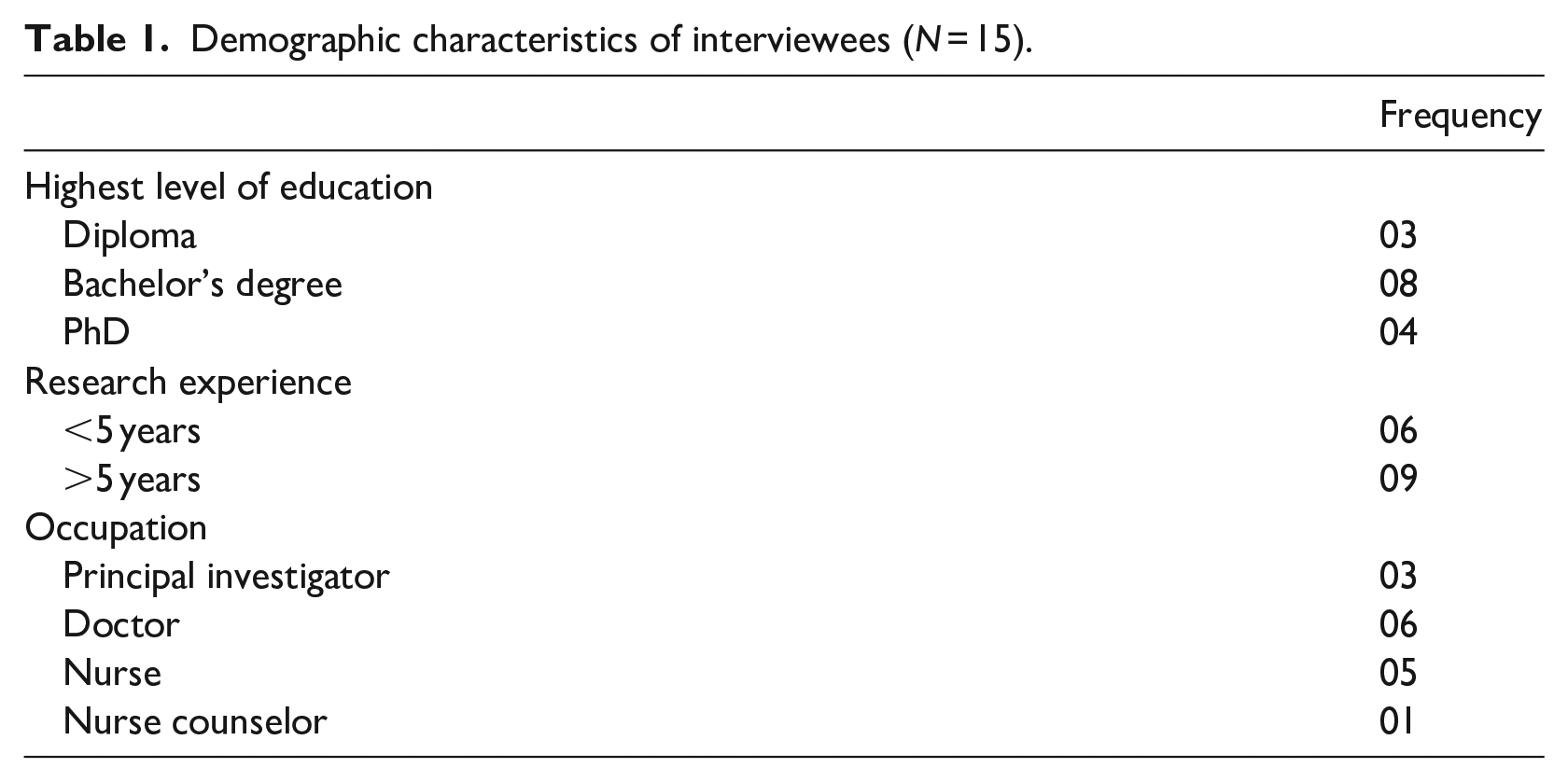
The majority of participants had attained at least a Bachelor’s degree (8); and had a research experience of more than 5 years (See Table 1).
Demographic characteristics of interviewees (N = 15).
The results of this study were summarized under two prominent themes: information delivery approaches and participants’ comprehension; and challenges faced during the consenting process.
Information delivery approaches and participants’ comprehension
The first theme describes the approaches used by researchers to convey study information to participants and how these approaches enhance participants’ understanding. Interviewees appreciated that pharmacogenetics is a new field of research in Uganda and that it is not well understood. They emphasized the importance of communicating with research participants in a language they understand well and are comfortable with. In addition, they indicated that the language should be simple, and the use of technical scientific jargon should be avoided. Instead, appropriate examples should be given to explain complex genetics concepts. Respondents opined that translation of consent documents into local languages facilitates comprehension during the consenting process: “It is actually very important to first find out the kind of language someone is comfortable with, then you use the simplest words possible. We avoid using scientific terms because most of the times these people don’t understand the scientific terms you’re using. . .” (KI 2, Nurse)
Both study nurses and doctors pointed out that most research participants prefer reading the consent forms together with their study doctor or nurse. They indicated that participants are given the opportunity to take consent forms home so that they can adequately study the information therein and if need be, seek the assistance or clarity from people they trust.
“We ask them, “do you want us to read together?, do you want to read alone?, or do you want to take the paper home?” so we give them options. So majority of them tell us “musaawo” [doctor] let’s read together; so you get the consent, if you have enough time for the day, we read sentence by sentence. However, if I don’t have enough time, I usually summarize each paragraph. I have noted that the longer you take reading for him/her, it becomes boring for the participants and me, and at the end of the day she’ll grasp nothing. So, in most cases we summarize the paragraph to explain the most important subject.” (KI 4, Nurse)
Another nurse agreed that at times the consent forms have a lot of information and require summarizing. She said this was necessary because, in her experience, the longer the consent sessions, the higher the chance of the participant becoming confused. Therefore, some study nurses do not read contents of the consent forms in their entirety. Instead, they deliver summarized information in a conversational and more interactive manner, based on the sub-headings in the consent form. Simplifying informed consent forms has also been shown to enhance comprehension of consent in genetics research (Hitchcock et al., 2020), particularly in settings with low literacy levels.
With regard to assessing participants’ understanding of study information, most interviewees reported that they use the “recall method.” Also known as “free recall” among educationists. In using this technique, the respondents (whose comprehension is being assessed) are “asked to retell everything that can be remembered” from the piece of literature they read or information provided to them in any other way (Clark, 1982).
Our interviewees indicated that this approach gives them a chance to correct any misconception that research participants might have about the study, and gives the research team an opportunity to offer a better explanation of concepts that participants might not have understood fully: “we use the recall method to assess their understanding, though it is not written on paper. . . we try to help them recall what we earlier discussed by asking questions on the purpose of the study, the procedures, the tests to be performed, etc. . . then we see how much they remember then we fill in the gaps and also correct any misconceptions or misunderstandings that may have been raised” . . .. (KI 6, Nurse)
Principal investigators indicated that employing nurses with prior genetics research experience enhances participant understanding. They pointed out that prior exposure to genetics research enables study nurses to grasp genetics concepts who can then communicate them effectively to participants during the consent process.
Interviewees indicated that they invite research participants who exhibit adequate understanding of genetics concepts to act as peer educators in the consenting process. Some of the participants, particularly those that have participated in several studies and developed a clear understanding of genetics concepts, are trained and routinely assist in the consenting process of fellow participants: “There are some volunteers who have been around for a number of years in the [Institute] clinic and have participated in the genetic studies before. We sometimes invite them for our trainings. They are very good at explaining to participants because they give live personal experiences which are very supportive and encouraging to the participants”. (KI 1, Doctor)
Some interviewees emphasized the need to develop innovative strategies for conveying vital information to enhance participant understanding. They highlighted several approaches they have used over time to explain genetic terms and promote comprehension of the genetics related information including: the use of video clips; cartoons, charts, and drawings to provide a visual interpretation of the information; and use of informative, stylized figurative drawings that generate certain mental images. Interviewees contended that the use of multiple information delivery approaches appears to engender clearer and longer-lasting cognitive impressions on research participants.
“I actually believe we can create better approaches to ensure that our participants understand the genetics concepts”. When ARV’s had just been introduced in our [Institute] clinic, we used things like cartoons to explain to the patients. We drew pictures of soldiers matching to war, and these represented the CD4 cells. Then we drew other groups of rebels to represent the HIV organism. And then we explained the support which the CD4 cells receive from the ARVs. . .. . .We can also use something like a lion is sleeping. . ..to represent undetectable viral load, and “the lion is awake to represent detectable viral load. . . we need to be creative to draw something that is very easy to understand and culturally acceptable.” (KI 15, Principal investigator) “We try to illustrate on a paper. It’s like teaching someone, the more you draw things on paper, the better that person understands. So you always have to be with a plain paper. If you’re like talking about how drugs move in the body and what happens while in the body, fine your diagrams may not be clear, but as you continue drawing this person later understands much more.” (KI 14, Nurse counselor)
Challenges to the informed consent process for genetics research
The second theme describes the challenges to the consenting process for genetics research. The challenges reported fell under three major categories: challenges on the part of study participant; research-related challenges and institutional-related challenges.
Participant-related challenges
Interviewees identified several participant related factors/variables that affect participants’ ability to adequately understand the information, thus posing a challenge to the validity of consent. Of these, low literacy level was mentioned by all interviewees as a daunting challenge to adequate understanding. Additionally, some interviewees indicated that the perception of genetic testing involves paternity tests which makes some research participants apprehensive about consenting to participate in these types of studies: “Our populations literacy levels are very low. Most of them assume that DNA is paternity testing and they may not understand what DNA is even if we use the Luganda word. It is a little bit hard. . . You will explain but she’ll keep nodding, but upon assessing his/her understanding you will real see that she or he has not understood much, not even up to 50%.” (KI 9, Doctor)
Other interviewees reported that many participants do not read consent forms; most of them are thought to be more interested in study procedures than reading consent forms in their entirety. This prevents them from adequately understanding the information provided: “Our reading culture is very poor. I don’t think they [participants] read the whole document themselves. They rely on the summary we give them. And lots of times they don’t really understand the objective of the study and other [consent] components if they don’t read. . .. I am sure most of them didn’t even know that they had consented for genetic testing. . .” (KI 9, Doctor)
Reluctance to read all the information can be related to the level of trust participants have in the doctors, who in some cases double as researchers. One principal investigator pointed out that some participants believe that their doctors (researchers) are in the best position to make decisions for them, particularly when it comes to sample storage and genetics research. This is not surprising because, over time, patients have developed trust in researchers and research institutions because of the ready availability and better-quality healthcare when compared with public health facilities. However, it is important to note that research regulatory guidance in Uganda recommends that doctors who provide routine clinical care to patients should not participate directly in the consenting process for research to prevent exploitation and coercion of patients.
Societal misconceptions and suspicion about the goals of foreign sponsored genetics research were also singled out as a hindrance to consent: “They get the right information at the enrollment stage but after interacting and sharing this information with their friends or relatives and when they come back for [follow up] visits, you find out that someone is really talking about the misconceptions and myths” (KI 4, Nurse) “One participant told me that she always feared joining a research study because she believed that the research brought into Uganda by the white man is intended to wipe away the black race,” she further asked, “why don’t they do this research among their own people?” (KI 14, Nurse counselor)
Research related challenges
One principal investigator highlighted the challenge of determining how much information would be adequate for disclosure to participants without confusing them, particularly in populations with low literacy levels: “My concern is that when it comes to ethics, it is hard to define what is “adequate” in regards to the information we should provide to our participants. It becomes complicated to balance between understanding and confusing the person at the end of the day because genetic information is usually very complex for a lay man.” (KI 10, Principal investigator)
The same respondent further argued that this is compounded by the lack of formal tools for assessing participants’ understanding of genetics concepts: “We do not have a formal assessment of understanding around genetics concepts.” Sometimes it may become embarrassing for the participant to realize they didn’t understand anything from the information provided. This may prevent them from fully opening up to the research team hence we may lose out on some vital information. (KI 10, Principal Investigator)
Issues concerning language were also cited as hindering the consent process. Interviewees indicated that language barriers between the study team and participants impact upon comprehension. They cited the lack of appropriate direct translations of genetics terms into local languages as a barrier to the accurate disclosure of information. This lack of understanding was thought to affect both participants and the study staff administering the consent.
Apart from the aforementioned issues, our interviewees revealed other challenges that negatively affect the process of consent. One such factor was the handling of genetics results. They noted that oftentimes participants expect individual genetics test results but in most cases these are not available. Some study nurses thought that this lack of feedback could be a demotivating factor for participants and equally frustrating for the research team. One study nurse recalled: “So sometimes they ask us, shall we get the results? And we are like no, we don’t have the machines here: we shall get the results: but we never given them the results. We are not giving feedback about their genetics.” (KI 8, Nurse)
Several interviewees highlighted the importance of returning results of genetics analysis to participants, particularly if the results have a bearing on patient medical care, but with prior genetic counseling. They also emphasized the need for letting participants decide whether or not to have their genetics results returned to them.
Institutional challenges
Interviewees also identified some institutional challenges that adversely affect the consent process. Two study nurses criticized the bureaucratic nature of the recruitment process and the long waiting hours participants have to endure before study enrollment. Specifically, they pointed out the practice of referral of patients from peripheral health units to IDI for study enrollment. They were of the view that these negatively affect the attention span of participants and their capacity to adequately understand and retain what is disclosed to them during the consent process. By the time they consent, many of them are too tired, hungry, and just want to complete the process and go home: “we recruit from the clinics from outside [Institute] and then refer them to IDI. For this particular study, they are pregnant women who have never started ART and by the time they reach [the Institute], they [participants] are frustrated, they are tired, yet they have to be started on ART that very day. According to the protocol, they have to be consented that day: the protocol does not accept to postpone. So the participants end up to be frustrated and at the end of the day, they don’t understand.” (KI 2, Nurse)
Discussion
This study explored experiences and practices of key research team members in obtaining informed consent for pharmacogenetics research and identified several barriers, facilitators, and challenges affecting the consenting process. It was not the first study to explore informed consent practices in HIV research in Uganda. In 2012, Ssali, Poland, and Seeley (Ssali et al., 2015, 2016) explored informed consent practices in two HIV clinical trials in Uganda where they interviewed various stakeholders about their experiences during the informed consent process. Unlike our study that focused on challenges to comprehension of informed consent and ways to enhance understanding during consenting, Ssali et al. (2016) mainly focused on informed consent procedures, with particular emphasis on the signing of the consent documents and the role of the independent witness. They argued that understanding of study information was not majorly influenced by participant literacy. However, this is contrary to our findings because low literacy came out as a strong barrier to the comprehension required for valid consent. This difference may arise from the fact that our study was specific to the understanding of genetics information which is regarded as difficult to understand for both investigators and research participants alike in low and middle-income countries (Chokshi et al., 2007; Marsh et al., 2010; Marshall et al., 2006; Masiye et al., 2017; Ogunrin et al., 2019; Tindana et al., 2012; Traore et al., 2015). None of the clinical trials investigated by Ssali et al. (2016) involved genetics or genomic procedures.
It has been noted elsewhere that obtaining consent for genetics and genomics research across Africa is complicated and very challenging, especially in populations with “ethno-linguistic barriers and low literacy” (Adebamowo et al., 2018). This is understandable partly because obtaining consent is not just a matter of providing relevant information; active promotion of understanding is integral to ensuring that the participant actually makes an informed decision. Even though it is now common knowledge that comprehension of study information by the study participants is a sine qua non for the validity of consent, interviewees in this study highlighted several barriers to adequate understanding. Further, the interviewees noted lessons from their experiences, particularly about how they attempt to mitigate existing challenges. Some ways to navigate challenges of comprehension noted in this study depart from traditional and more common methods of delivering study information. For example, the use of peer educators drawn from previous and current participants is worth emphasizing. Traditionally, researchers have relied upon study team members, including research assistants, to deliver study-related information to participants but the respondents in this study suggest that sometimes experienced study participants can communicate the information better as peer to peer. Potential fears around the practice of using lay-persons to communicate technical information to their peers can be allayed by including peer educators in training sessions; this has proven to act as a reasonable safeguard against potential distortions. Potential concerns wane even further when peer educators act under the guidance/supervision of the technical personnel.
The use of visual and audio interfaces to explain highly technical and complex concepts that cannot easily be explained using literal and verbal means, also proved useful. Even though some of these approaches have been used elsewhere and in other fields, the manner in which they are being used in this setting appears to be quite novel. For example, one respondent indicated that delivering the information through drawings, trying to depict what is being said, even haphazardly, seems to enhance participants’ understanding better than mere words.
Another suggested potential divergence from more traditional means of delivering information involves assessment of when it is appropriate to read the whole consent document to the letter and when to summarize such information to deliver it in a conversational and more interactive manner. This can make a critical difference, given that some participants arrive at the study center tired and unable to concentrate well during the long consenting process. Limited attention span affects comprehension and retention of the delivered information. Further, there were concerns about participants’ lack of interest in reading lengthy documents. Consequently, summarizing and delivering information in a conversational manner seems to be a reasonable solution for these challenges.
These adaptions are critical for all research, but even more important for pharmacogenetics research in Uganda. This contention is based on one of the most emphasized concerns by our interviewees: unlike other old and familiar fields of research, pharmacogenetics is a new field of research in Uganda and is not yet well understood by either the research staff or participants. The novelty of this field, and the associated unique ELSIs, suggests that traditional approaches to seeking consent are may not be adequate for genetics research participants. As mentioned by some of the interviewees, we appreciate that some of these improvised approaches have not yet been widely used, independently verified, systematized, and standardized. Consequently, we recommend further rigorous studies for wide use of such approaches in research.
In our closing remarks, we note that another important revelation to reflect upon is that people can lack interest in reading consent documents. However, our findings suggest that research participants do not necessarily need to read the entirety of the consent documents to achieve adequate comprehension. Indeed, some study participants prefer to receive summarized information that is delivered to them in a conversational and a more interactive manner; others seem to understand better when such information is delivered to them using audio and visual means. Researchers need to be flexible and reflexive enough in the way they think and go about the consenting process in genetics research (Barugahare, 2019). Since the reading of the study-related information to the letter is not the only, and arguably not the best, means of ensuring comprehension and retention, especially amidst people with low literacy levels, researchers should not worry so much about lack of interest to read. There are sufficiently effective alternatives; with or without reading, there are ways of ascertaining comprehension, for instance, via free recall, and researchers can take steps to close comprehension gaps, if any, thereafter.
Further still, it needs to be emphasized that participants can have many worries about taking part in genetics research (Masiye et al., 2017). People can have pre-existing prejudices and beliefs with regard to research involving genetics procedures and bio banking that may influence their decision-making and hinder adequate understanding during the consent process (Furr, 2002; Gollust et al., 2012; Isler et al., 2013; Jegede, 2009). Some interviewees expressed their discomfort with foreign funded genetic research. This perception probably stems from the historical inequality and exploitation of researchers and research participants from the global south in collaborative research (Munung et al., 2017; Sathar et al., 2014). It is therefore important that participants are given ample time (more than usually given in the case of more established and familiar fields of research) (Ssali et al., 2015) to adequately understand before consenting to participate in genetics research. Although it did not come out clearly in this study, we recommend robust community engagement processes through which adequate community sensitization can be undertaken to dispel misconceptions and negative prejudices about genetics research. This will help to ensure that the public adequately understands the goals, nature, procedures, risks, and benefits of the study before its implementation. Understanding community cultural values and potential concerns fosters public trust, mutual collaboration, and acceptance from communities (Adebamowo et al., 2018) which are vital for valid informed consent.
Conclusions
For any consent to be valid, research participants should adequately understand all relevant information about the study. This can be particularly difficult to achieve for studies involving new technologies. The results from our interview study about obtaining consent for pharmacogenetic testing from HIV positive research participants is broadly in line with the literature, with three exceptions. First, literacy levels do matter in terms of achieving consent for genetic testing. Second, peer educators who obtain consent together with research team members can offer an excellent means of enhancing understanding of study content. Third, flexible approaches and innovative methods for obtaining consent can lead to better understanding than more traditional literature-based methods. This finding warrants further study and independent verification.
Footnotes
Authors’ contributions
This article is part of NS’s dissertation for the partial fulfillment of the requirements for the award of a Master of Health Sciences in Bioethics. NS and ME developed the concept and designed the study. This work was supervised by ME and IC from proposal development, study implementation to manuscript writing; ME, KMD, NJ, BJ, and TA participated in data collection and qualitative analysis. ME, NS, SN, and NF participated in the interpretation and discussion of the data. NS and ME drafted the manuscript with substantial contribution from all authors. All authors read and approved the final version of the manuscript (and any substantially modified version that involves the author’s contribution to the study).
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]()
Research reported in this publication was supported by the National Human Genome Research Institute (NHGRI) of the National Institutes of Health under Award Number U01HG009810 and the International Health Research Training program (IHRET) under Award Number 5R25TW009730-05. The IHRET grant awarded NS a scholarship to pursue a Masters’ Health Sciences in Bioethics training program; and contributed to the design of the study. NHGRI supported the design of the study and collection, analysis, and interpretation of data and in writing the manuscript. NS is now a PhD student on the Makerere University International Bioethics Research Training Program award number D43TW010892 supported by Fogarty International Centre of the National Institutes of Health.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical approval and consent to participate
This research was reviewed and approved by Makerere University School of Biomedical Sciences Higher Degrees and Research Ethics Committee (SBS-524) and Uganda National Council for Science and Technology (HS 199ES). Written informed consent was obtained from all participants prior to interview. All participants were assured of confidentiality.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.