
Abstract
Monitoring of clinical trials is important to ensure adherence to protocol, to safeguard the rights of research participants and to achieve compliance with principles of good clinical practice. Recent regulatory changes in India require Ethics Committees to keep an oversight of ongoing clinical trials including on-site monitoring. In this article, we share the experience of on-site monitoring of clinical trials by the Ethics Committee of a tertiary care, academic and research centre in India. We found a large number of shortcomings in the areas of informed consent, adverse events, insurance and reimbursement, which would not have been detected by off-site document review. Interestingly, many shortcomings were also not detected by on-site monitoring arranged by clinical trial sponsors. We therefore conclude that on-site monitoring of ongoing clinical trials is a highly important activity for Indian Ethics Committees.
Introduction
Good clinical practice (GCP) is an international ethics and scientific standard for clinical trials involving human participants. Its stated purpose was to improve patient protection and data integrity. The GCP guidelines were first introduced in 1997, since then the monitoring of ongoing clinical trials by Ethics Committees (ECs) has been formalized: 3.1.4 The IRB/IEC
1
should conduct continuing review of each ongoing trial at intervals appropriate to the degree of risk to human subjects, but at least once per year (E6 R2 Good Clinical Practice Guideline).
GCP does not specify whether the clinical trial review should be performed off-site, on-site or both. The GCP guidelines were initially developed for use by European countries, Japan, the United States, Australia and Canada. Yet, Indian law also requires that clinical trials conducted in India need to abide by GCP (CDSCO, Central Drugs Standard Control Organisation). In addition, the same requirement for ongoing monitoring of clinical trials can also be found in the Indian National Ethical Guidelines for Biomedical and Health Research involving Human Participants (ICMR), which state: ECs [Ethics Committees] are entrusted with the initial review of research proposals prior to their initiation, and also have a continuing responsibility to regularly monitor the approved research to ensure ethical compliance during the conduct of research.
Over the recent decades that ECs have provided appropriate review and oversight, the severe consequences for human participants involved in research have been drastically reduced. The ‘scarcity of contemporary examples [of severe consequences] demonstrate that regulations for the protection of humans participating in research have evolved in a way that minimizes the probability of harm’ (White, 2020). An ongoing real-time monitoring by an EC can be instrumental in guiding research towards following ethical principles. Efforts ‘should be taken to identify and manage ethical issues as early as possible in order to provide ethical guidance throughout the entire research process, and mitigate negative effects, harms and wrongs’ (Sugarman and Bredenood, 2020)
How does the monitoring of clinical trials by ECs work? Most ECs require the principal investigators to submit annual reports of their ongoing projects to the EC. These reports are then examined by ECs off-site. In addition to these annual reports, ECs also review protocol amendments and serious adverse event (SAE) reports and notifications. However, off-site monitoring may be inadequate as it may miss protocol violations, misreporting or discrepancies in consent administration and records thereof, to give some examples. At the same time, on-site monitoring by ECs does not seem to be a common practice and there are very little published data (Davis, 2018; McCusker et al., 2001; Ochieng et al., 2013; Bediako and Kaposy, 2019; Shetty et al., 2012).
The purpose of this article is to document our observations made during on-site monitoring conducted by our EC. A secondary aim was to check the adequacy of monitoring conducted by the sponsor of a clinical trial.
Overview of approach
This article reports on the findings of a systematic investigation of experiences of on-site monitoring by an EC based at a tertiary care institute in North India. In India, tertiary care is usually provided in large hospitals with access to specialist medical care, which also provide research and training facilities. The EC of the tertiary care institute reviews protocols submitted for research with human participants. These protocols can also cover research funded from external sources such as sponsor initiated drug and vaccine trials.
To adhere to GCP and the Indian National Ethical Guidelines for Biomedical and Health Research involving Human Participants, a sub-committee of the EC was formed to conduct on-site monitoring of research. The sub-committee prepared standard operating procedures (SOPs) for on-site monitoring, which were discussed and approved by the parent EC.
The following steps were undertaken, following the SOPs:
• The five members of the monitoring team familiarized themselves with the study protocol.
• The team was introduced to the research team, which was to be monitored.
• The monitoring process itself focussed on three important aspects: Documentation and record keeping, Participants’ rights and compliance with the protocol and Storage and access of trial supplies.
Documentation and record keeping
The Trial Master File was checked for completeness and being up-to-date with respect to EC approvals, insurance documents, clinical trial agreements and various logs such as duty delegation and monitoring of SAEs. Depending on the number of participants, a decision was made either to randomly see files containing records of participants or to see all of them.
Participants’ rights and compliance with the protocol
The files were also examined for consent forms, case record forms, source document validation, compliance with EC reporting requirements, reimbursement to participants for visits as approved by the EC and compensation for SAEs, if applicable, to ensure participants’ rights are respected.
Storage of trial supplies and access to trial-related supplies
The main EC sub-committee work in this area were temperature logs checked against specific temperatures needed for storage.
All findings were recorded by a stenographer who accompanied the monitoring team. The sub-committee submitted its monitoring report to the full EC for deliberations, suggestions regarding further action to be taken and ratification. Finally, the principal investigator was provided with a report from the EC.
This article summarizes the findings of on-site monitoring to highlight the most common GCP violations. This is conceived as a learning opportunity for those conducting clinical trials as well as ECs monitoring clinical trials on-site.
Monitoring details
Over a period of three years, the sub-committee conducted on-site monitoring of 14 studies. Ten of these clinical trials were multinational and four were multicentric with all centres being in India. While the majority of the studies were sponsored by the pharmaceutical industry, two studies were funded by the Indian government. One of the studies was sponsored by a government funding agency with trial management and monitoring being outsourced to a Contract Research Organization. The studies were mostly confirmatory clinical trials, 2 two studies were proof-of-concept studies for a new indication of an already approved agent and one was a pragmatic study for a new dosing regimen. For the purpose of confidentiality, we are abstaining from detailing other features of the studies.
GCP violations and other discrepancies discovered during on-site monitoring
The major findings of our study of 14 clinical trials are shown in Table 1 organized into area of discrepancy (e.g. consent) and type of discrepancy.
GCP discrepancies identified by on-site monitoring.
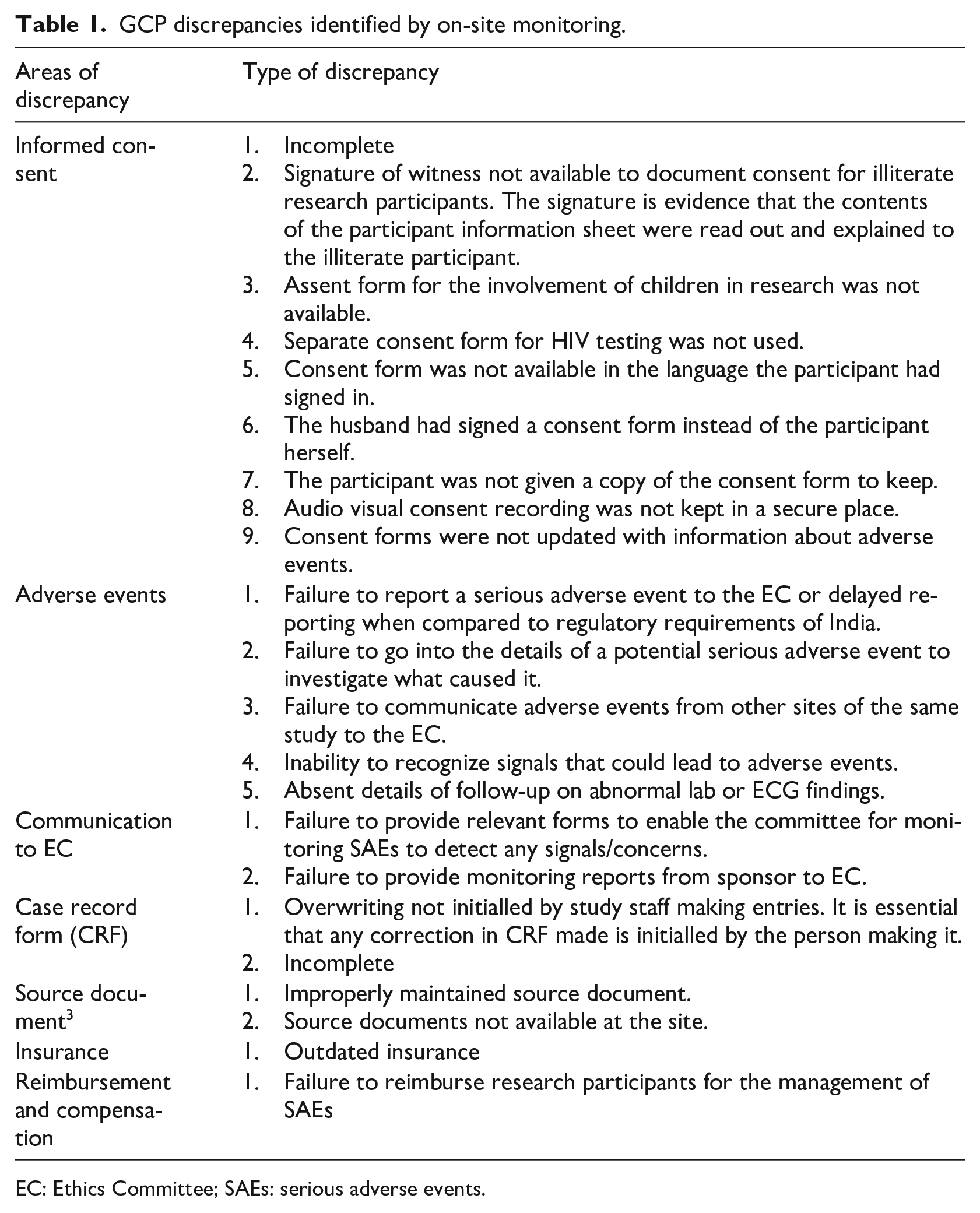
EC: Ethics Committee; SAEs: serious adverse events.
Discussion
Protection of research participants is the major responsibility of the EC. On-site monitoring is one possibility to achieve this protection (Pickworth, 2020). Our on-site monitoring of ongoing clinical trials discovered several issues that may not have been detected by off-site review of annual reports alone.
Similar studies discovered protocol violations, including problems with the informed consent process, missing signatures of participants/investigators/witnesses and delayed reporting of SAEs (Ochieng et al., 2013; Pickworth 2020; Shetty et al., 2012; Smith et al., 1997). Noticeably, informed consent related issues have been raised universally by all the papers. While the entire lack of informed consent documentation (Ochieng et al., 2013; Shetty et al., 2012) was not a concern in our case, other issues emerged. For instance, although decisions regarding healthcare of females can be heavily influenced by family members (Lobato et al., 2013), the practice was uncritically extrapolated to informed consent processes in an Indian clinical trial. This is a cause of major concern since the ethical principles of voluntariness, autonomous decision making and transparency are implemented through informed consent processes. Without wanting to repeat the findings as presented in Table 1, we want to concentrate on the following additional points here:
Is on-site monitoring conducted by the sponsor of a clinical trial adequate (our secondary study aim)?
Are there ways to make on-site monitoring less costly?
Can on-site monitoring be seen as excessive policing that stops valuable research?
Is monitoring conducted by the sponsor of a clinical trial adequate?
For the majority of trials, on-site monitoring had already been undertaken by the sponsors’ representatives (Clinical Research Monitor (CRM)). The GCP violations and discrepancies discovered by the sub-committee were detected despite earlier monitoring visits by CRMs. There could be several reasons for this. It may be that not all CRMs possess sufficient expertise, experience or training in terms of monitoring. CRMs are typically very well versed with the documentation aspect of monitoring and devote most of their time to checking the completeness of documentation and matching entries with the source document. While this is important, it is also important to check things that may not have been recorded. For instance, in one of our cases, a potentially missed SAE was tracked by medications prescribed to the patient. In this context it is important to note that members of the sub-committee were medical professionals with training in GCP and experience in conducting clinical trials themselves. Hence, they were able to make medical observations relevant to the well-being and protection of research participants. Another example where a medical background was useful and where CRMs missed a GCP violation was a mismatch between recruitment and inclusion and exclusion criteria. Given that the sub-committee discovered considerably more GCP violations than the CRMs, models may be required, as suggested by the Clinical Trials Transformation Initiative, to improve GCP training (Arango et al., 2016).
Are there ways to make on-site monitoring less costly?
Indian ECs face a large number of challenges especially those reviewing clinical trials, which have risen steeply (Kadam and Karandikar, 2012). Most challenges are resource related, such as insufficient training and insufficiently varied expertise on existing ECs (Kadam and Karandikar, 2012). On-site monitoring adds yet another resource-related issue to already stretched ECs.
In this context, the concept of ‘risk-based monitoring’ has been developed emphasizing source document verification (SDV) (Ansmann et al., 2013; Smith et al., 2014). SDV helps in checking if the data in case report forms matches with the source data to ensure the accuracy, reliability and completeness of the data. The cost effectiveness of undertaking SDV for 100% of research participants is not ideal (Andersen et al., 2014). More recently tiered approaches were suggested, which included a consideration of risks (Baigent, 2008). In these approaches only a certain percentage of SDVs were being looked at if prior monitoring visits were satisfactory. Conversely, a higher percentage of SDV was checked at sites that performed poorly during prior monitoring visits (Baigent, 2008). This may be a way forward to deal with resource constraints, as long as checking SDVs is still undertaken. Checking SDVs is an important method for analysing information that may not get captured in Case Report Forms, particularly those that are likely to reflect on patient safety and investigator’s involvement in the trial. For instance, the study objectives do not require capturing data about vision and a participant may inform the physician investigator about occasional flashes of light, which the physician investigator then records in the case file. But since there is no specific column in the case record form for this, it may get missed.
It is also important, in terms of good resource management, to have a clear distinction between on-site and off-site monitoring. For what types of research on-site monitoring should be mandatory, desirable or not needed needs to be clarified. The current guidelines are not very clear on the oversight mechanisms to be followed. In the context of resource constraints, it is also important to remember that most EC members have other responsibilities—patient care, research and administrative duties.
Can on-site monitoring be seen as excessive policing that stops valuable research?
There have been concerns that increasing intervention by ECs can be seen as excessive ‘policing’ that could hinder research (Makhoul et al., 2014). Our experience was different as most investigators were only too happy to have discovered deficiencies well in time and immediately took steps to rectify problems. What is more problematic is what the EC should do when it discovers violations of GCP (in other words, what it should do as a result of the ‘policing’). In the worst case, a trial can be stopped but this should be a last resort. A step-wise approach is sensible, which also aligns with the ECs policies on follow-up for monitoring.
Conclusion
On-site monitoring of ongoing clinical trials is a relatively new EC practice in India. Our research showed that it is a highly important activity. On-site monitoring detected GCP violations that were missed by off-site monitoring and also by monitoring arranged through trial sponsors. How the time-consuming and costly on-site monitoring can be undertaken effectively when Indian ECs already face resource constraints remains to be determined.
Footnotes
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]()