
Abstract
The COVID-19 pandemic has brought unprecedented, major challenges to the ethical conduct of research including challenges for the rapid and robust ethical review of biomedical research. The Indian Council of Medical Research’s “National Guidelines for Ethics Committees Reviewing Biomedical and Health Research during COVID-19 Pandemic” aim to assist ethics committees in this time of crisis, whilst simultaneously protecting researchers and research participants. Whilst ethics committees are encouraged to approve studies rapidly, the Indian guidelines also make clear that no shortcuts will be taken. Informed consent must be obtained innovatively, but cannot be dispensed with. Vulnerable people should only be involved in clinical research that is relevant to their health needs. Approaching communities for research also requires new, trust-building methods, given that healthcare workers and researchers have been assaulted during their COVID-19 research. Importantly, the media must carry their share of responsibility and avoid spreading fake news. From an Indian perspective, the question of whether we are sitting on a volcano that might erupt at any time causing more damage than we ever expected is currently unclear. Only global collaborative efforts will help to tide over in the present crisis.
Introduction
In May 2018, the Nipah virus infection was detected in 23 people in Kerala, India. Twenty-one of them died (Plowright et al., 2019). Like SARS-CoV-2 virus, Nipah is a zoonotic virus, which normally exists in animals (most notably bats and pigs) but can also be transmitted to humans, as well as between humans. Although there have been relatively few known outbreaks of Nipah virus in Asia, it causes severe disease and has a fatality rate of 40%–75%. As a result, it is a serious concern to public health (World Health Organization, 2016, 2018). Hence, India—unlike many other countries—has experience with zoonotic viruses that cause a severe threat to human beings.
Research is of paramount importance in the fight against serious threats to public health. Firstly, research can contribute to solutions, such as treatments or vaccines. Second, research can inform institutional and individual responses to such threats. Third, research can inform plans on how to handle future episodes of threats.
In India, lessons learned from the containment of the Nipah virus in Kerala (Arunkumar et al., 2019; Kumar and Kumar, 2018) have improved preparedness for dealing with COVID-19. The national machinery to tackle the coronavirus came into action immediately with lockdown, social distancing, isolation, and quarantine—never experienced before in India, a country with a population of 1.3 billion.
Research has to remain ethical whether or not a country faces a serious threat to public health. Even in humanitarian emergencies, the rights of individuals not to be exploited and to be treated ethically remain. The Ebola crisis in Africa was an eye opener for the planning of emergency research and ethics. It revealed just how difficult it is to provide guidance with regard to medical practice and research in such difficult circumstances. As a result of the spread of the Ebola virus, the World Health Organization (2016) published its “Guidance for Managing Ethical Issues in Infectious Disease Outbreaks.”
In 2006, ethics review of research on disaster management was addressed briefly in the revised Ethical Guidelines of the Indian Council of Medical Research (ICMR, 2006). This was further elaborated as a separate section on humanitarian emergencies and disaster research in the “National Ethical Guidelines for Biomedical and Health Research Involving Human Participants” (Indian Council of Medical Research, 2017). While much has been learned from experience with other infectious diseases like Ebola, Nipah virus, and HIV, the COVID-19 pandemic has ushered in a new phase globally.
This pandemic’s onslaught on humans and health systems has raised multifaceted and unprecedented ethical challenges for reducing morbidity and mortality, which have caused great human suffering and great economic losses. Numerous matters about how the rapid design, conduct, and review of research can and should be tackled, within the context of a devastating global pandemic, need to be resolved. Furthermore, while the restrictive lockdown measures are essential for disease containment, this environment raises significant practical challenges for researchers and ethics committees (ECs) about the conduct of research and appropriate review procedures. Ethics preparedness during humanitarian emergencies such as the current pandemic is an essential requirement to enable appropriate research (Mathur, 2020).
The response in India has been to develop new and bespoke guidance for ECs to assist them with their routine functions as well as the new challenges generated by the COVID-19 pandemic. In April 2020, the ICMR released the “National Guidelines for Ethics Committees Reviewing Biomedical and Health Research during COVID-19 Pandemic.” (ICMR 2020) While regulators have facilitated the fast track approval of drugs for the treatment of COVID-19, this needs to be preceded by fast track and effective ethics review of research. The new guidance is intended for researchers and EC members and considers how to set priorities in the conduct and review of research so urgently needed.
The remainder of this article summarizes the Indian approach to conducting ethical health research during the COVID-19 pandemic.
Addressing the primary challenges for ethical research in India
The threat of infection from the coronavirus, and the associated implementation of lockdown restrictions and social distancing, have implications for research at all stages from review to conduct, reporting, evaluation, and dissemination. While it is not possible to describe all the challenges in detail, the following is intended to provide a snapshot of major topical concerns for research ethics in India and what the new guidelines have to say about them. An overview is provided in Table 1.
Main Ethical Issues for Indian ECs during COVID-19.
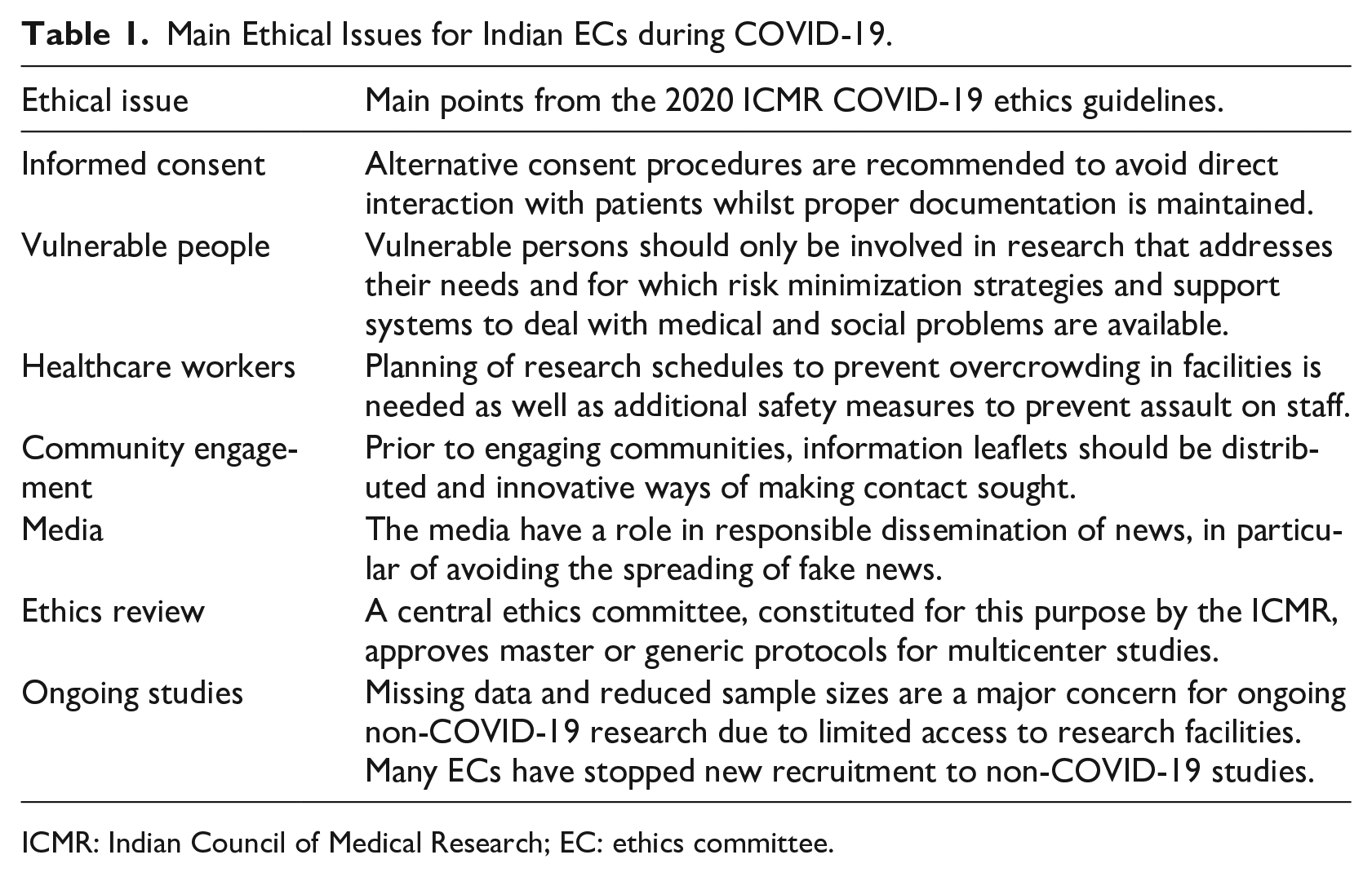
ICMR: Indian Council of Medical Research; EC: ethics committee.
Informed consent
Informed consent for clinical studies in India can pose complex challenges at the best of times. Issues such as language barriers, therapeutic misconceptions, cultural and religious differences, and trust in the medical system (Nijhawan et al., 2013) require careful consideration by researchers and ECs. Now, in a time of lockdown and social distancing, it is impossible for researchers to use their customary, tried, and tested methods for seeking consent. COVID-19 patients may be very unwell and/or kept in quarantined environments with access permitted only for healthcare workers. It can also be difficult to gain consent from legally authorized/acceptable representatives (LARs) because they are not allowed inside the healthcare premises either.
The new guidelines recommend that alternative procedures to avoid direct interaction with patients be explored. However, the importance of proper documentation is emphasized. Electronic consent can be a suitable method if the participant and/or their LAR is conversant with the technology. However, most of the ECs in India are not confident about obtaining informed consent through digital means. Furthermore, the privacy and security features of a virtual tool pose ethical challenges.
An alternative means of obtaining consent might therefore involve frontline healthcare workers who have access to the COVID-19 restricted zones. At the same time, this extra burden on overstretched frontline workers is an ethical issue in itself and it increases the risk of therapeutic misconceptions. It has also created a problem, never before experienced to this extent, of assault on healthcare workers. In India, a traffic light system is being used to distinguish between districts with higher numbers (red zones), lower numbers (amber zones), and no cases (green zones) of COVID-19. Government healthcare workers are conducting surveillance work in red zone areas, which has generated fear and suspicions, and has resulted in instances of resentment and assault on healthcare workers (Deccan Herald, 2020). This bodes very ill for researchers accessing potential research participants outside of hospitals in those red zones. Yet, some approved research projects, for testing of traditional remedies as a prophylaxis against COVID-19 under the aegis of the Ministry of AYUSH (Ayurveda, Yoga, Unani, Siddha, Sowa Rigpa and Homeopathy), which have also required visits to red zones, have encountered no resistance in obtaining written consent. This is likely due to the greater acceptance of traditional remedies. The situation in the red zones highlights the need for trust, education, and community engagement (refer to section on “Community engagement” later in the article).
Vulnerable people
Vast numbers of people in India who would have already been considered as vulnerable in research, now bear significant additional burdens.
It is common knowledge that the private sector is the dominant player in the healthcare arena in India. Almost 75% of healthcare expenditure comes from the pockets of households, and catastrophic healthcare cost is an important cause of impoverishment. (Kasthuri, 2018: 142)
A disease such as COVID-19 combines the economic costs of social distancing with the potential need of out-of-pocket payments for healthcare or hospitalization. In these situations, any possibility of access to healthcare through research opens the possibility of undue inducement (Srinivasan, 2010), which ECs need to guard against.
To address the above concerns, the 2020 ICMR COVID-19 ethics guidelines recommend additional safeguards for vulnerable participants which include ensuring that the involvement of vulnerable persons is justified fully because the research will address their needs; the implementation of risk minimization strategies; and the establishment of support systems to deal with associated medical and social problems.
Healthcare workers
At the same time, the coronavirus infection has no respect for economic or social status; one group that is particularly vulnerable to infection, due to the larger possibility of exposure, are healthcare workers and possibly the researchers themselves. These groups do not have the option of social distancing and rely upon health administrators to supply personal protective equipment (PPE), prophylaxis, and other facilities. “India, like most parts of the world, is in a race against time to procure personal protective equipment (PPE) for the safety of its medical teams fighting to halt the spread of coronavirus” (Pandey, 2020: np).
For healthcare workers and researchers, the 2020 ICMR COVID-19 ethics guidelines recommend additional precautions. These include the planning of research schedules to prevent overcrowding in facilities, the provision of protection gear/PPE to research facilities, psychosocial and emotional support, and additional safety measures to prevent assault on staff.
Community engagement
Trust in research can be eroded significantly when both the print and the visual media seek to sensationalize news and social media outlets aid the rapid spread of fake news. According to Palit (2020), social media in India have been “hyperactive” in the spreading of inaccurate and unverified information. There is a flood of misleading claims and inaccurate information, which adds uncertainty to already heightened levels of fear. In these situations, community engagement is essential.
The “Global Code of Conduct for Research in Resource-Poor Settings” (2018), stipulates that local communities and research participants should be included throughout the research process, from planning through to post-study feedback and evaluation, to ensure that their perspectives are fairly represented and also aligning with “Good Participatory Practice.” Public and community engagement improves responsiveness to local health needs and encourages public trust in research. This, in turn, improves community confidence and willingness to participate fully in research. However, understanding of the community dynamics and effective engagement is extremely challenging in a lockdown situation with social distancing, isolation/quarantine requirements, and restricted/absence of public transport systems.
The 2020 ICMR COVID-19 ethics guidelines emphasize the need for preparation and dissemination of public educational materials prior to approaching communities. Additionally, researchers are encouraged to employ innovative measures for contact and communication as direct contact with the research participants is risky and could result in harm (see also the potential for assault on healthcare workers covered earlier in this article).
Media
The 2020 ICMR COVID-19 ethics guidelines also suggest that efforts should be made to prevent the spread of fake news. While researchers might be able to promote the dissemination of verified information, which addresses fears to some extent, the media must also play their part. Media outlets must take a more responsible role to banish fake information from their platforms. (SpringM 2020)
Ethics review
Ethics committees have a vital role in the review of COVID-19 studies during the outbreak, especially intervention studies that might cause physical injury to patients. Ethics committees need not only to improve the review efficiency, but also to make sure the standard of ethical review is not relaxed. (Luo and Qin, 2020: m1369)
Whilst the 2020 ICMR COVID-19 ethics guidelines fully agree that ethical review must not be compromised to protect Indian research participants, it is also important to expedite review. For fast track ethics review of research protocols, the guidelines recommend ad hoc virtual meetings to secure ethics approvals faster. However, many EC members are not conversant with the required virtual technologies and network connections can be unstable due to heavy dependence on the internet during lockdown. This can hamper the smooth functioning of the EC. Despite their best efforts, some EC members are not able to participate due to technological issues and ECs must rely upon members who have access to stable connections and knowledge of the relevant virtual meeting platforms.
Due to time constraints, and the urgent need for results, many COVID-19 projects are being conducted as multicenter studies to obtain the desired sample sizes in the shortest period of time. For multicenter studies, the 2020 ICMR COVID-19 ethics guidelines encourage review by one designated EC for approval at all the sites to facilitate rapid review. Indeed, a central ethics committee, constituted for this purpose by the ICMR, for proposals initiated or coordinated by the National Task Force for COVID 19 research, is approving master or generic protocols. The guidelines also suggest that local ECs can accept the decision of the designated committee or they can opt to conduct their own rapid review if there are site-specific issues which require attention. The onus of monitoring the approved studies lies with the local ECs.
Challenges for ongoing studies
The COVID-19 pandemic has many and varied impacts upon ongoing studies, including recruitment and the safe continued involvement of participants.
Principal investigators (PIs) working in hospital settings might become infected or preoccupied with the coronavirus patients. The 2020 ICMR COVID-19 ethics guidelines encourage that persons are designated to replace PIs to ensure smooth continuation where and when required.
If patients feel reluctant to visit the research site because of fear of contracting the coronavirus or due to the existing restrictions for travel, an alternative safe place is agreed for the clinical assessment or follow-up for scheduled investigations. However, not all patients can comply with this, leading to missing data and reduced sample sizes, a major concern for ongoing research. Access to facilities for either routine or specified testing of samples can also be difficult or impossible because the facilities are being used for testing related to COVID-19.
Although the 2020 ICMR COVID-19 ethics guidelines state that suitable measures should be put in place for ongoing studies, the reality is that many ECs have stopped new recruitment for such studies. In addition, when large numbers of non-COVID-19 studies are allowed to continue, researchers are forced by pandemic-related restrictions to make protocol deviations. For instance, visits have been replaced by phone call follow-ups.
Conclusion
The COVID-19 pandemic has brought unprecedented, major challenges to the ethical conduct of research including challenges for the rapid and robust ethical review of biomedical research. No other humanitarian emergency to date posed similar global concerns to all research stakeholders. Governments around the world are trying their best to put in place sound governance mechanisms for urgently needed research. The coordinated efforts of all the Ministries of the government of India are trying their best to keep the pandemic under control.
The Indian Council of Medical Research’s “National Guidelines for Ethics Committees Reviewing Biomedical and Health Research during COVID-19 Pandemic” is one such effort. Ethics committees, which are themselves under pressure from lockdown measures, are encouraged to be innovative in their support for researchers; to approve studies rapidly but simultaneously ensure that informed consent is not endangered; that vulnerable people are only involved in research that is relevant to their health; that healthcare workers are protected, including from assault; that communities are approached in such a way that they can build trust with researchers; that the media accept their responsibility for avoiding fake news; and that researchers whose ongoing studies suffer from missing data and low sample sizes are supported.
The road to normalcy being remote, all the recent changes made in the system may become the new normal for the future. It is difficult to predict whether the situation for research will stabilize soon or whether we are sitting on a volcano which can erupt at any time causing more damage than we ever expected. Only global collaborative efforts will help to tide over in the present crisis.
Footnotes
Acknowledgements
Thanks to Dr Kate Chatfield and Prof. Doris Schroeder for comments on earlier drafts.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]() .
.