
Abstract
Background:
Despite growing evidence that participation in psychological trauma research is well tolerated by children and parents, ethics boards may voice concerns regarding research with families with recent acute trauma exposure. Factors impacting child and parent experiences of research participation are not well documented, particularly for methodologies including observational components.
Objectives:
This study describes child and parent perceptions of research participation involving an observational task following an acute traumatic event and explores potential relationships between research experience and selected demographic factors (race/ethnicity, sex, age, prior trauma exposure), and post-traumatic stress symptoms.
Methods:
As part of a larger study on the role of biopsychosocial factors in post-traumatic stress symptoms, 96 child–parent dyads (ages 8–12 years, M = 10.6) participated in a three–time point study following hospitalization for pediatric injury. At baseline, children and parents completed measures of reactions to research participation, post-traumatic stress symptoms, and trauma history. Measures of post-traumatic stress symptoms were repeated at 6- and 12-week follow-up assessments.
Results:
The majority of families reported they were glad they participated in the research study (61% children; 72% parents) and felt good about helping others (74% children; 93% parents). Negative feelings were uncommon (<10% of families). Perceptions of participation were not related to race, sex, or trauma history, but child age significantly factored into trust of the research team and informed consent (Spearman’s ρ = .289, p < .01). Reactions to research were not significantly related to child or parent post-traumatic stress symptoms at any time point.
Conclusion:
Current results extend past research to suggest that most children’s and parents’ research experience is positive, even when completing an observational task during hospitalization for an injury. Children under the age of 10 years may perceive their participation as less voluntary, supporting prior findings that additional steps be taken to ensure their understanding of their choice in participation.
Keywords
Introduction and background
Over the past several years, research on psychological trauma and its effects has resulted in a greater understanding of how potentially traumatic events (PTEs) affect psychological and physical health (Holbrook et al., 2005, Hughes et al., 2017; Kalmakis and Chandler, 2015). Many of these studies required the direct participation of those who have experienced potentially traumatogenic events and who, due to their histories, are considered a vulnerable population with whom to conduct research. Although a growing body of evidence indicates there is little risk of harm from participating in trauma research, ethics boards continue to seek empirical data confirming that the well-being of participants will not be jeopardized by study participation. Investigators face additional challenges when recruiting participants with other factors that increase their vulnerability, such as children and individuals with complex trauma or current post-traumatic stress symptoms (PTSS) (McClain et al., 2007). Research focused on reactions to participation continues to inform project design and offer guidance to Institutional Review Boards (IRBs) on how to support investigators in mitigating potential risks (Cromer and Newman, 2011; Newman et al., 1997).
Existing literature on reactions to research participation
The vast majority of adults who have taken part in trauma-related research after exposure to various types of trauma (e.g. interpersonal/sexual violence, natural disasters, war, accidental injuries) have reported their experience to be positive (Bassa and Collings, 2012; Carter-Visscher et al., 2007; DiLillo et al., 2006; Edwards et al., 2009; Griffin et al., 2003; Grubaugh et al., 2012; Hetzel-Riggin, 2016; Johnson and Benight, 2003; Massey and Widom, 2013 McClain and Amar, 2013; Ruzek and Zatzick, 2000; Scotti et al., 2012). This is also true for children (Chu et al., 2008, Hambrick et al., 2016, Kassam-Adams and Newman, 2005) and adolescents (Chu and Deprince, 2013; Priebe et al., 2010; Ruzek and Zatzick, 2000). Those who reported negative feelings typically experienced mild-to-moderate distress while answering questions, but most did not regret their decision to participate (Carlson et al., 2003; Chu and Deprince, 2013; Hambrick et al., 2016; Newman et al., 1999). For example, 10 out of 203 children participating in trauma-focused research after an acute injury reported feeling sad or upset while answering questions, but only three of them indicated that they wished they had not taken part in the study (Kassam-Adams and Newman, 2005).
Trauma-related research can have positive effects on participants such as developing new insights, clarifying memories, and providing a space for reflection (Carlson et al., 2003). For example, in a study conducted with 29 child and adult refugees, all participants indicated some relief from trauma symptoms after their research interview (Dyregrov et al., 2000). Participants also may derive meaning from altruism: In research conducted with children hospitalized after a traffic-related injury, 77.3% of children and 90% of parents felt good about helping others by being in the study (Kassam-Adams and Newman, 2005).
Several demographic factors have been explored as possibly contributing to research participants’ experiences (e.g. age, sex, trauma history, race). In children, age has been positively correlated with perceptions of participation as voluntary and confidential, with older children having a better understanding about their choice and confidentiality of their information (Kassam-Adams and Newman, 2005). In both adult and child research participants, no significant relationships between participant sex and reactions to participation have been found (Boothroyd, 2000; Hetzel-Riggin, 2016; Kassam-Adams and Newman, 2005; Ruzek and Zatzick, 2000; Scotti et al., 2012). Other studies have indicated that those with a history of trauma are more likely to have negative reactions to research participation (Carlson et al., 2003; Chu et al., 2008; Palesh et al., 2007). Results have been mixed for participant race, with some studies finding little to no relationship (e.g., Boothroyd, 2000; Boscarino et al., 2004; Grubaugh et al., 2012; Ruzek and Zatzick, 2000) and others identifying possible differences based on race (e.g., Kassam-Adams and Newman, 2005; Massey and Widom, 2013). More research is needed regarding the impact of these factors on participants’ experiences in trauma-related research, particularly in parents and children.
Individuals who have significant PTSS may be considered a particularly vulnerable population; thus, ensuring that research participation does not negatively impact their well-being is of particular importance. Several studies have identified a relationship between PTSS and negative appraisals of research participation (Bassa and Collings, 2012, Boscarino et al., 2004; Carlson et al., 2003; Gaela et al., 2005; Gariti et al., 2009; Griffin et al., 2003; Newman et al., 1999; Palesh et al., 2007; Parslow et al., 2000). In these studies, adult participants were asked questions related to PTEs (e.g. childhood abuse, domestic violence, war, terrorism). A single study of children with injury detected no significant relationships between parent or child acute stress severity score and negative appraisals of research participation (Kassam-Adams and Newman, 2005). Other research has demonstrated PTSS was not related to retention rates or to participants’ feelings of regret of taking part in trauma-related research (Grubaugh et al., 2012; Hebenstreit and DePrince, 2012). In addition, research has suggested that adults who have been exposed to trauma were not more susceptible to coercion or less able to fully understand the informed consent process (Newman and Kaloupek, 2009; Ruzek and Zatzick, 2000). Thus, research in the field is mixed, with most research being conducted concerning participation in studies that utilize self-report and interview methods, and with adult participants. More research is needed to understand how children (and their families) with PTSS react to trauma-related research participation and how they react to a broader range of study designs and methods.
Purpose and research hypotheses
The purpose of the current study was to explore various factors that influence the way children and parents perceive trauma-related research participation immediately following a PTE (i.e. an acute injury). This paper adds to the existing literature by examining both child and parent reactions to participation in research tasks that go beyond completing questionnaires or interviews and take place in a hospital setting soon after the time of an acute PTE. The current study aims to: (a) describe child and parent perceptions of trauma-related research participation, including an observational task, following an acute traumatic event; (b) explore the relationship between reactions to research participation and selected demographic factors; and (c) examine the relationship between appraisals of research participation and PTSS over time.
Methods
Participants
As part of a larger study, participants were recruited at a level 1 Pediatric Trauma Center in the northeastern United States while they were receiving inpatient medical care for an acute injury (Marsac et al., 2017). Participants were eligible if: (a) the child was between the ages of 8 and 13 years, (b) the child had a Glasgow Coma Scale greater than 12, (c) the child and parent had sufficient English language proficiency and cognitive ability to answer questions, (d) the injury occurred within the past two weeks, (e) the injury was not due to family violence, and (f) the child perceived the injury as potentially traumatic based on a validated screener.
Ninety-six parent–child dyads participated. Children were between 8 and 13 years old (M = 10.6, SD = 1.7); parents were between 27 and 54 years old (M = 40.7, SD = 6.8). Consistent with typical rates of pediatric injury in boys versus girls, 65% of child participants were boys; 81% of parents identified as female. Reported race/ethnicity for children was 52.1% White, 40.6% African American, and 7.3% other; parents’ reported race/ethnicity was 54.7% White, 41.1% African American, and 4.2% other. The types of injuries were as follows: fracture (62.5%), laceration (7.3%), cellulitis (4.2%), concussion (4.2%), open wound (4.2%), burn (3.1%), and other (14.5%).
Procedures
All research procedures were conducted in accordance with an IRB-approved study protocol. Research assistants (RAs) identified prospective participants using hospital records and approached caregivers of potentially eligible children in their hospital room when they were not otherwise engaged in medical treatment. Parents first provided consent (children provided assent) to an initial screening assessment to determine whether the child perceived the injury as potentially traumatic—a validated four-item screen derived from the Acute Stress Checklist for Children (Kassam-Adams, 2006). For those who screened positive, parental consent and child assent was obtained for the full study. As part of the larger study, at baseline, the child and parent completed an interactive observational task and self-report measures assessing PTSS, cognitive appraisals, and coping, followed by a questionnaire assessing reactions to research participation. PTSS, coping, and cognitive appraisal assessments were repeated during phone interviews 6 and 12 weeks later. For the current study, data analyses were limited to the reactions to research participation and PTSS questionnaires. Child and parent participants were each offered US$15 each to thank them for their time.
Measures
Child–parent interactions (observational task)
While no data from the Trauma Ambiguous Situations Tool (TAST) are presented in this paper, the TAST is described here as a primary component of the research study that the child and parent were reporting their experience and reactions on. The observational task administered at baseline was the TAST. The TAST was adapted from child anxiety literature and includes three modules: independent interviews, child–parent discussion, and child final response. In the first module, we presented the child (and the parent, separately) with four situations, each ambiguous as to potential threat, that could be related to the child’s PTE. For each situation, we first asked for open-ended responses regarding the participant’s appraisal (what might be happening), and coping (what the parent/the child should do), and then asked the participant to select one of four responses regarding appraisal and one of four responses regarding coping. We then brought the child and parent together and asked them to discuss two of the four scenarios, considering what might be happening and what the child should do, and at the end of this discussion we asked the child to provide a final appraisal and final coping response. The TAST was administered in the child’s hospital room, and was video and audio recorded. See Marsac and Kassam-Adams (2016) for a full description of the TAST (Marsac and Kassam-Adams, 2016). To our knowledge, this is the first time this interactive task has been used in trauma-related research.
Prior trauma exposure
At baseline, children were also asked to complete The Trauma Screen from University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index for DSM-IV. A 22-item measure, this survey assesses prior exposure to a variety of traumatic events, such as a natural disaster, accident, war, violence, or medical incident. It is intended for use with children ages 7 years and older (Pynoos et al., 1998).
Posttraumatic stress symptoms
Children completed the Child PTSD Symptom Scale (CPSS), a 24-item self-report questionnaire that yields a PTSD severity score and a likely PTSD diagnostic status (Foa et al., 2001). The CPSS has excellent reliability and convergent validity with structured clinical interviews for PTSD and allows evaluation of whether the child meets the criteria for PTSD as defined by the DSM-IV (American Psychiatric Association, 2000). Parents completed the PTSD Checklist (PCL), a well-validated 17-item self-report questionnaire that yields a PTSD symptom severity score and a determination of likely PTSD diagnostic status (Blanchard et al., 1996; Foa et al., 1997, Weathers and Ford, 1996). The PCL has also been used to assess PTSD symptoms in parents of injured children (Manne et al., 1998).
Reactions to research participation
The Reactions to Research Participation Questionaire for Children and Reactions to Research Participation Questionaire for Parents are 12-item measures for children and parents designed to assess the emotional impact of research participation. Each measure was adapted from the original RRPQ measure for adults to be a practical tool that researchers could incorporate into larger studies (Kassam-Adams and Newman, 2002). Measures examine four aspects of research participation: (a) positive appraisals, (b) negative appraisals, (c) trust and understanding of informed consent, and (d) understanding one’s rights during participation. Parent and child versions of the RRPQ differ in response scales—the RRPQ-C uses a three-point scale (No, Maybe, Yes) and the RRPQ-P uses a five-point scale (Strongly disagree—Strongly agree; Kassam-Adams and Newman, 2002). For the purposes of the current analyses, we combined “Strongly disagree” and “Disagree,” and combined “Agree” and “Strongly agree” in the RRPQ-P to correspond with the child measure’s three-point scale.
Additional study measures
Additional self-report measures administered in the larger study (but not analyzed here) included, for children: the Child Post-Traumatic Cognitions Inventory (CPTCI), How I Coped Under Pressure Scale (HICUPS) (Ayers et al., 1996; Meiser-Stedman et al., 2009), and for parents: the Post-Traumatic Cognitions Inventory (PTCI), the Parent Socialization of Coping Questionnaire (PSCQ), and the Social Problem-Solving Inventory—Revised (SPSI-R Short Form; D’Zurilla et al., 2002; (Foa et al., 1999; Miller et al., 1994).
Statistical analyses
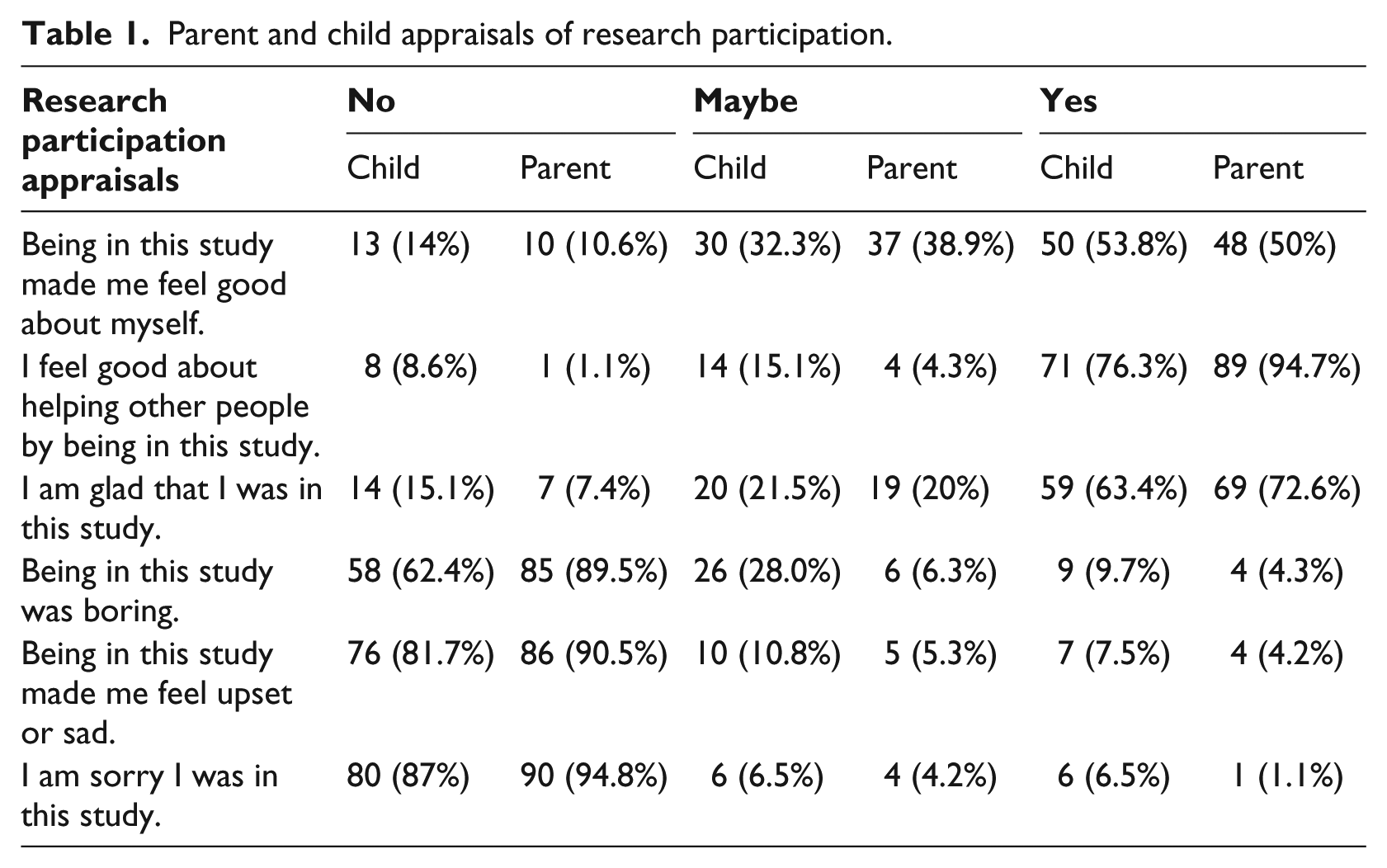
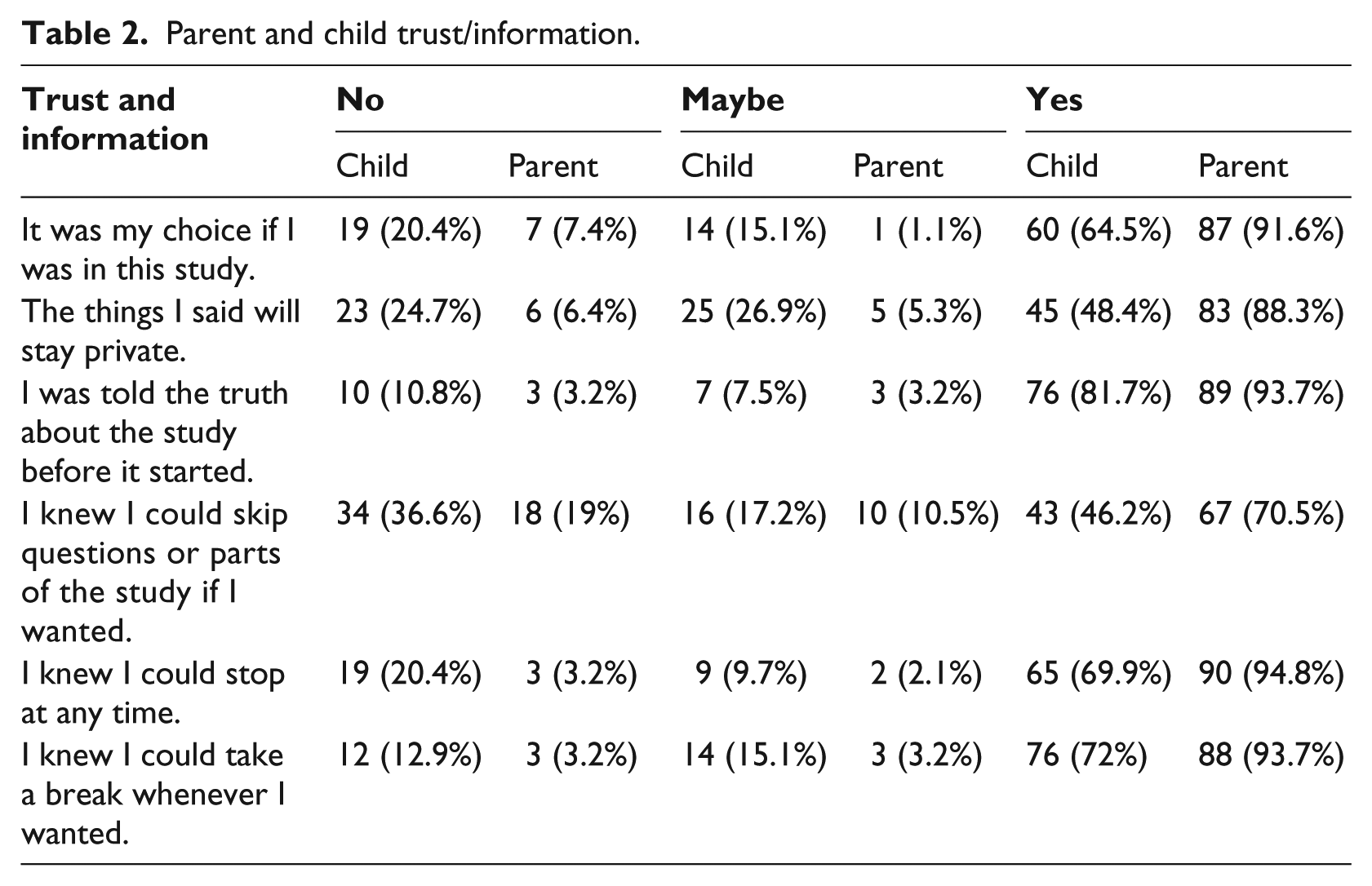
To examine perceptions of research participation (objective 1), we calculated frequencies of child and parent responses using two subscales of the RRPQ measure (see Table 1). The first subscale, Appraisals, was created by combining the first two constructs of the RRPQ (positive and negative appraisals of research participation). The second subscale, Trust/Information, consisted of answers pertaining to trust and understanding of informed consent and an understanding of one’s rights during participation in the RRPQ measure (see Table 2). Next, an exploratory analysis using cross tabulation was conducted to determine whether children who reported distress during participation also regretted taking part in the study. We then conducted the Mann–Whitney U t-test and Spearman’s ρ correlations to examine relationships between research perception (i.e. Positive Appraisals and Trust/Information RRPQ subscales) and selected demographic factors including age, sex, race, and child prior trauma exposure (objective 2). Due to limited racial diversity among participants, race was categorized as Black, White, or Other. To achieve objective 3 (to examine relationships between reactions to participation and PTSS), Spearman’s ρ correlations were conducted using the subscales of the RRPQ (at baseline), the CPSS (across three time points), and the PCL (across three time points).
Parent and child appraisals of research participation.
Parent and child trust/information.
Results
An overview of participant research appraisals indicated that the majority of children and parents reported positive experiences, high levels of trust, and an understanding of the informed consent process and their rights as research participants (see Table 1 for frequencies). Only seven children reported that being in the study made them feel sad or upset, and just two (2.1% of the entire sample) of those children regretted their participation. Six children overall reported regretting participation. Four parents endorsed being sad or upset during the study, only one of whom reported regretting participation.
No significant correlations emerged between child or parent sex and their appraisals of research participation or trust/information. Likewise, there was no statistically significant relationship between race and perceptions of trauma-related research (appraisals or trust/information). Child age was associated with trust/information: Older children’s scores tended to be higher on the trust and informed consent subscale (ρ = .289, p < .01). No significant relationship was detected between child age and positive appraisals of research participation. Parent age was not significantly correlated with their research perception scores. There was no statistically significant association between child perceptions and child prior trauma exposure, nor did perceptions of research significantly relate to child or parent PTSS at any time point. See Table 3 for correlations.
Spearman Rho correlations of potential factors with RRPQ subscales.
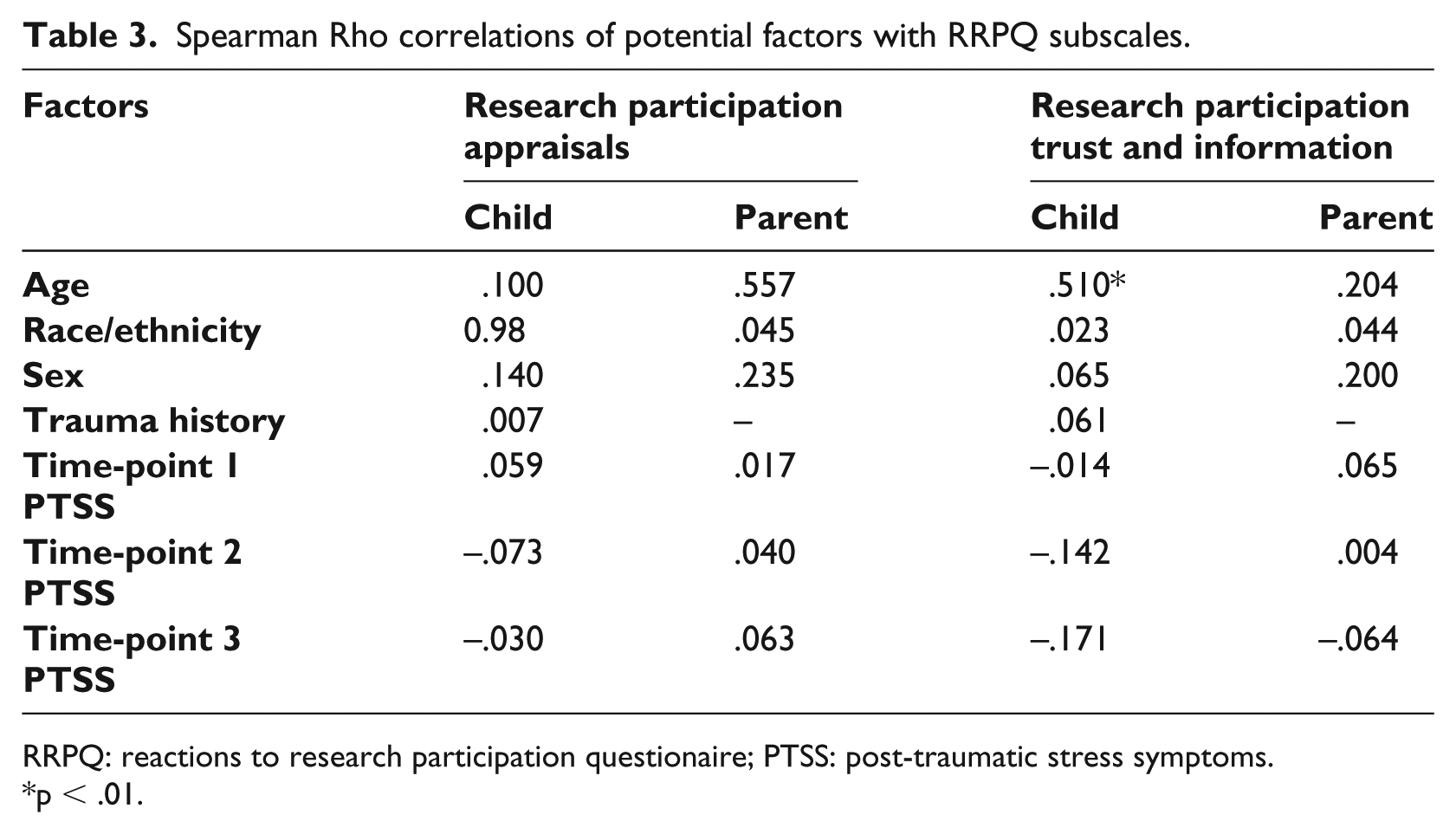
RRPQ: reactions to research participation questionaire; PTSS: post-traumatic stress symptoms.
p < .01.
Discussion
IRBs and ethics committees may have misgivings about research that enrolls children in the immediate aftermath of a PTE, such as an injury, or that asks them to actively engage in discussion of related situations (e.g. observational tasks). The findings of the current study provide a strong indication that this type of study carries low risk of distress for children or parents and that even when distress occurs it generally does not lead participants to regret their decision to engage in the research. This is important because while self-report methodology provides insight into many processes and has advantages (e.g. inexpensive, eliminates interviewer bias, provides a degree of anonymity and privacy; Babbie, 1995), observational methods protect against memory bias and may provide a more accurate picture of parent–child interaction at a given time (Cipiani and Schock, 2011; Hersen, 2006). By incorporating both self-report and an observational method, trauma-related research can offer a fuller picture of parent–child communication after a traumatic injury.
Aside from examining children’s understanding of assent, very little research exists regarding how children under the age of 10 experience potential trauma-related discomfort or distress during the research process (Hambrick et al., 2016). Although prior findings indicate that most participants value the research experience despite possible discomfort when answering trauma-related questions, the majority of these studies were focused on adolescents or adults (Carlson et al., 2003, Chu and Deprince, 2013, Hambrick et al., 2016, Newman et al., 1999). Similar to a study conducted by Kassam-Adams and Newman (2005), the results of the current study suggest that this finding holds true for young children, including those who have suffered a recent traumatic injury (Kassam-Adams and Newman, 2005).
In examining demographic factors that may contribute to an individual’s perception of research participation, only child age emerged as a potentially important factor in this study. The older the child, the more likely they were to rate higher levels of trust and information, which is consistent with results from previous studies (Kassam-Adams and Newman, 2005). This may be a result of a developmental trend regarding children’s autonomy from their parents. Youth begin to gain feelings of autonomy between the ages of 10 and 13 years, when they start transitioning from childhood to adulthood and the family decision-making process often becomes more child driven (Eccles, 1999). Therefore, children within this age range may perceive their participation in the research process as more voluntary. These results add to the body of literature encouraging researchers who are working with young children to incorporate additional processes, such as “consent quizzes,” that ensure the full understanding of the voluntary nature of their participation (Chu et al., 2008). This is especially important when conducting research in a hospital setting, where participants who have suffered traumatic injuries often tend to concede decisions regarding their care (or their child’s care) to those with expertise and may not be able to differentiate between medical treatment and research participation (Ruzek and Zatzick, 2000).
Unlike most prior research, results from the current study found that those with a history of trauma and current PTSS did not report higher rates of negative reactions to research participation (Bassa and Collings, 2012; Boscarino et al., 2004; Carlson et al., 2003; Gaela et al., 2005; Gariti et al., 2009; Griffin et al., 2003; Newman et al., 1999; Palesh et al., 2007; Parslow et al., 2000). More research is needed to better understand this finding. It may be that the nature of the parent–child observational task provided a mechanism through which child participants felt supported by their parents. This aspect of the process may have influenced child participant perceptions in a positive manner, as research has shown that parental coaching and support can have a significant influence during the peri- and post-trauma phases (Hitchcock et al., 2015; Marsac et al., 2014).
Limitations and future research
There are some limitations of the current research that should be noted. Due to a limited sample, racial/ethnic differences could only be examined between those who identified as Black and White, and the majority of parents enrolled in the study were mothers. Future research could continue to explore how these demographic factors impact participants’ experience of the research process. In addition, only a small number of participants endorsed negative appraisals of the research process, leaving a limited sample size in which to explore predictors of adverse reactions. Additionally, the RRPQ-C and RRPQ-P measures were part of a larger study that were not specifically intended for assessing research experience and therefore only completed at baseline. While immediate perceptions of the research experience were examined, the long-term effects of trauma-related research participation could not be determined in the context of this study. Future longitudinal studies could incorporate these measures during follow-up in order to better understand how participation affects individuals over time.
Conclusion
This study confirms the existing literature that trauma-related research is generally well accepted and a positive experience for both children and their parents following a pediatric injury. Few participants reported adverse reactions to participation and even fewer regretted taking part in the study; adverse reactions were not associated with either a history of trauma or PTSS at the time of participation. Younger children may perceive their role in the research process as less voluntary than those above the ages of 10–12 years. While this is likely developmentally appropriate, given younger children’s greater reliance on their parents to guide decision-making, it does suggest that researchers incorporate additional measures to ensure that children understand and assent to participation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]() .
.