
Abstract
Background:
Africa is increasingly becoming an important region for health research, mainly due to its heavy burden of disease, socioeconomic challenges, and inadequate health facilities. Regulatory capacities, in terms of ethical review processes, are also generally weak. The ethical assessment of social and behavioral research is relatively neglected compared to the review of biomedical and clinical studies, which led us to develop an ethics review assessment tool for use in the review of social and behavioral research in Ethiopia, which could potentially be of value in low- and middle-income settings.
Methods:
Initially, we did a comprehensive literature review on principles, guidelines, and practices of research ethics, on social and behavioral studies, from which we extracted query terms to explore the opinions of selected key informants and focus groups in Ethiopia. The discussants and informants were selected using a convenience sampling method to evaluate an ethics review template, which integrated issues that commonly arise in social and behavioral studies. Finally, we directly solicited opinions from the discussants about the desirability, feasibility, acceptability, and relevance of the ethics review assessment tool and used the resulting data to refine our initial draft.
Results and conclusion:
Although the same basic ethics principles govern all research studies, social and behavioral research have some disciplinary particularities that may require reviewers to exercise a different orientation of ethical attention in some cases. Using a qualitative approach, we developed a review assessment tool that could potentially be useful to raise awareness, focus attention, and strengthen the review of social and behavioral studies by ethics review committees, particularly in settings without a long-standing tradition of reviewing such research. This process also exposed some areas where further capacity building and discussion of ethical issues may be necessary among stakeholders in the review of social and behavioral research.
Introduction
Due to its high disease burden, poor health indicators, emergence of threatening new diseases, and relatively weak health-care infrastructure, Africa has increasingly become an important region for health research over the past decades. African educational institutions are also increasingly demanding the conduct of research by students as part of the fulfillment of their diploma and degree programs, and much of this research involves interactions with human participants or their data. However, although there are a number of long-standing and well-functioning African research ethics committees (RECs) (Cleaton-Jones, 2010, 2012; Cleaton-Jones and Vorster, 2008), studies have shown that many African research institutions do not have RECs and those that have the committees have inadequate capacity in terms of infrastructural and financial resources, membership diversity, and training of members to effectively and efficiently review proposed research, monitor ongoing studies, and optimally run REC activities (IJsselmuiden et al., 2012; Mokgatla et al., 2017; Motari et al., 2015; Nyika et al., 2009a; Silaigwana and Wassenaar, 2015). In addition, studies have also indicated that many African RECs lack national ethics guidelines, standard operating procedures (SOPs), as well as accreditation processes to evaluate the review of biomedical and social/behavioral studies (Nyika et al., 2009b; Silaigwana and Wassenaar, 2015).
Biomedical research is typically understood as research involving a systematic investigation of biological processes and the causes of disease through careful experimentation, observation, laboratory work, analysis, and testing; this includes (but is not reducible to) basic science studies and clinical trials. In what follows, we use the phrase ‘social and behavioral research’ to refer to studies involving human participants that are not primarily seeking to understand or observe purely physical processes related to health, or to test devices or drugs in order to improve measurable health outcomes by means of biomarkers. More positively, social and behavioral research seeks through a wide variety of methodologies to understand human behavior, including psychological processes (cognition, emotion, temperament, and motivation), biosocial interactions, and social influences on individual and group behaviors. Terms such as ‘qualitative research’ and ‘social and behavioral studies’ are also used interchangeably to describe the same domain, though some social and behavioral studies can also incorporate quantitative approaches and involve direct interventions. While many social and behavioral studies are health related, they commonly use approaches standard and distinctive for the disciplines of, for example, anthropology, sociology, or psychology.
In many African teaching and academic institutions, social and behavioral studies are often overlooked by RECs, partly because (unlike biomedical studies) such research is believed by some to pose little or no risk of physical harm to participants. Moreover, the very idea of subjecting social and behavioral research to review by ethics committees is sometimes considered controversial (Wassenaar and Mamotte, 2012) and some argue against the practice (Schrag, 2011). Commentators, such as the authors of the Illinois White Paper, argue that such review threatens academic freedom by inhibiting valuable research and substitutes awareness of ethical issues with concern about compliance with regulations (Gunsalus et al., 2007). On the basis of such criticisms, there have been calls to revise the U.S. Code of Federal Regulations (CFR) in order to ‘streamline’ the ethics review of social and behavioral studies, under the questionable assumption that such research poses little or no risks (Emanuel and Menikoff, 2011). Nevertheless, IRBs in the US continue to provide robust review of social and behavioral research, including full board review, particularly when proposed studies pose substantial concerns about privacy, confidentiality, social or legal harm, psychological distress, and the appropriateness of the methods by which the data are collected and managed (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada and Social Sciences and Humanities Research Council of Canada, 2010; Emanuel and Menikoff, 2011). However, critics are correct in pointing out that the existing ethics guidelines are strongly modeled around the constructs, objectives, methods, and preoccupations of biomedical research (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada and Social Sciences and Humanities Research Council of Canada, 2010; Emanuel and Menikoff, 2011), clearly suggesting for a critical need to develop appropriate ethics review tools in low- and middle-income countries (LMICs), such as Ethiopia, where the ethical review of social and behavioral research is still in its infancy.
Methodology
Study design and setting
The study design was prospective and conducted between March and September 2013 with the aim of developing an assessment tool for RECs that can be used to review social and behavioral studies. For this, we used qualitative research methods in a stepwise process.
Step 1: Literature review
We conducted a comprehensive literature review using PubMed and Google scholar as primary databases and retrieved relevant articles published in English using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Hutton et al., 2015). Key terms such as ‘qualitative research’, ‘ethics’, ‘risk’, ‘privacy’, ‘informed consent’, ‘confidentiality’, ‘vulnerability’, ‘social science research’, ‘behavioral science’, and ‘non-biomedical research’ were used to search for relevant articles. In addition, we hand searched for books, working papers, and sources related to research with vulnerable populations under conditions of poverty through hand searching. Eligible articles were screened, narrowed down, and checked for relevance, i.e. the presence of issues related to ethical review of social and behavioral studies conducted globally.
Step 2: Focus group discussion
Using insights from the literature review, we extracted and thematically categorized relevant issues in a form of semistructured, open-ended questions and assessed for inclusion as a discussion guide for a focus group discussion (FGD). The FGD guide was divided into two main themes of scientific review and ethical review. The subthemes in the scientific review included scientific rationale, methodology, study population, research environment, and investigator expertise. The themes in ethical review included subthemes of the potential sensitivity of the research question, social value of the research, vulnerabilities of study populations, consent, confidentiality, potential exploitation, and dissemination plans.
The primary author conducted the FGD using the interview guides, where the second and third authors also assisted in probing and leading the FGD, which took approximately four hours. The focus group discussants (n = 12) were selected using convenience and purposive sampling methods (Marshall, 1996; Teddlie and Yu, 2007) from one of the local institutional ethics review committees in Ethiopia, the AHRI/ALERT Ethics Review Committee (AAERC). The group consisted of 12 members with favorable gender balance (6 men and 6 women), of whom 2 were experts and knowledgeable in the field of social and behavioral research, 6 medical doctors (with specialties in internal medicine, microbiology, and dermatovenerology), 1 lawyer, and the remainder were biomedical scientists. This committee has a position of authority in Ethiopia, having received recognition from the Strategic Initiative for Developing Capacity in Ethical Review (SIDCER) of the World Health Organization (http://www.who.int/sidcer/en/) in 2009 and 2015. All members of the committee had taken online Good Clinic Practice (GCP) and research ethics training. Using the discussion guide, we directly solicited opinions from the focus group on the desirability, feasibility, acceptability, relevance, and content of a social and behavioral research review assessment tool. The FGD was conducted in English, audio recorded, and captured in note-taking. Although only one FGD was considered in this study, the participants sampled for the FGD likely represented a group of experts best placed to discuss the ethics review of social and behavioral research in the Ethiopian context. For the analysis, we used a phenomenological approach and partially adopted the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007), where the information and perception were extracted through inductive methods and coded according to recurrent themes.
Step 3: Development of draft template
Based on the literature review and the content analysis of the FGD data, a draft review template was developed by the first three authors. The presentation style and content of the draft template were partly inspired by instruments developed by the AAERC and templates from RECs at the University of North Carolina (UNC) and the Kenyan Medical Research Institute (KEMRI).
Step 4: Further template refinement with key informants
Five key informants, who were experts in diverse academic disciplines, and who mainly worked in social and behavioral research, were selected for interview (via e-mail) to refine the draft template. Data collected from the FGD and key informants were synthesized in the form of opinions, comments, and suggestions, which were further developed and filtered in the context of existing literature. The resultant template was a result of a triangulation process between the literature review, FGD, key informant data, and existing review templates from other institutions. However, since only one focus group and a small number of informants participated in the data collection procedure, it was not possible to appraise data saturation according to CORED (Tong et al., 2007).
Ethical approval
Informed consent was obtained from all individual participants included in the study. Ethical approval for the research was obtained from Health Research Ethics Committee 2 at the Faculty of Medicine and Health Sciences, Stellenbosch University in Cape Town (Ref # S13/04/065) and the National Research Ethics Review Committee in Ethiopia (Ref # 3.10/310/05).
Results
Generalizability and societal benefit
The focus group initially discussed three core ethical principles: autonomy, beneficence, and justice as described in the Belmont Report (Sims, 2010), in terms of their applicability and feasibility in social and behavioral studies. A question arose in the discussion about beneficence, understood in terms of research having benefits for society. Does research have to be generalizable in order to have social value? The social value of biomedical studies is often tightly linked to scientific validity, and generalizability is often seen as a hallmark of scientific validity, if not a defining characteristic of research itself (Emanuel et al., 2004; Wassenaar and Mamotte, 2012). Since social and behavioral research is often context dependent and not easily generalizable, this paradigm can draw doubt on the societal benefit of this kind of research (Green and Thorogood, 2004). This has been also reflected in a comment by one of the key informants: What may be socially valuable may not be easily generalizable and the value of such research might not lie in the generalizability, as such studies are also criticized for their inability to draw generalizable conclusions and hence assessing a qualitative study on the basis of generalizable knowledge might raise some concerns by researchers working in the field of social sciences. (Key informant # 4)
This resonates with the views of some researchers and ethicists working in LMICs, who argue that societal benefit in social studies can take forms different than the production of generalizable knowledge, such as enhancing the relationship between the researcher and the community, improving knowledge about health in local communities, and helping government agencies identify areas of need for future interventions (Molyneux et al., 2009). On the contrary, a recent commentary has described that qualitative studies may also pursue theoretical generalizability and transferability, provided it is described as the aim of the research or terminology precautions are considered (Carminati, 2018).
Regarding some controversial and challenging methodological approaches in social and behavioral studies, such as the use of deception, the discussants indicated that reviewers must consider ‘ . . . whether valid justifications are considered to perform such studies and whether such studies are also accompanied by debriefing sessions’ (Focus Group Member #6). In keeping with dominant trends in the scholarly literature (Benham, 2008b; Boynton et al., 2013; Miller et al., 2008; Wilson, 2015), one of the discussants also suggested what makes deceptive or covert research exceptional and ethically acceptable in certain circumstances: ‘. . . such methods can only be accepted on conditions that the study cannot be done using other methods or if disclosing the information to participants severely compromises the outcome of the research, despite debriefing sessions’ (Focus Group Member #2). Another discussant also indicated the need for tools to check the quality of a proposed study, including . . . the need for proper sampling design that can be applicable for social and behavioral research, whether there is a predefined inclusion and exclusion criteria for the study and whether data recording and transcription tools are described to maintain the quality and integrity of data. (Focus Group Member #5)
To ensure the integrity and credibility of the proposed research, the qualification and role of researchers involved in the proposed study was also raised (Focus Group Member #6).
Informed consent
With regard to informed consent, the focus group indicated that informed consent must be viewed from a perspective that includes, but transcends, the level of individual study participants (Sommer and Sommer, 1997). During the process of obtaining informed consent, some focus group members indicated that . . . it is ideal to obtain permission from relevant officials, who have direct link with the proposed research, namely institutional permission, permission from community leaders and head of households to subsequently obtain consent from participating individuals before the conduct of a research. (Focus Group Member #4, 6, and 8)
One of the members in the focus group also commented that ‘RECs are better off advising researchers on this to ensure the feasibility and smooth conduct of a proposed research, which otherwise could compromise the overall performance of a given study’ (Focus Group Member #5). Community participation and sensitization has been suggested as one possible mechanism that can set the stage for the process of valid informed consent (Shah and Sugarman, 2003; Tekola et al., 2009). In this regard, the group likewise advised RECs to check and evaluate materials used for community sensitization such as posters, pamphlets, advertisements, and scripts of media announcements or other forms of communication. Similarly, the Joint United Nations Programme on HIV/AIDS (UNAIDS) global advocacy for HIV prevention group has also developed a guideline to enhance community participation in research in a transparent and ethical way (UNAIDS/AVAC, 2011).
Social and behavioral research can also involve most-at-risk or hard-to-reach and legally unprotected communities such as commercial sex workers, drug users, asylum seekers, women who practice abortion in situations where abortion can be penalized (if not conducted for medical reasons), and vulnerable groups such as refugees, victims of disasters or disease epidemics and outbreaks, victims of sexual abuse, and segregated communities, particularly in low- and middle-income settings, which makes the process of getting genuine informed consent very challenging. In such conditions, one of the discussants suggested the possibility of waiving the documentation of consent (i.e. the participant may give verbal consent to participate without putting a signature on the consent form) (Focus Group Member #6). For similar reasons, attempts to reach and gain consent from ‘hard-to-reach’ and stigmatized populations can increase research-related risk even in seemingly innocuous ethnographic and observational studies. The discussants suggested the possibilities of obtaining permission from gatekeepers such as community leaders or heads of households in such scenarios. Some scholars have likewise argued that in certain contexts, particularly where the consent process itself can pose risks, this can be a valid approach (Morrow, 2009). However, uncritical deference to local authorities in regard to consent can also be ethically questionable, particularly in contemporary Africa, where social changes have problematized the legitimacy of traditional leaders and where gender and other hierarchies are not necessarily protective of the rights and welfare of individuals (IJsselmuiden and Faden, 1992).
One of the key informants in this study expressed a concern about potential ‘inflexibility’ regarding how the requirements of informed consent are implemented and the need to customize safeguards in the context of particular study designs: . . . informed consent by participants in a research is a very good idea, it is usually easier said than done. The consent template might do for people who are ‘educated’ as some of the questions tend to be abstract. As I worked in different research projects in some rural parts of Ethiopia, even in longitudinal research, most of the participants are always puzzled by the continuous visits and interviews; they may not understand the objective of the research. They happily participate and give information though without any need for documentation of informed consent. (Key Informant # 2)
Rather than suggesting seeking informed consent for rural populations is futile, this quote indicates the need for customization of the consent process, depending on the study population, in order to enhance comprehension. The same informant continued by stating ‘ . . . if we start to disclose full information about the whole study before we even enter into the main interview questions; participants often got reluctant and even become suspicious of the aim of the research’(Key Informant # 2), further emphasizing the need to find ways of making the process both engaging and informative, while leaving prospective participants with the liberty to refuse participation after having gained adequate understanding of the research.
Regarding studies that involve individuals with mental disabilities or psychotic disorders, one of the key informants indicated that . . . if informed consent is considered as one eligibility criteria for participation in a research, excluding those patients who are unable to provide informed consent because of their medical conditions may not reflect fair selection and fail to respect the principles of justice. Instead seeking consent in the continuum of the research, i.e. asking participants to provide consent while they are already in a research study, after they have recovered from their ‘transient’ problems could be considered. (Key Informant #1)
Extending this line of thought, the discussants and informants made reference to other ways of making consent requirements more flexible such as ‘. . . offering participants to withdraw themselves or their data from the study after data collection’ (Focus Group Members #2 and 6) or ‘seeking proxy consent from care providers or close families’ (Key Informant #1), or ‘seeking a waiver of consent from the respective REC, particularly for studies involving secondary data from archives or medical records’ (Focus Group Member #2, 5, and 6).
Privacy and confidentiality
The discussants indicated that privacy, anonymity, and confidentiality may not always be fully guaranteed in social and behavioral studies, particularly due to the specific methodological approaches that are characteristic of these disciplines. In some qualitative research (such as key informant interviews), deductive disclosure of participants’ identities (Kaiser, 2009) can occur as a result of their particular health condition, social status, or professional position. Given that this is a risk that cannot be eliminated completely, the discussants suggested the possibility of providing information about irreducible risk to participants to obtain genuine consent. In other scenarios, where participants occupy publicly recognizable positions such as government employees and other positions of authority, the discussants suggested that RECs need to check whether sensitive national or institutional information is duly protected and whether (especially when the information is politically, economically, or pragmatically sensitive) the agencies involved have agreed to have individuals participate in research about their institutions. They also emphasized that the voluntariness of consent should be a special focus when collecting data from high-profile participants. In such cases, the group also suggested the possibility of waiving documentation of consent or unlinking the consent forms from participant data sheets as at least one layer of confidentiality protection. Depending on the nature of the study, the use of pseudonyms was also suggested to hide the participant’s identifiers or study site location. But anonymity is not only ethically appropriate for research with those who are better-off and better known. As one participant noted, . . . among poor populations with limited level of literacy, the use of names and signatures can be sensitive and mentioning their names and asking for signature will make matters worse. And I think people will be open and give information when their identities are kept anonymous, especially for sensitive issues. (Key Informant # 2)
In many resource-poor settings, people live in close proximity out of economic necessity and/or in accordance with familial traditions. This situation can raise problems for privacy and confidentiality that both biomedical and social/behavioral research must manage, since clinics in these contexts often struggle to maintain patient privacy and confidentiality (Riaz et al., 2017). Social and behavioral research may involve discussion of private matters through interviews, phone calls, and home visits, and confidentiality on sensitive topics can be compromised already in the recruitment process. The focus group suggested that particular attention be paid to the ethical implications of study procedures that engage with the domestic lives of participants. The group stressed that separate consent should be sought for home visits or phone calls to arrange private discussions and interviews. A few of the discussants also stated that (depending on the study) participants should be explicitly told about the limitations researchers face in maintaining their confidentiality, allowing them to agree or not agree to participate under those conditions.
On the other hand, the discussants acknowledged that confidentiality requirements are not absolute, particularly giving examples of illegal activities, reportable (infectious) diseases, or psychological danger to self or others. In such cases, the group highlighted moral and professional responsibilities to disclose information to stakeholders such as close family members, health-care providers, or other relevant bodies. Citing confidentiality concerns, the group did not fully support the collection of highly personalized data such as biometric information (iris photography and fingerprints).
Psychosocial harm and interventions
Unlike biomedical studies, most social and behavioral studies are perceived to pose minimal risk, these being typically psychological, social, or emotional in nature rather than physical (Council, 2008; Rhodes et al., 2011). One of the discussants however indicated that . . . in some instances these psychological, social or emotional distresses could be traumatic and stigmatizing as a result of relived experiences from the past and hence participants need to be provided adequate counseling or rehabilitation services and RECs need to ensure the involvement of qualified researchers such as counselors or psychotherapists in the study team. (Focus Group Member # 6)
This indicates a perceived need for psychological support in some studies and an obligation on the part of researchers to design and provide mechanisms such as facilitated referral. Nevertheless, the focus group also acknowledged that these risks, while they may be neglected to some extent by more biomedical-oriented ethics committees, are not unique to social and behavioral studies.
Evoking discussions in the scholarly literature (Sommer and Sommer, 1997), one of the discussants highlighted that reviewers should reflect about the timing of research interventions and more generally engage the moral imagination when examining the ethics of social and behavioral research. Referring to qualitative studies posing sensitive questions such as in cases of gender or sexual violence: . . . the appropriate timing or mental readiness of the participants to respond to some sensitive questions, how the research questions are communicated to the participant and the medical conditions need to be checked and evaluated in order to minimize study-related psychological distress. (Focus Group Member # 6)
Since the use of questionnaires and interview guides are commonly key interventions in such studies, the group further emphasized that one should try to imagine how the deployment of the instruments is likely to impact on participants, and that the structure, content, and context of where the instruments are used should be a focus in social and behavioral research ethics review.
Payments to participants
Judgments about fair compensation in social and behavior studies revolved around opportunity costs, damage to reputation, or costs of exposure of illegal activities, provided such considerations do not unduly induce participants (Council for International Organizations of Medical Sciences (CIOMS), 2016; Morrow, 2009; U.S. Department of Health and Human Services Food and Drug Administration, 2018). In this study, the issue of remuneration was a point of robust discussion by the focus group, partly because participants in resource-constrained settings are vulnerable to influence due to poverty. Unlike the other discussion points, opinions here were more mixed. There were two main strains of thought. Considering the modest funding opportunities for qualitative research, particularly in resource-limited settings, some discussants argued that ‘participants need not be paid as long as they voluntarily participate in a particular research’ (Focus Group Member # 5), whereas others suggested that ‘all participants need to be reimbursed for time spent in the research, opportunity cost or any anticipated harm, provided the offers will not unduly induce participation’ (Focus Group Members # 2, 4, and 6).
Template development
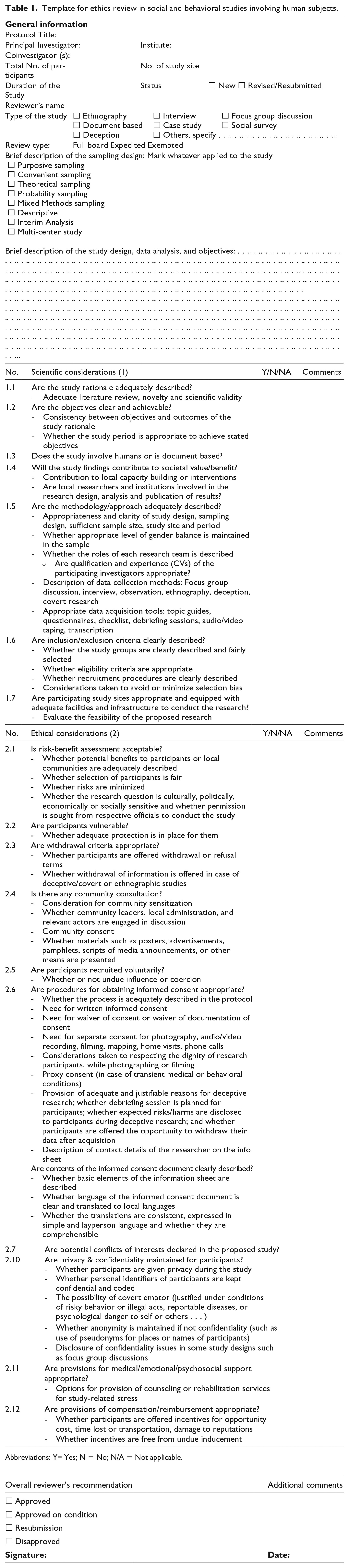
Based on the relevant literature, opinions, considerations, and arguments from the discussants and key informants, we developed an ethics review assessment tool in order to facilitate and structure ethics review of social and behavioral research (Table 1). The template is meant to assist RECs when preparing their ethical assessments of particular studies. The participants regarded the template as a useful tool when reviewing social and behavioral studies in humans, even though most of the points described in the template are also relevant when reviewing biomedical studies. The added value of the tool largely consists in raising reviewer awareness and heightening attention to certain considerations and provisions in regulations (such as use of deception) more commonly in play when reviewing social and behavioral research. Considering the overall neglect and negative perception to reviewing social and behavioral research (Mamotte and Wassenaar, 2009), the template could be important to RECs in LMICs who are conducting or planning to ethically review such research, as part of a wider movement to address the overall inadequate capacities of RECs in LMICs (Mokgatla et al., 2017; Silaigwana and Wassenaar, 2015). Clearly, to enhance potential impact, the template would need to be embedded in a coherent network of other tools and requirements, such as a similarly structured application form to be used by researchers when submitting their studies for ethics review.
Template for ethics review in social and behavioral studies involving human subjects.
Discussion
The basic research ethics elements (Emanuel et al., 2000) are similar in both biomedical and non-biomedical fields of research that involve human participants. Several ethics guidelines have been developed since the Second World War, including the Nuremberg Code (1947) (Law No. 10, 1949), the Helsinki Declaration (1964) (WMA Declaration of Helsinki, 2013), and later the Belmont Report (1979) (Cassell, 2000). More recent ethical guidelines have also emerged, with particular emphasis on the conduct of clinical trials that are conducted in resource-limited settings, namely, guidelines from the Council for International Organizations of Medical Sciences (CIOMS) (Council for International Organizations of Medical Sciences (CIOMS), 2016) and the International Conference on Harmonization Good Clinical Practices (ICH-GCP) (U.S. Department of Health and Human Services Food and Drug Administration, 2018). Most of these guidelines, however, mainly focus on biomedical studies, rendering their applicability to social and behavioral research sometimes questionable and impractical, particularly with regard to the ways in which privacy, confidentiality, and informed consent may best be protected and enhanced in such research (Atkinson, 2009; Cassell, 1980; Pollock, 2012). Partly for these reasons, many social and behavioral scientists are skeptical and critical of the procedures of ethical reviews (Dingwall, 2008; Hammersley, 2009; Hedgecoe, 2008). In addition, some argue that ethics reviews of some social and anthropological studies prevent original research because they require study procedures worked out fully in advance, which may run the risk of losing important information by following a rigidly defined protocol in the field (Zwanikken and Oosterhoff, 2011). While acknowledging the importance of respecting international standards, Zwanikken and Oosterhoff emphasize that adequate review of social and behavioral research, particularly in LMICs, requires highly context-sensitive operationalization of ethics guidance (Zwanikken and Oosterhoff, 2011). In this respect, some associations such as the British Sociological Association (British Sociological Association, 2002) and the National Association of Social Workers (NASW Code of Ethics, cited in Rubin and Babbie, 2001) advocate self-regulation and have developed their own ethical guidelines for social and behavioral research. The template drafted in the current study is not a tool to direct REC reviewer attention to ethical considerations in social and behavioral research as expressed in current literature as well as in views of key stakeholders in ethics reviews in Ethiopia.
Despite the challenges and gaps in the ethical review procedures of biomedical and non-biomedical studies, the focus group remained of the opinion that all research protocols involving human participants should be subjected to formal ethical review, except for categories of exempted studies such as nationwide surveillance, policy papers, minor projects to study educational systems, or studies emerging from public domain. The discussants in the focus group affirmed that ethics reviews should apply to different disciplines beyond biomedicine, and this approach conferred better participant protections than the alternative of not reviewing social and behavioral research as a whole.
According to the CIOMS guidelines, informed consent is defined as the process of information disclosure to enable individuals to make an informed decision about their participation in a particular research study. Although this process may seem straightforward, obtaining genuine informed consent in social and behavioral studies is sometimes challenging (Ruth and Guerrero-Cohen, 2008). As suggested by the focus group, it is crucially important that reviewers capitalize on the flexibility that is inherent in ethics guidelines, in order not to inhibit potentially socially useful research. Giving ethical approval to well-designed studies involving deception of research participants is a case in point (Macklin, 2002; Ruth and Guerrero-Cohen, 2008). CIOMS guidelines indicate some preconditions for justifiable use of deception and waiver of consent, i.e. if the procedure does not expose the potential participant to more than minimal risk, if there are no other research methods that would suffice to investigate the outcome of the research, or if debriefing sessions are provided to participants to explain the reasons for deception at the end of the study (Council for International Organizations of Medical Sciences (CIOMS), 2016). Responsible conduct of research involving deception may include debriefing as a way of apologizing to participants for breaching their autonomy and dignity as persons by offering them an opportunity to withdraw the information obtained in that way (Benham, 2008a, 2008b; Miller et al., 2008). On the other hand, RECs need to be vigilant with regard to the use of deception by ensuring that the debriefing includes adequate disclosure of the rationale for deception and be aware of the expected risks/harm that the participants may face from the deception process (Benham, 2008a).
The respondents were aware and saw the utility of regulatory provisions that permit flexibility in the review of social and behavioral research, such as providing a waiver of consent or waiver of documentation of consent. The repertoire of such provisions, including consenting in the continuum of a research study or seeking proxy consent have also been described earlier (Aldridge and Charles, 2008; Council, 2008; Shah and Sugarman, 2003; Wiles et al., 2005) for qualitative research, particularly when involving hard-to-reach participants such as individuals with ‘transient’ conditions (such as drug or alcohol addicts). Similar to biomedical studies, adequate disclosure of information to potential participants is one of the first steps in order to secure valid informed consent in social and behavioral studies, which is sometimes challenging either due to the complexities of research design (such as observational or ethnographic research) or due to logistic barriers (such as language, ethnicity, economic or social status). In such cases, prior dissemination of information through community sensitization and engagement of community leaders has been described as a means to facilitate the process of informed consent (Tekola et al., 2009). Engaging communities in research can also facilitate the conduct of a given study, particularly with regard to safeguarding and empowering vulnerable groups, enabling them to weigh the distribution of benefits and burdens of research protocols, minimizing the potential conflicts of interest that could arise, and securing valid informed consent (Morrow, 2009; Sachs et al., 1993; Wallwork, 2008). Worryingly, however, some of our respondents seemed to hold untenable views in regard to ‘community consent’, i.e. failing to distinguish between (a) engaging with gatekeepers with the purpose of better protecting research participants in their community and (b) asking permission from authorities to conduct studies in order to ensure that they are conducted as planned. Gatekeepers and authorities are stakeholders to be reckoned with when planning and implementing research, but consent should ultimately be individual (Nuffield Council of Bioethics, 2005). This suggests that more capacity building is needed in regard to the ethical review of research conducted in traditional, hierarchical communities.
Perceptions of privacy and confidentiality in certain societies may be culturally different to some extent from what is described in the bioethics literature, which has a predominant US and Western European world view (Monshi and Zieglmayer, 2004). In the standard literature, issues of confidentiality, privacy, and anonymity are strongly emphasized because of the value placed on the rights of autonomous individuals (Goodwin, 2007; Pollock, 2012; Rubin and Babbie, 2001). Our focus group was more sanguine regarding these issues, regarding confidentiality protection as more of a means of maintaining trust than absolutely securing individual information private from public disclosure. Perhaps for this reason, our respondents were aware of and receptive to the idea that breaches of confidentiality can be ethically justified in social work studies when illegal activities are observed or when maintaining confidentiality could lead to harm to the public or the researchers themselves. Literatures also suggest the principle of caveat emptor: . . . stating the ground rules and debriefing on the participant information sheet and communicating potential participants in the recruitment phase and allowing them to read in advance about the execution of the planned research and the ethical dilemmas over confidentiality, anonymity and the issue of informed consent with more transparency
as a useful way of maintaining internal confidentiality, particularly in focus group research (Tolich, 2009). These ethical safeguards are mainly facilitated by the moderators of FGDs, where RECs need to critically evaluate the level of the moderator’s skill (Tolich, 2009) in conveying the procedures and the judgment and integrity of researchers in the field (Cassell, 1980; Pollock, 2012).
Overall the study involved only one focus group during the discussions and this could have affected members’ responses, as a result of peer influence or participation with colleagues. The first three authors were also members of the ethics review committee that was selected for the FGD. This could be a source of bias in questions asked and interpretation of findings. In addition, the limited number of social and behavioral scientists involved in the study is also a limitation; the template could be further enriched and nuanced by future research consulting a broader and more diverse sample of social scientists. However, much of the data extracted resonate with the existing scholarly literature, and our developed template had overlaps with similar templates created elsewhere.
Conclusions and recommendations
In general, both the process of developing the review assessment tool and the outcome of the process were important first steps, considering the relative neglect of the ethical review of social and behavioral research in the African region. The current template is meant to help orient ethics reviewers of social and behavioral research in resource-poor countries. This is important for two reasons. First, higher education institutions in Africa are increasingly requiring students to conduct research involving human participants as part of their degree requirements. Some of this is likely to be social and behavioral research, because of its relatively lower cost. Second, if this type of research increases, institutions will need to respond by investing in resources for ethics committees.
Since research regulations differ in different jurisdictions, the template would have to be adapted for use in regions other than Ethiopia. The process we used in developing the template (literature review, draft template, qualitative research, and final draft) could be adopted in other contexts. To function well, however, a reviewer template requires coordination with other mechanisms, such as application forms used by researchers when they submit their research for review. The ethics application form should direct researchers to answer questions responsive to the provisions of local research regulations, and the reviewer template should to some extent mirror the application form in order to evaluate to what extent the research is compliant with the regulations. Based on anecdotal information, in many African countries, researchers simply submit research protocols, forcing ethics review committees to search for relevant content. Coordination would distribute this burden. In this paper, we did not attempt to design a corresponding ethics application form as others have done (see: http://www.hsrc.ac.za/en/about/research-ethics/documentation, last date accessed in March 2018). In conclusion, the development of this ethics review template will help address the relative neglect of the ethical challenges involved in social and behavioral research involving human participants in low-resource settings and further lay the foundation for further follow-up studies on validating the template’s effectiveness by engaging researchers and reviewers who have used it.
Footnotes
Acknowledgements
We would like to acknowledge the Armauer Hansen Research Institute (AHRI) for facilitating the required logistics to hold the FGDs and key informant interviews. We also would like to thank all the then members of the AAERC and key informants (from Addis Ababa University-colleges of Social and Health Sciences, Addis Ababa University, Canada, UNICEF Ethiopia, and Young Lives, Ethiopia), who participated and significantly contributed to the discussions and shared their expertise. We also would like to thank Dr Christine Wasunna, who was a member of the ethics review committee at the KEMRI for sharing the structural template used in the respective ethics committee.
Authors’ Contribution
All authors contributed to the study conception, planning, design, analysis, and manuscript writing. LW, SG, and GT held the interview and collected the data and SR supervised the whole study. LW drafted the manuscript. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]() .
.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the Bioethics postgraduate diploma of the Advancing Research Ethics in Southern Africa (ARESA) training program at Stellenbosch University, funded by the Fogarty International Center of the National Institute of Health, USA (grant number R25 TW 008981).