
Abstract
Background:
Body mass index does not distinguish between lean and fat body mass; therefore, its utility defining body composition is limited in pregnancy. Anthropometric measurements may better represent variation in body composition among women who are overweight or obese. We sought to examine body fat composition using maternal anthropometric measurements in late pregnancy and correlate with mode of delivery.
Methods:
A prospective study of pregnant patients who were overweight (body mass index: 25–29.9 kg/m2) or obese (body mass index ⩾ 30 kg/m2) with singleton pregnancies who underwent anthropometric measurements between 27 weeks, 0 days to 34 weeks, 6 days gestation. Maternal skinfold thicknesses from eight sites were used to estimate body fat mass. Correlation of skinfold thickness, anthroprometric measurements, and estimated body fat percentage on mode of delivery were analyzed with p < .05 as significant.
Results:
A total of 41 women with overweight (34.1%) or obese (65.9%) body habitus were included. Mean age was 29.9 years, and the majority (43.9%) were Black and 31.7% identified Hispanic/Latinx. The average gestational age at recruitment was 30 weeks, 2 days and 38 weeks, 6 days at delivery. A greater weight at recruitment (94.2 vs 81.8 kg, p = .023), waist circumference (47.1 vs 43.5 inches, p = .010), Huston–Presley body fat percentage (36.4% vs 31.8%, p = .030), triceps skinfold thickness (20.1 vs 15.7 mm, p = .030), biceps skinfold thickness (18.6 vs 15.0 mm, p = .042), and skinfold thickness, as well as sum of skinfold sites (83.3 vs 68.8 mm, p = .049) were associated with cesarean delivery compared to vaginal delivery on univariate analysis.
Conclusion:
Third-trimester anthropometric measurements may help predict increased risk for c-section in women with obesity. Further research may elucidate utility in nutritional counseling and delivery planning.
Keywords
Introduction
There are several contributions to maternal weight gain during pregnancy, such as the feto-placental unit, uterine, and amniotic fluid expansion, increased blood volume, and increased fat stores. 1 Approximately 35% of gestational weight gain results from products of conception including the fetus, placenta, and amniotic fluid. 2 In addition, lean body mass accrual secondary to an increase in total body water occurs throughout pregnancy. While body mass index (BMI), defined as weight (kg)/height(m2), is widely used as a surrogate marker of obesity, it does not separate the contributions of maternal and fetal weight to gestational weight gain, nor does it take into account individual components of body composition including adipose tissue and lean muscle mass. 3 Therefore, BMI may not be the most accurate measure of maternal body composition during pregnancy.
A few studies have explored the nature of body composition changes in women with obesity during pregnancy. Using the 1990 Institute of Medicine (IOM) guidelines for weight gain in pregnancy, Berggren et al. found that excess gestational weight gain in women with an overweight or obesity body habitus was primarily associated with accrual of maternal fat but not with lean body mass or fetal mass.4,5 Using air displacement plethysmography, Most et al. 6 observed that fat mass accumulation during pregnancy differed by class of obesity. The study found that women with Class I or II obesity gained fat mass during the second trimester and those with Class III obesity loss fat mass. Similar to findings reported by Berggren et al., the study observed no differences in fat-free lean body mass or fetal mass. 6
A number of methods have been developed to assess maternal body composition and changes throughout pregnancy in addition to BMI. 7 Traditional methods to measure body composition and fat mass require expensive equipment involving densitometry with underwater weighing and isotope dilution. These methods are cumbersome and are not realistic to use in the clinical setting. Use of dual-energy X-ray absorptiometry (DXA) scan has also been used to measure composition by passing both high- and low-energy X-ray photons through differing body tissues. 8 Although considered to be a gold-criterion in body composition measurement, routine DXA may not be suitable for pregnancy due to potential radiation exposure to the fetus. Bioimpedance analysis (BIA) is a simpler method that utilizes alternating low- and high-frequency electrical currents to distinguish lean and adipose tissue mass. However, it does not further differentiate between maternal and fetal contributions, and is therefore also limited in pregnancy. 3 Anthropometric measurements of waist, hip, and limb circumferences, as well as skinfold thicknesses, have gained increased interest due to being relatively easy and inexpensive to obtain.7,8 The use of biceps, triceps, subscapular, and suprailiac skinfold thicknesses, for example, are thought to give more information about pregnancy-related changes in adipose tissue that are not influenced by fetal growth or edema. 3 Furthermore, mid-upper arm circumference has been found to be an effective screening tool for maternal nutritional status due to its strong correlation to body weight.9–12
Several studies have looked at the association between skinfold thickness measurements on perinatal outcomes with varying conclusions. A study by Frisancho et al. 13 showed that maternal arm fat was correlated to infant percent body fat and maternal arm muscle area was related to infant length. Another study by Maso et al. 14 found that changes in maternal arm fat and arm circumference during gestation were correlated with infant birth weight in teenage pregnancies. In a cohort of women with obesity, Redfern et al. 15 found that second trimester changes in the sum of upper extremity maternal skinfold thickness in were inversely associated with infant birthweight z-score, after adjustment for maternal age, BMI, and parity. Hediger et al. 16 also observed an inverse relationship between change in triceps, but not subscapular skinfold thickness and infant birthweight, but this was during the third trimester.
We wanted to expand current knowledge regarding the use of maternal body composition measurements, rather than BMI alone, for assessing pregnancy-related risk in women with obesity. Thus, the purpose of this study is to explore the relationship between maternal anthropometric measures mode of delivery in a cohort of women with obese or overweight body habitus. We hypothesize that anthropometric measurements of skinfold thickness may identify patients at increased risk for adverse maternal and fetal outcomes.
Materials and methods
This is a prospective study of pregnant patients who underwent prenatal ultrasound between 27 weeks, 0 days and 34 weeks, 6 days gestational age and who had planned delivery at Richmond University Medical Center (Staten Island, New York) between February 2019 and December 2019. This study was approved by the Institutional Review Board at Richmond University Medical Center (IRB# 2019-01-21-RUMC), and all patients signed informed consent prior to participation. Exclusion criteria included BMI ⩽ 24.9 kg/m2, under 18 years old, multifetal pregnancy, or intrauterine fetal demise at study recruitment. Information about maternal demographics including age, race/ethnicity, parity, gravidity, as well as maternal comorbidities, were obtained from the medical record. Timing and mode of delivery, intrapartum complications, and infant outcomes including birth weight, APGAR scores, neonatal respiratory support, and neonatal intensive care unit (ICU) admission were also recorded.
Anthropometric measurements
Anthropometric measurements were obtained between 27 weeks, 0 days and 34 weeks, 6 days gestation (Recruitment). Measurements of skinfold thickness were performed in duplicate on the right side of the body using a certified skinfold caliper (Harpenden Skinfold Caliper, 10 g/mm2 constant pressure) (West Sussex, UK). The skinfold measurements were collected by a single member of the study team (N.A.L.). N.A.L. had prior formal training and experience with using the Harpenden skinfold caliper, and thus did not undergo formalized training for the purpose of this study. In order to assure reliability, the Harpenden skinfold Caliper was calibrated on a weekly basis using the calibration kit purchased from the company (Harpenden, West Sussex, UK). The average of two measurements were used for skinfold thickness at each site. Skinfold thickness was performed at the triceps (posterior aspect, vertical fold at same level of mid-arm circumference measurement), biceps (over short head of biceps, vertical fold at same level of mid-arm circumference measurement), subscapular (below inferior angle of scapula, at an angle of 45° to the vertical), and suprailiac (immediately above the iliac crest at the mid-axillary line). 3 Measurements of circumference were performed on the right side using a non-stretch measuring tape to the nearest 0.1 cm for mid-upper arm (lateral aspect, midpoint between the acromion, and olecranon process), mid-thigh (lateral aspect, midway between the trochanterion, and tibia), waist, and hip. 3 Maternal height was calculated at recruitment using a stadiometer to the nearest 1.0 mm, and weight was obtained at recruitment and at delivery using a calibrated scale to the nearest 0.01 kg. Height and weight were used to calculate BMI (kg/m2) at recruitment and delivery, and waist and hip circumferences were used to calculate a waist:hip ratio. The “sum of 4 skinfold sites” were calculated by adding the skinfold thickness values for triceps (mm), biceps (mm), subscapular (mm), and suprailiac (mm). 8
Anthropometric measurements of skinfold thickness were used to calculate fat mass using the following equation by Huston Presley et al. 17

Percentage body fat was calculated by dividing fat mass by maternal weight.
Statistics and power analysis
The associations of BMI at Recruitment and Delivery, waist:hip ratio, sites of skinfold thickness, and calculated body fat percentage on maternal and fetal outcomes were statistically analyzed using IBM SPSS Version 24. After calculating for descriptive statistics (mean, median, and standard deviation), differences between the groups were tested for significance using univariate analysis for continuous variables by Student’s t-test or Mann–Whitney U-test. Categorical data were compared using chi-square test or Fisher’s exact test. Correlation was determined using Spearman’s R test and Pearson’s correlation coefficient. A p value < .05 was considered statistically significant. Variables that were statistically significant on univariate analysis were tested for interaction of terms. Non-redundant variables were entered into a multivariable logistic regression model to test for adjusted associations with respect to maternal age, race, and parity (multiparous vs nulliparous). Regression imputation was used to preserve all cases and replace missing data with a probable value estimated by other available information. Variables that retained statistical significance were reported as adjusted odds ratios (aORs) with 95% confidence intervals.
We conducted a priori power analysis with the program G*Power 3.1 (Erdfelder, Faul, & Buchner, 1996) using data from Cnattingius et al. 18 This study examined 1,599,551 deliveries and the risk of cesarean delivery, our primary outcome measure, with increasing BMI. Based on these data, we estimated a medium effect size of 0.45. Assuming two-tailed t-test with at least 80% power and alpha = .05, the total number of 36 will be the minimum required sample for sufficient power.
Results
A total of 41 pregnant women with an overweight (34.1%) or obese (65.9%) body habitus who underwent a prenatal visit between 27 weeks 0 days and 34 weeks 6 days gestation were included. Maternal demographics are shown in Table 1. Pre-pregnancy BMI was available for 38 of the 41 patients. Of these patients, 9 (22.0%) had a pre-pregnancy BMI less than 25 kg/m2. The average age was 29.9 years (range: 18–43 years) and the majority (43.9%) of patients were Black and 31.7% of patients identified as Hispanic/Latinx. The average gestational age when anthropometric measurements were obtained was 30 weeks, 0 days (range: 27 weeks, 4 days to 34 weeks, 2 days), and the average gestational age at delivery was 38 weeks, 5 days (range: 33 weeks, 0 days to 41 weeks, 1 day). Sixteen (37.2%) of patients underwent cesarean section. Reasons for cesarean section included scheduled repeat cesarean section (n = 11), breech presentation (n = 1), macrosomia (n = 1), arrest of dilatation (n = 1), and placenta accreta (n = 1). Thirty-four (82.9%) patients delivered at term. Of the seven patients delivering prior to 37 weeks, reasons included: scheduled repeat cesarean section at 36 weeks for obstetrical indications (n = 3), preterm premature rupture of membranes (n = 2), placenta accreta (n = 1), and preterm labor (n = 1). Average maternal anthropometric measurements are shown in Table 2.
Maternal demographics.
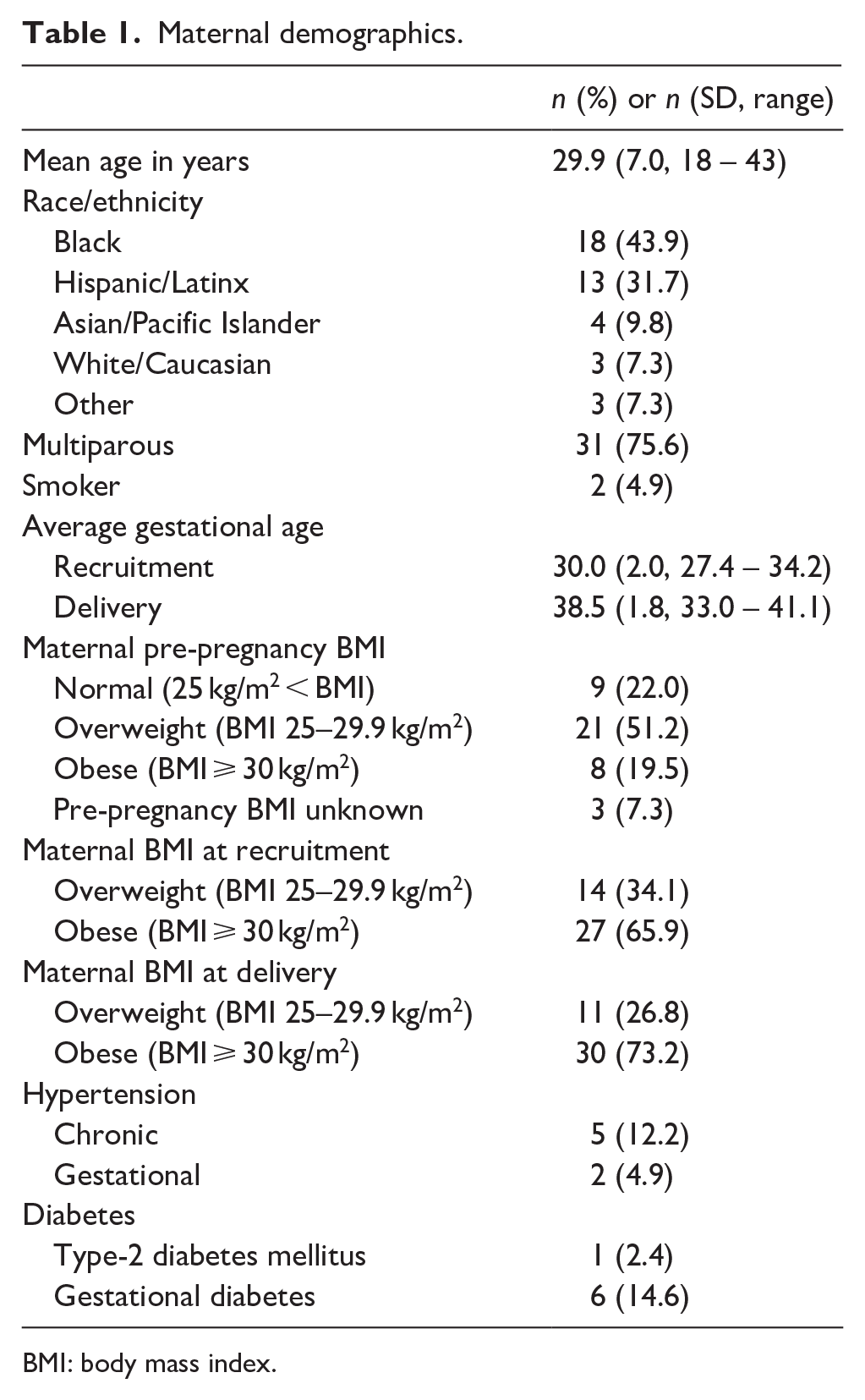
BMI: body mass index.
Maternal anthropometric measurements.

When analyzing the association of maternal anthropometric measurements on mode of delivery, a greater weight at recruitment (94.2 kg vs 81.8 kg, p = .023), weight at delivery (97.9 kg vs 85.6 kg, p = .024), waist circumference (47.1 in vs 43.5 in, p = .010), BMI at recruitment (36.2 kg/m2 vs 31.6 kg/m2, p = .007), and BMI at delivery (36.6 kg/m2 vs 32.9 kg/m2, p = .036) were associated with cesarean section compared to vaginal delivery (Table 3). With regards to skinfold thickness measurements, greater triceps (20.1 mm vs 15.7 mm, p = .030) and biceps (18.6 mm vs 15.0 mm, p = .042) skinfold thickness, as well as the sum of four skinfold sites (83.3 mm vs 68.8 mm, p = .049) were also associated with cesarean section. In terms of body fat percentages, a higher body fat percentage was associated with cesarean section (36.4% vs 31.8%, p = .005) and had a moderate, positive correlation with infant birth weight (r = .332, p = .034).
Association of maternal anthropometric measurements on mode of delivery.

A multinomial logistic regression was designed to assess independent predictors of cesarean section. Variables that were statistically significant on univariate analysis (BMI at delivery, triceps skinfold thickness, biceps skinfold thickness, sum of four skinfold sites, waist circumference, and Huston Presley body fat %) were tested for adjusted associations with respect to maternal age, race, and parity. The model containing nine variables outperformed the null model with χ2 = 27.09, df = 12, with p = .008. As a result of the regression, Huston Presley body fat % was an independent predictor of cesarean section (p = 0.022, aOR: 2.12 (95% confidence interval (CI), 1.12–4.09) independent of maternal age, race, or parity.
Discussion
In this prospective study of women with an overweight or obese body habitus, we explored the relationship between maternal skinfold measurements and estimated body fat percentage with mode of delivery in overweight and obese patients. We found that increases in weight, waist circumference, and BMI were associated with cesarean section. Furthermore, our data showed that a higher biceps and triceps skinfold thickness, as well as the sum of the four skinfold sites were also associated with increased risk for cesarean section. Due to our findings, we further reviewed the data to understand this correlation and found that 73% of our cesarean sections were repeat cesarean sections, which potentially confound our results. In these patients, the reasons for the primary cesarean section were prolonged premature rupture of membranes (n = 1), arrest of dilation (n = 1), failed induction of labor (n = 1), maternal request (n = 1), and triple gestation (n = 1). Prior records were unavailable for six patients. Although we do not have retrospective data of anthroprometric measurements at the time of their primary cesarean section, these women may have had similar risks. While our findings of the association of higher BMI with cesarean section has been supported by the literature, 19 it was interesting that anthropometric measurements and body fat percentage maybe useful to further stratify risk. A larger study of primigravida woman would be needed to examine this finding.
Anthropometric measurements have been used as a less-expensive and less-invasive method to develop equations to estimate body fat percentage in pregnant and nonpregnant individuals.12,13,15,16 Due to the excess water retained during pregnancy, skinfold thicknesses vary among pregnant women and nonpregnant women. Several regression equations exist to convert skinfold thickness measurements into body fat percentage that plot results against a criterion standard to create an estimate of composition. 8 However, it has been shown that equations derived from nonpregnant subjects often overestimate fat change during pregnancy.20-23 After reviewing several equations to estimate body fat, we chose to use an equation developed by Huston Presley et al. 17 which estimated maternal body composition in late gestation. We chose to apply Huston Presley’s equation because their cohort was most comparable to ours with regards to gestational age as well as maternal age. However, the Huston Prelsey equation was developed using a cohort of predominantly (90%) white women who had an average BMI of 25.8 kg/m2. Furthermore, the average body fat mass in their group was 30.6% versus 33.5% in ours, which is likely explained by the fact that our cohort was composed of women with an overweight or obese body habitus. An equation estimating body fat mass in pregnant patients with obesity may be useful when further investigating association of body fat mass on maternal and fetal outcomes. In spite of these limitations, after adjusting for maternal age, race, and party, we found the Huston Presley body fat % was the only independent predictor of cesarean section in this study.
Another more direct method advocated by The International Society for the Advancement of Kinanthropometry (ISAK) is the summation of the skinfold thickness from the sum of 4, 7, or 8 sites reported sites. 8 The sum of skinfold thicknesses has a high degree of agreement with whole-body measures from DXA scans and does not require use of regression equations or conversion to body fat percentages. 8 For the purpose of our study, we evaluated the sum of four sites (triceps, biceps, subscapular, and suprailiac) and found a positive association with increased risk for cesarean delivery on univariate analysis. Summation of skinfold measurement sites has primarily been evaluated in elite athletes; thus, further research is needed in pregnant population to further assess its utility. 8
There is other data supporting the utility of anthropometric measurements in pregnant populations. A study in Nigeria, for example, showed that mid-upper arm circumference (MUAC) has a strong positive correlation with maternal weight and could be used to identify obesity in women regardless of stage of pregnancy. 24 The authors found that MUAC values of 33 cm might be reliable cut offs for diagnosing obesity throughout pregnancy. Further evaluation of MUAC for the utility of low-resource settings could be used to characterize patients who may have had limited prenatal care with no access to accurate pre-pregnancy BMI measurements. In a study of 100 teenage pregnancies in the United Sates, Maso et al. 14 found that depletion in mean mid-arm circumference was predictive of low birth weight and poor nutritional status. In addition, as describe earlier, other studies evaluating perinatal outcomes have inversely correlated increased maternal upper extremity skinfold thickness infant birth weight.13,15,16 Interestingly, body composition studies on women with obesity found a different pattern of maternal weight gain. For example, Most et al. observed that fat mass accumulation during pregnancy differed by class of obesity, as women with Class-I or II obesity gained approximately 1.1 kg fat mass during pregnancy, while those with Class-III obesity lost 4.1 kg of fat mass. However, other components of gestational weight gain were not affected. 6 In addition, the study found that skinfold thickness was found to be larger at all sites in women with more severe obesity, suggesting that subcutaneous adiposity may be associated with maternal BMI. 6 With respect to sum of skinfold thickness, women with Class-I obesity had the largest increase (23 ± 5 mm) compared to women with Class-II obesity (17 ± 7 mm) and those with Class-III obesity showed a reduction in skinfold thickness (−10 ± 14 mm). 6 The authors hypothesize that these inverse associations between class of obesity and weight gain and skinfold thickness may reflect a biological adaptation to minimize the risk for pregnancy complications and fetal outcomes related to obesity. Other studies have also reported a correlation between gestational weight gain and fat mass accrual. For example, Berggren et al. 4 found a significant association between excessive gestational weight gain during pregnancy and accrual of maternal fat mass. Excess gestational weight gain beyond the recommendations of IOM guidelines for weight gain was associated an absolute difference in median fat mass accrual of 7.9 kg compared to those with adequate gestational weight gain. 4 Lederman et al. 25 described positive linear correlations between gestational weight gain and fat mass accrual in women with varying body weights. These studies highlight the importance of understanding how changes in body composition affect women with obesity during pregnancy, as patterns differ from women with normal BMI.
We present prospective data from a diverse patient population in an attempt to further identify pregnant patients at risk for adverse outcomes than can be predicted on BMI alone. While our analysis did not find significant non-confounded correlation to clinical outcomes of interest, future studies examining body composition in overweight and obese women may help to better those at higher risk of adverse perinatal outcomes. Our findings demonstrate the clinical utility of using maternal anthroprometric measurements for the obstetrical management of women with obesity. As the literature demonstrates, BMI alone is a poor surrogate of maternal fat mass gain in pregnancy. Other methods of measuring maternal body composition in pregnancy are either not feasible (DXA) or have limitations (BIA). Thus, use of anthroprometric measurements may be a more useful method for assessing maternal nutritional status and fat gain during pregnancy. Furthering our understanding of maternal body composition changes may help shape future guidelines of regarding weight gain, risk stratification, and nutrition in pregnancy. In addition, it has been demonstrated that maternal anthroprometric measurements can be reliably obtained from pregnant women with obesity using only minimal resources in several clinical settings. 26
Some limitations to our study include our sample size, which was relatively small and thus we could not correlate the anthroprometric measurements to other maternal outcomes, including gestational hypertension, gestational diabetes, as well as delivery complications such as shoulder dystocia. Larger studies may elucidate more information regarding how maternal body composition as determined by skinfold thicknesses may help predict adverse outcomes. In addition, we had a limited number of nulligravid women in our study, which confounded our ability to assess mode of delivery. Study strengths included a high-risk diverse population of women with overweight and obese habitus, as well as prospective nature of the study.
Conclusion
Maternal body composition and fat distribution may be associated with pregnancy outcomes. As BMI does not accurately reflect body composition in pregnancy, additional measures to stratify patients at risk for adverse perinatal events may be useful for predicting outcomes, timed intervention, and patient counseling. Future studies may consider exploring how changes in anthropometric measurements throughout pregnancy may predict outcomes among women with obesity, rather than these measurements taken at a single point in time. Furthermore, looking at how anthropometric measurements of skinfold thickness differ in patients with normal BMI versus obese BMI may be a better method to identify factors to further counsel patients.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.