
Abstract
Objective:
Women experiencing homelessness are at increased risk of cervical cancer and have disproportionately low Pap screening behaviors compared to the general population. Prevalence of Pap refusals and multiple kinds of trauma, specifically sexual trauma, are high among homeless women. This qualitative study explored how trauma affects Pap screening experiences, behaviors, and provider practices in the context of homelessness.
Methods:
We conducted 29 in-depth interviews with patients and providers from multiple sites of a Federally Qualified Health Center as part of a study on barriers and facilitators to cervical cancer screening among urban women experiencing homelessness. The Health Belief Model and trauma-informed frameworks guided the analysis.
Results:
Trauma histories were common among the 18 patients we interviewed. Many women also had strong physical and psychological reactions to screening, which influenced current behaviors and future intentions. Although most women had screened at least once in their lifetime, many patients experienced anticipated anxiety and retraumatization which pushed them to delay or refuse Paps. We recruited 11 providers who identified strategies they used to encourage screening, including emphasizing safety and shared decision-making before and during the exam, building strong patient–provider trust and communication, and individually tailoring education and counseling to patients’ needs. We outlined suggestions and implications from these findings as trauma-informed cervical cancer screening.
Conclusion:
Discomfort with Pap screening was common among women experiencing homelessness, especially those with histories of sexual trauma. Applying a trauma-informed approach to cervical cancer screening may help address complex barriers among women experiencing homelessness, with histories of sexual trauma, or others who avoid, delay, or refuse the exam.
Keywords
Introduction
Cervical cancer (CC), which is responsible for over 311,000 deaths each year across the globe, is preventable through routine screening and treatment of precancerous lesions. 1 Over half of CC cases in the United States are diagnosed among women who rarely or never screen. 2 Although national estimates indicate 83% of women are up-to-date with CC screening recommendations, coverage at Federally Qualified Health Centers (FQHCs), which provide care to uninsured, immigrant, homeless, and other underserved populations, was much lower at 56% in 2017. 3 Women experiencing homelessness have disproportionately low screening rates 4 and a fourfold increase in CC incidence compared to the general population. 5 Low screening is likely driven by structural barriers to access; however, refusing Paps is also common among homeless women. 6 Understanding their difficult and traumatic lived experiences may provide insight into reasons for refusal.
Compared to the general population, women experiencing homelessness or housing insecurity frequently face multiple kinds of trauma, including interpersonal violence, incarceration, discrimination, and neglect. 7 Multiple studies among women facing housing insecurity found 60% to 70% experienced physical, sexual, or emotional violence in childhood.8–10 Childhood trauma increases the risk of repeated victimization later in life. Trauma during adulthood is also frequent: 20% to 60% of homeless women reported violence in the last year.11,12 Sexual trauma, housing instability, and homelessness are strongly correlated. 13 For example, recent intimate partner violence increases housing insecurity. 14 Homeless women, especially those with longer episodes of homelessness, 15 are more likely to experience sexual trauma.9,16
Trauma can shape an individual’s stress responses, sense of safety, perception of control, ability to self-regulate, interpersonal relationships, and preexisting mental health issues.15,17 The effects may be immediate, long-lasting, and exacerbated by repeated exposures. Sexual violence experienced in childhood and adulthood has been linked with pelvic exam avoidance 18 and some cancer screening behaviors.19–21
Despite the high prevalence of sexual trauma among homeless women, data are lacking to explain how it influences CC screening. Therefore, the objective of this qualitative study was to explore how trauma, especially sexual trauma, affects CC screening experiences, behaviors, and provider practices in the context of homelessness.
Methods
Setting
As part of a study on CC screening barriers and potential for self-sampling among homeless women, we interviewed providers and patients at a large, urban Health Care for the Homeless (HCH) program in the northeast. The HCH program is an FQHC providing care to more than 11,000 homeless men, women, and children annually in hospital-based clinics, shelters, outreach sites, and a medical respite unit. 22 In the catchment area, 5% to 10% of the homeless population sleeps unsheltered; in 2019, 62% were in homeless families. 23
Sample
We used provider and clinic screening quality measures to inform the sampling strategy. We purposively recruited providers employed by the FQHC from primary care, gynecology, and internal medicine to capture differences in site, gender, and screening volume.
In alignment with screening guideline eligibility,24,25 we recruited a convenience sample of English-speaking females aged 21 to 64 years with no history of CC or total hysterectomy from the FQHC sites. Initially, we targeted women overdue for screening (i.e. >3 years since last Pap). Due to low accrual and provider interview data about some women agreeing to screen despite significant hesitancy, we expanded eligibility to women currently up-to-date but due soon and recently screened women. We reviewed medical records to confirm eligibility.
Data collection
The interview guides addressed screening barriers and facilitators based on the Health Belief Model, 26 which has been used extensively in screening intervention planning and evaluation.27,28 Providers were asked to give specific examples of declined Paps and trauma as it emerged as a key barrier, as well as strategies used to encourage screening. We asked patients why they had not screened, and included probing questions based on posttraumatic stress disorder (PTSD) screening to understand whether they ever had an experience that was “so frightening, horrible, or upsetting” with an example of physical or sexual assault, 29 and how that experience affected decisions about pelvic exams. Interviewers reiterated patients’ safety, confidentiality, and control of responses, and offered counseling referrals. Interview summaries were analyzed immediately. We recruited participants until we reached data saturation. 30
The protocol was approved by the Dana-Farber Harvard Cancer Center Institutional Review Board (17-319). Interviews were conducted in-person in a private location (October 2017–July 2018). Female social scientists with no affiliation to the FQHC collected patient AMA and provider PC data. Consistent with research practices at the FQHC, study staff reviewed a study information sheet with potential patient participants and then documented verbal informed consent. Providers signed written consent forms. All consent conversations took place before interviews were conducted; verbal consent to record was confirmed on the recording and participants were reminded throughout the interview that consent to participate was an ongoing process. All interviews were transcribed verbatim. Interviews lasted on average 42 min.
Analysis
We iteratively analyzed the data reviewing transcripts and interview summaries repeatedly to develop an initial coding framework. We organized the codes using theoretical constructs from the interview guide. As trauma and discomfort themes emerged, however, we revised the codebook applying trauma and trauma-informed frameworks, recognizing the wide-reaching impact of trauma on individuals’ physical, behavioral, or psychosocial health and care-seeking behaviors.7,31–33 Two independent study team members coded transcripts in NVivo (QSR International, Version 12), resolving discrepancies and refining the codebook through group discussion. We analyzed concepts within and across interviews and subgroups of participants (e.g. patient screening status, provider gender) to identify themes through additional transcript review, reflection, and team discussion using an immersion/crystallization process until we reached thematic saturation.34,35 We followed the consolidated criteria for reporting qualitative research. 36
Results
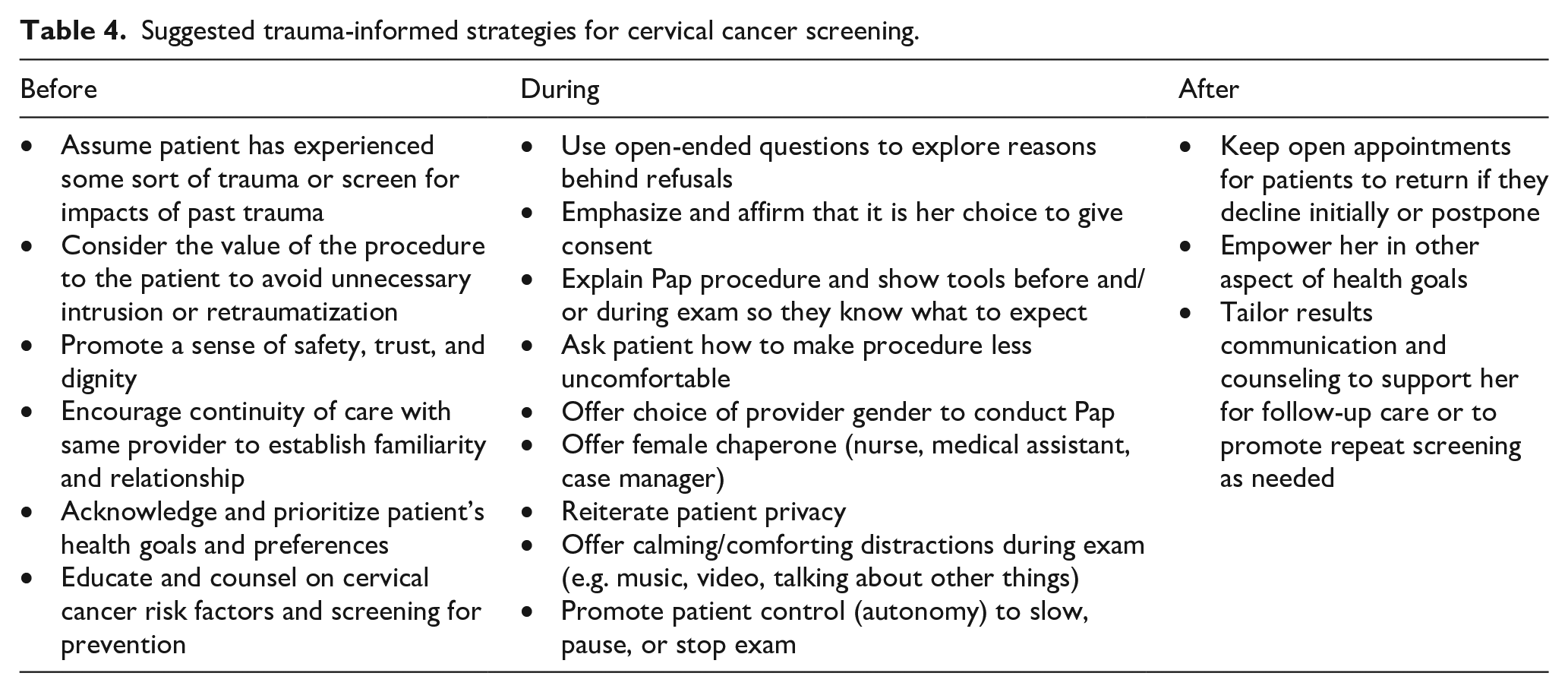
We analyzed 29 interview transcripts, including 18 patients (Table 1) and 11 providers (Table 2). Below, we describe patients’ screening behaviors, trauma experiences, how trauma influences screening perceptions, and providers’ strategies to address discomfort (Table 3). We discuss suggestions for trauma-informed CC screening (Table 4).
Characteristics of HCH patient participants.

HCH: Health Care for the Homeless; PTSD: posttraumatic stress disorder; UTD: up-to-date.
Characteristics of HCH provider participants.

HCH: Health Care for the Homeless; NP: nurse practitioner; RN: registered nurse; PA: physician assistant; MD: medical doctor.
Influence of sexual trauma on cervical cancer screening among HCH patients and providers.

HCH: Health Care for the Homeless.
The presented quotes are illustrative of the thematic findings, not dyadic perceptions of specific scenarios. Patients and providers were not recruited as dyads.
Suggested trauma-informed strategies for cervical cancer screening.
Screening behaviors
Of the 18 patients interviewed, 9 were underscreened (i.e. refusing, overdue, never screened), including 5 women who had not screened in over 10 years. Four of the underscreened women disclosed trauma. Five additional underscreened women found the procedure too uncomfortable and/or upsetting to be screened but did not report trauma. One up-to-date patient strongly opposed future screening.
Experiences of trauma
Overall, nine patients disclosed some type of sexual assault, violation, and/or physical trauma. Most of the patients experienced trauma in childhood; seven patients described flashbacks/re-experiencing, avoidance, numbing, and arousal/reactivity, which are signs of PTSD. 31 Although some of the nine women disclosed significant details of their histories and/or the event(s), others alluded to a traumatic experience and talked around it, not explicitly naming what happened to them. In addition to sexual trauma, providers identified human trafficking, domestic violence, physical assault, and homelessness as trauma. Providers believed the prevalence of undisclosed sexual trauma was high in their population given patients’ strong negative reactions to Paps.
Pap pain and discomfort
Women with and without trauma histories described physical and psychological discomfort related to the Pap. Many found it physically uncomfortable, describing pain they experienced and emphasizing how invasive it was. The instruments hurt: the large, heavy, cold speculum created pressure and pain, especially for those who had not been sexually active for many years. Many women referred to what happens during a Pap as painful “scraping”: I just didn’t like that feeling [. . .] When you put it [the speculum] on and you clamp it and you lock it and you let go and it’s heavy. And then you’ve got to do the scraping, and that’s just too much. It just hurts too bad. (Patient 10)
Although they acknowledged the discomfort, some providers worried misinformation from patients’ peers, a prior bad Pap experience, or perceptions of “outdated technology” (e.g. single size metal speculum) may influence anticipated anxiety and discomfort for patients who had not been screened recently.
Importantly, the women who described no or exclusively physical discomfort with the procedure did not disclose trauma history and were generally accepting of future screening.
Embarrassment, fear, and anxiety
Some women had psychological responses to screening, ranging from feeling “uncomfortable” about the exam to much stronger reactions. Position during the exam—to “expose myself with spreading your legs and have people looking at you”—was humiliating and embarrassing. Some “don’t like being touched” around their genitals and stated that even thinking about it was upsetting. A couple of women noted how the concept of “being scraped” inside their bodies contributed to their anxiety and avoidance.
Sexual trauma exacerbates Pap discomfort
Women with trauma histories had either physical and psychological responses or only psychological responses to the procedure. They also used stronger language, including that their last Pap was “terrifying” and they were “scared to death” of being touched; some explicitly said it was “overwhelming” and “nerve-wracking.”
In addition, being offered a Pap unexpectedly during an appointment for an unrelated complaint was difficult and off-putting for women with trauma histories. Patients recalled declining Paps offered on-the-spot saying they needed time to mentally or emotionally prepare for the procedure, but admitted they avoided thinking about it after the appointment and postponed again at subsequent encounters.
Paps can retraumatize women
Providers confirmed patients’ fears of screening due to trauma histories, noting that some patients went to great lengths to avoid discussing anything related to a pelvic exam. Thinking about the procedure “triggers a lot for them [. . .] just having another person in that area is very triggering.” Some patients we interviewed asked to change the subject because thinking about a Pap brought back distressing memories.
Although one woman directly linked her sexual trauma history to her decision to not screen, others acknowledged trauma influenced their screening experiences, behaviors, and future intentions. Some experienced flashbacks during previous Paps, particularly because of the positioning: “. . . when I close my eyes, it just remind me of what—of being violated.”
Others talked about their aversion to not having control over what happened to their bodies and objecting to “any foreign object going in there” because it is “like your body’s being invaded by something.” Some patients who were up-to-date described accepting screening reluctantly. Some felt they lacked a choice: “you have to do it” despite the physical discomfort and psychological distress. Multiple patients weighed the pros and cons of past Pap experiences, which affected future intentions. Although they had previously screened, they delayed the exam and then struggled through it after agreeing; they still considered Pap screening a trigger.
Providers hesitate to screen
Providers sometimes hesitated or decided to postpone offering Paps to patients who providers believed had experienced sexual trauma. Providers deferred because patients often had a “strong, negative reaction,” were not “able to tolerate” the Pap, or might be retraumatized by the exam. Providers were concerned about protecting the provider–patient relationship and promoting continuity of care, so they were careful not to push for a procedure that might “destroy the relationship or destroy our rapport—it’s not worth it, no matter what. Because if they’re not gonna come back and see us then what good is doing a Pap?”
Providers reported that some women were strongly against screening and “adamantly decline” the exam without giving a reason. They also thought it was common for patients to prioritize other health or social issues and put off the Pap for a later appointment.
And in general, wellness, health maintenance, is low on their [patients’] priority list because there’s often so many other very pressing matters, like addiction and management of acute issues [. . .] but particularly yes, a little bit more for Pap smears, because it’s an uncomfortable thing. (Female provider at outreach clinic)
Providers noted that when women declined Paps, they usually offered “superficial” excuses to delay screening, such as bathing or shaving. When providers felt that they had earned the patients’ trust they would ask additional questions, often about past exams, to understand the underlying reasons for avoidance.
Patient–provider relationships facilitate behavior change
Some women were willing to accept Paps despite finding the exam physically uncomfortable and emotionally stressful. They emphasized that having a trusting relationship with a provider and receiving kind and compassionate care influenced their decisions.
Most providers thought patients with trauma histories required a gradual approach of establishing and earning trust to create “a sense of safety.” They waited to broach the exam after gaining familiarity rather than urging Pap screening at an initial patient encounter. Providers employed various strategies for approaching and offering screening to patients with trauma histories, including whether, when, and how often they should bring up screening.
Shared decision-making and personal agency
Providers acknowledged that women had “their own health agenda,” and therefore preferred to “work on other concerns they [patients] identify” first. When providers sensed resistance from patients, they offered screening after addressing competing health issues.
However, this was notably more feasible for providers who worked at sites with established primary care panels or with opportunities for repeat visits, facilitating continuity of care.
Conversely, screening was a high priority for a few women: they were motivated to take better care of themselves and expressed strong intentions to screen in the future. Some women accepted screening as a routine procedure to stay healthy; the benefits of screening outweighed the risk of trauma-related discomfort. These women talked about how they were willing to “deal with” physical discomfort of Paps. One provider thought women who had recently been sexually assaulted might be more willing to have a pelvic exam “to make sure everything is okay,” though explaining the need for repeated Paps for CC prevention rather than acute sexually transmitted infections is important.
Counseling and communication strategies
Some providers felt that talking to patients about their concerns with the procedure and working together to make it less difficult helped address trauma-related fear and move patients toward screening. Providers sometimes described conversations about screening as a “negotiation,” for example, addressing patients’ health agendas was a “bargaining chip.” Others used motivational interviewing techniques to educate them about CC, acknowledge patients’ preferences, and help “nudge them towards the preventive stuff.” Although these strategies were generally helpful for women with trauma histories and other subgroups facing challenges (e.g. patients with mental illness, recent immigrants), providers still tailored their approach to individual patient needs.
When educating and counseling patients about Paps, providers emphasized privacy and that no one else would be in the room unless the patient wanted someone present. Male providers offered a female provider option. Providers explained the purpose of screening and the procedure before doing anything. Patients appreciated seeing the tools before the exam and hearing what was happening during the exam; it helped put them at ease. Providers took additional steps to calm, comfort, or distract patients during the exam depending on individual needs, including reassuring the patient she had control and could stop the procedure, talking to her about other topics throughout the procedure, or playing music.
Discussion
In this study, we describe how Pap screening is fraught with challenges for women experiencing homelessness. Many women had strong physical and/or psychological reactions to screening. Women’s trauma experiences and Pap perceptions influenced their behaviors: they often delayed or refused Paps. Providers aimed to avoid retraumatizing patients and employed various strategies to develop trust, address patients’ concerns, and change screening behaviors.
During interviews, half of our sample disclosed a history of sexual trauma, most often experienced when they were children. Other studies have also documented high prevalence of sexual violence among homeless and unstably housed women, 8 which is 2.5 times higher than national estimates. 37 Some of our participants did not reveal traumatic history but had similarly strong reactions to Paps compared to women who reported trauma, which may suggest a more widespread aversion to the exam or undisclosed trauma. Sexual trauma is generally underreported for numerous reasons, including fear of not being believed, retaliation, shame, or guilt.
Women’s traumatic experiences, Pap anxiety and discomfort, and unique motivations differentially influenced their screening behaviors and intentions. Although few solely linked sexual trauma to screening avoidance, this may be due to patients not recognizing effects of trauma, 32 not wanting to disclose their history, 38 or other competing social issues and structural barriers to preventive screening. 39 For example, some had been screened at least once in their lifetime, but that experience was so traumatizing that they refused to screen again and noted the negative experience was the main barrier. Others acknowledged Paps were uncomfortable but worked through the barriers. This difference regarding ever screening and adherence to repeat screening has also been found for certain adverse childhood events and other cancer screenings.20,40 Similarly, female veterans in California with histories of sexual violence and PTSD had more fear, embarrassment, and distress related to pelvic exams and believed that the exam was unnecessary. 41 This highlights the importance of providers educating patients about CC risk, routine screening, and follow-up of abnormal screening results in addition to recognizing the impact of trauma. Providers emphasized trust, communication, and shared decision-making as key strategies for changing patients’ screening behaviors, but education interventions to address avoidance of repeat screening and loss to follow-up may also be needed.
Although previous research found that homeless women have strong preferences about the speculum’s size, temperature, and material, 42 in our study, the invasive nature of the exam itself meant some traumatized women chose not to screen for years. Half of our patient sample was aged >50 years, so some had refused Paps for decades. National reports estimate a quarter of women aged 45 to 64 years are not up-to-date on CC screening. 43 Women who have not been adequately screened in many years likely require different interventions than those who are just recently overdue. Providers reiterated the importance of building and preserving patient trust and respecting patients’ reluctance to screen. For women who repeatedly postpone or refuse Paps, self-sampling—where women use a swab or brush to collect their own sample—may be beneficial for women at risk of retraumatization from traditional screening. Self-sampling, which we assessed in a separate analysis, 44 may also promote autonomy and shared control.
Based on these findings and the trauma-informed care literature emphasizing safety, trustworthiness, choice, collaboration, and empowerment,31,33,45 there are some practical implications for trauma-informed CC screening (Table 4). Women must feel safe, have their perceived needs addressed, and not be retraumatized. Understanding Paps as physical or situational triggers may help identify women at risk for adverse Pap experiences. Organizations and providers must recognize the signs of trauma and be prepared to screen for trauma and refer women to additional services if needed. 46 Providers must be comfortable and confident in their ability to identify signs of, and respond to histories of, trauma as such patient encounters can require additional training and time during an appointment. 47
Good patient–provider communication, trust, and a sense of safety were especially helpful in encouraging screening in our sample, which were similar to suggestions from a survey of British women who experienced childhood abuse. 38 Patient education is influential: explaining the preventive purpose of screening and the procedure so women knew what to expect was helpful and may correct misconceptions. Although providers we interviewed did not refer to “scraping,” some education materials use the word “scrape” to describe a Pap, which women may associate with harm and violence. Other work with sexual trauma survivors also found that the patient–provider relationship, quality of encounters, and understanding the procedure reduced anxiety and facilitated screening. 48
In this study, shared control of the exam and providers’ emphasis on patients’ choices to screen or not facilitated patients’ readiness to screen. Similarly making patients aware of options and letting them have control to stop an exam were also important to reverse the loss of power and control experienced during the exam and trauma. However, even when screening barriers are addressed, follow-up colposcopy and treatment for abnormal results may still be difficult for some women; education and navigation support to keep patients linked to care are critical.
This study has some limitations. We focused on patients and providers at one urban HCH program, so results may be generalizable to other HCH programs or urban clinics for the underserved. However, our sample is biased toward patients who engage in health care as we recruited from clinics and outreach sites. Similarly, the HCH providers we interviewed may be more aware of and accustomed to Pap refusals. Although they were recruited from the same sites, we cannot link patients’ experiences to providers’ practices; they were not recruited as dyads. Although we attempted to recruit Spanish-speaking patient participants, our sample was limited to English-speaking participants only who may have different traumatic experiences and other barriers to screening. We also had few young women participate, who may benefit from different interventions. Because this was part of a larger self-sampling feasibility study, we did not explicitly focus on trauma or mental illness a priori, so traumatic experiences and details may be underreported as patient participants may have chosen not to disclose. Although two participants acknowledged substance use disorder, two indicated they had obsessive compulsive or bipolar disorders, and one may have had paranoia, we could not access medical records to confirm diagnoses. However, these findings highlight the real-world challenges of CC screening in the context of providing health care to women experiencing homelessness and suggest solutions to improve prevention among vulnerable populations more broadly.
These findings underscore the importance of recognizing patients’ exposure to trauma in attempts to increase CC screening and suggest that screening for trauma is a first step in providing trauma-informed Pap screening that avoids retraumatizing women. These strategies may also be applied beyond women experiencing homelessness given that more than 40% of US women have experienced some form of contact sexual violence, including rape, forced penetratation, sexual coercion, and unwanted sexual contact. 37 Providing patient-centered, trauma-informed CC screening may help address Pap discomfort and other barriers women face and improve CC control in underscreened women.
Footnotes
Acknowledgements
We would like to thank the patients and staff at Boston Health Care for the Homeless Program who took part in this study, without whom this work would not have been possible. We also thank Anna Revette and the Dana-Farber/Harvard Cancer Center (DF/HCC) Survey and Data Management Core for providing qualitative data management services.
Author contributions
All authors meet the International Committee of Medical Journal Editors criteria for authorship. R.E.K. and C.H. were responsible for conceptualization, methodology, formal analysis, and investigation. J.S.R. was involved in formal analysis. A.A. and P.C. were involved in formal analysis and investigation. J.G. was involved in conceptualization. K.V. was involved in conceptualization, methodology, and formal analysis. All authors were involved in writing and/or reviewing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Dana-Farber/Harvard Cancer Center (DF/HCC) Nodal Award Program (Improving HPV testing and triage for cervical cancer in underserved women). DF/HCC is supported in part by an NCI (National Cancer Institute) Cancer Center Support Grant No. NIH 5 P30 CA06516. R.E.K. and J.S.R. were supported by NIH (National Institutes of Health) Grant No. 3R25 CA057711. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.