
Abstract
Hypertension is a risk factor for cardiovascular disease. Black women have high rates of hypertension compared to women of other racial or ethnic groups and are disproportionately affected by psychosocial stressors such as racial discrimination, gender discrimination, and caregiving stress. Evidence suggests that stress is associated with incident hypertension and hypertension risk. Stress management is associated with improvements improved blood pressure outcomes. The purpose of this review is to synthesize evidence on effects of stress management interventions on blood pressure in Black women. A comprehensive search of scientific databases was conducted. Inclusion criteria included studies that were: (1) primary research that tested an intervention; (2) in the English language; (3) included African-American women; (4) incorporated stress in the intervention; (5) included blood pressure as an outcome; and (6) were US based. Eighteen studies met inclusion criteria. Ten (56%) studies tested meditation-based interventions, two (11%) tested coping and affirmation interventions, and six (33%) tested lifestyle modification interventions that included stress management content. Thirteen of the studies were randomized controlled trials. Reductions in blood pressure were observed in all of the meditation-based interventions, although the magnitude and statistical significance varied. Comprehensive lifestyle interventions were also efficacious for reducing blood pressure, although the relative contribution of stress management versus behavior modification could not be evaluated. Coping and affirmation interventions did not affect blood pressure. Most of the reviewed studies included small numbers of Black women and did not stratify results by race and gender, so effects remain unclear. This review highlights the urgent need for studies specifically focusing on Black women. Given the extensive disparities in cardiovascular disease morbidity and mortality, whether stress management can lower blood pressure and improve primary and secondary cardiovascular disease prevention among Black women is an important question for future research.
Introduction
Hypertension, affects more than 116 million adults in the United States and is a risk factor for cardiovascular disease (CVD), the leading cause of death. 1 Racial and ethnic minorities suffer disproportionately high rates of hypertension and hypertension-related morbidity and mortality. 1 More than 50% of African-American women have hypertension, compared to 39% of non-Hispanic white women and 38% of Hispanic women. 1 Only 26.5% of African-American women with hypertension have controlled blood pressure (BP), despite high levels of awareness and treatment. 1 Suggested lifestyle modifications include dietary changes, weight loss, and increasing physical activity,2,3 but modifications are challenging to adopt and maintain.4–6 Targeting other behaviors, such as stress, may have the potential to improve hypertension management and outcomes.
Psychosocial stressors (e.g. discrimination, financial stress, and caregiving) and perception of stress are associated with hypertension and CVD outcomes.7–11 Adverse effects of stress on hypertension are hypothesized to involve psychological, behavioral, and pathophysiological mechanisms, including depression, diet, physical inactivity, sleep, and alterations in activity of the sympathetic and parasympathetic nervous systems.10,12–14 African Americans report higher exposure to stress and stressful life events compared to whites.15,16 African-American women face gender and race-related stressors, 17 as well as unique stressors related to gendered racism,18,19 which contribute to hypertension disparities and poor health outcomes.20,21
Maladaptive coping strategies may increase vulnerability to stress. For example, John Henryism, described as prolonged, high-effort, and active coping efforts, exacerbates physiological responses to stress and contributes to poor cardiovascular outcomes in African Americans.22,23 The “Superwoman Schema” posit that African-American women may feel obligated to be strong, to suppress emotions and vulnerability and to help others before themselves despite awareness of detrimental effects on their health. 24 Stress management augmented with other lifestyle interventions may be critical for hypertension management and prevention 25 as well as other CVD risk factors. 26 Meta-analyses suggest that stress management may be an effective tool for managing BP, 27 yet a few studies have assessed its effects on BP in African-American women. In this review, we summarize existing evidence on stress management interventions and BP and discuss priority topics for future research.
Methods
A medical librarian devised a comprehensive search strategy. Medical Subject Headings (MeSH), Embase’s EMTREE, and PsycINFO subject headings were identified along with relevant keywords. PubMed/Medline, Embase, PsycINFO, Web of Science Plus (which includes Biological Abstracts and BIOSIS Citation Index), AgeLine, and CINAHL databases were searched through October 2020. OpenGrey, OCLC’s OAISter, and the New York Academy of Medicine Grey Literature databases were searched using various combinations of the following search terms: (hypertension OR high blood pressure OR hypertension OR elevated pressure OR blood pressure OR blood pressure determination) AND (psychological stress OR mental stress OR life stress OR life stresses OR life stressors OR emotional stress OR nervous tension OR psychosocial stress OR coping OR perceived stress OR chronic stress OR stress management OR stress reduction) AND (early medical intervention OR early intervention education OR comparative effectiveness research OR health promotion OR intervention OR interventions OR trial OR trials OR outcomes) AND (women OR woman OR female OR females OR girls OR girl) AND (african americans OR african american OR blacks OR afro-americans OR afro-american OR Black American OR black americans OR Caribbean American OR Caribbean Americans OR ethnic groups OR minorities OR minority groups).
Inclusionary criteria included the following parameters: (1) primary research that conducted an intervention, (2) written in the English language, (3) included adults, specifically women and African Americans, (4) incorporated stress management in the intervention, (5) included BP as an outcome, and (6) were US based. Two authors separately reviewed article titles and abstracts to ascertain if they met the study’s inclusionary criteria. They classified articles as I (included) or an E (excluded). A third author broke the tie for articles.
Results
Figure 1 summarizes the search process for identifying eligible. A total of 882 articles were identified and 755 remained after removal of duplicates. Ultimately, 18 studies were eligible. Sample sizes varied across studies. Samples ranged from N = 20 to N = 2478. Some studies had small samples of African Americans. For example, in Gilstrap et al., out of N = 64 women, 2 were African American. Intervention duration varied substantially given the heterogeneity in study design and implementation across studies. Thirteen of the studies were randomized controlled trials (RCTs). One study was a quasi-experimental design and the remaining studies were non-RCTs. Intervention duration and follow-up ranged from 1 to 24 months.
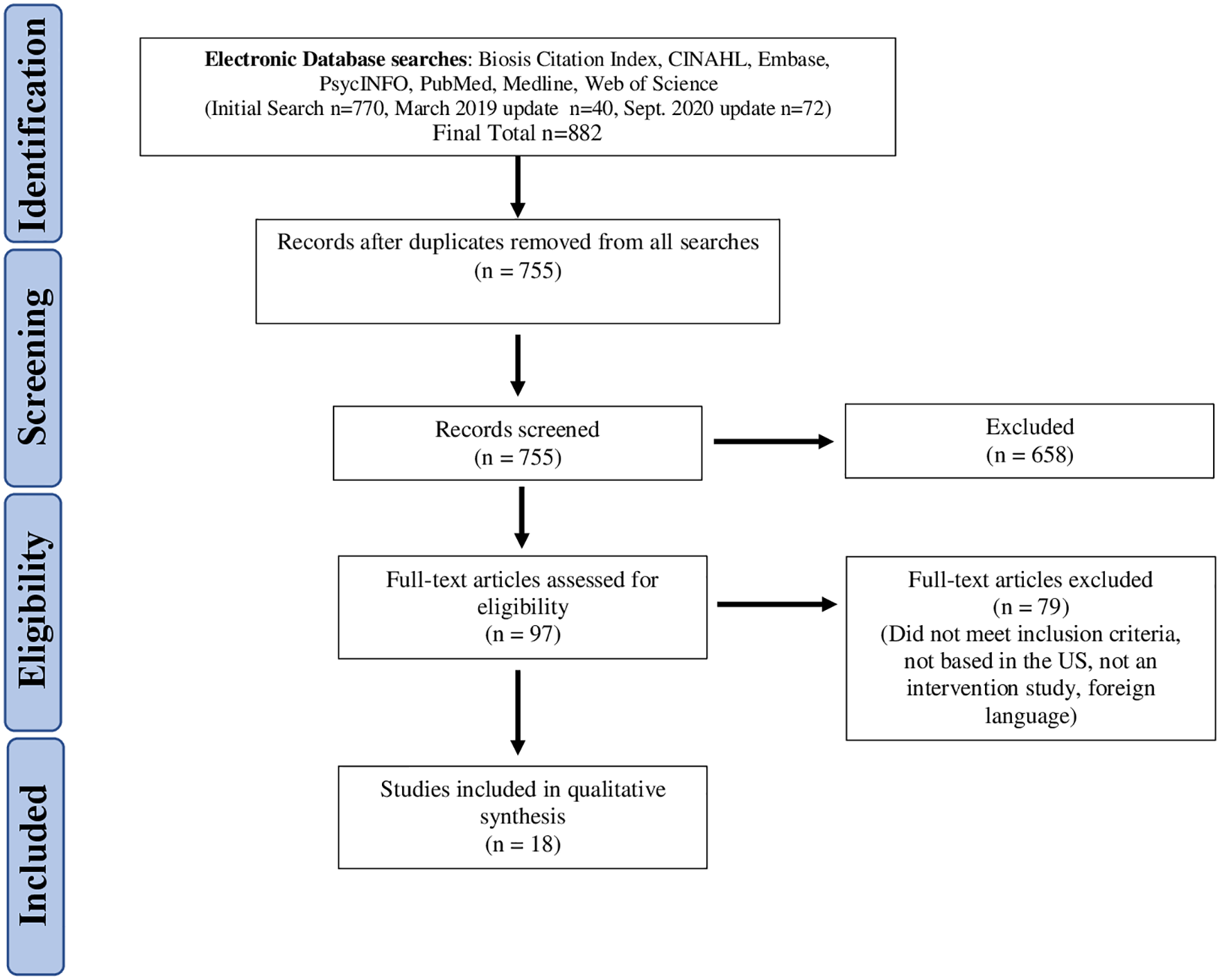
PRISMA flow diagram.
Measures of stress
There was variability in regard to how stress was measured. Half of studies examined stress in their outcomes. Of the studies that did examine stress, nine (50%) utilized the perceived stress scale (PSS), developed by Cohen and colleagues, which examines stress levels in the last month. In regard to the remaining nine studies, stress was either not captured or captured by other tools. In two studies, stress was captured using single-item measures.28,29 In Ward et al., stress was measured by a single-item question from the Society for Behavioral Medicine’s Common Data Elements examining past week distress on a scale of 0 to 10 (0 = no distress and 10 = extreme distress); whereas, in Thomas et al., stress was captured by a single-item question examining current levels of perceived stress rated from 1 (lowest) to 7 (the highest). Schneider 1995 utilized the National Survey of Black Americans subscale to measure self-efficacy, stress impact, and social support. They did not report on these measures. Tucker et al. utilized the strain questionnaire, which included questions about behavioral and health-related stress in the past week. Five studies did not report measuring stress. There was variability in when/how often stress was measured. For example, in Palta et al., stress was measured at baseline, but stress data were not reported at follow-up.
Overview of interventions
Study settings varied with one study being a workplace intervention at a childcare center, 29 nine studies at community-based settings, one church-based study, five studies at major academic medical centers, and one study at a senior center and one ambulatory care center. Studies were distributed over three categories: meditation and mindfulness-based interventions, lifestyle modification interventions, and affirmation and coping interventions. Ten studies (56%) included meditation, two studies (11%) included coping and affirmations, and approximately six (33%) included comprehensive lifestyle modifications (e.g. weight management, physical activity, and medication adherence). Study characteristics are presented in Table 1.
Summary of Interventions.

RCT: randomized controlled trial; SBP: systolic blood pressure; DBP: diastolic blood pressure; TT: Tension Tamer; CVD: cardiovascular disease; HAPPY: Health Awareness and Primary Prevention in Your; CI: confidence interval; BMI: body mass index; AA: african american; HTN: hypertension; PI: principal investigator; BL: baseline; BLBP: baseline blood pressure.
Meditation and mindfulness-based interventions
The most frequently studied meditation-based intervention was Transcendental Meditation (TM), a meditation program that encourages a state of relaxation, 39 which was in 6 (33%) of the 18 interventions. It is worth noting four (44%) of the nine studies on meditations were completed by Schneider and colleagues and largely assessed the effects of TM on BP and other cardiovascular outcomes.38,40,43,44 Consciously resting meditation (CRM), a sound-based meditation program was used as an intervention modality in 1 (5%) study. 45 Mindfulness-Based Stress Reduction (MBSR) 46 was utilized in one (5%) of the studies, 42 and Relaxation Response (RR), a relaxation technique resulting in an altered state of consciousness, 34 was used in another study (5%) of the studies. 33
Three meditation interventions reported no statistically significant differences between intervention and control arms.32,38,41 Duraimani et al. 32 examined TM versus extensive health education (EHE), both delivered over 16 weeks. African-American adults with stage I hypertension in both TM and enhanced health education (HE) control group demonstrated decreases in systolic blood pressure (SBP), but there was no statistical difference between the groups. Results also exhibited greater reductions in diastolic blood pressure (DBP) for participants in the enhanced HE group compared to the TM group (p = 0.04). Similarly, Castillo-Richmond et al. 41 explored TM and its effects on carotid atherosclerosis. While both the TM group and HE control group had significant reductions in SBP and DBP, there were no significant differences in BP reduction between arms. The study was underpowered to detect statistically significant differences between study arms. In Schneider et al., 38 they found within group decreases in SBP and DBP, but no statistical differences between arms.
Other studies included that utilized TM techniques reported positive results in regard to efficacy in lowering BP.40,43,44 Schneider et al., 43 examined effects of TM, Progressive Muscle Relaxation (PMR), and HE on BP and reported that African-American women in the TM group, compared to PMR and HE, exhibited the greatest improvements in BP and psychosocial distress. African-American women within the TM group exhibited lower BP decreased use of antihypertensive medications, and adoption of other behavioral modifications.
Dusek et al. 33 tested a stress management program that included training on breathing and RR training for adults over the age of 55 years. SBP statistically decreased in both RR and control groups. There were no between-group differences. Results showed that a higher proportion of patients were able to eliminate at least one antihypertensive medication maintaining BP control. 33
One study utilized a meditation mobile app to provide mindfulness training. 25 In Adams et al., 25 researchers assessed the effects of a mindfulness smartphone app, Tension Tamer (TT) on BP. Their sample was 48.4% African American and 45.3% female. Participants were randomized to specific groups, to practice breathing awareness meditation through TT for either 5, 10, or 15 min twice daily. The researchers noted significant decreases in SBP and DBP at 1, 3, and 6 months. 25 A higher TT dose resulted in significantly greater reductions in SBP at months 3 and 6. During the 3-month follow-up, significant differences were seen between the 5- and 15-min conditions, and 10- and 15-min conditions. During the 6-month follow-up, significant differences were seen in the 5- and 15-min conditions. Participants assigned to the 15-min condition demonstrated the greatest reduction in SBP over time. During the 1-month follow-up, there was a significant association between adherence and SBP changes.
A study that focused specifically on older African Americans with hypertension, (⩾62 years old, 95% female), and found an 8-week MBSR to be efficacious in reducing BP. Participants in MBSR arm exhibited 21.92-mm Hg lower SBP levels compared to the social support group (p = 0.020). Similarly, the intervention arm also exhibited 16.70-mm Hg lower DBP compared to the control arm (p = 0.003). 42
Lifestyle modification interventions
Of the 18 articles, 6 (33%) included interventions that incorporated stress management as part of a comprehensive lifestyle modification. Studies varied in regard to the patient populations served and study design. For example, one of the studies included focused on patients with type 2 diabetes and one study was a workplace intervention. Of the six lifestyle interventions, three were RCTs.
In a non-RCT, Thomas et al. 28 evaluated the effectiveness of a culturally tailored lifestyle intervention, Prime Time Sister Circles (PTSC), on stress management, physical activity, and nutrition for African-American women. PTSC was found to be efficacious in lowering stress by participants reporting significantly lower stress levels at 3-month and 6-month follow-ups. Women reported incorporating skills such as deep breathing and meditation more often than at baseline. They also reported engaging in more physical activity and higher levels of healthy eating patterns. At 3 months, a lower percentage of women fell within the hypertensive BP category (29.8%) and a higher percentage of women were classified as having normal BP (27.8%) compared to baseline (39.1% hypertensive and 25.1% normal). The same pattern was seen when Thomas et al. incorporated PTSC into a quasi-experimental design with women reporting higher levels of exercise, higher levels of healthy eating, and a lower proportion of PTSC women classified as hypertensive. 28 Gilstrap et al. (also a non-RCT) examined the effects of the Health Awareness and Primary Prevention in Your neighborhood (HAPPY) program on cardiovascular risk. The program incorporated lifestyle modification education on stress reduction, smoking cessation, and implementation of individualized exercise and dietary plans. The percentage of women with hypertension decreased from baseline to 1-year follow-up as well as 1-year to 2-year follow-up. Participants showed significant decreases in stress and BP by the 2-year follow-up. Just 3.1% of the sample was comprised of African-American women. 37
Lifestyle modifications incorporating stress management was also efficacious in managing BP in women with type 2 diabetes. Tucker et al. implemented a tailored community-based health promotion program to adults with type 2 diabetes and examined the effects of lifestyle behavior modifications on body mass index (BMI), BP, stress levels, and blood glucose levels. Sessions were delivered in a workshop format with counseling on stress management, nutrition, food preparation, and physical activity. Participants in the intervention group, consisting of 67.2% African Americans and 73.4% female, exhibited significantly lower stress scores and DBP.
In a cluster-RCT, Ward et al. tested the efficacy of a workplace-based intervention, Health Lifestyles, with content focusing on physical activity, stress management, and other behavioral lifestyle modifications. The control group received the Healthy Finances program which focused solely on managing personal finances. At 6 months, stress and mean arterial pressure decreased significantly within both groups. However, no statistically significant differences were reported between groups.
Bavikati et al. led a non-RCT, community-based comprehensive lifestyle modification program that included physical activity, stress management, nutrition counseling, as well as one-on-one behavioral counseling for adults with prehypertension. Their study reported significant improvements in BP, and also reported reductions in BP were higher in women than in men. They also found that BP changes varied by those reporting a BMI of <30 versus individuals reporting a BMI of >30. 30
Using a non-randomized, uncontrolled-single arm design, Emmert-Aronson et al. implemented a “behavioral pharmacy” approach that engaged multiple social determinants of health to engage patients at a federally qualified health center (FHQC) with conditions that can be managed through behavioral intervention. 35 The “behavioral pharmacy” approach was rooted in four components: physical activity, nutrition, social support, and stress reduction. This study’s approach incorporated comprehensive lifestyle changes while also including a meditation aspect for the stress reduction component. Their findings showed statistically significant decreases in SBP and improvements in other cardiovascular risk factors such as BMI and physical activity. Among individuals with depression, there were statistically significant reductions in depression and SBP at the conclusion of the program. They did not report findings on stress specifically. 35
Affirmation and coping interventions
Two articles (11%) were classified as affirmation and coping interventions. One study was performed in ambulatory care practices tested self-affirmation and positive effect on BP control in African-American adults with uncontrolled hypertension. 31 The results showed that individuals with greater stress or depressive symptoms at baseline were less likely to have controlled BP at 12-month follow-up. Multivariate analysis showed that females had 2.95 times greater odds of achieving the outcome BP of 140/90 mm Hg (p = 0.10). There was no difference in BP control between the intervention and control groups. The authors suggested that the intervention and control arm were not distinctive enough and that there could have been possible contamination given that the same research staff delivered both interventions.
One study (5%) was a faith-based intervention and categorized as a coping/affirmation intervention. Mendez et al. (2018) examined a church-based intervention for older African-American adults (>45 years old), Health for Hearts United (HHU), which centered around awareness building, clinical learning, and efficacy development. 36 HHU included individual and group sessions that incorporated stress management by introducing active coping skills. Lower life satisfaction (LLS) was found to be significantly associated with higher DBP at 6-month follow-up but had no associations with SBP. Active coping was adversely associated with BP, resulting in higher levels of SBP (p < 0.01) and DBP (p < 0.05) at 24 months. They reported that the coping intervention resulted in improvements in anthropometric measures related to CVD risk. Authors proposed that perhaps some elements of John Henryism may help to understand how participants were engaging in active coping.
Discussion
We reviewed 18 studies that were interventions incorporated stress management for BP control in Black women. Notably, meditation-based interventions statistically significant results varied. Lifestyle interventions were also efficacious as reducing BP. This review also demonstrates that more studies are needed to ascertain the true effects of stress on BP because so a few studies focused on African-American women or stratified by both race and gender. A number of studies examining stress management and hypertension were not included because they did not include stratifications by race and/or gender.47–49
The mixed findings relating to the affirmation/coping interventions included warrant further exploration. In Boutin-Foster et al., the authors suggested that a possible explanation for the negative trial may have been that affirmation and self-affect may not have been as effective mediators in comparison to patient education.
In the only coping intervention, Mendez et al. reported unexpected results showing that coping did not have an effect on the association between LLS and BP and an adverse relationship between coping and BP. This introduces critical questions regarding coping and their effects on BP among African Americans. Perhaps it is important to differentiate between high-effort coping and the presence of stress as particularly detrimental combinations for BP. For example, James et al. 22 hypothesized a construct within the John Henryism framework suggesting that high-effort coping alone may not necessarily be as detrimental as in the presence of high stress combined with high-effort coping. 22 A study examining the John Henryism hypothesis in the Jackson Heart Study (JHS) found that socioeconomic status may potentially exacerbate the effects of high-effort coping on hypertension in men. 50 These findings raise further research questions about what characteristics and populations may be particularly susceptible to the effects of John Henryism.
The relative success reported by the studies that included stress management in the lifestyle interventions may be promising—especially given the strong relationships between health behaviors and both stress and BP. Stress can inhibit adoption of positive health behaviors and lifestyle factors that can reduce risk for hypertension. For example, Gaston et al. 51 explored a behavioral health intervention for mid-life African-American women and found that 14.5% of women noted stress as a barrier preventing them from adhering to a regular exercise regimen. Kang et al. 52 found that among African-American women who reported high-stress levels, there was lower adherence to behavioral lifestyle modifications. In the JHS study, stress was associated with lower adoption of Life’s Simple 7, the American Heart Association (AHA) recommended lifestyle modifications for optimal heart health. 53 The finding that the “behavioral pharmacy” approach evaluated by Emmert-Aronson et al. may be helpful in patients with depression is critical, given that African Americans have increased the risk for severe depression, 54 depression is a major risk factor for CVD, 55 and individuals with depression may be more susceptible to the detrimental effects of stress. 56
The utility of mobile health applications (mHealth) has been increasingly recognized as potentially efficacious tools in public health. However, there are limited studies evaluating mHealth stress management interventions, particularly as they may pertain to BP control, and even less so on if they are acceptable, feasible or efficacious in African-American women. At the time of this review, only one published study examining an mHealth stress management intervention on BP outcomes was available. 25 The results demonstrated the potential in App-delivered mindfulness training as an mHealth modality for stress management. A systematic review on the effects of mHealth interventions on secondary CVD prevention noted that mHealth patients exhibited increased medication adherence and adherence to recommended non-pharmacological therapies for managing BP. 57 Another review that showed promising results for mHealth interventions and other risk factors for CVD and BP such as smoking and glycemic control. 58 Research suggests that mHealth interventions may be complementary when combined with other intervention components such as home BP monitoring. 59 This is especially promising for BP control in Black women given their high rates of mobile phone ownership and use of mobile phones for Internet access. 60 Despite these encouragements, the utility of mHealth mindfulness–based interventions among Black women remains largely untested.
The meditation interventions included in this review demonstrated some positive results in terms of reducing BP, although some were studies were statistically insignificant when comparing intervention versus control arms. There has been an increase of mindfulness-based interventions in modalities for stress management in scientific research in recent years. There is a growing body of evidence about the benefit of meditation practices as complementary approaches to pharmacotherapy for BP control. It has been shown to improve physical and mental health outcomes among individuals with coronary heart disease, prehypertension, anxiety, and depression.47,61–64 Despite the promising benefit of mindfulness-based interventions such as mindfulness-based cognitive therapy (MBCT), there are barriers associated with traditional in-person delivery of MBCT. Other studies have tested adaptations to MBCT, such as phone adaptation. 65 Limited evidence exists on how these may be efficacious in BP control in African Americans.
A notable challenge in stress and behavioral health research is the complexities in measuring stress in general, specifically in African-American women. There is no gold standard on how to measure stress, and a variety of validated tools have been used. Most commonly used in research is the PSS, developed by Cohen et al. 66 The PSS was originally developed as a 14-item tool by Cohen et al., 66 and evaluated as a 10-item tool. 67 Other measures of stress include the strain questionnaire, which measures behavioral, cognitive, and health-related stressors. Other previously utilized measures of stress include the Weekly Stress Inventory (WSI), an 87-item measure of stressful events occurring in the past week. 68 The Stress Overload Scale (SOS) has been used notably among African-American women in prior research, 69 which includes measurements of personal vulnerability and stressful event loads. 70 Future research should address challenges in measuring stress within the African-American community, particularly among women. Some research suggests that African-American women may underreport stress due to cultural and societal norms that may facilitate maladaptive coping and difficulty acknowledging stress. 71 More research is needed on assessments of stress in this population and whether or not currently available tools may not perform ideally in this population to capture stress levels accurately.
Conclusion
This review utilized rigorous search strategies to obtain published studies of stress management and samples that included African-American women. However, there are some limitations that should be considered. Because so a few studies focused specifically on African-American women, so even when positive effects were found, it is not possible to draw conclusions about effects in this population. Also, some studies did not have adequately powered sample sizes, thereby inhibiting ability to detect differences between study arms.32,40 Many studies had active control arms, which may have made it difficult to ascertain the true efficacy of the intervention. In addition, some studies did not include a control group, were not RCTs, and/or were underpowered. These methodological limitations hinder our ability to make causal inferences or establish generalizability. As previously mentioned, there was substantial variability in stress measures, limiting our ability to aggregate the data and conduct a meta-analysis.
This synopsis on stress management interventions and BP among African-American women highlights the need for efficacious interventions to reduce BP and cardiovascular risk. Increasing randomized clinical trials on stress management in African-American women is critical. There have been several adaptations and novel innovations of stress management programs, yet little is known about their efficacy in African-American women. Future research should examine if and how such adaptations can be effective tools for stress management in African-American women.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported in part by the National Institutes of Health grant T32HL129953 - Mentoring URM Scientists in Behavioral and Cardiovascular Health to Increase Academic Workforce Diversity and American Heart Association grant 19POST34380633.