
Abstract
Objective:
This study assessed the relationship between presence and number of chronic disease and reception of mammogram in women 65 years and older, and how this relationship is influenced by primary care provider visits.
Methods:
A total of 3306 women diagnosed with breast cancer from 2006 to 2008 from cancer registries in four Appalachian states were analyzed.
Results:
Having a mammogram within the past 2 years was associated with having at least one chronic disease. The presence of a chronic disease was associated with an increased likelihood of breast cancer screening adherence but was not a strong predictor when demographic variables were added.
Conclusion:
This study supports the findings that women with more primary care provider visits were more likely to adhere to breast cancer screening guidelines but having several chronic diseases presents a barrier to achieving guideline-concordant mammography screening, highlighting the importance of preventive screening for patients managing chronic diseases.
Background
Mammograms are a cost-effective method of detecting breast cancer early and reducing mortality from the disease.1,2 When people are diagnosed at earlier stages, treatment success and survivorship rates are high. 2 For example, the 5-year relative survival rate for cancer localized to the breast is 99% while that for cancer that has spread from the breast to distant parts of the body such as the lungs is 27%. 3 The United States Prevention Services Task Force (USPSTF) recommends that women who are 50–74 years old, and women aged 40–49 years who have average risk for breast cancer or placed a higher value on the potential benefits than harms should receive a mammogram every 2 years. 4 Other cancer organizations, such as the American Cancer Society, recommends that for women at average risk of breast cancer have the option to begin annual mammography at 40–44 years of age; while women 45–54 years should undergo annual mammography; and those 55 years of age or older may transition to biennial mammography or continue with annual mammograms. 5 Screening recommendations for high-risk women, such as those with a family history of cancer, include annual mammograms beginning at age 30. 6
Medicare provides health insurance coverage for eligible individuals 65 and older, and Medicare Part B covers most preventive services. 7 Mammography has been covered under the Medicare program since 1991, 8 and women over 65 make up a third of all mammograms conducted each year. 9 Even in this insured population, preventive services use, including mammogram receipt, is low. According to the American Cancer Society (2009), only 68% of women age 55 years and older received a mammogram consistent with recommended guideline. 5 Previous studies have identified a number of factors that predict lower rates of mammography use among the elderly. Minority women, women with less education, those not having a usual source of care, or those in poverty are all less likely to receive a mammogram.10 -12 In addition, availability of transportation, distance from metropolitan areas, a limited number of health care visits, a lack of related physician recommendations, and fewer available health care professionals have all been cited as barriers to cancer screening in Appalachia.13-14
About half of US adults have at least one chronic disease,15,16 while 25% have two or more chronic conditions.17,18 The percentage of adults with multiple chronic diseases (both 2 and ⩾3) increased with age as 90% of those age 65 and older have at least one chronic condition.15,19 Similar to preventive services, challenges to accessing chronic disease care are widespread in rural areas due to limited numbers of health care specialists and transportation barriers.20,21 Research on the association of between chronic disease and cancer screening have produced mixed results. Some studies have shown a negative association between the presence of chronic diseases and cancer screening.22 –24 Lipscombe et al. 22 in a retrospective cohort study of Canadian women found that women with diabetes had significantly fewer mammograms (with the previous 2 years) than those without diabetes even if the diabetic woman visited a primary care physician several times during the year. Liu et al. 23 also found that an increase in the number of chronic conditions was associated with decreased breast, cervical, and colorectal screening rates in a population in two rural Oregon communities. Conversely, other studies found that the presence of chronic diseases was associated with compliance with cancer screening guidelines.25 –27 Yasmeen et al. 27 found an increased uptake in mammography among women with more than three chronic diseases. Fleming et al. 25 examined the relationship between multiple chronic diseases and the prevalence of colorectal screening among residents in Appalachian Kentucky and found that individuals with more chronic diseases were more likely to have received colorectal screening.
These conflicting results may be due to the different study settings, geographic locations, and time periods, during which recommendations for breast cancer screening (BCS) and awareness about the disease changed. The 65 and older age group is the fastest growing segment of the US population, and cancer screening decreases with increasing patient age.24,28 Although an extensive body of literature exists on the determinants of BCS, little is known about how the presence of chronic disease affects screening behavior, especially among people with elevated cancer mortality risk and comorbidity, such as those living in Appalachia.
This study examines the associations between the number and prevalence of chronic health conditions and having received a mammogram according to screening guidelines among older women in four Appalachian states. We focus on receipt of a mammogram within a single time period and geographic location and specifically examined the impact of different chronic conditions on being up to date for BCS, while adjusting for potential confounders. The increasing older adult population, the escalating rate of chronic disease in the Appalachian region, and the unresolved relation between chronic disease care and cancers screening enhance the significance of this focus. This study addresses the following research questions: (1) is the presence of a chronic disease after controlling for other correlates of BCS independently associated with having received a mammogram and (2) is the number of chronic conditions after controlling for other correlates of BCS independently associated with having received a mammogram.
Methods
Data
Data from cancer registries in four Appalachian states, Kentucky, Ohio, Pennsylvania, and North Carolina, were analyzed to identify women diagnosed with breast cancer from 2006 to 2008 and living in Appalachian counties as defined by the Appalachian Regional Commission (ARC). Patients were linked to Medicare fee for service files available from the Center for Medicare and Medicaid Services for 2005–2009 using patient identifiers. Patient information was also geocoded and linked to the Area Resource File (2007–2009). A total of 3306 women were included in the sample.
Sample
Women 65 and older, having a positive breast cancer diagnostic histology, cytology, or microscopic confirmation (excluding autopsies) were included in the study sample. Only women who could be linked to Medicare data and were enrolled at least 2 years prior to and 1 year after diagnosis were included. Respondents were also restricted to those with a first ever diagnosed breast cancer tumor. Women with multiple or concurrent tumor, mismatched gender and birth dates, and without complete Medicare Parts A and B insurance, or with some managed care (e.g. health maintenance organization) coverage during the 24-month period before and including the month of cancer diagnosis were excluded.
Measures
The outcome variable of interest was BCS adherence. Women were examined for compliance with mammography guidelines prior to their breast cancer diagnosis. Adherence to BCS was based on 2009 USPSTF 29 guidelines, and women were categorized as adherent (or received a timely mammogram) to mammography screening if they reported having a mammogram in the previous 2 years. A 90-day to 24-month window prior to breast cancer diagnosis was used to classify prior use of mammography. 30 The 90-day restriction was put in place to reduce the chances that diagnostic mammograms would be erroneously counted as screening mammograms.
The primary independent variable included the presence of one of the following chronic conditions: arthritis, musculoskeletal disease, degenerative joint disease, asthma, emphysema, chronic obstructive pulmonary disease, chronic lung disease, cardiovascular disease, hypertension, chronic digestive disease, chronic pain, low-back pain, diabetes mellitus, depression, anxiety, and substance abuse. All chronic diseases identified from diagnostic codes in Medicare data from the 2-year period prior to breast cancer diagnosis were included in this analysis. Each chronic condition was coded as a binary variable (1 =condition present, 0 = condition absent) and categorized to 0, 1–2, 3–4, and 5+ number of chronic diseases. Other patient factors known to influence BCS were included as covariates as follows:
Demographic variables. Race was categorized as either non-Hispanic White or non-White. Marital status was coded as single or married. Age was included as a continuous variable in multivariate analyses.
Health care access and utilization variables. The number of visits to a primary care provider (PCP) in the 2 years prior to diagnosis to 90 days prior to diagnosis time window was included as an indicator of medical need. The health care access and utilization variable describe encounters of PCP for preventive or chronic disease management. The number of PCP visits was identified from the Medicare Physician/Supplier Part B claims file. PCP visits were only PCP medical specialty care and consultation services in an office or ambulatory facility.
Environmental variables. County-level economic statutes defined by 2009 ARC were included. The index used the 3-year average unemployment rate, per capita income, and poverty rate to create five levels of county deprivation: distressed, at risk, transitional, competitive, and attainment. 31 No county in this study was at the attainment level during study time window. In addition, counties were categorized based on rurality as determined by the United States Department of Agriculture (USDA) rural/urban continuum code. 32 Finally, state of residence at the time of diagnosis was also included to control for unmeasured differences among states.
Analyses
Descriptive statistics were estimated to examine the characteristics of the study sample. Bivariate analyses examined the associations among BCS adherence, chronic diseases, and the covariates representing sample characteristics. Multiple logistic regression models were used to determine the association between BCS adherence and (1) the presence of a chronic disease and (2) the number of chronic diseases present. In each regression model, each independent variable was entered to obtain the unadjusted estimate on mammography. Next, each set of covariates were sequentially added to the model to develop a logistic regression model for each independent variable. The fully adjusted models examined the unique associations of the independent variables and BCS adherence after controlling for each set of covariates. All analyses were carried out using Stata 14.
Results
Table 1 shows the characteristics of the sample and results of bivariate tests of associations among the independent variables, covariates, and BCS adherence. The mean age of women in the sample was 76 years with a minimum of 65 and a maximum of 99 years (not shown). Ninety-seven percent of the sample was non-Hispanic White and a little over half of the sample lived in Pennsylvania at the time of diagnosis. About half of the sample (50.2%) had received a preventive mammogram before being diagnosed with breast cancer, while nearly 16% of the sample had no chronic disease. The percentage of women who adhered to BCS was higher among those 70–74 and 75–79 years than among younger or older women. More than half (59%) of women had 1 or 2 chronic diseases; 19% had 3 or 4 chronic diseases; and 6% of women had 5 or more chronic diseases. Having a mammogram within the past 2 years was associated with having at least one chronic disease, having one or two chronic diseases, being married, having seen a physician within the past 2 years, and living in a transit county.
Characteristics of sample by breast cancer screening status.
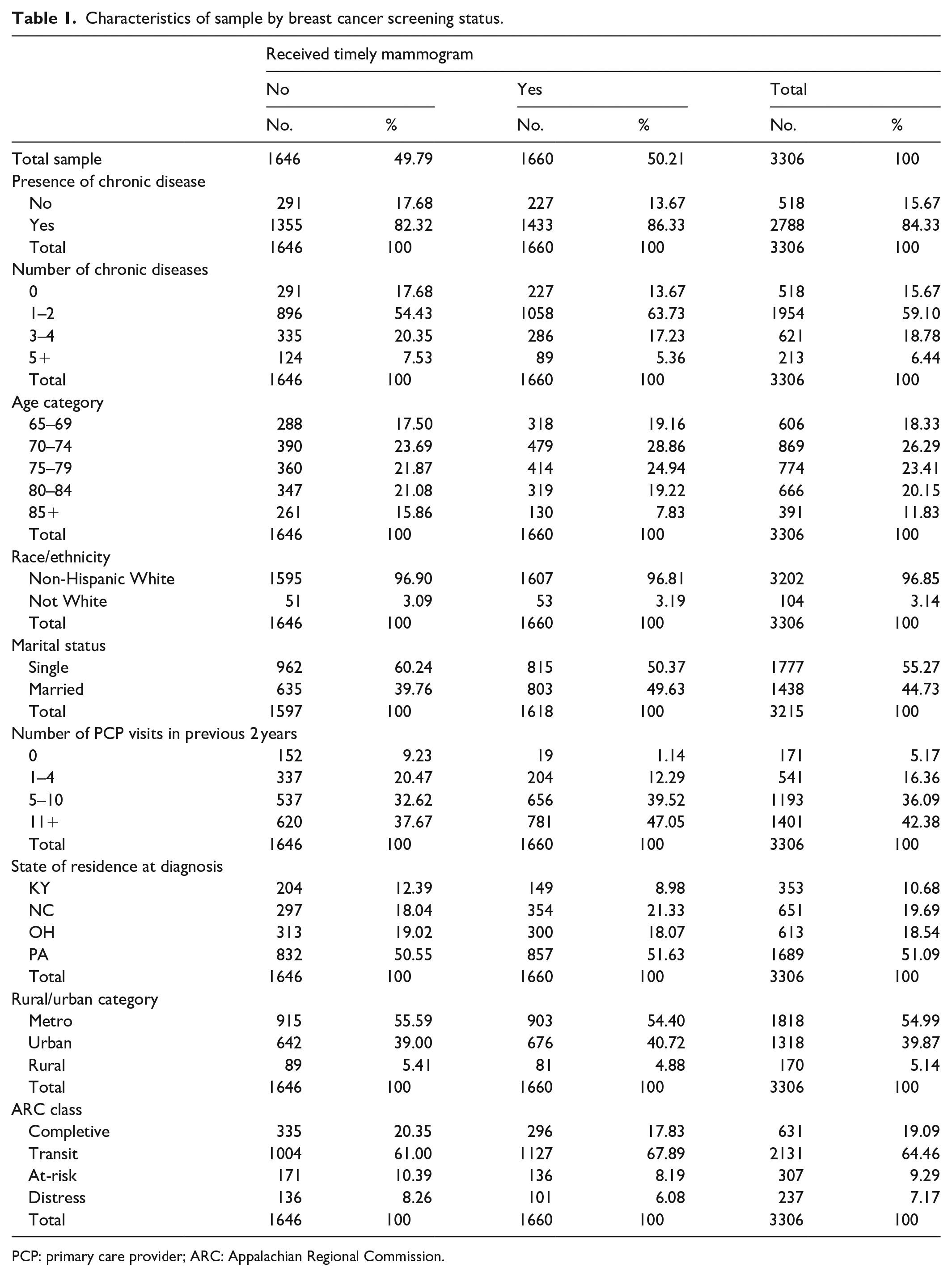
PCP: primary care provider; ARC: Appalachian Regional Commission.
Table 2 shows the association between having a chronic disease and BCS adherence, estimated in four models. In the unadjusted model, the presence of a chronic disease was associated with BCS adherence. Women with at least one chronic disease had 35% (confidence interval (CI): 1.122–1.637) higher odds of BCS adherence compared to women who did not have a chronic disease. This significance level remained (odds ratio (OR): 1.40, CI: 1.159–1.696) in the presence of county-level variables (model 2), but with the addition of demographic variables (model 3), the coefficient for chronic disease was no longer statistically significant. In the fully adjusted model (model 4), having a chronic disease was not a strong predictor for BCS adherence. The number of PCP visits was a strong predictor of BCS adherence, and the strength of the association increased as the number of PCP visits increased. Being married also increased that odds of BCS adherence (OR: 1.29, CI: 1.066–1.450). Finally, the odds of BCS adherence decreased with increasing patient age.
Logistic regression showing association between the presence of a chronic disease and having received timely mammogram.

ARC: Appalachian Regional Commission.
Exponentiated coefficients; 95% confidence intervals in brackets.
p < 0.05, **p < 0.01, ***p < 0.001.
Table 3 shows the association between number of chronic diseases and BCS adherence. The unadjusted model showed that having one or two chronic diseases was associated with an increased likelihood of BCS adherence (OR: 1.51, CI: 1.25–1.84). This significance remained when country-level variables were added to the model (model 2). When demographic variables were added to models 3 and 4, women with more than three chronic diseases were less likely to adhere to BCS guidelines. Model 4 shows that women with 3–4 chronic conditions had odds that were 33% (CI: 0.51, 0.88) lower than the reference group to adhere to BCS guidelines, while women with 5 or more chronic diseases had odds that were 41% (CI: 0.42, 0.86) lower. As in the previously analyses, BCS adherence decreased with increasing patient age, whereas being married (OR: 1.24, CI: 1.07, 1.45) and an increasing number of doctor visits was associated with greater BCS adherence.
Logistic regression showing association between numbers of chronic diseases and having received timely mammogram.

ARC: Appalachian Regional Commission.
Exponentiated coefficients; 95% confidence intervals in brackets.
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
This study aimed to determine the relationship between the presence and number of chronic diseases and BCS adherence among Medicare beneficiaries who reside in Kentucky, Pennsylvania, North Carolina, and Ohio. By controlling for factors known to predict BCS, results from this study highlight the presence of multiple chronic diseases as an additional barrier preventing elderly women from adhering to clearly beneficial screening recommendations. Half of the sample was being screened for breast cancer. Screenings rates of 50% are low given that this population of women has health insurance that covers mammograms. Contrary to this finding, Vyas et al. 33 found that Appalachian women age 65 years and above living in West Virginia have higher likelihood of being adherent to mammography screening guidelines due to the regular access to screening services. In addition to low screening rate, 84% of the sample reported the presence of at least one chronic disease, highlighting the importance of considering preventive services when patients are managing chronic conditions.
An association between the presence of a chronic disease and BCS adherence was not observed. However, adherence to BCS was inversely related to the number of chronic diseases, whereby women with three or more conditions had half the odds of having guideline-concordant screening compared to those without a chronic condition after controlling for socio-demographic, health, and county characteristics. These results confirm previous findings that having several chronic diseases presents a barrier to achieving guideline-concordant mammography screening.22 –24 Other studies have found that higher burden of chronic diseases was associated with increased rates of late stage cancer diagnosis,27,31 further highlighting the importance of preventive screening for patients managing chronic diseases. BCS strategies can be aimed specifically at increasing the number of screenings among vulnerable individuals who do not have a regular medical provider for the treatment of chronic conditions.
This study also found that women with more primary care visits were more likely to adhere to BCS guidelines. Since people with more chronic disease, theoretically, have more contact with health care providers throughout the year than those without chronic diseases, our results would have been expected to show that women with more chronic diseases were also more likely to be screened. There are several possible explanations for this discrepancy. Life-threatening or difficult to control chronic conditions were associated with increased uptake of screening mammography, while non-life-threating conditions were associated with decreased uptake of screening mammography. 34 This suggests that the type of chronic disease or the severity of each condition may have an indirect influence on screening adherence and not just the presence of a chronic disease. Future studies will need to consider if the presence of certain chronic condition or the severity of a disease predicts the number of provider visits. Another possible explanation is that Appalachian women with more chronic diseases are less likely to visit a PCP. Appalachia is an underserved region with a relative shortage of PCPs. 21
Having a chronic disease may further act as barrier that prevents women from seeking care from a provider due to lack of accessibility or high cost of care. 20 To investigate these points further, the study sample was stratified by number of PCP visits and the relationship between the presence, and number of chronic diseases, adjusted for other covariates, was re-examined (Table 4). Among women with no primary care visits, those with a chronic disease were more likely to adhere to BCS guidelines. This effect grew stronger as the number of chronic diseases present increased. Women in the category with the highest number of primary care visits (11 or more) were less likely to adhere to BCS guidelines. This implies that among women with chronic diseases, those without PCP visits adhere to BCS guidelines while those with primary care visits did not adhere to BCS guidelines. Despite having more PCP visits, some women may not follow through with cancer screening recommendations.
Adjusted logistic regression showing association between the presence- and number of chronic diseases and having received timely mammogram within each PCP category.
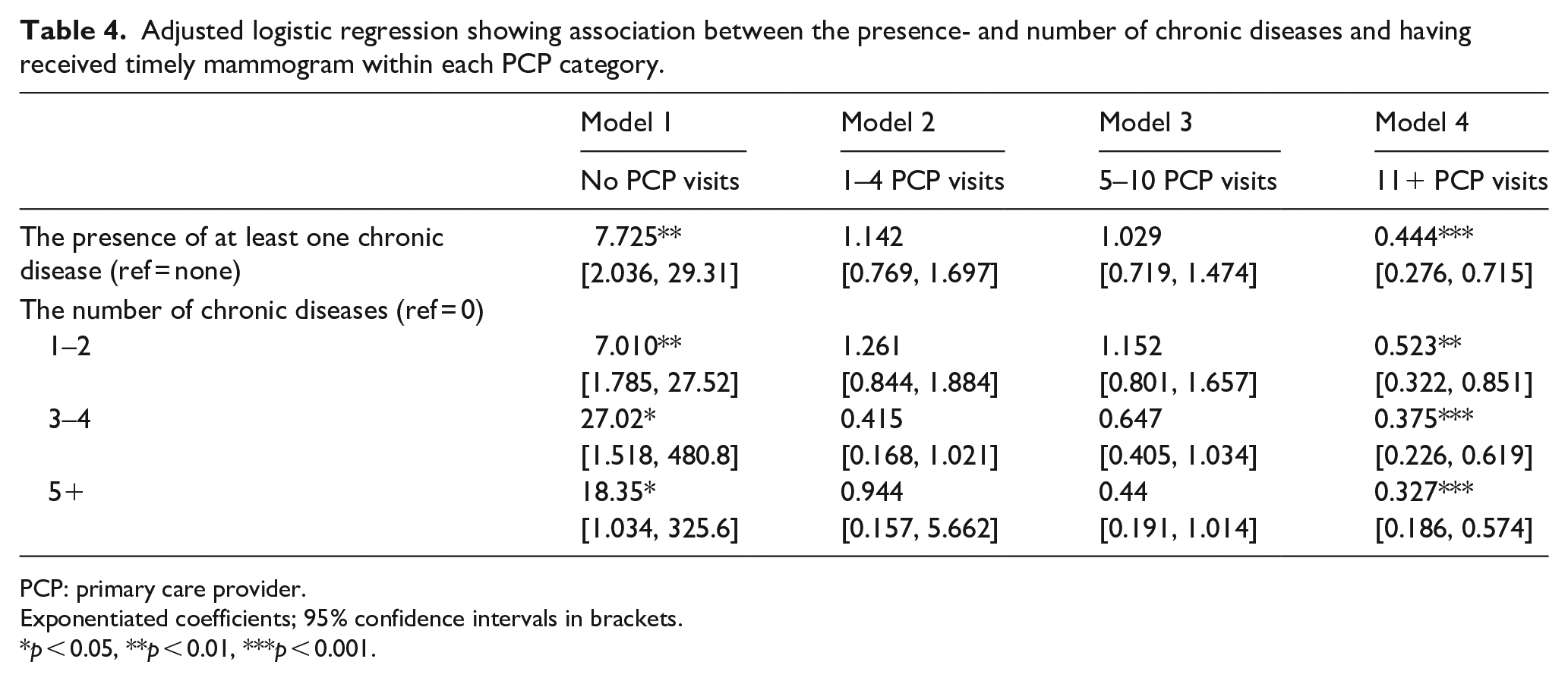
PCP: primary care provider.
Exponentiated coefficients; 95% confidence intervals in brackets.
p < 0.05, **p < 0.01, ***p < 0.001.
Alternatively, women without a regular PCP may rely more on urgent treatment centers, public health clinics, or emergency rooms for treatment for chronic conditions, and women do not always need a referral from a PCP to receive a mammogram. Suter and Elmore 34 found that some woman refer themselves for mammograms without a physician recommendation. In addition, among three of the major health insurers in Kentucky, only one of them required a mammogram referral from a doctor. In many cases, once an initial screening was conducted, subsequent appointments could be made at the screening center by the patient. 26 In addition, various local health departments offer free breast cancer services to those who are uninsured and less likely to have a usual source of care.
These findings are not consistent with other studies that show the level of rurality and county-level economic status act as a barrier to seeking health services among Appalachian residents. The observed associations seem to be explained by the individual-level factors, race, marital status, and primary care visits rather than the county-level variables included. One possible explanation is that chronic disease management is enough to overcome geographic barriers and leads women to seek care wherever they are, despite living in remote regions.
These results should be interpreted with a few limitations. As previously stated, an indicator for the severity of each chronic disease was not included. Future studies could use this variable to assess each woman’s probability of death from non–breast cancer causes or their risk of developing breast cancer and the possible influence that would have on screening decisions. Half of the women sampled were from Pennsylvanian counties. The level of heterogeneity within the Appalachian region and the fact that the sample was largely non-Hispanic White implies these results may not be generalizable to other parts of Appalachia or the rest of the country. Finally, the screening interval used to determine adherence to screening guidelines may be different in different parts of the states analyzed and does not necessarily represent long-term screening patterns for individuals resulting in misclassification between screening and diagnostic mammograms. Longitudinal studies that follow women over time to capture long-term screening patterns are to better classify mammograms but also determine whether regular screening help women with chronic diseases have lower morbidity and mortality from breast cancer.
Despite these limitations, this study has several strengths. It uses claims data and not self-reported use of mammograms or chronic disease diagnosis. This improves validity since the accuracy of self-reported information about cancer screening practices varies by patient characteristics and screening test and may differ from actual practice as individuals tend to over report their use of screening. 35 Having a homogeneous sample served as an advantage as lack of health insurance, screening costs and race/ethnicity have been found to be barriers for preventive services for women living in Appalachia. Results from this study may also help identify underserved, elderly populations that are under-screened for breast cancer based on health status yet face the highest rates of diseases. It may be important for specific age groups to be targeted for screening interventions especially those without a usual source of care, an important driver of screening. 31 Finally, having a physician recommendation is an important predictor of BCS utilization among women, even with regular visits. 36 Therefore, physicians need to be aware of any conscious or unconscious bias they may have toward screening recommendations for women with chronic conditions and also to understand barriers preventing women from following through with screening.
Public health implication
This study has considerable public health importance, considering that many more people are living into their 9th and 10th decades. Life expectancy will continue to increase through steady improvements in delaying the onset of and progression of chronic conditions and reducing mortality from chronic disease. With benefit declining during advancing age, screening older people should be more likely to lead to reduced disease-specific mortality, and increased quality of life. Older people are faced with increasingly burdensome, such as multiple chronic diseases, sensory, cognitive, and physical problems. Closing gaps in the delivery of clinical preventive services is one of the public health strategies for improving the health and quality of life of older adults. Considering an increase in the percentage of the population 65 or older by 2050, this study provides evidence to assist the nation’s efforts to prevent and control chronic diseases so that these added years translate into quality years.
Footnotes
Acknowledgements
The authors would like to acknowledgment the contributions and collaboration of the following people Rhonda BeLue, Marianne Hillemeier, Roger Anderson, and Fabian Camacho.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and consent
The study is a secondary analysis using data from the Center for Medicare and Medicaid Services. Institutional Review Board of Pennsylvania State University approved this study (STUDY00003080). The authors do not know the participants and did not collect the information directly from the patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.