
Abstract
Objective:
Most studies about truncal pain during and after pregnancy focus on low back pain, few prospectively define change in pain, and even fewer evaluate pain in all three major truncal areas: upper back, lower back, and pelvic girdle. Thus, the objective of this prospective cohort study was to describe, in primiparous women delivered vaginally, prevalence rates and severities of upper back, lower back, and pelvic girdle pain during pregnancy and 6–10 weeks postpartum and to describe the trajectory of pain constellations between time points.
Study design:
Participants completed questionnaires at each time point. Pain intensity was rated on a visual analogue scale ranging from 0 to 100.
Results:
Of the 288 participants, 94% reported truncal pain during pregnancy, while 75% did so postpartum. Prevalence rates of upper back, lower back, and pelvic girdle pain with or without other types of pain during pregnancy were 42%, 77%, and 74% and postpartum were 43%, 52%, and 41%, respectively. Pain severity was highest for women endorsing pain in three locations (median 55–60). Of women with the most common pain constellation during pregnancy, lower back and pelvic girdle (32%), 18% had persistent low back and pelvic girdle pain postpartum, 20% had no pain, and the remainder had pain in a different location. Of women with pain in all three locations during pregnancy (27%), 34% had persistent pain in three locations postpartum, 13% had no pain, and the remainder had pain in at least one location.
Conclusion:
More women experience pain in a constellation of locations than in a single location. Severity increases as number of pain sites increase. Women with pain in three sites during pregnancy are least likely to have pain resolve. Interventions should focus on the entire trunk and not simply one site of pain.
Introduction
The reported prevalence rates of pregnancy-related back and pelvic girdle pain range from 20% to 90% 1 and vary primarily due to differences in diagnostic criteria and terminology. In a review of 28 studies on pregnancy-related back and pelvic girdle pain, Wu et al. 2 estimated that 45% and 25% of women experience lumbopelvic pain during pregnancy and in the postpartum period, respectively. Back and pelvic girdle pain represent a significant burden to pregnant and postpartum women and can affect their mobility, ability to perform daily activities, and quality of life.3–12
Most of the studies about these common conditions are cross-sectional in nature, most investigate only one pain location (e.g. low back pain but not pelvic girdle pain), few assess upper back pain, 13 and most originate from populations outside of North America. In cohort studies, 15%–45%14–18 of women with pelvic girdle pain, back pain, or both during pregnancy continue to have pain between 1 and 3 months postpartum and 8.5%–51% report continued pain at 1–3 years postpartum.14,19–21 Limited data suggest that women with more than one type of truncal pain during pregnancy are more likely to report persistent pain postpartum. 9
Given that truncal pain is common and disruptive to quality of life, but prospective studies assessing its full spectrum are rare, the broad objective of this study is to add to our understanding of truncal pain in a population of primiparous women. Specifically, we aimed to (1) describe the prevalence rates of upper back, lower back, pelvic girdle, and overlapping pain constellations during pregnancy and at 6–10 weeks postpartum; (2) correlate visual analogue scale (VAS) pain severity scores at each site (upper back, lower back, and pelvic girdle) with pain constellation categories (pain at 1, 2, or 3 sites) for women with pain during pregnancy and again for women with persistent pain (pain at pregnancy and at 6–10 weeks postpartum); and (3) describe the trajectory of each pain constellation between pregnancy and postpartum.
Materials and methods
This observational prospective cohort study, ancillary to an ongoing study, 22 includes women who were enrolled in the parent study between the dates when questions about pain pertaining to this ancillary study were introduced (21 June 2016 for English speaking participants and 14 July 2016 for Spanish speaking participants) and 16 November 2017. The parent study was approved by the Institutional Review Boards at the participating sites, and all participants completed informed consent. Participants, nulliparous women >18 years and >28 weeks gestation, were recruited during prenatal visits at university and community clinics and community health centres. Other inclusion criteria for the parent study were English or Spanish speaking, singleton gestation, and planning vaginal delivery. Exclusion criteria for the parent study included major medical or surgical problems that precluded physical activity for the past 12 months (such as obstructive pulmonary disease or muscular dystrophy), collagen disorders that may increase the risk of pelvic organ prolapse (such as Marfan’s or Ehlers–Danlos syndromes), prior surgical procedures for urinary incontinence or pelvic organ prolapse, required ambulatory aid before pregnancy, and lack of access to a telephone or computer during the course of study. As the purpose of the parent study is to explore factors related to pelvic floor health after vaginal delivery, women delivered by caesarean were subsequently excluded after delivery.
Upper back, lower back, and pelvic girdle pain were assessed by questionnaire during the third trimester of pregnancy and again at 6–10 weeks postpartum. Back pain was operationalized according to a study which used a modified Delphi technique 23 as, ‘In the past four weeks, have you had pain in your lower back?’ This stem, used in the postpartum questionnaire, was modified in pregnancy to ‘During this pregnancy, have you experienced pain in your lower back?’ and ‘During this pregnancy, have you experienced pain in your upper back?’ We operationalized pelvic girdle pain consistent with the definition found in the 2008 European Guidelines for the diagnosis and treatment of pelvic girdle pain as, ‘During this pregnancy have you experienced pain “in the back side of your pelvic girdle?” or “in the front side of your pelvic girdle?”’ 24 Each question included an illustration of pain distribution (Figure 1). Women were categorized as having symptoms of pelvic girdle pain if they endorsed either front- or back-sided pain. Women who responded positively were then asked whether the pain was bad enough to limit usual activities or change daily routine for more than one day 23 and to rate the usual intensity of the pain on a VAS in which 0 represented no pain and 100 the worst possible pain. While a validated questionnaire exists for use in women with an existing diagnosis of pelvic girdle pain, 25 we were unable to identify such a tool for population-based research on pelvic girdle pain prevalence and therefore based our questions on the definition of pelvic girdle pain.

Illustration of pain distribution provided to participants.
Figure 2 details a flow diagram of eligible participants; 288 women were included in this final study.

Participant flow.
Adequacy of sample size
Statistical power calculations were performed for the analysis of (1) pain during pregnancy and (2) the trend in VAS scores at 6–10 weeks postpartum by number of pain sites at that time, for women with persistent pain, that is, women with no pain at either time point are excluded in the latter analysis. Based on approximation by statistical power calculations for Bonferroni-corrected tests of parametric or non-parametric correlations, the final sample size of n = 200 (after exclusions and missing values are taken into account) has more than 90% power to detect squared correlations of 0.10 (r = 0.32) between number of pain sites and VAS score for a particular type of pain (upper back, lower back, or pelvic girdle) at a single time point, at the two-sided 0.83% significance level (the overall 5% significance level was divided by six to take into account testing three types of pain at two different time points).
Statistical analysis
Prevalence rates of upper back, lower back, pelvic girdle, and overlapping pain constellations were tabulated for pregnancy and 6–10 weeks postpartum. We calculated means, standard deviations, medians, and ranges for women with nonzero scores in pain intensity according to the VAS score at each time point. As VAS scores did not always demonstrate normality, we elected to follow convention to present results as medians and ranges. 26 We proposed to perform multivariate linear regression to test whether VAS scores at each site increased as the number of sites of pain at each time point increased. However, residuals suggested non-normality, so we performed this analysis using Jonckheere’s test of trend and created boxplots of VAS scores by number of sites (not shown). Finally, we tabulated the trajectory of pain categories between pregnancy and 6–10 weeks postpartum. We a priori planned not to test differences between pain trajectories due to small cell sizes.
For combined pain constellations, women were considered to be limited by the pain if they responded ‘yes’ to the question about whether pain was bad enough to limit activities or change routine for any of the pain constellations. The VAS for this purpose was designated as the highest reported VAS for any pain type contained in that constellation (e.g. if a woman marked pain intensity as ‘60’ for upper back pain and ‘30’ for lower back pain, the VAS score for her combined pain constellation was ‘60’). We used SAS 9.4 for analyses.
Results
Participant characteristics are summarized in Table 1. The mean age at the pregnancy visit was 28.05 (5.31) years. Most (85%) were Caucasian and 23% were of Hispanic or Latina ethnicity.
Demographics of study populations (mean (SD) or n (%)).

BMI: body mass index.
Nearly all (94%) participants reported some type of pain during pregnancy, and 27% of all participants reported pain that limited daily activity. Table 2 summarizes the prevalence rates of pain and activity-limiting pain during pregnancy and postpartum. Postpartum, 75% and 13% of participants reported pain and pain that limited daily activity, respectively. During pregnancy, prevalence rates of upper back, lower back, and pelvic girdle pain with or without other types of pain were 42%, 77%, and 74%, respectively. The prevalence of upper back pain was similar during pregnancy and postpartum (42% and 43%, respectively), while the prevalence rates of lower back and pelvic girdle pain were lower in the postpartum period (52% compared to 77% during pregnancy and 42% compared to 74% during pregnancy, respectively).
Prevalence of pain constellations during pregnancy and postpartum.

UBP: upper back pain; LBP: lower back pain; PGP: pelvic girdle pain; NA: not applicable.
Missing all pain variables (1).
More women experienced pain in a combination of locations than in a single location at both time points (Figure 3). More than a quarter of women experienced pain in all three locations during pregnancy; this decreased to 14% of women postpartum.

Venn diagram demonstrating the overlap between pain locations.
The severities of pain across the pain constellations are summarized in Table 3. During pregnancy, pain severity ranged from 0 (in one woman) to 98 on the VAS scale, with severity lowest for women reporting low back pain only and highest for women endorsing pain in all three locations. Of the 212 women that provided VAS severity scores for pain postpartum, pain severity ranged from 1 to 91 on the VAS scale. Severity was lowest for the women endorsing pelvic girdle pain only and again highest for women endorsing pain in all three locations.
Pain severities across pain constellations during pregnancy and postpartum.
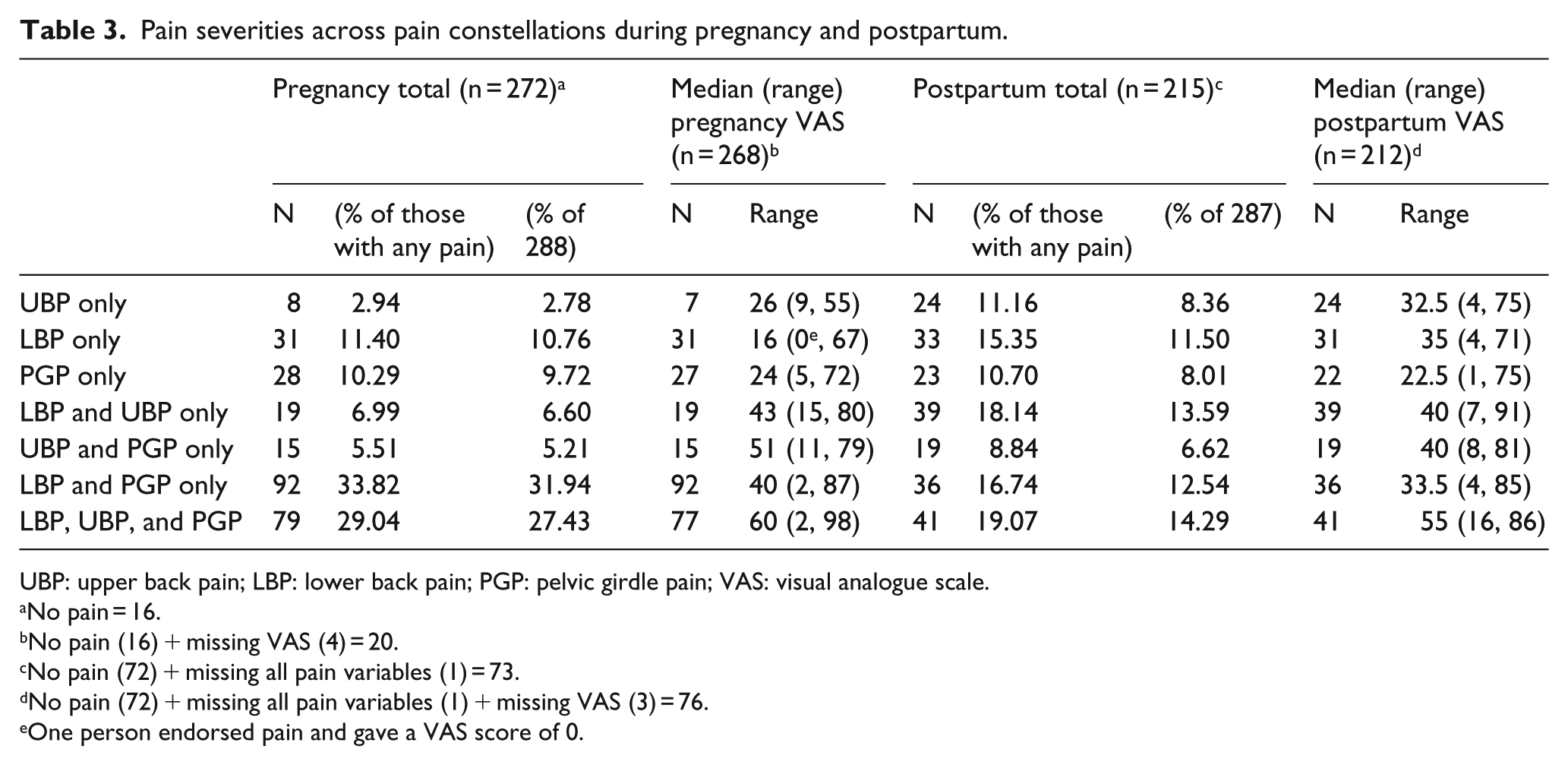
UBP: upper back pain; LBP: lower back pain; PGP: pelvic girdle pain; VAS: visual analogue scale.
No pain = 16.
No pain (16) + missing VAS (4) = 20.
No pain (72) + missing all pain variables (1) = 73.
No pain (72) + missing all pain variables (1) + missing VAS (3) = 76.
One person endorsed pain and gave a VAS score of 0.
There was a statistically significant trend in VAS scores for each of upper back, lower back, and pelvic girdle pain, in women with 1, 2, or 3 pain sites at third trimester. VAS scores increased as the number of sites in the pain constellation increased (p < 0.0001 for each variable by Jonckheere’s test of trend). For women with persistent pain (nonzero pain at some site at third trimester and nonzero pain at some site at 6–10 weeks postpartum), results were similar (p < 0.0001 for each variable).
The trajectories of pain over the two time points are described in Table 4. Resolution of any pain to no pain from pregnancy to postpartum ranged from 13% in women with all three pain types to 58% in women with low back pain only. Of women with pain in all three locations during pregnancy, 34% still had pain in all three locations postpartum, 53% had pain in at least one location, and 13% had no pain. Of women who endorsed pain in a single location during pregnancy, 21%–29% had pain in at least one additional location postpartum and 6%–29% endorsed pain in a new and different location. Of the 16 women with no pain during pregnancy, 10 went on to develop some type of pain postpartum.
Trajectory of pain constellations from pregnancy to postpartum.

UBP: upper back pain; LBP: lower back pain; PGP: pelvic girdle pain.
One woman with UBP and PGP during pregnancy had missing data at postpartum and is not included in this table.
Discussion
The prevalence of truncal pain is high in both pregnancy and postpartum. Nearly all women (94%) in this study experienced some form of pain in the pregnancy and a majority (75%) experienced pain postpartum. More women experienced pain in a constellation of locations than in a single location. For example, two-thirds of women in the pregnancy had low back pain in combination with upper back and/or pelvic girdle pain, but only 11% of women have low back pain only. While the prevalence rates of both back and pelvic girdle pain were higher in pregnancy than postpartum, the prevalence of upper back pain was similar in both time points.
Not surprisingly, the prevalence of any reported pain was quite high, but it is notable that a significant minority of women, 27% during pregnancy and 13% postpartum, had pain that limited daily activity. The more locations in which women reported pain, the greater they rated their pain severity. Women who experienced upper back, lower back, and pelvic girdle pain together reported the highest VAS scores and were also the most likely to report pain that limited daily activity at both time points. Women who experienced pain in all three locations during pregnancy were also the least likely to have their pain resolve; only 10 of the 79 (13%) women with pain in all three locations in pregnancy reported no pain postpartum. Experiencing pain in all three locations carries greater morbidity, suggesting that the effects of truncal pain in this population are additive.
The prevalence of low back pain in this study, 77% in pregnancy and 52% postpartum, is near the upper limit of values cited in the literature (20%–90% in pregnancy 1 and 0.3%–67% postpartum). 2 This study used a self-reported questionnaire to assess back and pelvic girdle pain, so higher rates were not unexpected. Our findings are consistent with a recent study on back and pelvic girdle pain in pregnancy in which the authors operationalize pain with the same questions stems as this study. 27
We are aware of only one other study that queried upper back pain in pregnancy and none that did so postpartum. 13 The authors operationalized pain with a self-reported questionnaire and pain drawings similar to that used in this study. About 10% of women reported ‘high back pain’ or ‘pain above the lumbar region only’ at 36 weeks in that study. This is greater than the number of women who reported upper back pain only in this study (8 of 288, 3%), but less than the number who reported upper back pain with or without other types of pain (121 of 288, 42%). To our knowledge, this is the only other study to report upper back, lower back, and pelvic girdle pain together. It is clear that prevalence rates differ according to whether the pain is limited to one location or includes one location among others. Few studies about back or pelvic girdle pain postpartum are prospective in design, and these generally report the persistence rate of one pain location from pregnancy to postpartum.14–21,28–30 We found rates of persistent low back pain (with or without additional pain categories added) between 35% (11 of 31) for women with low back pain only in pregnancy to 67% (53 of 79) for women with a combination of upper back, lower back, and pelvic girdle pain in pregnancy. The prevalence of pain postpartum persisting in at least one of the three locations for women who reported all three types of pain in pregnancy is well above the rates of persistent low back pain alone or pelvic girdle pain alone cited in previous literature (15% to 45% at 1–3 months postpartum).14–18
A much smaller proportion of women in our study reported the persistence of the exact same pain constellation that they endorsed in pregnancy; rather, most changed their pain constellation. For combinations of low back pain, this ranged from 6% (2 of 31) for women who reported low back pain only in the pregnancy to 16% (3 of 19) and 18% (17 of 92) for women who reported low back pain plus one other pain location to 34% (27 of 79) for women who reported pain in all three locations. Of women who reported no pain in the pregnancy, 63% (10 of 16) developed some sort of pain postpartum. These changes in pain constellation suggest differences in the aetiology of pain between the pregnancy and postpartum. This could be secondary to biomechanical changes following delivery or differences in daily activity between the pregnancy and postpartum (such as carrying a baby). In addition, it is likely difficult for women to completely differentiate each pain location, given that they all exist along the trunk.
That combinations of upper back, lower back, and pelvic girdle pain are highly prevalent in both pregnancy and postpartum suggests that asking women about all types of truncal pain, and not only low back or pelvic girdle pain, is important, so that clinicians can intervene. Compared to women who do not report back and pelvic girdle pain postpartum, women with pain report worse sleep, 9 lower self-rated health, 10 impaired ability to work and care for their children, 8 psychological stress, 3 and emotional detriment.4,8,12 The period from birth to 12 weeks postpartum is a transition period with unmet maternal needs, including addressing pain. 31 In one study, only 59% of US women with back and pelvic girdle pain informed their providers. 27 Only one-quarter received treatment – but of those who did, most reported benefit. Various interventions have demonstrated benefit, such as significant reductions in pain rating and disability scores, on back and pelvic girdle pain in pregnancy and postpartum, including manual therapy, physical exercise, education, yoga, and acupuncture.4,24,32–35 Previous interventions have targeted low back and/or pelvic girdle pain.32–35 Recognizing that upper back pain is not only prevalent, but contributes to greater morbidity combined with low back and pelvic girdle pain, presents an opportunity to target that symptom in future interventions.
Strengths of this study include the prospective cohort design, high questionnaire completion rate, and the collection of unique aspects of pain to include upper back pain, overlapping pain symptoms, and the trajectories of different combinations of pain locations between pregnancy and postpartum. This study is limited in generalizability. Our study population included only healthy primiparous women delivered vaginally in a US city with a relatively homogeneous population, though over 20% of participants were of Hispanic/Latina ethnicity. Women delivered by caesarean section were excluded from this study after delivery per protocol for the parent study. However, we found no significant differences in prevalence rates of pain constellations during pregnancy between these groups (data not shown). A self-reported questionnaire reflects participants’ subjective perceptions of pain rather than an objective measure of a condition. However, since the outcome of this study – pain – is primarily a symptom, focusing on the patient perspective still provides important clinical insight into women’s lived experiences. Finally, we did not collect information about whether women were treated for their pain during pregnancy or postpartum.
In conclusion, the prevalence of truncal pain is high both during pregnancy and postpartum. More women experience truncal pain in a constellation of locations than in a single location. Severity increases as number of pain sites increases. Women with pain in all three locations during pregnancy are least likely to have pain resolve postpartum. Given the diffuse nature of truncal pain and the large cross-over between pain sites in and after pregnancy, interventions should focus on the entire trunk and not simply one site of pain. In addition, as two-thirds of women that reported no pain during pregnancy went on to develop some type of pain postpartum, preventive interventions may also be important. Researchers interested in understanding the impact of an intervention on one type of truncal pain should collect information about all types of truncal pain to fully understand the impact of the intervention on resolution pain.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IN received an honorarium from Elsevier. The remaining authors had no competing financial interests to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant no. 1P01HD080629). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. The study sponsor had no role in the collection, analysis, and interpretation of data or writing of the manuscript.