
Abstract
Vitamin D a fat-soluble steroid hormone signals through Vitamin D Receptors (VDRs) located throughout the ovaries, uterus, placenta, hypothalamus, and pituitary gland, influencing immune regulation and female reproductive physiology. This review of studies from 2013-2025 found consistent associations between low vitamin D status and various disorders in women of childbearing age. In Premenstrual Syndrome (PMS), deficiency correlates with higher symptom severity, and evidence shows that supplementation significantly reduces total PMS scores, particularly improving mood-related domains. For uterine pathologies such as fibroids, endometriosis, and adenomyosis, low vitamin D status is linked to increased risk and severity. Repletion trials suggest antifibrotic and analgesic benefits, although larger, more rigorously designed studies are still needed for definitive clinical guidelines. In Polycystic Ovary Syndrome (PCOS), low vitamin D links to adverse metabolic and hormonal profiles. Multiple randomized controlled trials (RCTs) confirm that correcting deficiency improves insulin resistance, lowers total testosterone and free-androgen index, raises sex-hormone-binding globulin (SHBG), and helps regularize menstrual cycles. Targeted supplementation is recommended, especially for insulin-resistant or obese phenotypes. During pregnancy, maternal deficiency is associated with adverse outcomes including pre-eclampsia, gestational diabetes, and pre-term birth risk. However, intervention trials have yielded inconsistent preventive results, often complicated because rising Vitamin D-Binding Protein (VDBP) may mask true vitamin D status. In Assisted Reproduction like In Vitro Fertilization (IVF), correcting deficiency early during pre-conception or early folliculogenesis appears beneficial. This early dosing enhances oocyte quality, promotes granulosa cell proliferation, and modulates local transcriptomes toward anti-inflammatory pathways. In contrast, single high-dose boluses administered shortly before embryo transfer show limited impact on outcomes. The overall evidence is limited by heterogeneous study designs, variable dosing, and reliance on total serum levels rather than bioavailable vitamin D. Future research should prioritize large, multicenter RCTs utilizing standardized daily/weekly dosing, stratifying by genetic and phenotypic factors, and measuring bioavailable vitamin D to establish reliable effects on patient-centered outcomes.
Plain language summary
Although commonly classified as a vitamin, vitamin D functions as a critical hormone with extensive influence on female reproductive health. This review synthesizes findings from studies published between 2013 and 2025 to elucidate the relationship between vitamin D status and common reproductive conditions in women of childbearing age. Vitamin D plays a significant role in modulating reproductive hormones. Clinical evidence indicates that supplementation can alleviate premenstrual symptoms, particularly those related to mood. In women with Polycystic Ovary Syndrome (PCOS), vitamin D has been associated with the restoration of ovulatory cycles. Furthermore, insufficient vitamin D levels are linked to uterine pathologies with preliminary data suggesting that repletion may reduce pain symptoms. During pregnancy, adequate vitamin D supports maternal immune tolerance and proper placental development, potentially lowering the risk of complications including preeclampsia and preterm birth. Despite these promising associations, the existing body of research is constrained by methodological limitations, including small sample sizes, heterogeneous study designs, and inconsistent approaches to measuring vitamin D status. Notably, while several trials employed high-dose regimens (50,000 IU weekly), potential adverse effects were also reported. Future research priorities should include large-scale, multicenter randomized controlled trials targeting vitamin D-deficient women. Such studies should employ standardized supplementation protocols initiated prior to conception and focus on clinically meaningful outcomes such as live birth rates. Additionally, more precise measurement of bioavailable vitamin D and incorporation of genetic determinants are necessary to develop evidence-based clinical guidelines.
Introduction
Vitamin D is a fat-soluble steroid hormone that acts more like a hormone than a traditional vitamin, relying on cutaneous synthesis triggered by UVB exposure, subsequent hydroxylation in the liver and kidneys, and transport via vitamin D binding protein (VDBP) to mediate its biological effects. Its activation is strictly regulated through coordinated expression of genes encoding the vitamin D receptor (VDR) and key metabolic enzymes (CYP2R1, CYP27B1, CYP24A1), which together sustain homeostasis. 1
The primary source of vitamin D is cutaneous synthesis upon exposure to ultraviolet B (UVB) radiation, which converts 7-dehydrocholesterol to cholecalciferol (D3). This inactive precursor is transported by VDBP to the liver, where it undergoes hydroxylation to form 25-hydroxyvitamin D [25(OH)D3], the major circulating metabolite. Further hydroxylation in the kidneys yields the biologically active form, 1,25-dihydroxyvitamin D [1,25(OH)2D3] (calcitriol).2,3 The regulation of this synthesis and hydroxylation involves coordinated control of VDR and key metabolic enzymes (CYP2R1, CYP27B1, CYP24A1), which collectively preserve vitamin D balance. 4 In addition to endogenous synthesis, vitamin D can be obtained from few dietary sources as ergocalciferol [25(OH)D2], fortified foods (e.g. milk, cereals, fruit juices, eggs) and supplements; all of which contribute to overall vitamin D status. 5
Vitamin D plays an essential role in modulating female reproductive hormones, with its receptors (VDR) expressed across multiple reproductive tissues, including the placenta, ovaries, uterus (both endometrium and myometrium), fallopian tube, and central reproductive regulators such as the hypothalamus and pituitary gland.6–8 The presence of VDRs in granulosa cells of ovarian follicles further emphasizes the involvement of vitamin D in follicular development and steroidogenesis. This widespread distribution of vitamin D receptors highlights its significant influence on reproductive physiology, including hormone synthesis, ovulation, implantation, and overall fertility.6,9,10
Vitamin D inadequacy is prevalent in women of childbearing age and associates with higher adiposity and lower muscle mass.11,12 In infertile women vitamin D shows negative associations with BMI and waist circumference.
13
Mechanisms include adipose sequestration and volumetric dilution of vitamin D, alongside reduced hepatic CYP2R1 gene activity in obesity.
12
Population data show lower vitamin D in women with infertility or decreased fecundability.
14
Given the complex interplay between vitamin D biology and female reproductive endocrinology, and the heterogeneity of existing clinical findings, this narrative review consolidates evidence from mechanistic studies, observational research, and randomized trials to summarize vitamin D’s physiological roles in female reproduction, evaluate clinical associations and trial data across key conditions (PMS, PCOS, uterine pathologies, pregnancy, and IVF), and identify methodological gaps and priorities for future research Figure 1. Vitamin D metabolism within the body starting from the skin, UVB exposure converts 7-dehydrocholesterol in the skin to vitamin D3 (cholecalciferol), while diet supplies vitamin D2 (ergocalciferol). Both forms enter the circulation and are hydroxylated in the liver to 25(OH)D, then activated in the kidney to 1.25(OH)2D3, this active form acts through VDR which is expressed in the hypothalamus, pituitary gland, ovaries, uterus, fallopian tubes, and the placenta. Created by Azza Alsuwaidi et al. using BioRender software.
Methodology
This narrative review was conducted in alignment with principles recommended by SANRA (Scale for the Assessment of Narrative Review Articles) 15 to ensure a comprehensive and high-quality integration. While no prior protocol was registered, no quantitative meta-analysis was performed, and a formal risk-of-bias assessment of individual studies was not conducted. Efforts were made to apply systematic and transparent literature search methods. Electronic databases including PubMed, Google Scholar, Scopus, Cochrane library, and Web of Science were systematically searched for relevant studies published between 2013 and 2025. The search strategy incorporated a combination of medical subject headings and free text terms related to both vitamin D and reproductive health conditions in females. Key search terms for the exposure included “vitamin D″, “25-hydroxyvitamin D”, “VDR”, and “Cholecalciferol”, while reproductive outcomes were captured using terms such as “polycystic ovary syndrome”, “fertility”, “IVF”, “ovarian reserve”, “endometriosis”, “pregnancy”, and “Premenstrual syndrome”. Boolean operators (AND between concept blocks, OR within them) and phrase searching were applied to optimize retrieval. Eligible studies included observational research, randomized controlled trials, and mechanistic investigations examining vitamin D status, supplementation, VDR activity, or associated reproductive outcomes. Throughout this review, evidence hierarchy was considered when drawing conclusions about therapeutic efficacy. Priority was given to findings from randomized controlled trials for questions of supplementation benefit, while observational studies were primarily used to establish associations, describe prevalence, and generate mechanistic hypotheses. Where discrepancies exist between study types, these are explicitly noted and discussed as areas requiring further investigation. Prioritization for inclusion was based on studies focusing on women of reproductive age. Therefore, post-menopausal studies were excluded. Only studies in English language were included. Full texts were assessed following title and abstract screening, and bibliographies of included studies were manually reviewed to capture any additional relevant literature.
Throughout this review, we apply a hierarchical framework to interpret evidence: biological plausibility (mechanistic studies, animal models, VDR expression) establishes potential pathways; associations (observational studies) identify relationships that may exist but cannot prove causality; surrogate marker improvement (RCTs showing changes in intermediate endpoints) suggests biological activity but does not guarantee clinical benefit; and proven clinical benefit (RCTs demonstrating improved patient-centered outcomes). Where interventional data conflict with observational findings, these tensions are explicitly discussed as areas requiring further investigation. This framework is essential because vitamin D research is particularly prone to confounding-factors such as sun exposure, adiposity, physical activity, and dietary patterns independently influence both vitamin D status and reproductive outcomes, potentially creating spurious associations.
Vitamin D’s role in female reproductive hormones and fertility
To lay the groundwork for this review, the first section is going to explain how vitamin D impacts the regulation of female hormones which are key to reproductive health. Several hormones that are central to fertility, including anti-mullerian hormone (AMH), luteinizing hormone (LH), follicle stimulating hormone (FSH), estradiol, and androgens, as well as the ovarian insulin-like growth factor axis (IGFBP-1/IGF) and more are influenced by Vitamin D. Acting through the VDR in ovarian granulosa cells and central neuroendocrine hubs, vitamin D tunes follicle recruitment and reserve by modulating AMH expression and signaling, with evidence that supplementation raises AMH and helps temper the abnormally high levels, in part by reducing AMHR-II activity via SMAD pathway restraint.16–19 At the level of gonadotropins, vitamin D is linked to hypothalamic and pituitary control, where it can shift the LH/FSH balance in toward a more ovulatory pattern and enhance granulosa cell responsiveness to FSH, supporting healthy folliculogenesis.20,21 Within steroidogenesis, vitamin D promotes estradiol synthesis by upregulating aromatase and other key enzymes, and supports progesterone output through increased expression of StAR and 3B-HSD, reinforcing luteal function essential for implantation.9,22 In hyperandrogenic states, improving vitamin D status is associated with lower circulating androgens and free androgen index and higher sex hormone binding globulin changes that ease the hormonal bottlenecks hindering ovulation.23,24 Finally, vitamin D interfaces with ovarian IGF axis by regulating IGFBP-1, a gatekeeper of local IGF bioactivity that coordinates granulosa cell growth and differentiation.
17
Taken together these coordinated actions highlight vitamin D as a key regulator in the reproductive system, helping to synchronize hormonal rhythms, steroid production, growth factor signaling, and reserves, all in ways that promote healthy cycles and improve the chances of conception (Figure 2). With this foundation in mind, the following sections will explore in detail the role of vitamin D in various female reproductive conditions. Key pathways through which vitamin D influences female reproductive function, including regulation of AMH signaling, follicular FSH sensitivity, steroidogenic enzyme expression, progesterone and estradiol production, androgen availability, IGF-related pathways involved in folliculogenesis and modulation of placental steroidogenic and immune pathwyas. These proposed mechanisms are based on emerging evidence and remain under active investigation. Created by Azza Alsuwaidi et al. using BioRender software.
Vitamin D and premenstrual syndrome (PMS)
The relationship between vitamin D and PMS emerges from convergent but varied body of evidence, randomized trials, mechanistic studies, population analyses, and nutrigenetic data together indicate that vitamin D status is plausibly involved in both the biological pathways that generate PMS symptoms and in clinically meaningful symptom reduction when deficiency is corrected, however, the effect size, affected symptom domains, and the baseline deficiency vary across studies and contexts. Mechanistically, vitamin D behaves as a neurosteroid with receptors in brain regions and reproductive tissues, modulating neurotransmitter synthesis (serotonin, dopamine, Gamma-aminobutyric acid), calcium homeostasis, and immunoinflammatory signaling pathways that map directly onto mood, pain, sleep, and fluid retention features of PMS.25–28
High quality RCTs that targeted women with hypovitaminosis D (vitamin D insufficient or deficient) consistently show that restoring serum vitamin D to sufficient levels reduces total PMS symptoms scores and yield the largest benefits in mood related domains. For example, fortnightly 50,000IU dosing raised mean serum vitamin D into sufficient range and achieved significant reduction in total PMS scores with particularly large improvements in depression/anxiety subdomains. 26 Complementing these clinical effects, a mechanistically focused randomized trial in vitamin D deficient university students with a mean age of 21.3±1.6 demonstrated that vitamin D correction markedly lowered proinflammatory cytokines and increased total antioxidant capacity, changes that parallelled clinically meaningful symptom improvement, supporting an inflammation/oxidative stress pathway linking deficiency to symptom burden. 25
The evidence is not uniformly simple, trials comparing vitamin D against psychosocial intervention or alternative delivery methods reveal important qualifiers, a three-arm RCT that compared weekly vitamin D tablets with online positive oriented counseling and lifestyle training found all three interventions reduced PMS scores, but counselling produced the greatest and most durable symptom reductions and higher satisfaction, while vitamin D’s benefits attenuated after supplementation stopped, implying that sustained biochemical repletion or maintenance dosing may be required for ongoing symptom control, and that psychosocial skills can deliver longer lasting functional gains independent of serum levels. 29 It is worth noting that the delivery format and target population can significantly modify the outcomes of supplementation. A pilot trial using nano-encapsulated vitaminD3 fortified in dairy successfully raised serum vitamin D levels across subgroups but produced a significant reduction in restless legs syndrome severity only in women with severe PMS, suggesting a threshold or subgroup effect in which fortified dietary approaches may benefit those with greatest baseline symptom burden or comorbidity such as abdominal obesity. 30 Similarly, high single or loading doses of vitamin D reduced primary dysmenorrhea pain and analgesic use in deficient young women, but did not change menstrual blood loss, indicating that vitamin D’s anti-prostaglandin or nociceptive modulation alleviates pain without necessarily altering hemostatic or endometrial bleeding mechanisms. 27
Observational and population levels studies provide complementary context as well. Analysis of NHANES data shows that vitamin D insufficiency or deficiency is associated with short sleep duration in reproductive aged females and that coexisting iron deficiency amplifies sleep problems, this finding is relevant to PMS because sleep disturbance and fatigue are common PMS symptoms and may be exacerbated by combined micronutrient deficits, suggesting clinicians should screen for both nutrients when sleep or PMS complaint occur simultaneously. 31 A large cross-sectional dietary study in Turkey found that average vitamin D intakes were far below recommended levels across both healthy and symptomatic women, which complicates cross-sectional associations but emphasizes population level inadequacy as a public health concern rather than as a differentiator of case status in that cohort. 32 In contrast, a case-control study from District Sialkot in Pakistan found an extremely strong association where 100% of PMS cases were vitamin D deficient versus only 10% of controls, arguing that in some populations vitamin D deficiency may be a dominant, modifiable risk factor for PMS severity and that local epidemiology such as sun exposure, diet, and cultural practices, can determine the population attributable risk. 28
Summary of studies on vitamin D and PMS.
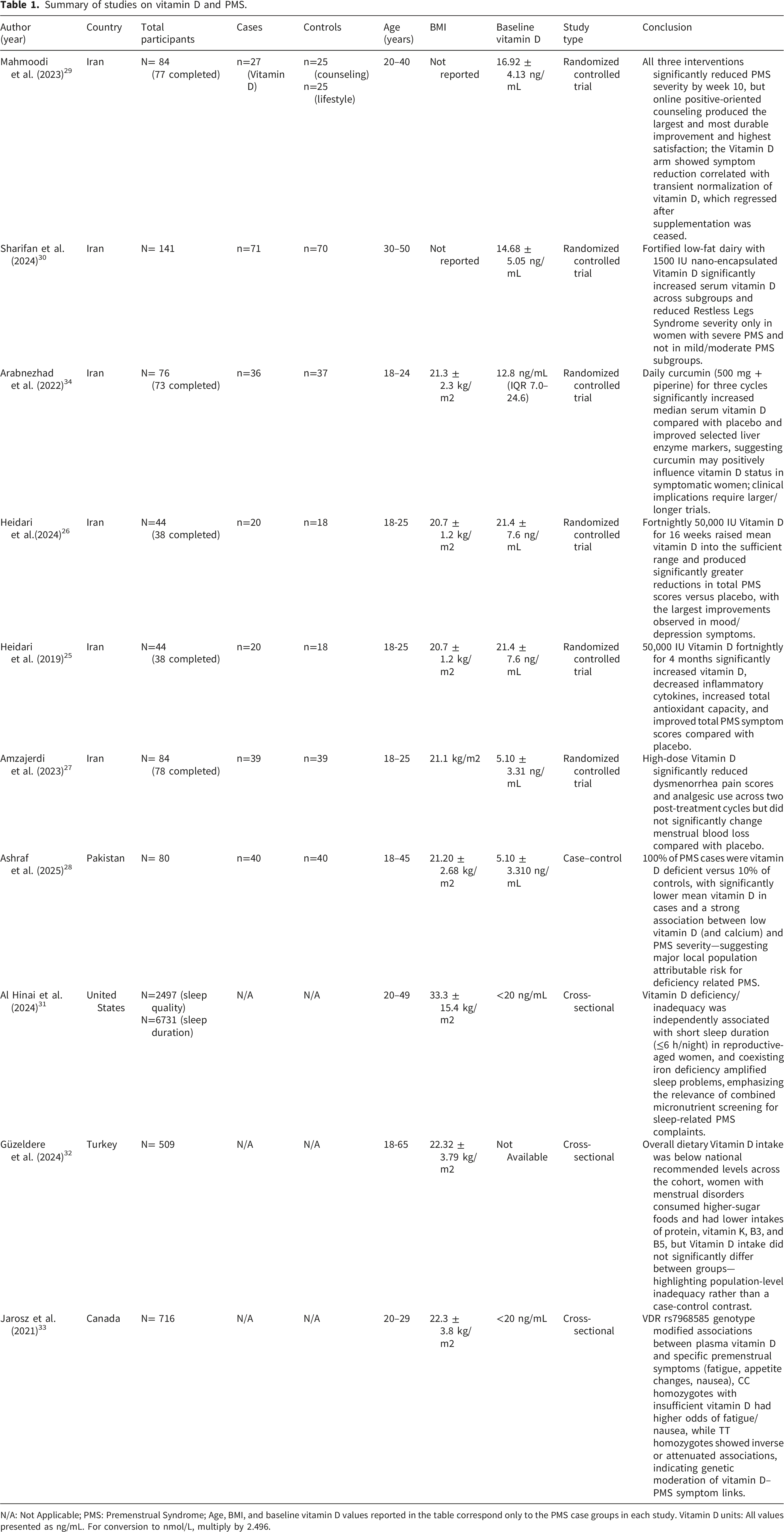
N/A: Not Applicable; PMS: Premenstrual Syndrome; Age, BMI, and baseline vitamin D values reported in the table correspond only to the PMS case groups in each study. Vitamin D units: All values presented as ng/mL. For conversion to nmol/L, multiply by 2.496.
Vitamin D and Polycystic Ovary Syndrome (PCOS)
Before examining the evidence, it is critical to distinguish between well-documented metabolic effects and less consistent reproductive outcomes in PCOS. While multiple RCTs demonstrate that vitamin D repletion improves insulin resistance, lipid profiles, and androgen measures representing surrogate marker improvement translation of these changes into enhanced ovulation, clinical pregnancy, or live birth rates remains inconsistent across studies. This disconnect may reflect heterogeneity in PCOS phenotypes, baseline vitamin D status, supplementation regimens, and the multifactorial nature of infertility in this population.
Across cross-sectional and intervention studies, vitamin D deficiency is notably common in women with PCOS across different populations and correlates with worse reproductive and metabolic phenotypes, suggesting both a marker and a modifiable contributor to disease expression.35–37 Mechanistically, Vitamin D signaling is present throughout the reproductive axis and in metabolic tissues, providing pathways to influence folliculogenesis, gonadotropin balance, androgen bioavailability via sex hormone binding globulin (SHBG), insulin secretion/action, adipokine production (adiponectin) and even endometrial receptivity mechanisms supported by both human trials and preclinical models.17,18,36,38–40 RCTs offer deeper insights: supplementation regularly corrects serum vitamin D and in many studies improves ovulation rates, dominant follicle development, menstrual regularity, androgen measures (total testosterone, free androgen index) and hirsutism scores, yet translation into consistent increase in clinical pregnancy or live-birth rates remains less robust and likely multifactorial. 23 In a prospective study of 100 vitamin D deficient PCOS women, adding weekly/monthly vitamin D (60,000 IU) and daily calcium (1000 mg) to metformin significantly regularized menstrual cycles and reduced mean ovarian volume by 30%. 41 Similarly, high-dose Vitamin D (50,000 IU weekly) in vitamin D deficient overweight women produce significant reductions in total testosterone, free androgen index, and hirsutism and increased SHBG and ovarian sonographic normalization and cycle regularity, yet showed some regression after cessation, highlighting dose, duration and maintenance as practical considerations for sustained benefit. 23 In contrast a small observational study reported unexpectedly higher serum vitamin D levels the PCOS positive subjects and proposed possible enhanced accumulation linked to hyperandrogenemia, highlighting population heterogeneity and contrasting many deficiency focused reports. 42
Metabolic endpoints in PCOS show a consistent but phenotype dependent pattern: vitamin D repletion improves indices of glucose handling (fasting plasma glucose, certain oral glucose tolerance test time points), Beta-cell function (HOMA-B), adiponectin, and insulin concentrations, homeostatic model of insulin resistance (HOMA-IR), and atherogenic lipids (triglycerides, total cholesterol, Low density lipoprotein) especially in obese or insulin resistant subgroups as shown in several RCTs and descriptive cohorts whereas effects are blunted or absent in lean/non-insulin resistant PCOS phenotypes.43,44 supporting this observation, a cross-sectional study of 50 Indian women with PCOS found that 84% were vitamin D deficient, where deficiency was associated with higher HOMA-IR, and elevated parathyroid hormone in 64% of participants. 45 Moreover, a randomized trial showed significant rises in adiponectin and decreases in fasting glucose and improved beta-cell function after eight weeks of high dose supplementation, while visceral fat changes were not significant over that short interval, indicating some metabolic pathways respond faster than body composition endpoints. 44 Observational and clinical data also link low vitamin D with dyslipidemia and an atherogenic profile in infertile PCOS women, strengthening the argument for vitamin D assessment in cardiovascular risk stratification in this group. 37
Beyond metabolism and reproduction, vitamin D appears to affect neuropsychological symptoms that commonly co-occur with PCOS, such as mood, anxiety and sleep, particularly when supplemented with omega 3 fatty acids, suggesting compounded neuroendocrine and anti-inflammatory effects that may indirectly benefit PCOS management and quality of life. 46 Preclinical work in vitamin D deficient hyperandrogenic rodent model reinforces causality, vitamin D deficiency alone induced polycystic ovarian morphology and when combined with hyperandrogenism it exacerbated anovulation, increased oxidative and nutritive stress, lowered estrogen receptor density, and impaired vascular relaxation which are all mechanistic pathways that plausibly link vitamin D status to both reproductive failure and increased cardiovascular vulnerability in PCOS. 40 Genetic context further complicates the picture: polymorphisms in the VDR (e.g. ApaI, BsmI, Cdx2, Taq1) are associated with altered PCOS susceptibility and may modify metabolic responses to supplementation, arguing for more personalized intervention trials that stratify by genotype and phenotype. 18
Summary of studies on vitamin D and PCOS.

N/A: Not Applicable; PCOS: Polycystic ovary syndrome; FAI: Free androgen index; SHBG: Sex hormone binding globulin; TC: total cholesterol; TG: triglycerides; LDL: low density lipoprotein; VLDL: very low density lipoprotein; HDL: high density lipoprotein; FSH: Follicular stimulating hormone; LH: luteinizing hormone; AMH: anti-mullerian hormone; PTH: parathyroid hormone; Age, BMI, and baseline vitamin D values reported in the table correspond only to the PCOS case groups in each study. Vitamin D units: All values presented as ng/mL. For conversion to nmol/L, multiply by 2.496.
Vitamin D and uterine pathologies: Fibroids, endometriosis, and adenomyosis
The relationship between vitamin D and estrogen-dependent uterine pathologies is supported by robust biological plausibility, including anti-inflammatory, anti-proliferative, anti-angiogenic, and antioxidant actions mediated through VDR expressed in endometrial and myometrial tissues.47–49 Research into underlying mechanisms reveals that vitamin D has the ability to inhibit key disease-related pathways common to these disorders, it modulates prostaglandin synthesis and degradation, thereby potentially reducing pain and uterine hypercontractility, it also promotes apoptotic and antifibrotic signaling, and suppresses pro-proliferative cascades such as the Wnt/B-catenin axis which is implicated in endometrial invasiveness and progesterone resistance.48,49 However, it is essential to distinguish between mechanistic evidence, observational associations, and proven clinical benefit. While observational epidemiology consistently reports lower circulating vitamin D levels in affected women linking deficiency to higher disease odds and, in some studies, greater lesion size or severity these associations do not establish causality. Reverse causation (disease pathology altering vitamin D metabolism), confounding by shared risk factors (obesity, physical inactivity, sunlight avoidance), and the potential for local tissue consumption of vitamin D in diseased tissue may all contribute to observed associations. Importantly, interventional evidence for disease modification remains preliminary and, in some cases, contradictory.47,48,50,51 In uterine fibroids specifically, cross sectional and case-control work report inverse associations between serum vitamin D and fibroid prevalence or burden, and one randomized clinical trial using weekly 50,000 IU for 12 weeks suggests that supplementation inhibited fibroid growth compared with a placebo group that experienced fibroid enlargement over the same period, although absolute shrinkage in the intervention arm did not reach statistical significance within that short timeframe.51,52 These human data align with robust preclinical evidence that vitamin D analogs reduced fibroid cell proliferation and fibrotic marker expression in vitro and in animal models, supporting a plausible antifibrotic effect that supports the need for longer, larger human trials.53,54
Adenomyomas, though less extensively studied, show a similar pattern. Retrospective cross-sectional analysis demonstrates markedly lower mean vitamin D in women with histopathological confirmed adenomyosis versus controls, and deeper or more infiltrative disease phenotypes are associated with even lower vitamin D levels and higher pain scores and CA-125, suggesting a severity gradient that aligns with a role for vitamin D in restraining local inflammation, neovascularization and fibrosis. 47 These findings are tempered by heterogeneous reports in the literature and potential confounders such as VDBP polymorphism and altered local tissue consumption of vitamin metabolites, which may decouple serum concentrations from tissue availability. Thus, adenomyosis data are compelling but demand prospective interventional validation. 47
Summary of studies on vitamin D and uterine pathologies.

N/A: Not applicable; IQR: interquartile range; AOR: Adjusted odds ratio; OR: odds ratio; TAC: total antioxidant capacity; hs-CRP: high sensitivity c-reactive protein; DIE: Deep infiltrating endometriosis; VAS: visual analog scale; Age, BMI, and baseline vitamin D values reported in the table correspond only to the uterine pathology case groups in each study. Vitamin D units: All values presented as ng/mL. For conversion to nmol/L, multiply by 2.496 Vitamin D and Pregnancy.
Vitamin D emerged as a multifaceted regulator of pregnancy, influencing immune tolerance, placental development, metabolic pathways, and neonatal nutrition. Yet the evidence for clinical benefit of supplementation and dose remains nonuniform. Early gestation transcriptome profiling from Vitamin D Antenatal Asthma Reduction Trial study cohort linked maternal vitamin D insufficiency to a distinct set of 146 differentially expressed genes that converge on innate immunity, Inerlukin-6, Interleukin -8, and Inerlukin-10 pathways, with VDR positioned as a hub within the spontaneous preterm birth network and metalloproteinase-8 upregulation suggesting deterministic bridge between deficiency and premature labor. 59 Observational data reinforces a protective trend for higher vitamin D concentrations, as cohorts reporting >40ng/mL showed up to 60% lower risk of preterm birth, 59 while other studies failed to demonstrate a clear association, highlighting methodological differences such as gestational timing of vitamin D assessment and preterm birth subtype definition. 59 randomized trials provide further insights, a triple blind trial administering 4000 IU vitamin D from 8-10 weeks’ gestation raised serum levels but did not improve fasting glucose, insulin, HOMA-IR, depressive scores or miscarriage rates, although it markedly reduced knee, ankle, and leg pain, confirming a robust effect on musculoskeletal comfort. 60 Parallel work in overweight/obese pregnant women achieved Vitamin D sufficiency with 1600 IU but failed to influence maternal or fetal lipid profiles, body fat distribution or birth size, suggesting that in a population already replete the metabolic impact of supplementation may be limited. 61
A major methodological limitation in pregnancy vitamin D research and a potential explanation for inconsistent trial results is the reliance on total serum 25(OH)D rather than measurement of bioavailable (free) vitamin D. Pregnancy induces profound physiological changes in vitamin D metabolism: circulating VDBP concentrations increase markedly due to estrogen-stimulated hepatic synthesis, typically rising by 40-50% by the third trimester. This elevation in VDBP increases total vitamin D carrying capacity, meaning that total 25(OH)D levels may appear adequate or even elevated while the free, biologically active fraction remains low
Conversely, early high dose vitamin D (60,000 IU monthly for six months) in primi-gravid women dramatically lowered preeclampsia risk, halved preterm delivery and low birthweight rates, and improved Apgar-5 scores, underscoring the potential of early intensive dosing to modify hypertensive and growth outcomes. 62 Yet, a threatened miscarriage cohort measuring vitamin D at presentation found no overall association with subsequent miscarriage, except for subgroup presenting <6 weeks where deficiency correlated with higher loss, indicating that the protective window may be earlier than the clinical encounter. 63 Retrospective analyses of missed abortion further identified vitamin D deficiency as an independent risk factor and revealed synergistic risk when combined with hyper-homocysteinemia or thyroid dysfunction, pointing to intersecting metabolic and endocrine pathways. 64 A separate retrospective gestational diabetes study reported a 55.7% deficiency prevalence and an inverse dose response where each 1 ng/ml increase in vitamin D decrease gestational diabetes mellitus odds by 8.7%, reinforcing the link between vitamin D status and glucose homeostasis, although within a minor sample. 65
Pregnancy causes a marked increase in circulating VDBP, which lowers the free bioavailable fraction of vitamin D even when total serum vitamin D levels appear adequate. This shift can mask true deficiency and affect reproductive outcomes such as infertility, PCOS, endometriosis, miscarriage, preeclampsia and fetal growth restriction. Moreover, genetic polymorphisms in the gene that encodes VDBP further modify an individual’s risk for these adverse events. Since total serum vitamin D alone does not reflect the physiologically active vitamin D pool during pregnancy, more accurate assays that measure free bioavailable vitamin D are needed to assess deficiency properly. 66
Nutritional patterns also shape vitamin D status. A cross-sectional study analysis identified a ferritin related dietary pattern rich in fish, shellfish, and organ meats that improved iron biomarkers but was inversely associated with serum vitamin D levels possibly due to predominance of vitamin D2 rich foods and limited UVB exposure, illustrating that dietary sources alone may not guarantee sufficient vitamin D. 67 By contrast, a preconception and pregnancy supplement containing 400IU vitamin D daily plus B-vitamins, increased human milk vitamin D levels during the first three months of lactation. On average, milk from supplemented mothers contained 141ng/L of vitamin D versus 118 ng/L in the control group, which corresponds to an adjusted mean difference of 1.20 which is equivalent to 20% increase. The effect was strongest in the New Zealand participants, where seasonal UVB deficits are pronounced, suggesting that early, sustained supplementation can enhance infant vitamin D exposure even if the absolute increase is modest. 68
Immune modulation emerges as a recurrent theme in pregnancy. In women with unexplained recurrent spontaneous abortion, vitamin D deficiency correlated with elevated cytokines (Interleukin-2, Tumor necrosis factor-alpha, Interferon-gamma), increased T cells, B cells and Natural killer (NK) cells and a shift toward a proinflammatory Th1/Th2 ratio. Vitamin D in turn restored a Th2 dominant immune profile, reduced NK cytotoxicity and lowers miscarriage recurrence, supporting its role as tolerogenic agent at the maternal-fetal interface. 69 Extending these finding, a broader study have further linked low vitamin D levels to elevated T cells, B cells, and Nk cells, alongside an increased T-helper cell (Th1/Th2) ratio, down regulation of Human leukocyte antigen (HLA-G1/G5), reduced vitamin D binding protein expression, altered Hepatocyte Nuclear Factor (HNF1a/B) transcription, and suppression of key glucose transporters (GLUT1, GLUT3, SGLT-1) and adenosine metabolizing enzymes (ENTPD1, NT5E). 70 Collectively, these molecular and cellular alterations impair placental immune tolerance, energy supply, and vascular function, supporting vitamin D’s central role in maintaining immune homeostasis and preventing miscarriage.69,70 Moreover, Maternal vitamin D level during pregnancy impacts fetal health, as it has been found that daughters of vitamin D deficient pregnancies show more prolonged mini-puberty with sustained elevations of urinary FSH and LH and higher salivary estradiol accompanied by larger ovaries and uterus, suggesting early axis programming by maternal vitamin D. 71 Finally, maternal obesity interacts with vitamin D status to affect fetal growth. In a large cohort, early gestation low vitamin D levels combined with a higher BMI, reduced first trimester crown-rump length and raised the risk of early fetal growth restriction by 13% to 35%, while higher vitamin D concentrations mitigated these adverse effects even among overweight women, suggesting a synergistic nutrient body composition axis. 72
Summary of studies on vitamin D and pregnancy.

IL: Interleukin; LDL: low density lipoprotein; HDL: high density lipoprotein; RR: relative risk; GDM: gestational diabetes mellitus; URSA: unexplained recurrent spontaneous abortion; OR: odds ratio; HLA: human leukocyte antigen; CTLA4: Cytotoxic T lymphocyte associated protein 4; VDBP: vitamin D binding protein; Age, BMI, and baseline vitamin D values reported in the table correspond only to the vitamin D deficient pregnant women case groups in each study. Vitamin D units: All values presented as ng/mL. For conversion to nmol/L, multiply by 2.496.
Vitamin D and in vitro fertilization (IVF)
Across studies in the field of assisted reproduction, vitamin D impinges at the intersection of ovarian biology, endometrial receptivity and systematic metabolism, yet clinical results diverge by dose, timing, and patient profile, which makes a careful synthesis essential for practice and research planning.9,74,75 At the ovarian level, vitamin D receptors in follicles and granulosa cells coordinate cell cycle progression, steroidogenesis, and antioxidant defenses, mechanisms that support oocyte competence and protect the follicular microenvironment under metabolic or inflammatory stress.9,75
Experimental and translational work shows that vitamin D promotes granulosa cell proliferation, modulates genes tied to meiosis and cell cycle, and reduces reactive oxygen species while improving in vitro maturation, all of which link nutrient status to the quality of gametes generated for IVF.9,75 In vivo evidence from women undergoing IVF indicates that oral supplementation raises follicular fluid vitamin D and reshapes granulosa cell transcriptomes toward anti-inflammatory and antioxidant pathways, with upregulation of the VDR and downregulation of Prostaglandin-Endoperoxide Synthase 2 (PTGS2) and Vascular Endothelial Growth Factor (VEGF), consistent with a dampened hyperstimulation response rather than shifts in follicular steroid hormones at retrieval. 74 On the uterine sides, vitamin D regulates endometrial genes important for receptivity an decidualization, and in mice a cyclic intrauterine protocol enhanced angiogenesis, increase uterine natural killer cell recruitment, stabilized early embryo attachment, and yielded more implantation sites with heavier fetuses when treatment spanned several cycles before mating.76,77 These mechanistic and preclinical layers frame how clinical trials should deliver vitamin D across the months of folliculogenesis and the peri-implantation window.77,78
Clinical data reflects this timing sensitivity. A prospective randomized pilot investigation adding 2000 IU cholecalciferol nightly from the early luteal phase to a background regimen raised serum levels and nearly doubled implantation rate, suggesting peri-implantation conditioning of the endometrium may be decisive even when endometrial thickness is unchanged. 79 A double blind randomized trial of a 6 week mediterranean-style dietary preconception intervention supplement that included vitamin D did shift the primary morpho-kinetic endpoint but accelerated the fourth cell cycle, short ended synchrony, and improved a day 3 embryo quality score, indicating that short periconceptional nutrition can influence embryo development even when early cleavage timing and clinical outcomes remain similar. 80
In contrast the large SUNDRO randomized trial, conducted in Italy on women with normal body weight who had preserved ovarian reserve and low vitamin D levels that used single 600,000IU oral bolus 2-12 weeks before stimulation found no improvement in clinical pregnancy or embryological surrogates, and subgroup analyses were null, and outcome that argues against one-off dosing close to treatment as a strategy to improve success in generally healthy women with preserved reserve. 78 In frozen embryo transfer cycles, a prospective cohort study of infertile women that supplemented all insufficient women and compared them to replete supplemented control observed no differences in ongoing pregnancy or related outcomes across serial measurements during endometrial preparation, which adds to the mixed picture and raises questions about whether serum cutoffs derived from bone health map accurately onto reproductive thresholds. 76
Population-based data is important when vitamin D supplementation is assessed in IVF. In patients with normal ovarian reserve undergoing a first IVF or Intracytoplasmic Sperm Injection (ICSI), a large retrospective analysis found no significant differences across vitamin D strata in mature oocytes, fertilization, available embryos, implantation, or biochemical pregnancy, although clinical pregnancy was higher in the non-deficient group with some protocols, underlining how design, protocol choice and sample size shape signals. 81 By age, an analysis reported that deficiency was linked to worse clinical pregnancy in advanced age, potentially mediated by reduced HOXA10 expression that compromises receptivity, whereas younger women showed no clear decrement, highlighting age and endometrial biology as modifiers of clinical relevance. HOXA10 is a crucial gene that regulates endometrial receptivity for embryo implantation, and its reduced expression is linked to poor outcomes. In women aged >35 years, vitamin D deficiency was significantly correlated with poorer clinical pregnancy outcomes and decreased endometrial HOXA10 levels, suggesting the deficiency is more detrimental to embryo implantation in this age group. 82
In PCOS, A systematic review synthesized 59 studies and found that higher baseline vitamin D or supplementation tended to associate with better embryo quality, pregnancy and cumulative live birth, along with improvements in insulin resistance and androgen profile, while also stressing heterogeneity, moderate risk of bias and the need for standardized dosing and timing. 75 complementing these data, a controlled study reported that preprocedural supplementation with vitamin D plus myo-inositol, folic acid, and melatonin improved embryo quality regardless of stating status, increased progesterone among deficient women, and showed trends toward higher implantation and lower miscarriage that did not reach significance, which suggests embryo grading may be a more sensitive endpoint than near term pregnancy when exposure is short and multifactorial. 83
A critical SWOT style narrative focused on women over 40 collated meta analytic signals linking sufficiency to higher implantation, biochemical and live birth rates, while emphasizing inconsistent trials, unclear optimal dosing and frequency, and the absence of age specific randomized evidence that would justify routine supplementation as an add on in this demographic. 84 Finally, a prospective study restricted to frozen embryo transfers reiterated the controversy by summarizing discordant RCTs and meta-analyses and calling for larger standardized trials that compare replete, insufficient supplemented and insufficient supplemented groups across the cycle, a design that could resolve whether vitamin D acts mainly on endometrium or oocyte in different settings. 76
Summary of studies on vitamin D and IVF.
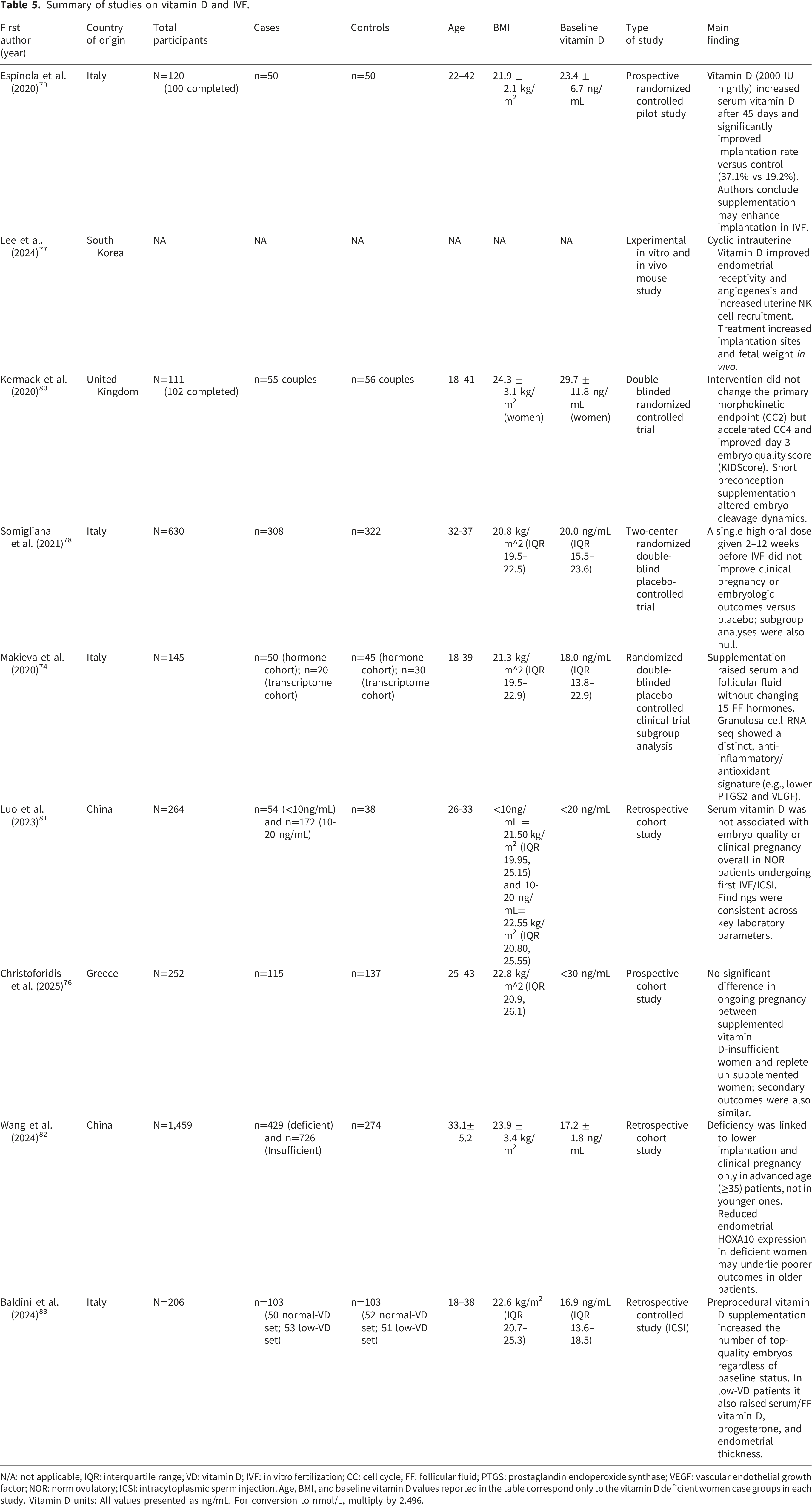
N/A: not applicable; IQR: interquartile range; VD: vitamin D; IVF: in vitro fertilization; CC: cell cycle; FF: follicular fluid; PTGS: prostaglandin endoperoxide synthase; VEGF: vascular endothelial growth factor; NOR: norm ovulatory; ICSI: intracytoplasmic sperm injection. Age, BMI, and baseline vitamin D values reported in the table correspond only to the vitamin D deficient women case groups in each study. Vitamin D units: All values presented as ng/mL. For conversion to nmol/L, multiply by 2.496.
Limitations and implications for future research
Across literature, several consistent weaknesses limit firm conclusions and guide what should come next. Many studies are small, single center, cross-sectional, or retrospective, with inadequate control of key confounders like diet, sun exposure, season, and ethnicity, which makes causal inference difficult and restricts generalizability. Measurement issues are common as well, investigators often rely on total serum vitamin D without accounting for VDBP or free vitamin D levels, and assay methods and cut points for deficiency vary, all of which can bias exposure classification and inflate heterogeneity across results. Intervention trials frequently enroll women who are already vitamin D replete, use disparate doses or bolus schedules, start too late relative to critical reproductive windows, and prioritize surrogate endpoints over live birth or long-term child outcomes, which together may obscure meaningful effects. Although vitamin D toxicity is a recognized risk, particularly given the widespread availability of supplements, evidence on adverse effects specifically related to female reproductive health remains limited. Excessive intake, especially above the institute of medicine upper limit of 4,000 IU/day or through large bolus doses like 500,000 IU annually, can cause hypercalcemia, leading to symptoms such as nausea, vomiting, and weakness, and has paradoxically been associated with increased risk of falls and fractures. 85 Nonetheless, most trials report mild or no adverse events, underscoring a gap in systematically assessing toxicity in relation to reproductive outcomes. Condition specific trials add further constraints, endometriosis and pain studies are underpowered, often show strong placebo responses, and rarely standardize does or duration. IVF trials struggle to isolate vitamin D from co interventions and sometimes measure only clinical pregnancy rather than live birth. PCOS trials vary in baseline status, dosing, and outcome selection, with many focusing on metabolic surrogates rather than ovulation, conception or live birth. Even well-designed randomized studies face pragmatic limits, such as incomplete blinding, high attrition in challenging settings, or inability to capture environmental exposures and genetics that shape response to supplementation. The field needs large, multicenter randomized trials that target deficient or high-risk women, begin preconception or early gestation, use standardized daily or weekly dosing, and track patient centered outcomes such as live birth, miscarriage, preeclampsia, and neonatal health, while rigorously measuring free vitamin D levels alongside total and VDBP with harmonized assays. Trials should be designed to minimize residual confounding, include diverse populations, and integrate genetics, including VDR and related variants, to enable precision supplementation and clarify gene environment interactions, paralleled mechanistic studies using validated multi omics and functional assays in reproductive tissues should probe immune regulation, angiogenesis, oxidative stress, and endometrial signaling to tie molecular effects to clinical benefit. Finally, specialty areas require tailored designs, IVF studies should compare timing strategies and dosing without bolus regimens and adopt live births as the primary endpoint. Endometriosis and dysmenorrhea trials must be adequately powered to overcome placebo effects and standardize co therapies, and PCOS trials should stratify by baseline vitamin D status and phenotype to link metabolic improvements to real fertility gains. Only with standardized exposure assessment, careful timing, and robust, diverse, mechanism informed trials will the field resolve current ambiguity and define when, for whom, and how vitamin D meaningfully improves female reproductive outcomes.
Conclusion
In summary, the current evidence linking vitamin D to female reproductive health is promising but uneven, with small heterogeneous studies and variable measurements limiting clear guidance for practice. A stronger path forward will pair well-designed, multicenter trials that begin with standardized dosing and patient centered outcomes, alongside careful assessment of vitamin D status and key confounders. Integrating genetics, diverse populations, and mechanistic work in reproductive tissues can help explain who benefits most and why.
When examining the evidence across different reproductive conditions, notable variations emerge in the strength of support for supplementation. The most robust findings appear in women with PCOS, where multiple RCTs demonstrate that vitamin D repletion improves insulin resistance, reduces hyperandrogenism, and may enhance ovulatory function. Positive signals also arise in endometriosis, where trials show vitamin D can reduce pelvic pain and inflammatory markers, though data remain preliminary. In pregnancy, strong observational links between deficiency and adverse outcomes like preeclampsia have not consistently translated into clear preventive benefits from supplementation in trials, suggesting the need for better timed interventions.
The weakest and most contested evidence surround IVF, where despite strong epidemiological associations, the largest RCT to date (SUNDRO) found no benefit from single high dose regimen on clinical pregnancy rates. This discrepancy highlights that observational associations may reflect confounding rather than causality. Evidence for preventing miscarriage or improving uterine fibroid outcomes also remain suggestive but unconfirmed, with insufficient trial data to guide practice.
Footnotes
Ethical considerations
Not applicable as the study was based exclusively on published literature.
Author contributions
AA: Conceptualization; Data curation; Methodology; Writing original draft; Writing review and editing. DP: Investigation; Supervision; Methodology; Validation; Writing review and editing. FA: Investigation; Validation; Writing review and editing. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Artificial intelligence policy
The authors used ChatGPT-5.3 to assist with language editing and improving clarity of sections of this manuscript. The authors reviewed, verified, and take full responsibility for all content.