
Abstract
Background
Brazil is globally known for its high rate of cesarean section despite endorsing the WHO’s current recommendation of 15%.
Objectives
Determine if socioeconomic status correlated with the rate of cesarean section (CS) at a mixed private and public hospital in the west-central region of Brazil. Describe the maternal and neonatal outcomes by mode of delivery (MOD) in the same population.
Design
Cohort study
Methods
Data from all delivering patients at São Lucas Hospital were collected during an 18-month period and analyzed. Demographics, baseline maternal health status, pregnancy and delivery information, maternal outcomes, and neonatal outcomes were entered into a secure database.
Results
Data from 2,103 women who delivered at São Lucas Hospital were collected. 75% of women delivered via CS. 53.7% were elective in nature. Women who had ≥ 8 prenatal visits (OR1.36, 95% CI 1.06- 1.72, p= 0.013) and had insurance type plan (OR 1.88, 95% CI 1.43-2.50, p<0.001) were more likely to undergo CS. Women who worked in the commercial sector were less likely to undergo CS (OR 0.53, 95% CI 0.33-0.90, p= 0.015). Women who were older (OR 1.05, 95% CI 1.03-1.07, p <0.001) and had a high BMI (OR 1.11, 95% CI 1.08-1.13, p<0.001) were more likely to undergo CS. When examining women who underwent CS those women who were white (OR 1.40, 95% CI 1.11-1.78, p=0.005), were older (OR 1.04, 95% CI 1.03-1.06, p<0.001), worked in agriculture (OR 2.06, 95% CI 1.22-3.57, p=0.008), and had insurance type private (OR 1.79, 95% CI 1.22-2.65, p=0.003) or plan (OR 2.47, 95% CI 1.92-3.19, p<0.001) were more likely to have an elective CS. MOD was not associated with maternal or neonatal outcomes.
Conclusion
CS rates at São Lucas Hospital are high. Socioeconomic factors and maternal demographics were predictive of MOD. Maternal and neonatal outcomes in term deliveries did not differ by MOD.
Plain language summary
At São Lucas Hospital, cesarean section rates are high. Patient socioeconomic factors and characteristics were associated with how babies were delivered (vaginal birth versus cesarean section). However, among full-term births, maternal and newborn health outcomes were similar regardless of the method of delivery.
Introduction
Cesarean sections (CS) are an effective measure to decrease maternal and neonatal morbidity and mortality. The World Health Organization (WHO) describes the ideal rate for CS in clinical practice as 15%; however, this rate has increased in recent years in both developed and developing countries. 1 In 2015, CS made up 21.1% of live births worldwide—almost double the reported number in 2000, with the highest rates reported in Latin American countries (44.3% of all births). 2 Second only to the Dominican Republic, Brazil is globally known for its high rate of CS at 56.3% of all births in 2019, despite endorsing the WHO’s current recommendation of 15% as the ideal rate of CS. 3
While CS is considered safe, it is an abdominal surgery which poses both short- and long-term risks to maternal and neonatal health. These risks are often more prevalent in low-to-middle income countries (LMIC). Short term adverse events for the mother include infection, hemorrhage, visceral injury, venous thromboembolism, and maternal death. 4 Long term adverse events for the mother include chronic pain, dysmenorrhea, abnormal uterine bleeding, sexual dysfunction, subfertility, childhood asthma, atopy, obesity, irritable bowel disease, and increased healthcare costs in neonates. 4 Delivery by CS also has implications for subsequent pregnancies including diseases of the placenta (placenta previa, placenta accreta, placental abruption), uterine rupture, spontaneous abortion, ectopic pregnancy, stillbirth, postpartum and antepartum hemorrhage, preterm labor, and intrauterine growth restriction. 4 Adverse maternal outcomes of elective CS include higher frequencies of maternal mortality, hospitalization in intensive care unit (ICU), blood transfusion, hysterectomy, antibiotic therapy, and longer hospital stays. 5 Neonates may be more likely to be admitted to the neonatal ICU (NICU) with delivery by elective CS. 6
Comparatively, vaginal deliveries (VD) involve their own risks to maternal morbidity including significantly greater odds of developing pelvic floor disorders (PFD) years post-delivery. 7 Work by Zandvakili et al. demonstrates that women who undergo VD with episiotomy may suffer from increased risk of postpartum hemorrhage, perineal laceration, cervical rupture, and ICU hospitalization when compared to women who underwent CS. 8 Additionally, planned CS among singleton pregnancies are associated with less frequent low neonatal umbilical artery pH levels, need for tube feeding, birth trauma, chorioamnionitis, urinary incontinence, and perineal pain. 9
Previous Brazilian studies have identified several factors associated with the high rate of CS: maternal education, maternal desire, and the Brazilian healthcare system.10,11 Many studies highlight the impact of socioeconomic status on the rate of CS. Behague et al. found that women from families with higher incomes and higher levels of education had CS more often. 10 Additionally, more antenatal care, usually among women of higher socioeconomic status, has been associated with having a 47% higher chance of CS. 12 Regional and hospital-type (private versus public hospitals) disparities confirm the impact of socioeconomic status on the rate of CS. Despite the association of high rates of CS with some worse maternal and neonatal outcomes, women in the Southeast, South, and Central West regions of Brazil (well-developed areas with better socioeconomic conditions and more use of private hospitals) had a 45%, 65%, and 73% higher chance of CS compared with other less wealthy regions of Brazil, respectively. 13 80% of private hospital deliveries occur via CS. 11 In short, it is now a Brazilian cultural norm that women will give birth by CS.
In this study, we aimed to describe obstetric practices at one hospital in rural Brazil. Specifically, we set out to determine if socioeconomic status, measured using proxy indicators of race, maternal occupation, insurance, neighborhood of residence and number of prenatal care visits, correlated with the rate of CS at a mixed private and public hospital in the west-central region of Brazil (São Lucas Hospital in Lucas do Rio Verde, Brazil). The secondary aim of this study was to describe the maternal and neonatal outcomes by mode of delivery (MOD) [vaginal, assisted vaginal-vacuum or forceps, and CS] in the same population. To our knowledge, no such work is published in this practice setting. Our work adds to the growing body of literature on the topic of factors impacting, and effects of, mode of delivery.
Methods
This is a prospective cohort study utilizing data from quality improvement programming. The STROBE cohort checklist was followed for manuscript preparation. 14 Lucas do Rio Verde is a city of approximately 88,000 people in Matto Grosso state in west-central Brazil. Several large agribusinesses operations have been established and contributed to rapid growth of the community over the last 20 years. The hospital included in this study, São Lucas Hospital, is the only hospital in the area. It was built when the area’s population was only 30,000 and has grown to provide services to the enlarging population. The hospital serves patients with both private and government issued insurance.
As part of quality improvement programming, data from all delivering patients at São Lucas Hospital were collected from June 10, 2023 to December 31, 2024. Inclusion criteria were all delivering patients who presented to São Lucas Hospital between the dates listed. No delivering patients were excluded to our knowledge. The data were entered into a secure REDCap (Research Electronic Data Capture) database prior to discharge from the delivery hospitalization. REDCap is a secure web platform for building and managing online databases and surveys available to academic institutions who are partnered——see Acknowledgements. Data included demographics, baseline maternal health, pregnancy and delivery information, maternal outcomes, and neonatal outcomes. Data were deidentified on entry. Consent to participate and data collection were Institutional Review Board (IRB) exempt as determined by the University of Iowa IRB given the intention for quality improvement programming (letter of exemption provided).
When examining the impact of socioeconomic status on CS rate, the entire delivery cohort was included. Markers of socioeconomic status included race, occupation, insurance, neighborhood, and number of prenatal care visits. When examining maternal and neonatal outcomes by MOD, only deliveries occurring at term (37 weeks 0 days and after) were included. Maternal occupation was entered into the REDCap database in a free text field. ChatGPT version 4.0 (query performed on January 8, 2025) was used to categorize maternal occupations into one of six mutually exclusive categories: agriculture, business, commercial, healthcare, other, unknown. The entire list of free text occupations was pasted into ChatGPT and the chatbot was instructed to “group these occupations into 5 categories with another category for unknown or vague terms.” Indications for CS included: elective, medically indicated, non-reassuring fetal status, failed induction, malpresentation, repeat CS, and desire for sterilization. The delivering physician was responsible for determining the indication for CS based on their medical knowledge rather than specific criteria. Indication for CS was recorded in the medical record at time of delivery. The categories listed under indication for CS were not mutually exclusive.
Statistical analysis
Continuous variables were reported using medians and inter-quartile ranges, while categorical variables were reported using counts and percentages. The number of missing observations for each variable was reported as well. To assess for a relationship between socioeconomic status and CS rate, univariate logistic regression models were fit in which several measures - maternal race, occupation, insurance, neighborhood, and number of pre-natal visits – served as predictors with the outcome of whether a delivery was performed via CS. Additionally, univariate logistic regression models were fit with these same predictor variables to evaluate whether socioeconomic factors influence the likelihood of CS being elective. Given the distribution of neighborhood of residence and inability to group this in a meaningful way this predictor was not included in the final models. Univariable models were chosen to preserve power modeling the multi-category explanatory variables in our study.
To assess for a relationship between MOD and maternal outcomes (ICU admission, prolonged postpartum stay defined as more than 24 hours after a spontaneous VD or CS, endometritis, pyelonephritis during delivery admission, sepsis during delivery admission, postpartum hemorrhage, thromboembolic disease, blood transfusion, maternal death) contingency tables for each outcome with MOD (vaginal, assisted vaginal -vacuum or forceps, CS) serving as the predictor were made. The neonatal outcomes (Apgar score less than 7 at first minute of life, Apgar score less than 5 at 5 minutes of life, need for respiratory support, infant disposition (with mom, in neonatal nursery, in NICU), sepsis, hypoglycemia, malformations, diagnosis of hypoxic ischemic encephalopathy, and neonatal death) were evaluated and presented in the same manner as the maternal adverse outcomes. P-values less than 0.05 were considered statistically significant with corrections for multiple comparison not employed due the exploratory nature of the analysis. R version 4.4.1 was used for all analyses.
Results
Demographics.

IQR: interquartile range.
CS: cesarean section.
HELLP: hemolysis, elevated liver enzymes, and low platelets.
UTI: urinary tract infection.
75% of deliveries occurred via CS, 20% via VD, and 4.6% via assisted VD in the population. 847 of 1,578 (53.7%) CS were elective. CS were documented as medically indicated in 27.9% of cases with the most common medical indication being maternal health conditions (10.8%). Additional indications for CS were non-reassuring fetal status (27.9%), failed induction (1.2%), malpresentation (1.8%), and desire for sterilization (3.3%). Indications for CS were not mutually exclusive (Table 1).
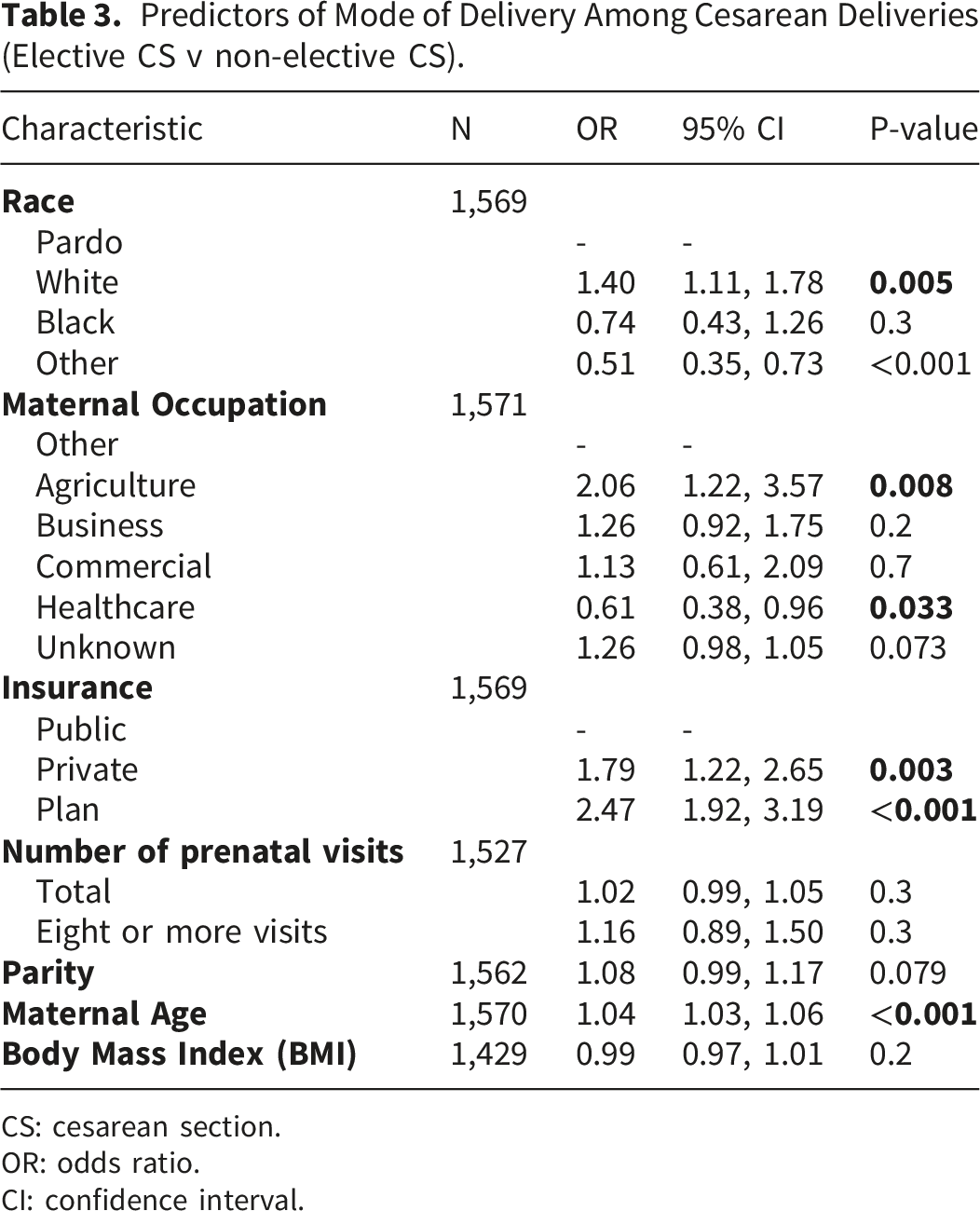
When examining if socioeconomic factors are associated with CS as compared to VD among our entire cohort, women who had ≥ 8 prenatal visits (OR1.36, 95% CI 1.06- 1.72, p= 0.013) and had insurance type plan, an employer-sponsored private coverage, (OR 1.88, 95% CI 1.43-2.50, p<0.001) were more likely to undergo CS (Figure 1). Women who worked in the commercial sector were less likely to undergo CS compared to VD (OR 0.53, 95% CI 0.33-0.90, p= 0.015) (Figure 2). Women who were older (OR 1.05, 95% CI 1.03-1.07, p <0.001) and had a high BMI (OR 1.11, 95% CI 1.08-1.13, p<0.001) were also more likely to undergo CS compared to VD (Table 2). When examining socioeconomic factors among those who underwent CS, women who were white (OR 1.40, 95% CI 1.11-1.78, p=0.005), worked in agriculture (OR 2.06, 95% CI 1.22-3.57, p=0.008), and had insurance type private (OR 1.79, 95% CI 1.22-2.65, p=0.003) or plan (OR 2.47, 95% CI 1.92-3.19, p<0.001) were more likely to have an elective CS. Women whose race was listed as other (OR 0.51, 95% CI 0.34-0.71, p<0.001) and worked in healthcare (OR 0.61, 95% CI 0.38-0.96, p=0.033) were less likely to undergo elective CS. Women who were older (OR 1.04, 95% CI 1.03-1.06, p<0.001) were more likely to undergo elective CS (Table 3). Mode of Delivery by Insurance Type. Mode of Delivery by Maternal Occupation. Socioeconomic Factors and Demographics Predicting Mode of Delivery (CS v VD). CS: cesarean section. VD: vaginal delivery. OR: odds ratio. CI: confidence interval. Predictors of Mode of Delivery Among Cesarean Deliveries (Elective CS v non-elective CS). CS: cesarean section. OR: odds ratio. CI: confidence interval.


Maternal Outcomes by Mode of Delivery for GA greater than or equal to 37 weeks using Fisher’s Exact Test.

GA: gestational age.
ICU: intensive care unit.
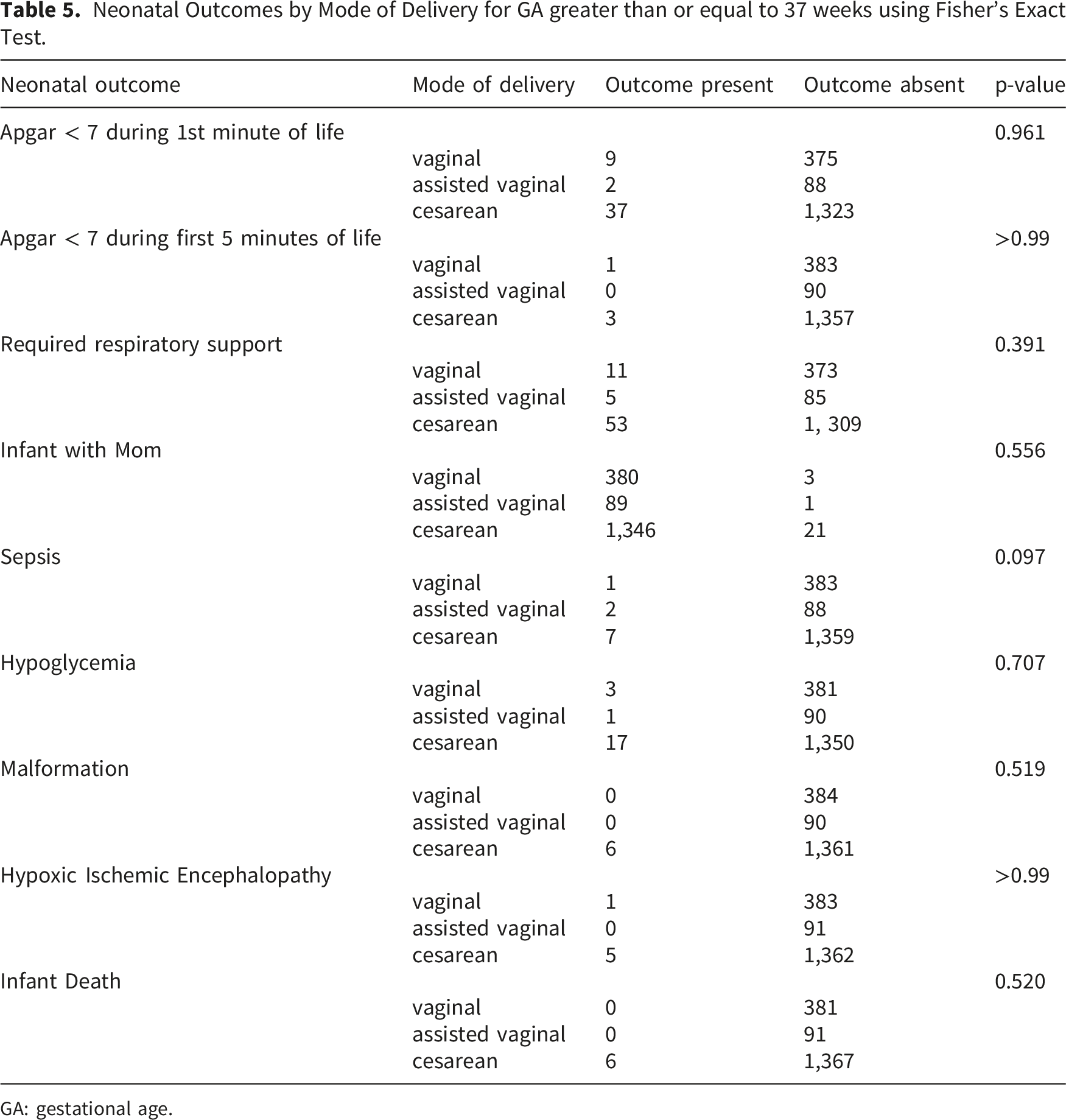
Neonatal Outcomes by Mode of Delivery for GA greater than or equal to 37 weeks using Fisher’s Exact Test.
GA: gestational age.
Discussion
Cesarean section rates in Brazil
The CS rate of 75% in this study aligns with findings from previous research, highlighting a national trend of high CS utilization in Brazil. 56% percent of all live births in Brazil occurred via CS in 2019, and had increased from 38% in 2000 with a wide variation based on regional location and type of hospital. 12 Allowing cesarean delivery upon maternal request is law in Brazil, which allows any patient access to cesarean delivery when she chooses. 15 In our study, greater than 40% of CS indications were listed as elective. These CS rates are well above the WHO’s recommendation of 15% of total live births, but consistent with current practices in Brazil.
The etiology of Brazil’s high CS rate is complex. Rapid expansion of access to healthcare in Brazil following the introduction of universal healthcare in 1990 gave way to increased medicalization of birth with increasing CS, episiotomies, and ultrasounds. CS are significantly easier for physicians to schedule and avoid the uncertainties associated with labor and vaginal deliveries. There are also perceptions that scheduled CS may avoid liability associated with poor outcomes from spontaneous labor and delivery complications. 16 In one Brazilian study, surgeons with the perception of higher risk of litigation against obstetricians had a 6-fold statistically significant increase in CS rate compared to those who did not perceive higher risk of litigation, suggesting an element of defensive medicine contributing to rising CS rates in Brazil. 17 57% of CS in Brazil occur in primiparous women and almost half of all CS were scheduled which supports the idea of maternal preference for CS over VD11,13 40.4% of CS performed in our cohort were in primiparous women. When looking at primiparous women in this study 75.8% delivered via CS. This might be explained by the influence of prenatal care providers and women’s desire to avoid pain during delivery or risk of future PFD. In a recent survey, nearly half of ∼1250 surveyed physicians reported the main reasons given for CS on request were fear of pain, fear of vaginal birth, previously poor vaginal birth experience, and convenience for women. 18
In another Brazilian study, women who had their prenatal care in the private sector had a higher rate of CS even when their delivery care was provided by the public sector. Contrarily, a disconnect between information provided during prenatal care and delivery care can also contribute towards the decision of delivery providers to choose a CS. 16 As culture in Brazil has shifted to most women delivering by CS, the medical community has moved to support womens’ right to request a CS for any reason, including personal preference. A Federal Council of Medicine (CFM) resolution allowing elective CS from 39 weeks with informed consent was enacted in 2016. 19 Additionally, several Brazilian states, including Matto Grosso in 2025, have enacted statutory laws explicitly guaranteeing this right within the public health system. 20 A recent study from São Paulo State showed a statistically significant increase in CS deliveries following the enaction of the law. 21
Impact of socioeconomic factors
In this study, maternal occupation in either commercial or unknown fields was predictive of undergoing VD over CS. The socioeconomic factors and maternal demographics associated with increased odds of CS over VD included insurance plan, 8 or more prenatal visits, maternal age, and BMI. When looking just at individuals who underwent CS white race, maternal occupation in agriculture, both private and plan insurance (a type of private insurance that is employer-sponsored with contracts to specific healthcare facilities), as well as maternal age were predictive of elective CS over non-elective CS. Women working in healthcare and who did not identify as Pardo, White, or Black were less likely to undergo elective CS. The data in this study align with previous research which has shown a strong correlation between CS rate and socioeconomic factors. Prior work has identified well-educated, Caucasian, partnered, women as more likely to receive CS when compared to other demographics. In this other study, 55% percent of women from families earning more than $1000 per month underwent cesarean section in Pelotas, Brazil. 10
In regard to race specifically, prior publications have reported women from Indigenous, Black, and Brown (what our study referred to as Pardo) ethnic backgrounds in Brazil are less likely to undergo CS and face a higher risk of mortality from direct obstetric causes. 22 This was confirmed in a study from 2025 in which the CS rate among Pardo women was 51.11%, 49.69% in Black women, and 21.23% in Indigenous women compared with 66.66% in White women. White women were most likely to receive CS compared with all other ethnic backgrounds regardless of Robson classification, a standardized framework for analyzing obstetric populations and CS rates. 23 According to one study in Rio de Janeiro, Black mothers have to visit more hospitals before being admitted for delivery care and are less satisfied with the quality of care they receive when compared to White mothers. 11 In another Brazilian study, frequency of CS was 64% and 44% lower in women with less than 8 years of education and Brown women, respectively. 12 Women in our study had a median of 10 prenatal visits, which may partially explain the high rate of CS. Prior literature from Brazil suggests that women who had more than 6 prenatal visits, which often includes women of higher socioeconomic status and more access to care, had an increase in rate of CS by 47%. 12 Our findings further demonstrate the complex relationship between societal, medical, and individual influences on MOD in Brazil.
Where women live and deliver impacts their rate of CS. Compared to the national CS rate of 55.1% in primiparous women, the rate of CS in the Central-West region, where this study takes place, has previously been described as 62.3%.13,24 In private hospitals in the Central-West region, CS rates increase to more than 80% at all gestational ages. 13 A publication from Brazil’s Northern region, one of the country’s poorest areas, has the lowest CS rate (in both public and private hospitals) and a higher likelihood of death from direct obstetric causes.13,22 Rates of CS are consistently higher in private hospitals across all Brazilian regions though these hospitals have had a slight reduction in CS rate over recent years. 25 The rate of CS (75%) in our study hospital with a mix of public and private patients is thus similar to facilities in this region, whereas the overall rate of CS in public hospitals nationally in Brazil is 62.3% and more than 80% in private hospitals. 13 Data from 2014-2020 showed an increase in CS rate in public hospitals among all Robson classification groups including those groups characterized by conditions favorable to vaginal birth further highlighting the impact of hospital setting on CS rate. 25
Maternal and neonatal outcomes
In our study, there were no differences in maternal and neonatal outcomes by MOD, which is different from other studies. This difference may be attributable to a generally healthy population at baseline, short length of follow-up, and low number of overall vaginal deliveries. Although 15% of the patients in our cohort developed gestational diabetes, only 6% of the patients had any type of hypertension, and very few patients had pre-existing health problems. While many studies around the world have shown increased complication rates for patients delivering by CS, the cohort in this study did not have worse outcomes. The rate of maternal mortality remains moderately high in Brazil as a whole, with the recent Maternal Mortality Rate of around 68/100,000 live births. 26 There were no instances of maternal mortality in our cohort. Near miss events defined as events in which a pregnant woman comes close to death but does not die affect about 13.5% all deliveries in Brazil, according to a recent study of the Brazilian public health system. 27 However, in our study, we saw few near misses with only 8 postpartum hemorrhages in the entire cohort, 3 blood clots, 1 need for blood transfusion, and no cases of sepsis. In addition to reflecting the high quality of obstetric care at São Lucas Hospital, this is also likely related to the healthy population in our cohort; patients with higher risk pregnancies are often referred to larger cities with more resources and maternal fetal medicine specialists for their care when possible.
Among the term deliveries analyzed there were six infant deaths reported at delivery via CS (1 non-reassuring fetal well-being, 2 elective, 2 medically indicated, and 1 no recorded indication). This finding was not statistically significant when examining MOD. While adverse outcomes associated with CS in other published work were present in our cohort, they were not shown to have a significant association with MOD. These include low Apgar scores, need for respiratory support, NICU admission, hypoglycemia, sepsis, malformations, and hypoxic-ischemic encephalopathy.4,13,28
Strengths
Strengths of this study are that it includes all deliveries at the São Lucas Hospital during the study period and the data were prospectively collected in a standard format. The findings in this study do align with the high rate of CS seen across Brazil and more specifically the Central-West region. These findings also highlight the impact of socioeconomic factors on MOD.
Limitations
Limitations of this study include use of proxy measures for socioeconomic status rather than markers like level of education or household income. These proxy indicators may not fully capture the complexity of socioeconomic conditions and could limit the precision of the findings. It is possible we were unable to capture socioeconomic status accurately by the measures used (race, occupation, neighborhood, insurance, and number of prenatal care visits). Additional limitations include a short length of follow-up (discharge from delivery encounter) which may mask the magnitude of poor maternal and neonatal outcomes associated with MOD. As the data in this study were initially collected for use in a quality improvement project, another limitation is that this is a non-powered study.
Conclusion
There is a high cesarean delivery rate at São Lucas Hospital in Lucas do Rio Verde in Central-West Brazil, similar to other Brazilian hospitals. In this study, socioeconomic factors and maternal demographics (maternal occupation, insurance, number of prenatal visits, race, age, and BMI) were predictive of MOD. Maternal and neonatal outcomes in term deliveries did not differ by MOD in this cohort and there were few adverse outcomes.
Footnotes
Acknowledgments
Gabriela Refatti, Juliana de Lima Cunha, Rodrigo Amorim Dillemburg, and the clinicians at São Lucas Hospital who assisted with data collection. REDCap is a secure web platform for building and managing online databases and surveys. REDCap use in this publication was supported by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number UM1TR004403. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical considerations
The University of Iowa Institutional Review Board (IRB) determined this project (202507342) does not meet the regulatory definition of human subjects research and therefore does not require IRB approval or consent to participate. Letter of exemption from July 18, 2025 is included.
Author contributions
Ramya Vemulapalli: Manuscript writing/editing Roni Arienti: Protocol/project development, Data collection, Data management, Manuscript editing Linder Wendt: Data analysis, Manuscript writing/ editing Brooks Jackson: Protocol/project development, Manuscript editing Mary B Rysavy: Protocol/project development, Manuscript editing Kimberly A Kenne: Protocol/project development, Data management, Data analysis, Manuscript writing/editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fueling Sustainability Foundation Lucas Do Rio Verde, Brazil, University of Iowa Clinical and Translational Science Award granted with funds from the NIH [UMITR004403], the Mark Gilbert and Karen Simmonds Gift Fund, and the University of Iowa Global Research Partnership Award.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified data may be available on request to corresponding author.