
Abstract
Background:
Mothers experience a wide range of maternal health problems after childbirth, which in turn, affect their well-being and ability to care for their newborn. These problems may be influenced by factors such as mode of delivery or socio-economic status.
Objective:
This study aims to investigate the prevalence of common maternal health problems and their correlates in a public primary healthcare institution in Singapore.
Design:
This was a cross-sectional study, based on a self-administered questionnaire.
Methods:
A total of 373 mothers (mean age 31.9 years) who accompanied their infants for their 4- to 8-week development assessments at a public primary care clinic in Singapore completed a self-administered questionnaire from June 2021 to December 2021. The questionnaire assessed demographic factors, mode of delivery, number of children, number of individuals providing significant help, and the frequency of common physical and mental maternal health problems using a 5-point Likert-type scale.
Results:
The five most common maternal health problems were fatigue (77.7%), lower back pain (59.3%), Caesarean wound pain (54.3%), upper back pain (53.0%) and vaginal pain (41.2%). The prevalence of depression and anxiety was 22.0% and 11.3%, respectively. With respect to the symptoms’ correlates, pain on passing urine was more frequent after assisted vaginal deliveries than all other forms of deliveries (all pairwise p < 0.01), and pain on passing motion was more frequent in vaginal deliveries than in Caesarean deliveries (all pairwise p < 0.05). Mothers having a larger number of children more frequently experienced headaches (β = 0.17, SE = 0.05, p = 0.002) and less frequently experienced breastfeeding difficulties (β = –0.28, SE = 0.08, p < 0.001).
Conclusion:
Mothers experienced a high prevalence of maternal health problems in multiple domains during the first 8 weeks after childbirth. Mode of delivery and number of children were associated with increased prevalence of certain problems. Mothers’ physical and mental well-being should be investigated early after delivery and addressed with adequate treatments and resources.
Introduction
Childbirth marks a period of significant changes 1 for women during which they experience physical and mental health problems as they transition into a motherhood role. A number of studies have highlighted the prevalence of these health problems during the post-partum period. At 4- to 8-week post-partum, nearly 50% of women reported back pain in an Australian study, 2 while 63.8% of women in a Swedish study reported experiencing tiredness. 3 In addition, about 62.5% of women in a Canadian study experienced between two and five physical symptoms 4 while 43.6%–44.2% of women reported back pain at 6 weeks post-partum in a Spanish study. 5 These health problems have also been reported to last for months after delivery. Webb et al. 6 reported that 69% of women surveyed in Philadelphia, USA, still had at least one physical health problem 9–12 months after childbirth. Moreover, the presence of post-partum maternal health problems has resulted in limiting women’s functions such as looking after children, and are associated with worsening maternal emotional health.6 –8 Untreated and persistent health problems have long-lasting consequences: longitudinal studies9,10 have found that persistent or untreated maternal health conditions in women have been associated with problems with their children’s health and behaviour. Hence, the early detection and treatment of post-partum health problems plays a key role in the well-being and development of mothers and their children. 11
Factors that increase the likelihood of post-partum maternal health problems have also been investigated. Morgan and Eastwood 12 and Haas et al. 13 found that difficult financial circumstances were risk factors for poor maternal health among post-partum women. Conversely, good social support has been found to be positively associated with better post-partum maternal health outcomes.14,15 Henderson et al. 16 found that substantial fatigue was higher among post-partum women of greater age and parity, and lower in women with practical help and support from partners.
Furthermore, the mode of birth delivery has been associated with many maternal health problems. As compared with unassisted vaginal deliveries, assisted vaginal deliveries had a higher risk of pelvic floor dysfunction problems. 17 Rowlands and Redshaw 18 noted an increased risk of bodily changes such as backache and stress incontinence in assisted vaginal births while Ansara et al. 4 linked this mode of delivery to a statistically significant increase in the prevalence of haemorrhoids. Moreover, vaginal deliveries in general increased the risk of urinary and faecal incontinence19,20 as compared with Caesarean deliveries. On the contrary, Caesarean sections have been associated with breastfeeding difficulties, including earlier cessation.21,22
In the past, Singapore has been successful in improving their infant and maternal mortality rates: Singapore’s infant mortality rate has decreased from 27.6 to 1.7 cases per 1000 live births from 1965 to 2021, 23 while the maternal mortality rate has likewise decreased from 39.5 to 2.6 cases per 100,000 live births 24 in the same time period. In the past few years, the focus has evolved beyond mortality rates to improving maternal physical and mental well-being. 25 A national task force has been set up in 2021 to focus on Child and Maternal Health and Well-being (CAMH) Strategy and Action Plan, 26 where resources and capabilities are developed to support mothers and their health. In line with this strategy, there are ongoing large-scale local studies investigating the relationship between maternal health before and during pregnancy (such as nutrition, mood, metabolic disorders)27,28 on the subsequent health and development of mother and children. With regard to post-partum maternal health, a study found that the prevalence of postnatal depression was 6.8% 29 in an obstetric ward of a Singapore hospital. However, to date, there has not been any study investigating the prevalence of common post-partum physical and mental health problems in women in the Singapore primary care setting. This study aims to fill that knowledge gap for healthcare professionals in primary care to better identify and treat women with post-partum health problems.
The study was conducted in Choa Chu Kang (CCK) Polyclinic, one of seven clinics in the National University Polyclinics (NUP), which is a part of the National University Health Systems (NUHS) that provides public healthcare services to the Western part of Singapore. The primary aim of this study was to describe the prevalence of common maternal health problems experienced by a sample of mothers during the early post-partum weeks in a primary care setting in CCK Polyclinic. The secondary aim was to identify associations between such health problems and independent variables such as the mother’s sociodemographic characteristics, mode of birth delivery, number of children and the number of individuals providing significant child care support to the mother.
Method
Study design and participants
A cross-sectional study was carried out in CCK Polyclinic from June 2021 to December 2021. CCK Polyclinic provides primary care services, including women’s health services such as post-partum care, contraception counselling and cervical cancer screening. CCK Polyclinic was chosen as the site for our research project because of the large numbers of mothers who brought their 4- to 8-week-old newborn infants (approximately 160 infants per month) for their developmental assessment visits.
Mothers who accompanied their children for their development assessment appointments at 4–8 weeks post-delivery at the clinic were invited to participate in the study which involved completing a self-administered questionnaire. The inclusion criteria for recruiting the mothers were age at 18 years and above, have given birth in the past 4–8 weeks, not having any known cognitive impairment, and able to understand and complete the questionnaire in the English language. Convenience sampling was used in this study. Mothers who fulfilled the inclusion criteria were informed about the study and invited to participate. Implied informed consent was considered when participants completed the questionnaire, without explicit written or oral consent required. Implied consent is acceptable by the National Healthcare Group DSRB for anonymized surveys. Mothers who did not fulfil the inclusion criteria or declined to participate were not included in the study.
Procedure
The research was approved by the National Healthcare Group DSRB (Study reference: 2020/01446). Mothers who accompanied their infants to the 4- to 8-week development assessment at the clinic were invited to participate in the study by the nurses conducting the initial assessment for the infant. If the mothers were agreeable, they received a paper copy of the questionnaire that was self-administered with the instruction of bringing it back to the nurses once they had completed it. The completed responses were collected by the nurses after each day and stored in a locked cabinet. The responses were then collated by a research assistant. There were no participant identifiers used in the questionnaire to ensure patient confidentiality.
Variables
The questionnaire used in our study was adapted with permission from the questionnaire used in the Maternal Health Study, 30 a longitudinal cohort study investigating the well-being of first-time mothers in Melbourne, Australia. The questionnaire consisted of two parts: the first part comprised information about participants’ age, ethnicity, marital status, highest educational qualification, current housing type, average monthly household income per person, employment status, number of children, parity, mode of delivery and number of people who provided significant help in the care of their youngest child. These covariates have been chosen as previous studies have shown an association between them and a higher prevalence of maternal health problems.12 –22 The second part consisted of a 5-point Likert-type scale (never, rarely, sometimes, often, always) that measured the subjectively experienced frequency of 24 common post-partum problems encountered by mothers. Two of these were from the mental health domain: ‘feeling depressed, low or blue’ and ‘experiencing intense anxiety’. The other 22 were physical symptoms.
We then conducted a content and face validation of the study’s questionnaire. Content validation was done by an expert panel of senior family physicians as well as obstetrics specialists from the National University Hospital and KK Women’s and Children’s Hospital. The expert panel consisted of a mixture of female and male physicians, who were invited by the research assistant to participate anonymously as part of the Domain Specific Review Board ethics board criteria for content validation. Face validation was conducted from May to June 2021 by the research assistant in a small pilot study involving 10 invited participants who fulfilled the study’s inclusion criteria. The pilot study participants’ responses were not included in the main study. Based on the validation process, two questions (‘major bleeding from the vaginal area after birth’ and ‘heavy vaginal bleeding or other bleeding that worried you’) in the section on maternal health problems that were deemed to be overlapping and equivalent were combined into one: ‘Heavy vaginal bleeding or any bleeding that worried you after the birth of your child’. In addition, a majority of the experts suggested adding a question on breastfeeding difficulties based on their experience of a high prevalence of women experiencing this problem. The final version of the questionnaire used in the study is included in the Supplemental material section.
Our measure of symptom frequencies was subjective, which made it impossible to quantify objective occurrence rates, but did reflect mothers’ subjective experience of symptoms. This was the aspect we wanted to focus on in the present study as it was more likely to reflect to what degree mothers would notice and report symptoms during clinical consultations. After completion, collection and compilation of the questionnaires, data accuracy was ensured by the principal investigator conducting spot checks on the dataset after values were copied to an Excel worksheet from the paper forms by the research assistant. The principal investigator also looked at the paper forms of the questionnaire to double-check missing values indicated in the worksheet.
Bias
An element of selection bias could not be excluded as it was not possible to collect the demographic data of the mothers who declined to participate in the study or determine response rate. This was because these mothers were not registered patients during their infants’ developmental assessment visits and had declined to share their demographic information. Some infants were also accompanied by family members other than their mothers, hence their mothers could not be invited to participate in the study. Finally, there was a risk of recall bias although this was mitigated as the duration of recall (4–8 weeks) was short.
Sample size
Sample size for our study was calculated from the most prevalent maternal health problem in prevalence studies – fatigue – at a prevalence of 37%–67.3%.25,26 Based on the higher prevalence of 67.3%, the total sample size of a minimum of 340 patients was required to provide statistically significant results with a 95% confidence level and an accepted margin of error of 5%. A power analysis for the secondary aim (identifying correlates of health problems) was performed using G*Power (version 3.1.9.7) and indicated that the confirmatory multivariable analysis (see below) would be powered at 90% to detect a small effect size of f2 = 0.062, considering a sample size of 340 (see above), a margin of error of 5%, and the inclusion of 10 independent variables in the model.
Statistical analysis
All statistical analyses were performed using R (version 4.1.2, 2021). Descriptive statistics were used to determine the characteristics of the participants (age, ethnicity, marital status, highest educational qualification, current housing type, average monthly household income per person, employment status, number of children, parity of latest birth, mode of delivery and number of people who provided significant help to care for the newborn). The prevalence of post-partum maternal health problems was based on their frequency in the categories of never, rarely, sometimes, often, always. The last three responses were additionally collapsed to identify ‘major problems’ experienced (i.e. health problems experienced more frequently (sometimes, often or always)), while ‘minor problems’ were denoted to health problems that were never or rarely experienced. Missingness in the data collected was dealt with by performing complete case analysis.
Exploratory bivariate analyses were conducted to look for associations between the prevalence of maternal health problems (the dependent variables) and sociodemographic factors (the independent variables). One-way ANOVA was used for categorical independent variables as all of them had more than two categories, and Pearson’s correlation was used for continuous independent variables. Pearson’s correlation coefficient of 0–0.25 was considered a small correlation, 0.25–0.5 a medium correlation and 0.5 and above a strong correlation. As the association with each independent variable needed to be tested separately for each maternal health problem, Bonferroni correction was applied to the comparisons’ p-values for each independent variable across all 24 maternal health problems to account for multiple testing. Marriage and parity were not included in the bivariate analysis due to the very low number of single participants and unmarried participants with partners (respectively, 2 and 4, thus 0.5% and 1.1% of the total sample) as well as of participants with a parity of more than 1 at the most recent delivery (a single respondent reported a parity of 2, thus 0.3% of the total sample).
Finally, a confirmatory multivariable analysis used multiple linear regression to test the robustness of the associations found in the bivariate analyses while controlling for all other sociodemographic factors. We built a separate model for each health problem that was associated with any demographic factor in the bivariate analyses after Bonferroni correction, entering them as the dependent variable. The independent variable(s) of interest were those that were significant in the bivariate analysis; the models additionally controlled for the following sociodemographic factors: age, ethnicity, housing type, number of years of formal education, average monthly income per person, employment status, number of children, mode of delivery and number of individuals providing significant help for the care of the newborn. In cases where the independent variable of interest was categorical with more than two categories and had a significant main effect, we followed up with post hoc pairwise comparisons using Tukey’s Honest Significant Difference (HSD). A p-value of less than 0.05 was considered statistically significant throughout all statistical analyses.
Results
Sample characteristics
There were 373 eligible participant responses. Some participants were missing specific variables: number of children were missing in six participants (1.6% of total sample), age in five participants (1.3% of total sample), employment in three participants (0.8% of total sample), education and income in two participants (0.5% of total sample) and ethnicity, housing, and parity and mode of delivery of most recent delivery in one participant (0.3% of total sample). Missingness was dealt with by performing complete case analysis.
Table 1 shows the characteristics of the participants (N = 373). The mean age of the participants was 31.9 (SD = 4.38) years with a mean of 1.9 (SD = 1.02) total number of children. The participants reported a mean of 2.0 (SD = 1.07) other people providing significant help for the care of their most recent child. The mean total number of years of education was 13.8 (SD = 2.99), while 69.2% of the participants were in full-time employment; 58.9% of the participants had an unassisted vaginal delivery (vaginal birth without instrument assistance), 6.5% had an assisted vaginal delivery (instrument-assisted vaginal birth such as vacuum-assisted or forceps assisted), 17.5% had an elective Caesarean section (where the Caesarean section was decided in advance, prior to going into labour) and 17.2% had an emergency Caesarean (where the Caesarean section was unplanned, generally decided during labour).
Demographic information table.
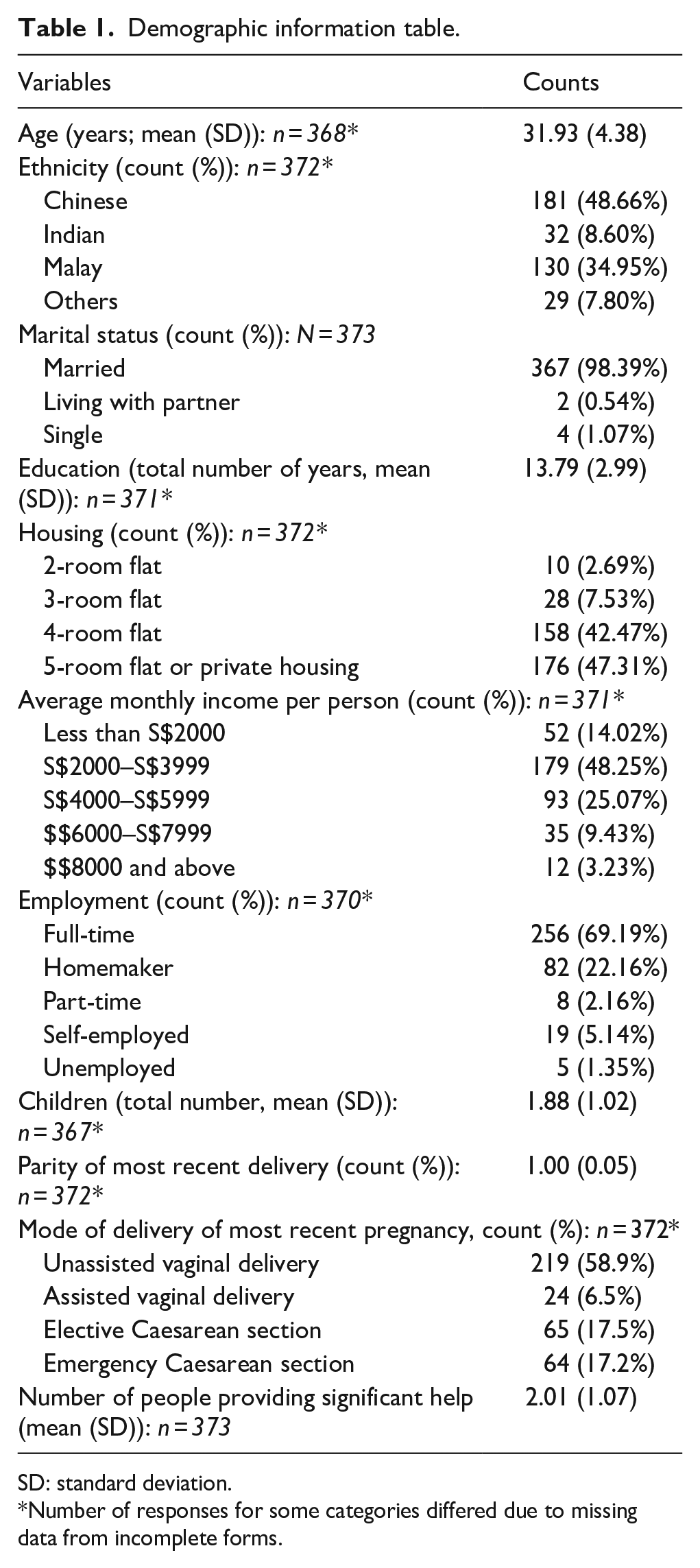
SD: standard deviation.
Number of responses for some categories differed due to missing data from incomplete forms.
Prevalence of post-partum maternal health problems at 4–8 weeks post-partum
Figure 1 shows the prevalence of major health problems that were present sometimes, often or always. The most frequent was fatigue with 77.7% (n = 372) of participants reporting experiencing significant fatigue. This was followed by lower back pain (59.3%, n = 371), Caesarean section wound pain among participants who had undergone a Caesarean section (54.3%, n = 70 out of 129), upper back pain (53.0%, n = 372) and vaginal pain among participants who had a vaginal delivery (41.2%, n = 100 out of 243). Multiple participants also reported difficulties with breastfeeding (38.0%, n = 371). The prevalence of mental symptoms, namely depression and anxiety, were, respectively, at 22.0% (n = 373) and 11.3% (n = 373). Supplemental Figure S1 included in the Supplemental material breaks down the prevalence of problems according to their frequency of never, rarely, sometimes, often and always.

Prevalence of post-partum health problems.
Significant associations between post-partum health problems and independent variables
For clarity, only demographic variables with significant associations to health problems are detailed below, namely modes of delivery and number of children. Associations with the other sociodemographic variables did not reach significance after Bonferroni correction for multiple testing, as detailed in Supplemental Tables S1–S9 in the Supplemental material.
Health problems associated with mode of delivery
One-way ANOVA analysis showed a significant effect of mode of delivery on pain on passing urine (F(3) = 6.365, p < 0.001, corrected p = 0.008 after Bonferroni correction) and on passing motion (F(3) = 9.305, p < 0.001, corrected p < 0.001 after Bonferroni correction; refer to Supplemental Table S1). Both of these results were confirmed by multiple linear regression (respectively (F21, 339) = 1.68, p = 0.003, R2 = 0.09 and (F21, 338) = 2.10, p = 0.004, R2 = 0.12; Table 2). Post hoc pairwise analyses further indicated that pain on passing urine was most pronounced with assisted vaginal deliveries compared with Caesarean and unassisted deliveries, whereas both assisted and unassisted vaginal deliveries predicted more pain on passing motion than elective and emergency Caesarean deliveries (Table 3).
Confirmatory multiple linear regression testing significant associations between the dependent variables of pain on passing urine (Model 1) and pain on passing motion (Model 2) with modes of delivery, the main independent variable of interest.

Legend:
Assisted vaginal delivery: instrument-assisted vaginal birth (e.g. vacuum-assisted or forceps-assisted).
Unassisted vaginal delivery: vaginal birth without instrument assistance.
Elective Caesarean: Caesarean section decided in advance, prior to going into labour.
Emergency Caesarean: unplanned Caesarean section, generally decided during labour.
Post hoc pairwise comparisons of modes of delivery in Models 1 and 2 adjusted with Tukey’s HSD.

SE: standard error.
Health problems associated with the total number of children
There was a small positive correlation between the number of children and the prevalence of headaches (r(364) = 0.181, p < 0.001, corrected p = 0.012 after Bonferroni correction), such that women with more children reported more headaches. There was also a small negative correlation between the number of children and the prevalence of breastfeeding difficulties (r(363) = –0.191, p < 0.001, corrected p = 0.006 after Bonferroni correction; refer to Supplemental Table S2) In our confirmatory analysis, these associations were supported by multiple linear regression (respectively (F21, 339) = 0.17, p = 0.002, R2 = 0.11 and (F21, 338) = −0.28, p < 0.001, R2 = 0.10; Table 4).
Confirmatory multiple linear regression testing significant associations between the dependent variables of headache (Model 1) and breastfeeding difficulties (Model 2) with number of children, the main independent variable of interest.

Discussion
Discussion of results
Our study found that the most prevalent problems experienced among post-partum women were fatigue (77.7%), lower back pain (59.3%), Caesarean wound pain (54.3%), upper back pain (53.0%) and vaginal pain (41.2%) at 4–8 weeks post-delivery. Assisted vaginal deliveries were associated with a higher prevalence of pain on passing urine while both assisted and unassisted vaginal deliveries tied in with higher prevalence of pain on passing motion. There was a small but statistically significant association of women with more children experiencing a higher prevalence of headache and a lower prevalence of breastfeeding difficulties.
The post-partum problems found to be the most prevalent in this study were consistent with other studies. Fatigue has been reported as the most prevalent post-partum maternal health problem experienced by women by many other studies conducted in countries such as Australia, Sweden, France and Italy.3,31 –33 Likewise, back pain has also been consistently high in the list of most prevalent problems in studies (between 43.5% and 62.7%4,31 –33). Pain over the Caesarean section wound was also a prevalent problem with Brown and Lumley 33 reporting a similar prevalence of 60.7%.
Differences in the prevalence of other maternal health problems may be attributed to different definitions for maternal health problems used in different studies. For example, Chee et al. 29 used a diagnostic interview to identify clinical post-natal depression at a prevalence of 6.8% while our study asked participants to self-report symptoms of depression that they have experienced and obtained a prevalence of 22.0%. Although less precise than objective measures, this relatively high prevalence of self-reported depressive symptoms (more than one-fifth of mothers) is concerning.
Mode of delivery has been consistently flagged out as having a significant association with various maternal health problems. Our study has found significant associations between assisted vaginal births and a higher prevalence of pain on passing urine and any vaginal birth with pain on passing motion. Similarly, Thompson et al. 34 found a higher prevalence of perineal pain among women who underwent vaginal deliveries, although they did not separate vaginal births into assisted and unassisted. Urinary incontinence has been found to be associated with vaginal deliveries as compared with Caesarean deliveries by various studies.35 –37 In particular, assisted vaginal deliveries38 –40 have been significantly linked to urinary incontinence prevalence. Our study did not find the same association between mode of delivery and presence of urinary incontinence, although this could be attributed to a difference in timing of investigating the prevalence of urinary incontinence, as our data collection was cross-sectional and took place fairly early, between 4 and 8 weeks after delivery. Urinary incontinence may take time to develop, and its prevalence tends to be higher in longitudinal studies29,30 that followed up women years after their initial delivery.
With regard to participants with vaginal deliveries reporting a higher prevalence of pain on passing motion, this was not directly corroborated by an existing study as the specific rates of this problem were either not included in or reported by studies so far. It is possible that this problem is self-limiting as studies focusing on problems months to years after delivery did not report an association of vaginal deliveries to faecal problems such as incontinence. However, there was evidence linking labour-related trauma such as anal tears, to faecal incontinence rates.41,42 In other pelvic floor-related physical problems, Hicks et al. 43 found an association between higher prevalence of dyspareunia and assisted vaginal deliveries which our study did not find, and this could be due again to the timing of our study’s sampling as many mothers may not have resumed sexual activities 4–8 weeks after delivery. There is indeed ample evidence that assisted vaginal deliveries may result in more pelvic floor dysfunction 18 and healthcare professionals should screen for these problems in women who have undergone assisted vaginal deliveries for early diagnosis and treatment.
Our study showed that women with more children tend to report a lower prevalence of breastfeeding difficulties. This is supported by studies44,45 showing that primiparous women had more breastfeeding difficulties compared with multiparous women. A qualitative study 46 done in Singapore also reported first-time mothers expressing significant concern about breastfeeding difficulties such as low breast milk supply and physical discomfort. However, there is otherwise a paucity of studies that reported on the association of the number of children on physical problems, such as headaches, that mothers may experience. Further studies are warranted to shed more light on this association.
Although various studies have linked young maternal age 47 and low income12,47 to mothers experiencing more physical problems, our analysis of socio-economic correlates of maternal health problems did not find a similar correlation. This could be due to a relatively good support system for most mothers as measured by an average of two other individuals providing what mothers consider as significant help for the first 4–8 weeks post-partum in all age groups of mothers. Singapore, being a small country, allows for easy accessibility for family members to provide support and it is still relatively affordable for families to hire a helper or confinement nanny. This may relieve some of the caregiving burden to allow mothers to recover from the delivery process. With regard to income, the difference in association with physical problems found by other authors may be due to the differences between healthcare costs and standards of living between countries and study populations. A majority (86.4%) of our study participants reported an average monthly household income per member of S$4000 and above, which is slightly higher than the 2021 national median average monthly household income per member of S$3027. 48 For our participants in the lower income group, Singapore has relatively affordable subsidized healthcare that is accessible to all and additional financial subsidies for those who qualify for them, which reduces the financial burden on parents.
Implications for clinical practice
Our study results inform healthcare professionals about the prevalence of common maternal health problems. A more structured and targeted way of screening can allow for earlier and better detection and subsequent adequate treatment of these problems that can positively impact a mother’s physical and mental well-being. As such, the study’s findings can be used to further enhance current clinical guidelines for the care of post-partum women seen in primary care. Although Singapore, to date, does not have a national post-partum care guideline, each public primary care institution has its own guidelines. NUP guidelines for post-partum care advises the healthcare professional to go through common problems such as depression, breast issues (mastitis, engorgement, breastfeeding difficulties), constipation or haemorrhoids, urinary symptoms, wound or episiotomy care and the management of antenatal issues such as gestational diabetes. In addition, other care providers in Singapore have been placing a growing emphasis on the detection and management of post-natal depression from incorporating the use of screening tools such as the Edinburgh Postnatal Depression Scale49,50 and appropriate management and referral to Maternal Wellness Services in tertiary centres.
However, current guidelines lack emphasis on assessing if the high prevalence of pain that post-partum women experience – from back pain to perineal or Caesarean pain – is detected and adequately managed during the post-partum period during visits to primary care providers. Amendments to guidelines that emphasize and prioritize the most prevalent health problems can allow healthcare professionals to improve care for mothers in the post-partum period. Factors associated with high prevalence of health problems should also be highlighted, such as paying particular attention to perineal problems in women who have undergone assisted vaginal deliveries. Informing mothers about the possible health problems they may experience may also empower them to self-treat or seek medical attention when needed.
In addition, despite guidelines containing information about common breastfeeding problems and lactation consultants available in tertiary medical centres, post-partum women still report a significant rate of breastfeeding difficulties. In a local qualitative study by Ong et al., 46 participants expressed a need for more guidance for breastfeeding in the home setting. Studies have supported an improvement in breastfeeding ability and duration when staff trained in lactation consultation were available in the primary care clinics51,52 while others acknowledged that besides healthcare professionals, there is a role for home visits, 53 peer support networks 54 or online guidance 55 such as videos for breastfeeding so that mothers could get enough support and help to overcome breastfeeding difficulties after childbirth. NUP has since started providing limited lactation nursing support in our clinics as of late 2022, after the conclusion of the study. Expansion of these services within the clinic and/or establishing links to refer mothers to appropriate informal community support groups can be considered to optimize support for these mothers.
Future studies may consider focusing on investigating the extent to which common post-partum maternal health problems are detected and treated adequately. This can help identify current care gaps and improve the tools used for screening, diagnosis and treatment of maternal health problems.
Strengths and limitations of the study
To our knowledge, this is the first study that investigated the prevalence of common maternal health problems in a primary care setting in Singapore. A wide range of common maternal health problems were included in the questionnaire that was validated through face and content validation.
A limitation of the study is recall bias as it relies on participants to remember any problems that they had over the past 4–8 weeks. However, this bias is likely to be small due to the short duration of recall. Another limitation is that there were no data collected on individuals who declined to participate in the study. Several factors that may be associated with common maternal problems were also not included; a limitation largely driven by the need to keep the questionnaire length reasonable for participants to be able to self-administer the questionnaire completely while they waited for their infant’s developmental assessment appointment. Some other factors that were not explored in this study include pre-existing maternal health problems, as well as health problems or sleeping difficulties experienced by their infants, 56 that may influence the prevalence of common maternal health problems. The impact of these factors needs to be investigated by future studies.
Conclusion
In conclusion, our study showed that a considerable fraction of women reported health problems in the first 4–8 weeks post-partum. Healthcare professionals should actively screen for these problems and treat them adequately for the physical and mental well-being of mothers, while granting particular attention to the most common maternal health problems and the group of mothers most vulnerable to them.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241227879 – Supplemental material for Common maternal health problems and their correlates in early post-partum mothers
Supplemental material, sj-docx-1-whe-10.1177_17455057241227879 for Common maternal health problems and their correlates in early post-partum mothers by Christine Ng, Anna Szücs and Lay Hoon Goh in Women’s Health
Footnotes
Acknowledgements
The study team thanks each mother who contributed her time to participating in the study. The authors also thank Professor Stephanie Brown and the Maternal Health Study team from the Murdoch Children’s Research Institute (Victoria, Australia) for sharing details of the questionnaire used in their study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.