
Abstract
Background:
Black maternal mortality is an urgent public health crisis in the United States. Community-based interventions show promise in addressing this crisis but remain underutilized.
Objective:
Using New York City (NYC) as a case study, we describe a formative study of a comprehensive community health worker (CHW)-led intervention, We Care About Brooklyn (WeCAB), designed to address structural drivers of NYC’s maternal health crisis: fragmented care and unmet health-related social needs (HRSNs), such as food insecurity and unstable housing.
Design:
Guided by the transcreation framework, we conducted a community-engaged, mixed methods formative study to design an intervention prototype.
Methods:
We conducted a document review (N = 7 HRSN screening tools), documentary film analysis, and primary qualitative data collection. We interviewed 10 key informants representing diverse community expertise. Interpretative phenomenology guided qualitative data analysis.
Results:
Analysis elaborated on five central themes—trust and rapport building, frequency of patient engagement and critical time periods, system fragmentation and care coordination challenges, technology for care coordination, and provider and client expectations. These findings, along with the document review, results of the film analysis, and evidence-based intervention inputs, informed the design of a remote precision support intervention with two core activities: (1) a digital closed-loop care navigation platform (Unite Us©) using a 41-item maternal HRSN screener, and (2) CHW check-in schedules based on gestational age and social risk, including care reminders, escalation protocols for patient concerns, urgent warning signs education, and linkage to urgent care.
Conclusion:
WeCAB was designed to enable CHWs to function as a human safety net and provide continuity of care in the context of a fragmented healthcare landscape. We propose that this approach fosters trust and patient empowerment, promoting physical and emotional well-being and engagement in care.
Introduction
Compared with its affluent peers around the world, the United States has the highest maternal mortality rate, driven largely by deaths among Black women. 1 The maternal mortality rate among Black women in the United States (49.5 per 100,000 live births) is more than twice that of the overall U.S. birthing population and nearly six times that of Canada. 1 Black maternal mortality remains a critical public health crisis in the United States rooted in longstanding historical injustices and social and structural determinants of health. 2 Meaningful solutions to this public health crisis require centering the lived experiences of Black women.
The epidemiology of the U.S. maternal health crisis: New York City perspective
In the United States, maternal mortality rates are highest in the southern states, 3 yet states with the largest birthing populations account for the greatest absolute numbers of maternal deaths. New York ranks third after Texas and Florida, with regard to total number of maternal deaths overall in the United States. 4 In 2022, NY reported 241 maternal deaths, compared with 263 in Florida and 532 in Texas. 4 New York City (NYC), the nation’s largest city, accounts for nearly 45% of the state’s approximately 206,000 annual live births, making it a major contributor to maternal deaths statewide. 5
NYC also exhibits a pronounced Black–White maternal mortality gap, making it a prime illustrative case for understanding and seeking solutions to the U.S. maternal health crisis. Between 2016 and 2020, the Black–White gap in pregnancy-related death was 6:1. 6 According to the New York State Maternal Mortality Review Committee, 70% of pregnancy-related deaths occurred within the postpartum period and 74% were preventable. 7 Major contributing factors include fragmented care, limited awareness of urgent warning signs, inadequate risk assessment and follow-up care, and dismissal of patient concerns due to race. 7
Because maternal mortality is a statistically rare outcome, severe maternal morbidity (SMM) has emerged as a critical focus for both understanding maternal health disparities and measuring impact of interventions. In NYC, Black women face a higher risk of SMM, often described as a “near miss” to maternal death, with the highest rates among Black immigrant women, who are concentrated in Central Brooklyn. 8 Three Central Brooklyn neighborhoods (Brownsville, East Flatbush, and East New York) have the highest SMM rates in NYC, reaching 568/10,000 deliveries, far exceeding NYC and U.S. averages and reflecting a 40% increase since 2008. 8 These neighborhoods comprise about 10% of Brooklyn’s 2.6 million population. 9 Central Brooklyn is also a historically disinvested area with a persistent, disproportionate burden of disease and mortality, a legacy that continues to shape the region’s maternal health crisis.10,11
The Black–White disparity in SMM in NYC reflects a history of structural racism and marginalization.12,13 To isolate system-level factors, Howell et al. ranked hospitals by adjusted SMM risk accounting for patient sociodemographic and medical factors. 13 They found that Black women were more likely than White women to deliver in higher-risk hospitals, and later demonstrated that racial disparities persisted within individual hospital systems. 14 A 2020 NYC study showed that women in ZIP codes with the highest concentration of poor Black residents relative to wealthy White residents experienced SMM rates four times higher than those in the lowest-concentration neighborhoods; delivery site explained only 35% of this difference. 12 Additionally, a 2024 NYS Department of Health report found poor perinatal hospital quality across Brooklyn, with the lowest scores in majority-Black neighborhoods. 15 Together, these findings indicate that NYC delivery sites with the highest SMM rates are located in historically marginalized neighborhoods, perpetuating a legacy of “separate and unequal care.”11,16
Moving beyond hospital-based initiatives to address the maternal health crisis
While responses to maternal mortality have historically focused on hospital-based interventions, there is growing recognition that community-based approaches are critical to addressing Black–White disparities in maternal death.17–19 Ricklan et al. conducted a systematic review of two decades of interventions to reduce maternal mortality in NY state. Of the 16 studies reviewed, all but 1 intervention was hospital-based. The dominant model was New York’s Safe Motherhood Initiative, which implemented clinical protocol “bundles” to address hemorrhage, severe hypertension, and venous thromboembolism; none reduced SMM or maternal death. The sole community-based intervention was associated with lower rates of preterm birth and low birthweight. 17 Authors conclude with a call for community-based initiatives that integrate community health workers (CHWs).
Addressing the disparities in maternal mortality and SMM require an explicit focus on root causes and the underlying structural and social drivers of these disparities. 2 Accordingly, addressing social determinants of health and prioritizing health-related social needs (HRSNs)—basic survival needs such as food security and adequate housing—remains paramount.20,21 Challenges to meeting HRSN may deter pregnant persons who have been systematically neglected from engaging in care. 22 Needed prenatal or postpartum care (PPC) may not be realized until individuals gain control over life stressors, consistent with Maslow’s “hierarchy of needs.” 23 Optimizing care engagement is fundamental to preventing adverse maternal outcomes. In NYC, the SMM rate among women with no prenatal care is more than twice that of women who receive care in the first trimester. 24
However, addressing HRSNs of the maternal population remains a challenge. NYC’s maternal health crisis is driven by a fragmented healthcare and social service landscape. Community-based organizations (CBOs) work independently and have differing areas of expertise. Their funding streams are diverse, cyclic, and uncertain. At the same time, healthcare systems have misaligned incentives, which can lead to inefficiency. 25 In the current standard care setting, clients must navigate this fragmentation on their own, and they are often lost to care, which can be fatal.25,26
Consistent with recommendations from the Ricklan et al. review, CHWs represent a vital link to healthcare and social resources in this fragmented care setting.27–31 The Pathways Community Hub (PCH) model, for example, is a community-based care navigation system that uses CHWs to connect high-need, high-risk clients with social and medical services.32–35 Under the leadership of CBOs, CHWs engage hard-to-reach clients where they are and identify a core set of HRSNs called “Pathways.” The PCH model is grounded in evidence-based principles that focus on health equity, care coordination, and patient-centered care.36–40 Evaluation studies of the PCH model provide evidence of efficacy and cost savings,34,41,42 but evidence remains limited on whether addressing social needs improves health outcomes.37,43
We report on a formative study of a CHW-led intervention prototype, We Care About Brooklyn (WeCAB), which builds on the PCH model and targets system-level drivers of maternal death and morbidity in NYC. The study draws on NYC’s long history of maternal health advocacy,44,45 and intentionally centers the voices and expertise of community practitioners and leaders to ensure meaningful integration of the perspectives from those most impacted by the maternal health crisis. 46 Accordingly, the community-engaged implementation science framework of transcreation, which places equal value on community practice and peer-reviewed evidence, was used to guide the selection of intervention inputs and the WeCAB design. 47
Methods
Overview
The transcreation implementation science framework for intervention development guided our community-engaged formative phase with the following steps: (1) identify community infrastructure and engage partners, (2) specify theory, (3) identify multiple inputs for a new intervention, (4) design intervention prototype, (5) design study, methods, and measures for community setting, (6) build community capacity for delivery, and (7) deliver the “transcreated” intervention and monitor the implementation process. 47 A long history of community engagement and extramural funding (2022–2024) has generated pilot data and guided us through all transcreation steps.48,49 The transcreation framework, a community-engaged intervention design framework, was used to guide our intervention prototype design. The WeCAB intervention prototype was developed in the context of a 2-year pilot efficacy trial. We describe our study setting and detail steps 1 through 4 of transcreation below.
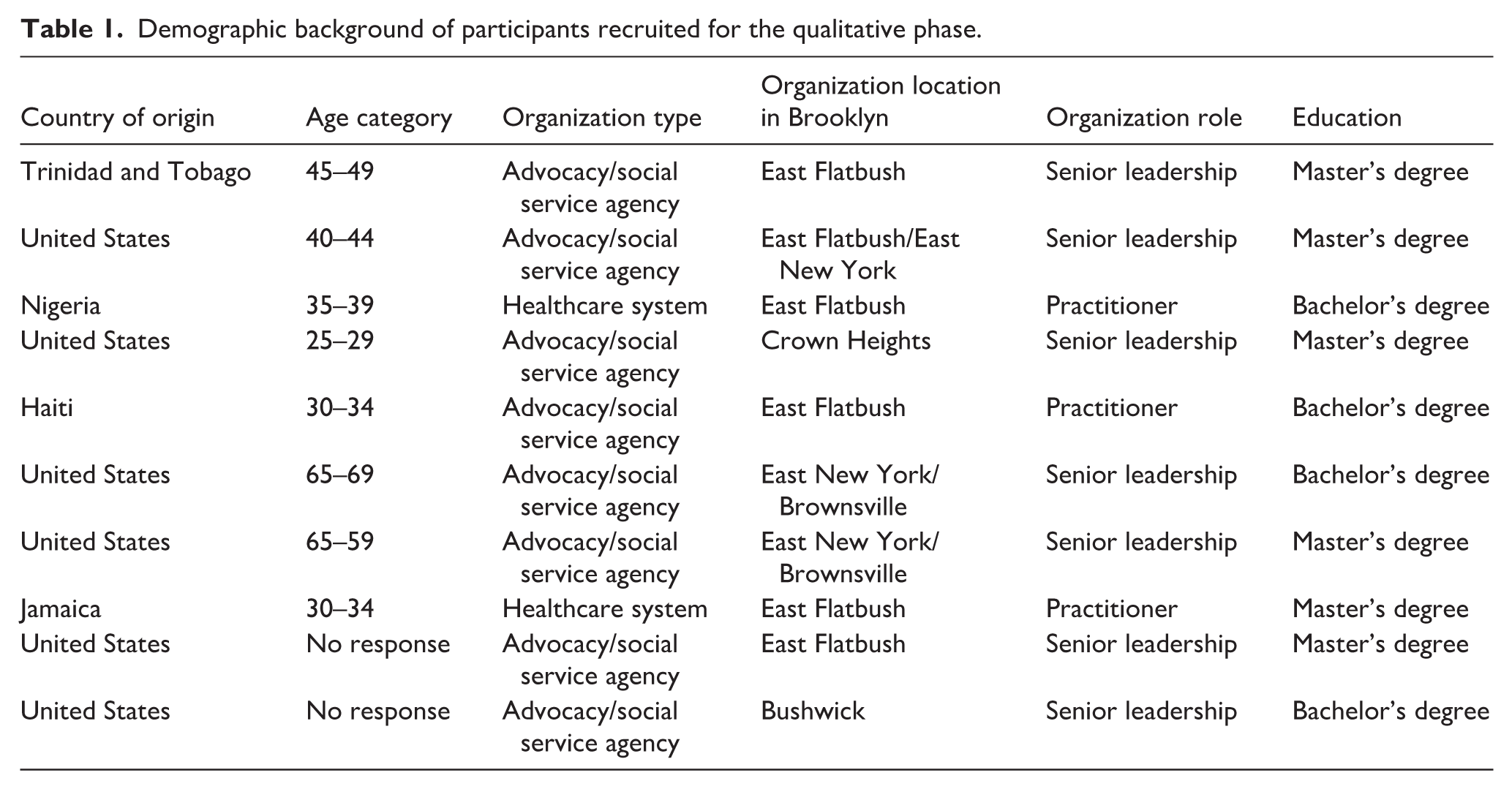
Our intervention setting was Brooklyn, NYC (a borough of 2.6 million people), which has a racial/ethnic demography that is distinct from the national landscape, warranting special focus. In Brooklyn, almost 27% of residents are Black (relative to 20% in NYC) and almost 35% of are foreign-born, the overwhelming majority originate from Asia, Latin America, and the Caribbean (over 75%). 50 Furthermore, the percentage foreign-born reaches 48% with most residents originating from Jamaica, Haiti, and Trinidad and Tobago (52%) in the catchment area of our academic medical center. 50 Our priority population was pregnant women residing in Central Brooklyn, NY (70%–90% Black and Latino). 51
SUNY Downstate Health Sciences University is the only academic medical institution in Brooklyn and is situated at the center of NYC’s maternal health crisis. Downstate has strong historical ties and trust among Central Brooklyn families. However, similar to many other institutions in Central Brooklyn, Downstate has suffered from long-standing structural inequities that have contributed to fragmented care. Our novel intervention was developed with the knowledge and experience of the challenges faced by such safety-net institutions.
Step 1: identify community assets and infrastructure
The WeCAB intervention design follows a long history of community engagement by members of our research team, addressing the foundational transcreation step of identifying community infrastructure and establishing partnerships. Collectively, our team has over 15 years of experience working and advocating for the Central Brooklyn community. Study authors are diverse with regard to race, ethnicity, life stage, and experiences of intersectionality (affinity toward distinct social identities). 52 Our team includes both faculty and student learners, representing public health, obstetrics, medicine, and community advocates. Authors self-identify as a Black woman, White woman, Haitian American, Filipina American, Eritrean American, and some as Brooklyn residents. While some of us were raised in the local Brooklyn community or similar communities in which we work and study, we acknowledge that professional training and social positions shape our worldview and data interpretation. We therefore practiced reflexivity throughout the research process to avoid assumptions about the diverse experiences represented in the study.
In 2018, our team led the formation of a consortium of four safety-net hospitals providing obstetric services to Central Brooklyn. Since 2019, in partnership with the Arthur Ashe Institute for Urban Health (AAIUH), a leading Brooklyn-based CBO, we have co-led the SUNY Women’s Health Community Advisory Board (CAB), which is comprised of community leaders, health and social service providers, and consumers. The CAB routinely co-designs and conducts community-engaged research to better understand the needs of the maternal population in Central Brooklyn. 53 We have also participated in a variety of community events and legislative debriefings designed to brainstorm solutions to NYC’s maternal health crisis.
Step 2: specify theory
Our conceptual approach centers on the notion that only when basic survival needs are met can pregnant persons feel a sense of agency and exert control over higher-order needs such as prioritizing prenatal and PPC.23,54 It is motivated by the PCH model, our team’s lived experiences and central tenets of classic behavioral theories including the social cognitive theory, the health belief model 54 and the Gelberg–Andersen Behavioral Model for Vulnerable Populations. 22 To understand health-seeking behaviors of vulnerable populations, central domains of this latter model include predisposing factors (sociodemographic factors that increase vulnerability), enabling resources, and perceived need for care. Addressing HRSNs falls under the domain of enabling resources, or factors that either facilitate or serve as barriers to engaging in care. This domain includes personal resources (e.g., health insurance, social support, partner status), community resources (well-coordinated versus fragmented services and information systems), and competing needs such as food insecurity, unstable housing, childcare, and transportation. The health belief model 54 additionally proposes perceived barriers and benefits of engaging in health promoting behaviors and cues to action, which are external stimuli needed to motivate recommended behavior change.
Step 3: identify intervention inputs
According to transcreation, the prototype development phase entails identifying scientific evidence and consulting with the community on locally developed programs, community resources, and target population. 47 Following this guidance, we implemented a formative phase from March to November 2023, which is summarized in Figure 1. This formative phase entailed community-engaged mixed methods research and a review of the scientific evidence on CHW interventions that addressed maternal health outcomes and those that addressed social needs in prenatal care settings. Our mixed methods included a document review to understand the current state of HRSN screening tools and qualitative interviews with community partners. In addition, the qualitative data we collected was triangulated against a thematic analysis of a documentary film. All qualitative research procedures followed the COREQ reporting criteria. 55 Study procedures were approved by Downstate and an external institutional review board (approval # 1978292). Respondents gave written consent for review and signature before starting interviews.

Overview of WeCAB prototype design.
Step 3a: qualitative data collection and analysis
A total of 10 participants were engaged through 2 focus groups and 2 key informant interviews. We approached potential key informants through a combination of face-to-face, email, and telephone communication. Eligibility criteria for participation in this qualitative phase was (1) age 18 years of age and older and (2) employment by one of our community partners representing the social service and healthcare sectors (doulas, social workers). Following Creswell, we utilized purposive sampling. 56 We identified key informants from our social network and members from the SUNY Women’s Health CAB. Key informants represented diverse providers and staff who were able to provide valuable insights on maternal health and care coordination of health and social services. This sample selection is consistent with rapid appraisal or community needs assessment methods that suggest anywhere from 4 to 15 key informants.57,58 Additionally, in qualitative studies, the researcher is considered an instrument in the collection and analysis of data. The researcher’s lived experience, professional expertise, and community knowledge allows he or she to build rapport, formulate open-ended questions, and listen actively. 59 Building on many years working in the Central Brooklyn community, our all female team collectively developed the semi-structured interview guides used; one of the study PIs moderated the focus groups, with support from a note-taker, and a rigorously trained graduate-level research coordinator conducted the key informant interviews. Each focus group or interview lasted approximately 2 h and was audio-recorded. Focus groups took place in a private workplace setting and interviews were telephone-administered.
Interview questions were designed to gain greater insight into locally developed programming and included the following a priori themes: frequency and timing of CHW check-ins and engagement, community assets and approaches to care coordination, CBO capacity for close-loop referrals, and range of social needs for the maternal population. Interviews were conducted until thematic saturation was reached. Data collection and analysis occurred simultaneously. Transcripts were transcribed verbatim and anonymized before coding to protect participant confidentiality.
Interpretative phenomenological analysis (IPA) was used as the guiding perspective to explore the lived experiences of our community partners with regard to serving pregnant persons in our Central Brooklyn population.56,60,61 IPA aims to explore in detail how participants make sense of their personal and social world and to deepen or extend understanding of the participants’ experiences. This process involved two trained coders reading and open-coding all transcripts, meeting to discuss initial codes, then collating the codes into themes and sub-themes. Over several meetings and re-reviews of the transcripts, themes were iteratively refined and defined. We used Dedoose version 9.2.012 (SocioCultural Research Consultants, LLC; Dedoose, 2023) to assign codes and conduct thematic analyses.
The central method of our analysis was the application of a hierarchical coding structure. Parent codes were designed to capture broad conceptual domains and child codes represented finer-grained subcategories which specified different aspects within these domains. Codes were developed through both deductive and inductive approaches. Deductive parent codes were derived from the study a priori themes and existing literature on maternal and child health. Inductive child codes were generated during open coding of transcripts. This ensured that the framework reflected participant language and emergent insights. Investigative team researchers independently coded the transcripts, applying both parent and child codes. Discrepancies were reviewed in debriefing sessions, during which consensus was reached and refinements to definitions were made. This iterative process emphasized the consistent application of child codes to illustrate specific practices or needs while maintaining alignment with broader parent categories. The layered coding framework contributes to validity by allowing patterns to be verified across multiple levels of abstraction (broad parent domains and detailed child subthemes). Triangulation across focus group and key informant data further reinforced confidence in the findings.
We also held two dissemination events in October of 2023, which provided an opportunity for member checking and sharing of preliminary findings: a grand rounds seminar (clinical teaching round) and a panel discussion of the documentary Aftershock.62,63 Following these events and to supplement the primary data, we conducted a thematic analysis of the Aftershock documentary. Our thematic analysis used the film’s overarching narrative as the unit of analysis with a specific focus on lived experiences of Black women interactions with a failed healthcare system. To assess risk of filmmaker bias we considered authenticity, credibility, representativeness, and meaning. 64 With regard to authenticity, the film centers the lived experience of the daughter of one of our community partners. In terms of credibility, we employed data triangulation by cross-referencing the documentary’s qualitative accounts with epidemiological data, authoritative agency reports on maternal mortality in the United States 7 and primary qualitative data collected in this formative study.
Step 3b: document review of HRSN screeners
We conducted a document review to understand the current state of HRSN screening tools. We chose an initial set of tools based on recommendations from our social network and selected those that were published and most commonly used. We reviewed four published, validated, or expertly developed screeners including the Accountable Health Communities (AHC)-HRSN Screening Tool,65,66 the Protocol for Responding to & Assessing Patients’ Assets, Risks & Experiences (PRAPARE),67,68 Montefiore Social Needs Assessment 69 and the American Academy of Family Physicians (AAFP) Social Needs Screening Tool. 70 A second phase of HRSN screening tool selection was implemented. The study team requested and reviewed copies of all forms used to screen for HRSN from staff and providers who participated in focus groups and key informant interviews. An additional three HRSN tools were reviewed. Finally, during the focus groups, we presented earlier pilot data on HRSNs, collected with the AAFP tool, in our maternal population and specifically queried about other HRSNs not captured in existing tools, unique to the maternal population.
Step 4: design intervention prototype
We examined commonalities of evidence-based interventions and considered community input on locally developed initiatives based on results of our qualitative phase and document review. 47 We report on this process below.
Results
Qualitative interviews
Characteristics of key informants are found in Table 1. Given the focused nature of the study and the modest dataset, saturation was reached early. By the second transcript, recurring patterns were evident at both the parent and child code levels. For example, themes of rapport, reliability, distrust, and structural barriers surfaced repeatedly across data sources, with child codes such as “keep promises” and “distrust of providers” appearing consistently. The repetition of these codes across all four transcripts suggests that the major thematic domains have been fully captured. The final codebook contained 34 parent codes and 75 child codes. Table 2 summarizes the key themes and subthemes derived from qualitative data collected through interviews and focus groups with providers and CHWs involved in maternal care in Central Brooklyn. While there was a range of themes that emerged, our analysis focuses on those that directly pertain to the a priori themes. The findings highlight critical areas such as trust and rapport building, patient engagement during key postpartum periods, challenges related to fragmented care, the role of technology in coordinating services, and the expectations held by both providers and clients. These themes reflect the systemic barriers and opportunities for improvement in the provision of maternal healthcare services and underscore the need for an integrated, community-engaged approach to care.
Demographic background of participants recruited for the qualitative phase.
Summary of themes from qualitative data analysis.

Trust and rapport building
We found that participants deemed trust and rapport as components that are critical for successful care coordination. Providers who demonstrated empathy, made efforts to connect with their patients on a routine basis and reliably followed through on promises cultivated credibility, which enhanced the receptivity of clients to referrals and health recommendations.
Patient engagement and critical time periods
The timing and frequency of patient engagement was another critical determinant of care quality. Frequent communication, particularly within the early postpartum period, was deemed essential for identifying and mitigating complications. Intensive support during this critical window prevents escalation of issues and may improve adherence to medical advice.
Challenges of care coordination, fragmentation and use of technology
Participants noted that fragmentation of services and capacity constraints frequently impair coordinated outreach. For example, funders, in many cases inadvertently, place a tremendous pressure on social service providers to take on high caseloads and thus providers must balance their funding directives with their capacity to provide responsive and supportive care. These constraints often result in the inability to provide adequate care and support to clients due to lack of resources, time and fragmentation, which can foster and exacerbate existing distrust among clients. Further, existing CBO referral processes are often managed via email or paper/pencil referral forms. The menu of services (food pantry, housing support, etc.) available to clients are based on word of mouth and the intelligence that many of our CBO partners have accumulated over the many years of serving the community and therefore result in referrals made to a small subset of agencies. Digital platforms for care coordination such as Unite Us© provide a centralized database for a universe of services across a larger geography, and in our case all of NYC, and therefore hold potential for a larger universe of services. Furthermore, the Unite Us© platform provides efficient close loop care coordination that allows a care manager such as a CHW to follow a client’s journey to ensure service uptake. We directly queried informants about whether existing care coordination web-based platforms such as Unite Us© would facilitate care coordination. While technology for care coordination could theoretically streamline resource matching, participants encountered outdated information, limited partnerships/restricted access, and complex referral pathways. Consequently, the promised efficiencies of digital tools remain underrealized.
Finally, Aftershock, a documentary film, that served a secondary source to the qualitative data gathered, echoes the urgency of NYC’s fragmented healthcare system discussed above. 63 Through a critical analysis of the Black maternal health crisis in the United States the film explores the story of two young Black women in NYC who both died after emergency C-sections. Despite the repeated calls to frontline healthcare staff about their symptoms (shortness of breath, chest pain, and severe belly pain), their concerns were dismissed; both received care at one of NYC’s safety-net hospitals. The film’s main plot relates the personal losses of the two women to structural inefficiencies and the systematic racism embedded in the healthcare system.
Provider and client expectations
Our qualitative analysis also demonstrated that provider and client expectations sometimes appeared misaligned. Providers struggle with high case loads and procedural red tape in their efforts to ensure that client needs are addressed and that close loop referrals are achieved. While these constraints can contribute to complacency, providers also report doing their best to meet client needs. At the same time, clients sometimes cannot appreciate the administrative barriers that providers face and often lose patience or trust in the process of long wait times or lack of follow-up care. Clients hoping for immediate or comprehensive solutions sometimes encountered system-level constraints (such as eligibility requirements and high caseloads) which provoked frustration on both sides.
Document review
To assist in developing the WeCAB Maternal Health Screener, we organized the items/questions for each HRSN screening tool based on population characteristics and domains from The Behavioral Model for Vulnerable Communities (Table 3). 22 This resulted in the development of the WeCAB Maternal Health Screener, a 41-item assessment tool designed to identify HRSNs in a maternal population. It was developed by integrating novel questions, informed by qualitative analysis of focus groups/interviews described above, with items from published screeners. We prioritized the AHC screener as it has been officially endorsed by the Centers for Medicare & Medicaid Services 71 ; as such, we ensured that we were inclusive of all the domains/items included in the AHC screener. Furthermore, the AHC screener achieved a good balance with regard to breadth and number of survey items contained within the AAFP and PRAPARE tools—both tools were validated or constructed using validated survey items and were already being widely used across departments within our institution. The WeCAB Maternal Health Screener assesses needs across predisposing and enabling population characteristics with traditional and vulnerable domains represented. The WeCAB Maternal Health Screener places emphasis on the following domains: mental illness/emotional well-being, social and instrumental support, newborn/mom material needs and experiences of violence.
Comparison of published HRSN Screeners including the Accountable Health Communities health-related social needs screening tool, PRAPARE, Montefiore social needs assessment, the American Academy of Family Physicians social needs screening tool and the WeCAB maternal health screener.

WeCAB: We Care About Brooklyn; HRSN: health-related social need; AHC: Accountable Health Communities; AAFP: American Academy of Family Physicians; PRAPARE: Protocol for Responding to & Assessing Patients’ Assets, Risks & Experiences.
Design of intervention prototype
Table 4 maps WeCAB intervention components to theoretically justified or evidence-based intervention activities and themes identified during the formative phase.72–76 Figure 2 provides a visual summary of the intervention mapping to illustrate how the qualitative themes map on to the seven competencies and how these competencies map onto the two core prototype activities. The WeCAB prototype competencies and activities were designed to center trust and rapport building between the client and CHW as well as to foster client trust in the hospital as an institution (our final theme). Competencies refer to learning objectives that guide the CHW curriculum. These seven foundational competencies can be mapped onto two core WeCAB intervention prototype activities. System fragmentation, challenges in care coordination, and use of technology are mapped onto the first core activity-digital close loop care coordination. Patient engagement, critical time periods, and provider/client expectations are mapped onto a hybrid in-person/remote precision check-in schedule based on social risk and gestational age that includes (1) urgent warning signs education based on the CDC Hear Her© campaign, 77 (2) linkage to urgent care, (3) cues to action to encourage American College of Obstetricians and Gynecologists (ACOG) recommended prenatal and PPC, 78 and (4) escalation of patient concerns including reports of implicit bias.
Mapping WeCAB intervention prototype competencies to evidence-base interventions and qualitative phase themes.

CHW: community health worker; WeCAB: We Care About Brooklyn.
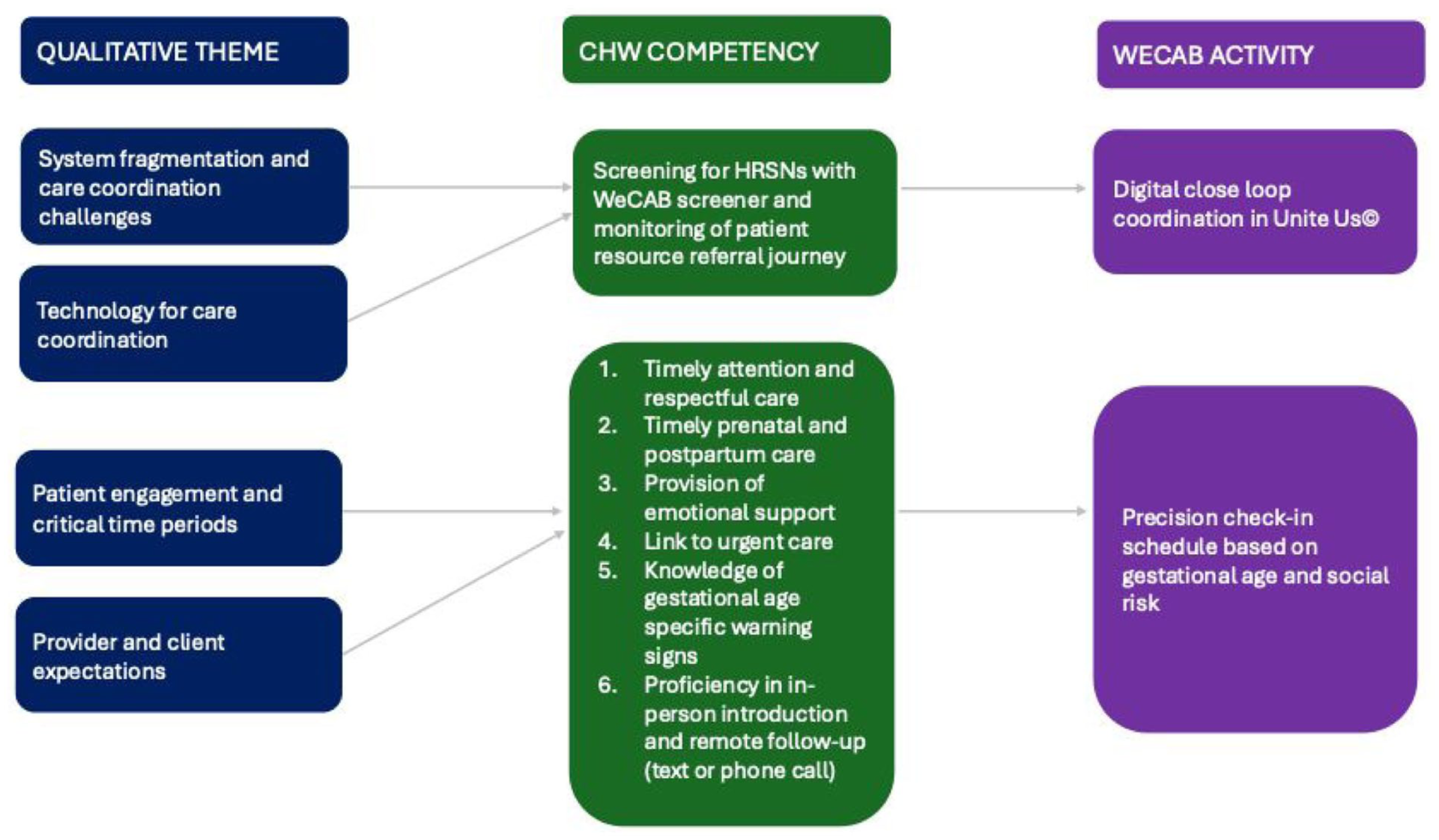
Mapping qualitative themes onto WeCAB competencies and activities.
The closed loop digital care coordination was implemented using the Unite Us© web-based platform, established in 2012 with funding from Medicare and Medicaid Innovation.93–96
The final 41-item WeCAB Maternal Health Screener was digitized and integrated it into the Unite Us© platform. WeCAB CHWs screen for HRSNs using our WeCAB screener and based on client responses the platform then provides a set of referrals. Referrals are sourced from information on community assets across NYC into a centralized database. Through its public-facing website, Unite Us© allows a client or healthcare professional (e.g., CHW or physician) to search and identify social and wellness resources across all of NYC, allowing us to optimize our: (1) chances of finding a service agency with adequate capacity, and (2) ability to close loop in care in a timely manner. CHWs have full visibility of a client’s record and can track whether referrals were closed/completed in the platform. Unite Us© currently houses one of the largest resource directories in NYC and includes 1670 in-network programs; the top 5 referred service types are individual/family support, mental/behavioral health, physical health, food assistance, and benefits navigation. We work closely with Unite Us© dedicated community engagement staff to ensure close-loop referrals with daily monitoring of the system, thus also ensuring follow-up and escalation when referrals are not accepted.
2. The precision check-in schedule (Table 5) and the supporting activities (warning signs education, linkage to urgent care, escalation of patient concerns, appointment reminders) were designed to address systemic failures and care fragmentation. The precision check-in schedule determines the number of CHW outreach attempts (via text or phone call) to clients based on social risk and gestational age; it allows the CHW to serve as a patient advocate and as a second line of defense after the clinical care team to prevent pregnant clients from falling through the cracks of such systems. For example to encourage recognition of warning signs among clients, CHWs are trained to provide a CDC urgent warning signs and symptoms info sheet at the commencement of the intervention and reinforce the information during follow-up communications. In the event a client reports on a warning sign/symptom either through a scheduled check-in with the CHW or through spontaneous outreach by the client to CHW, the CHWs are trained to instruct clients to seek urgent care immediately, report the incident to the assigned obstetrician and follow-up until the incident is resolved and addressed.
WeCAB CHW precision check-in schedule (minimum engagement requirement).

CHW: community health worker; WeCAB: We Care About Brooklyn; HRSN: health-related social need.
Risk level is determined by the WeCAB Maternal Health Screener. Low risk = 0 HRSN needs, high risk = >1 HRSN needs, critical risk = domestic violence or unhoused.
Figure 3 presents a logic model based on Kirby’s Behavioral-Determinant-Intervention approach, illustrating how WeCAB’s core activities influence PPC utilization through trust-centered causal pathways. 97 To help pregnant persons navigate a fragmented system of care, WeCAB shifts the paradigm from hospital-only care to shared hospital-community accountability for maternal health and social outcomes, addressing both interpersonal and systems-level factors.

Logic model for WeCAB.
At the system level, because approximately half of maternal deaths in NYS occur within 42 days postpartum, WeCAB introduces a new provider practice protocol aligned with the “4th trimester” concept and ACOG recommendations for contact within 3 weeks of delivery followed by a comprehensive visit by 6 weeks. 78 Clinics also link with CBOs and integrate CHWs into their clinical workflow. At the interpersonal level, intervention mapping (Figure 2), informed two core activities to foster timely support and advocacy in a respectful manner. Time is often overlooked as a social determinant of health, 82 despite evidence of racial disparities in receipt of timely care98,99 and evidence that responsiveness is central to trust-building, particularly amid fragmented care and historic marginalization.72,100
With regard to causal pathways that map WeCAB core activities onto outcomes and public health goals, caring for pregnant persons’ daily survival needs, providing opportunities for patient escalation/linkage to urgent care, urgent warning signs education and precision, timely support combined can increase patients’ trust in the provider. The core activities also synergistically work together to promote knowledge of warning signs and to influence patients’ perception of stress and social support/enabling resources.22,54 As proposed by the Gelberg–Andersen model, 22 collectively these determinants influence patient empowerment and capacity to prioritize healthcare. CHW check-ins and reminders will also serve as cues to action 54 and will directly impact PPC. At the system level, the clinic-community linkage influences enabling resources 22 while obstetrician 3-week guidance directly influences PPC.
Discussion
A community-engaged, mixed method formative research phase guided by transcreation 47 informed the WeCAB prototype design (Figure 1). Qualitative data and evidence-based intervention inputs informed a remote maternal health precision support intervention with two core components: (1) a digital closed-loop care navigation platform (Unite Us©) using a 41-item WeCAB HRSN screener and centralized referrals to community resources; and (2) CHW check-in schedules based on gestational age and social risk, including escalation protocols for patient complaints (including health concerns and provider implicit bias), reminders for prenatal and PPC, urgent warning signs education based on the CDC “Hear Her” campaign, and linkage to care. To build CHW capacity, the WeCAB curriculum includes seven core competencies (Table 4), aligned with the 10 core CHW roles identified by the Community Health Worker Core Consensus (C3) Project. 101 WeCAB trains CHWs to deliver precision support and advocacy in a hybrid in clinic/text/phone call format based on gestational age to pregnant persons and respond to their needs in a timely and respectful manner.
The CHW model is nearly a century old 27 and widely recognized as a cost-efficient strategy for under-resourced, fragmented healthcare systems. CHWs provide social support, serve hard to reach populations in urban and rural settings, and support task-sharing.27–31 In maternal health, evidence shows CHWs reduce illness and complications through education, reminders, and increased referrals to care, underscoring their vital role in facilitating timely access to urgent services.31,81,83–90 CHW interventions addressing unmet HRSNs have also demonstrated cost savings and improved referral success.20,21,102,103 Despite this evidence, CHWs are not integrated into routine maternal care in the United States. 104 In NY State, the absence of uniform CHW training requirements and standardized core competencies limits the collective impact of this essential workforce. 105
WeCAB’s comprehensive, CHW-delivered activities fill a critical gap in maternal health solutions for NYC. Reliance on hospital-based initiatives alone has shown no measurable impact on maternal mortality in New York, and effects on SMM remain inconclusive across broader U.S. and global settings. 106 The WeCAB model is simple, yet innovative, and sufficiently comprehensive to address failures in a fragmented care system. It aligns with the 2024 NYS Health Equity Reform 1115 Medicaid Demonstration Waiver, 107 which will reimburse eligible CBOs—organized as Social Care Networks—for selected health-related social services.
WeCAB’s conceptual foundation aligns with emerging NYC initiatives that have not been formally evaluated including neighborhood stress free zones 108 and the maternal medical home. 109 Notably, a Colorado evaluation of a hospital-based maternal medical home model found no measurable impact on maternal outcomes. 110 Maternal medical homes are hospital-based and rely on detailed sociomedical risk assessments to identify high risk patients and connect them to intensive supportive care teams. In contrast, WeCAB employs a shared hospital-community model, leveraging a wider network of community resources to address HRSNs through CHWs and close-loop referral system. Unlike previous prenatal interventions targeting single needs (e.g., domestic violence or food insecurity), 43 WeCAB’s maternal-specific HRSN screener within the Unite Us© platform enables CHWs to address a full spectrum of needs via a digitally-enhanced navigation and close-loop referral system. This digital innovation along with WeCAB’s remote check-in modality builds on the existing evidence base on digital maternal health solutions111,112 and promises improved access to care, patient engagement, and rapport building.
Limitations
This study reports on a formative phase to develop an intervention; further testing is needed to evaluate impacts on health outcomes. We acknowledge limitations related to scale and generalizability. The initial qualitative phase included a small sample, with key informants drawn from our CAB and partner organizations in Brooklyn. Although their deep community knowledge is a strength, perspectives may not generalize to other settings. Given the focused scope, thematic saturation was reached early without compromising depth.
Patient voices were not included in the present analysis. Although WeCAB patients were interviewed after the intervention to inform refinements, these data remain under analysis. We also recognize potential bias in using the documentary Aftershock as a secondary data source. While the film provides insight into the U.S. maternal health crisis, it focuses on NYC and birthing individuals, omitting provider perspectives. Rather than claiming universality, we triangulated the film’s themes with other evidence to support the conclusion that persistent maternal health disparities are structurally driven.
Scaling WeCAB across diverse health systems may be challenging due to variation in institutional resources and leadership buy-in. Implementation science frameworks can guide testing and refinement in new settings.47,113 The Consolidated Framework for Implementation Research (CFIR) identifies physical infrastructure and workflow compatibility as key “inner setting” determinants of implementation success. 113 Because WeCAB was designed for safety-net institutions in low-resource settings, its remote delivery modality may reduce demands on infrastructure and workflow integration.
Integration into routine practice and broader dissemination depend on CFIR “outer setting” factors, including policies and external incentives that support implementation. 113 The NYS 1115 Medicaid waiver, which reimburses selected social services, is one such mechanism. 29 However, barriers to integrating CHWs into the U.S. healthcare workforce remain including limited standardization of core competencies, workplace discrimination, and low reimbursement rates.114,115 Future cost-effectiveness studies of WeCAB could help advance these efforts.
WeCAB centers the lived experiences of women in Central Brooklyn, who are disproportionately affected by SMM and maternal mortality in NYC, which may limit generalizability. However, the prototype addresses broader concerns by targeting fragmented care and systemic racism—key drivers of the U.S. maternal health crisis that exist in both urban and rural settings.
Conclusion
Given fragmented care within a context of systemic marginalization, addressing NYC’s maternal health crisis requires an approach beyond improving hospital-level performance. We developed WeCAB as a systems-level, patient-centered solution to mitigate the cumulative effects of marginalization on maternal health.2,116 By addressing socioeconomic challenges, WeCAB was designed to reach pregnant individuals where they are, rather than requiring them to navigate a complex fragmented system. WeCAB CHWs are trained to provide a human safety net and timely, respectful care. Altogether, these competencies promote trust and perceived social support, which in turn enhances receptivity to referrals and health recommendations, reduces stress, and promotes care engagement. A future outcome evaluation will assess WeCAB’s impact on depressive symptoms, perceived stress, and PPC following the final steps of the transcreation framework. 47
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261435755 – Supplemental material for We care about Brooklyn: A remote precision support intervention designed to improve maternal health and well-being
Supplemental material, sj-pdf-1-whe-10.1177_17455057261435755 for We care about Brooklyn: A remote precision support intervention designed to improve maternal health and well-being by Aimee Afable, Sandra Bruening, Breanna Watson, Faven Araya and Christina Pardo in Women's Health
Footnotes
Acknowledgements
We would like to acknowledge and thank all the community leaders and members whose voices are represented in this work.
Ethical considerations
The Institutional Review Board at Downstate Health Sciences University and an external review board approved the study (approval no. 1978292).
Consent to participate
All participants gave written informed consent before starting interviews.
Consent for publication
We have obtained written informed consent to publish all information reported here.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work presented here was supported by a grant from NIH Award #R21NR020706.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available because the data is qualitative and includes a small set of participants with potential for participant identification.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.