
Abstract
Background:
Smoking during pregnancy remains a major public health issue and a leading preventable cause of adverse maternal and fetal outcomes. In France, midwives play a central role in antenatal care and are key actors in smoking cessation support. However, little is known about how smoking cessation is managed in routine maternity care and how organizational and professional factors shape these practices.
Objectives:
To explore midwives’ experiences in managing tobacco use during pregnancy, identify perceived barriers and facilitators in routine practice, and generate context-specific, practice-oriented recommendations to improve smoking cessation support within a maternity care setting.
Design:
A qualitative study using individual semi-structured interviews.
Methods:
Nine midwives working in a single French maternity unit participated in semi-structured interviews conducted between March and May 2023. Data were analyzed using a Framework analysis combining deductive coding informed by the capability, opportunity, and motivation-behavior (COM-B) model and the theoretical domains framework, with inductive refinement to capture emerging themes. Data saturation was assessed retrospectively. Reporting followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Results:
Midwives described heterogeneous practices in smoking cessation support and reported multiple barriers to optimal care. Three main challenges emerged: limited prioritization of smoking during consultations, insufficient knowledge and confidence in smoking cessation management, and organizational constraints, including lack of time, absence of structured care pathways, and limited coordination with addiction services. Engagement in smoking cessation discussions was often conditional on perceived patient motivation. These findings informed the development of practice-oriented recommendations targeting training needs, organizational improvements, and supportive tools within the maternity unit.
Conclusion:
This study highlights how individual capabilities, organizational opportunities, and motivational factors interact to shape smoking cessation support in routine maternity care. By adopting an implementation-focused perspective, it identifies modifiable levers to strengthen midwives’ capacity to address smoking during pregnancy. The recommendations proposed are exploratory and context-specific, intended to support local quality improvement initiatives rather than national guideline development.
Keywords
Introduction
Tobacco consumption during pregnancy remains a significant global health issue. 1 In Lange’s meta-analysis, the incidence of smoking during pregnancy was found to be 8.1% in Europe and 5.9% in the Americas, with a high proportion (72.5%) of pregnant smokers engaging in daily smoking. Notably, 30.6% of European women who are habitual smokers persist with this habit during pregnancy. 2 As of 2018, tobacco use among pregnant women in France has not decreased, contrasting with the declining trend observed in most other countries. 3 In France, 16.3% of women in their third trimester continue to smoke, ranking 20th among 22 surveyed countries in this regard. 4 Tobacco use is the primary preventable cause of pregnancy-related complications and mortality, increasing the risk of premature membrane rupture, placenta praevia, and intrauterine growth restriction. 5 A recent meta-analysis affirmed the impact of smoking on fetal growth retardation and reduced head circumference, with a clear dose–response relationship. 6 Therefore, it is crucial to proactively screen for and manage tobacco use among pregnant women.
To curb smoking during pregnancy, two primary types of interventions are employed: pharmacological and psychosocial approaches. 1 Focusing on psychosocial strategies, several interventions, such as counseling, health education, feedback, incentives, social support, and physical activity, effectively reduce the prevalence of smoking among pregnant women at the end of their pregnancy, as well as the incidence of low birth weight in newborns. 7 Additionally, despite limited evidence, the use of nicotine replacement therapy (NRT) may improve the likelihood of quitting smoking by the end of pregnancy. 8
The most recent French National Perinatal Survey (Enquête Nationale Périnatale, 2021) reported that 80% of women smoked before pregnancy and 46.3% continued to smoke during pregnancy. 3 In line with the 2014 guidelines of the French National Authority for Health, there is a recommendation for the implementation of continuous support interventions for smoking cessation throughout pregnancy. 9 Additionally, the French National College of Obstetricians and Gynaecologists (CNGOF) advocates for employing self-help and health education strategies to encourage quitting smoking during pregnancy. 10
Midwives, as integral members of the team providing care to pregnant women, play a pivotal role. Globally, they represent 10% of the workforce dedicated to sexual, reproductive, maternal, neonatal, and adolescent health and are crucial in delivering primary healthcare. 11 The World Health Organization recognizes midwives as essential in preventing and managing tobacco use during pregnancy. 12 They are equipped to assist pregnant women in quitting smoking through both psychosocial and pharmacological interventions. In France, since a law passed on 12 October 2005, midwives have been authorized to prescribe NRT to their patients. Furthermore, since 2016, this authorization has been extended to prescribing NRTs to the relatives of the pregnant woman or child during pregnancy and in the postnatal period.
The theoretical domains framework (TDF) is an established and comprehensive theoretical model encompassing various domains pertinent to professional practices and behavioral change. 13 Currently, there is a limited number of qualitative studies that thoroughly investigate these obstacles and identify factors that could enable midwives to more effectively address smoking during pregnancy.14–16 While previous qualitative studies have primarily examined individual beliefs or counseling attitudes, fewer have focused on how institutional organization, care pathways, and local resources shape midwives’ ability to implement smoking cessation support in routine maternity care. This study addresses this gap by adopting a practice-oriented perspective grounded in a single maternity unit, with the explicit aim of informing local guideline development.
This study aimed to explore midwives’ experiences in the management of tobacco use during pregnancy, with a specific focus on perceived barriers, facilitators, and organizational constraints encountered in routine clinical practice. Beyond describing practices and attitudes, the purpose of this qualitative research was to generate practice-oriented, context-specific recommendations to improve the organization and delivery of smoking cessation support within a maternity care setting.
Materials and methods
Study design
External independent researchers reviewed the study protocol before the collection of data began. These researchers provided methodological feedback on the interview guide and study design but were not involved in data collection or analysis. The research was conducted as a qualitative analysis using in-depth interviews. The analysis was directed by the COM-B model of behavior 17 and the TDF. 13 The COM-B model analyzes behavior by examining three elements: capability, opportunity, and motivation (COM), which collectively impact behavior (B). The COM-B model was used to structure the interpretation of barriers and facilitators at a conceptual level, while the TDF informed the identification of more specific behavioral and organizational determinants within each COM-B domain. The TDF includes 14 domains consisting of theoretical constructs that may affect behavior. The reporting of this study adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 18 The study was approved by the Foch IRB: IRB00012437 (approval number: 23-02-06) on 2 June 2023. Non-opposed consent was obtained from all participants.
Participants and recruitment
The participants of the current study were midwives working at the Foch hospital, a private not-for-profit hospital in France, realizing more than 3500 births per year, one of the largest maternity hospitals of Paris. Excluding the assisted reproductive technology unit, a total of 58 midwives work at the Mother–Child Unit of the Foch hospital. Sixteen midwives were offered an interview, while seven among them refused to be interviewed. Although the term “women” is used throughout the manuscript in reference to pregnancy, this terminology reflects the population included in this study and does not exclude gender-diverse individuals who may experience pregnancy.
Procedure
The research took place from March 1 to 5 May 2023, employing a qualitative methodology. To delve into the management of tobacco use during pregnancy at Foch Hospital, we opted to conduct semi-structured interviews with the midwives employed there. We considered interviews to be the most effective method for achieving this specific aim, as a questionnaire might have restricted the collection of pertinent information. Semi-structured interviews are advantageous because they facilitate an exploration of various viewpoints and the emergence of new themes, crucial for crafting tailored recommendations to enhance treatment for pregnant smokers.
These interviews were based on a pre-designed and tested semi-structured interview guide (Supplemental Table S1), covering several key topics:
Midwives’ perceptions of the factors that promote smoking during pregnancy.
The typical care process for pregnant women seeking to deliver at Foch Hospital.
How tobacco use is currently managed during pregnancy.
Midwives’ views on the primary shortcomings of the present tobacco management strategies during pregnancy.
Suggestions for enhancing tobacco use management during pregnancy at Foch Hospital.
Interviews were scheduled based on midwives’ availability and were only conducted with those who consented to participate in the study. If a midwife declined to participate, we requested their reason for refusal. The interview process continued until no new information was being generated (data saturation). Data saturation was assessed retrospectively using an iterative analytic process, whereby interviews were conducted and analyzed concurrently, and “saturation was considered achieved when no new codes or themes emerged in the final interviews, in accordance with established qualitative research guidance. 19 All interviews were then anonymized and subjected to transcription, coding, and thematic analysis.
Statistical analysis
Before the interview began, we ensured that verbal consent was captured digitally. The interviews were then transcribed word-for-word by MA. All interviews were conducted by MA, a trained midwife with clinical experience in maternity care and prior training in qualitative research methods. At the time of the study, MA was not hierarchically involved in the professional evaluation of participants. The interviewer was familiar with the clinical context but did not have a direct supervisory relationship with the interviewed midwives. This professional proximity facilitated rapport and openness during interviews. Reflexivity was addressed through regular discussions within the research team, during which potential influences of the interviewer’s professional background, and assumptions were considered during data analysis. Data were analyzed using a Framework analysis approach. An initial analytical framework was informed by the COM-B model and the TDF, 20 providing a deductive structure for coding. At the same time, the framework remained flexible and was iteratively refined to incorporate inductively generated codes emerging from participants’ narratives. This combined deductive–inductive approach allowed both theory-informed interpretation and openness to unanticipated themes. Once familiar with the transcripts, two researchers, MA and AV, independently coded the interviews. They established a provisional coding framework through consensus, which was refined after additional coding sessions and discussions. Coding was initially conducted independently by two researchers. Coding discrepancies were then discussed during regular analytical meetings and resolved through consensus, leading to iterative refinement of the coding framework and thematic matrices. The entire team engaged in discussions about the matrices to determine, label, and fine-tune the themes that most effectively interpreted the data. Each interview was thoroughly read multiple times and coded line by line, employing a broadly inductive thematic approach, facilitated by NVivo software (version 12). 21 Throughout the data gathering phase, field notes were maintained to document the researcher’s observations, opinions, and emotional responses, which were later considered during the thematic analysis.
Results
Data saturation was reached after conducting nine semi-structured interviews between March 1 and 5 May 2023 (Table 1). This was confirmed by the absence of new themes or codes during the analysis of the final interviews. The average approximate duration of the interviews was 40 min. All seven midwives who refused to be interviewed cited a lack of knowledge about the management of smoking during pregnancy. The analysis grid for the conducted semi-structured interviews can be found in the Supplemental Table S2.
Main characteristics of interviewed midwives.

First of all, the Mother–Child Unit of Foch Hospital asks pregnant women wishing to give birth at Foch Hospital to make an appointment for a registration consultation between 20 and 25 weeks of amenorrhea, which is primarily conducted by midwives (around the fifth month of pregnancy). As for the follow-up of pregnant women, it is mixed when the pregnancy is physiological – initially followed up by a private practitioner since the beginning of the pregnancy, and then exclusively at Foch Hospital from the eighth month onwards. If complications arise, the pregnancy becomes pathological and will therefore require close monitoring exclusively done by an obstetrician at Foch Hospital.
Furthermore, other optional services are offered to pregnant women such as the early prenatal interview (first trimester), antenatal diagnosis (first trimester), and all ultrasounds.
The prevalence of smoking during pregnancy was discussed. Indeed, four midwives reported a low prevalence of pregnant smoker women seen in consultation at Foch Hospital, while three others found there were considerably more. It is important to mention that only three midwives were aware of the recommendations of the HAS (French National Authority for Health) regarding the management of smoking during pregnancy. Four midwives among those who were not aware of these recommendations asked to be aware of them during the interview.
At Foch Hospital, all pregnant women are systematically asked about their tobacco use. However, there is no protocol describing the management and follow-up of a pregnant smoker. Therefore, each midwife acted differently and independently in managing smoking during pregnancy. According to six midwives, an informational booklet on the lifestyle to adopt during pregnancy, either digital or in paper format, could be offered to the woman who wished to be followed for her smoking. In this booklet, tobacco occupied a small paragraph. However, the pregnant smoker was free to accept or refuse it. On the other hand, three midwives stated that they systematically warned pregnant smokers about the risks of tobacco. For four midwives, the management of tobacco consumption depended on the desire and motivation of the pregnant smoker to quit smoking. Engagement in smoking cessation discussions was sometimes described as conditional on perceived patient motivation: “If she doesn’t really want to quit, I don’t insist” (Int1). Seven midwives stated that they offered the possibility of acupuncture and/or hypnosis sessions provided at Foch Hospital by their specialized midwife colleagues. Six midwives reported informing them of the possibility of using NRT. Only three midwives reported informing them of the possibility of consulting a private tobacco specialist. Thus, the observed differences in the management of pregnant smokers highlighted the lack of adherence to the recommendations of the HAS.
In light of the management of smoking during pregnancy as described by midwives, none found the management at Foch Hospital to be optimal for promoting maternal and fetal health. Three major limitations were identified: the lack of importance given to smoking, the lack of knowledge and professional skills in the management of smoking during pregnancy, and the lack of a defined organization for the care and follow-up of a pregnant smoker. Several midwives emphasized that smoking was not systematically prioritized during consultations, as illustrated by one participant: “When you open a file, tobacco has no more chapters than domestic violence or economic concerns” (Int8). Others explicitly reported a lack of skills and confidence, stating: “I think we don’t do it simply because we don’t know how to do it” (Int7). A selection of the most illustrative verbatim quotes is presented in Table 2.
Selection of the most illustrative verbatim concerning the main limitations of the current care of pregnant smokers at Foch Hospital.

Beyond describing reported practices, the findings also reflect midwives’ underlying perceptions, beliefs, and motivational processes regarding smoking cessation during pregnancy, particularly in relation to their perceived role, confidence, and ability to act.
Indeed, only two midwives reported giving importance to smoking by reiterating the risks of tobacco to pregnant smokers whenever they saw the note “tobacco (+)” on the sleeve of their file. Almost all midwives (n = 9) reported a lack of knowledge and professional skills in managing smoking during pregnancy, with five not being aware of the HAS’s recommendations. This lack of confidence was explicitly expressed by participants, for example: “I feel like I’m going to do anything that’s bad! I don’t even know what it’s called, and since these are not things we do on a daily basis, well in fact I admit that I’m a bit dumped” (Int7). This reflects uncertainty regarding both professional role and clinical competence in smoking cessation support. As for the lack of a defined organization for the care and follow-up of a pregnant smoker, several aspects were identified, with the main ones being: the absence of defined management and follow-up for smoking during pregnancy, lack of time, the current absence of tobacco counseling sessions, not having the same healthcare professional at each consultation, lack of communication with the addiction care team (ACT) of Foch Hospital, and the late-stage pregnancy follow-up at the Mother–Child Unit.
Lack of time was identified as the main limitation by seven midwives interviewed. Moreover, according to five midwives, the discontinuation of tobacco counseling sessions, previously provided to pregnant smokers, was no longer conducive to good management of smoking during pregnancy following the departure of the only specialized midwife in tobacco cessation. Time constraints were described as a major barrier, as one midwife explained: “When the woman tells you ‘I smoke and I want to quit,’ and you only have 30 minutes, you can’t start a motivational interview” (Int5). This highlights how organizational context limits opportunities for smoking cessation counseling in routine care. Similarly, not having the same healthcare professional at each consultation (n = 6), lack of communication with the ACT at Foch Hospital (n = 6), and the late-stage pregnancy follow-up at the Mother–Child Unit (n = 3) were seen as obstacles to the optimal management of pregnant smokers.
After identifying the aforementioned limitations, several recommendations were made by midwives, including the opening of targeted sessions on smoking during pregnancy within the Mother–Child Unit, offering an optional training in tobaccology/addictionology for interested midwives, providing pregnant smokers with an advice sheet/brochure/booklet regardless of their level of smoking, and the implementation of a “reminder” sheet for midwives detailing the typical care pathway of a pregnant smoker in order to better assist and guide them.
Indeed, the limitations of the current management of tobacco smoking and the possible solutions according to midwives, the following set of recommendations has been developed for a better management and adequate follow-up of pregnant women who smoke (Table 3 and Figure 1).
Set of recommendations aimed at enhancing the management of tobacco use throughout pregnancy.

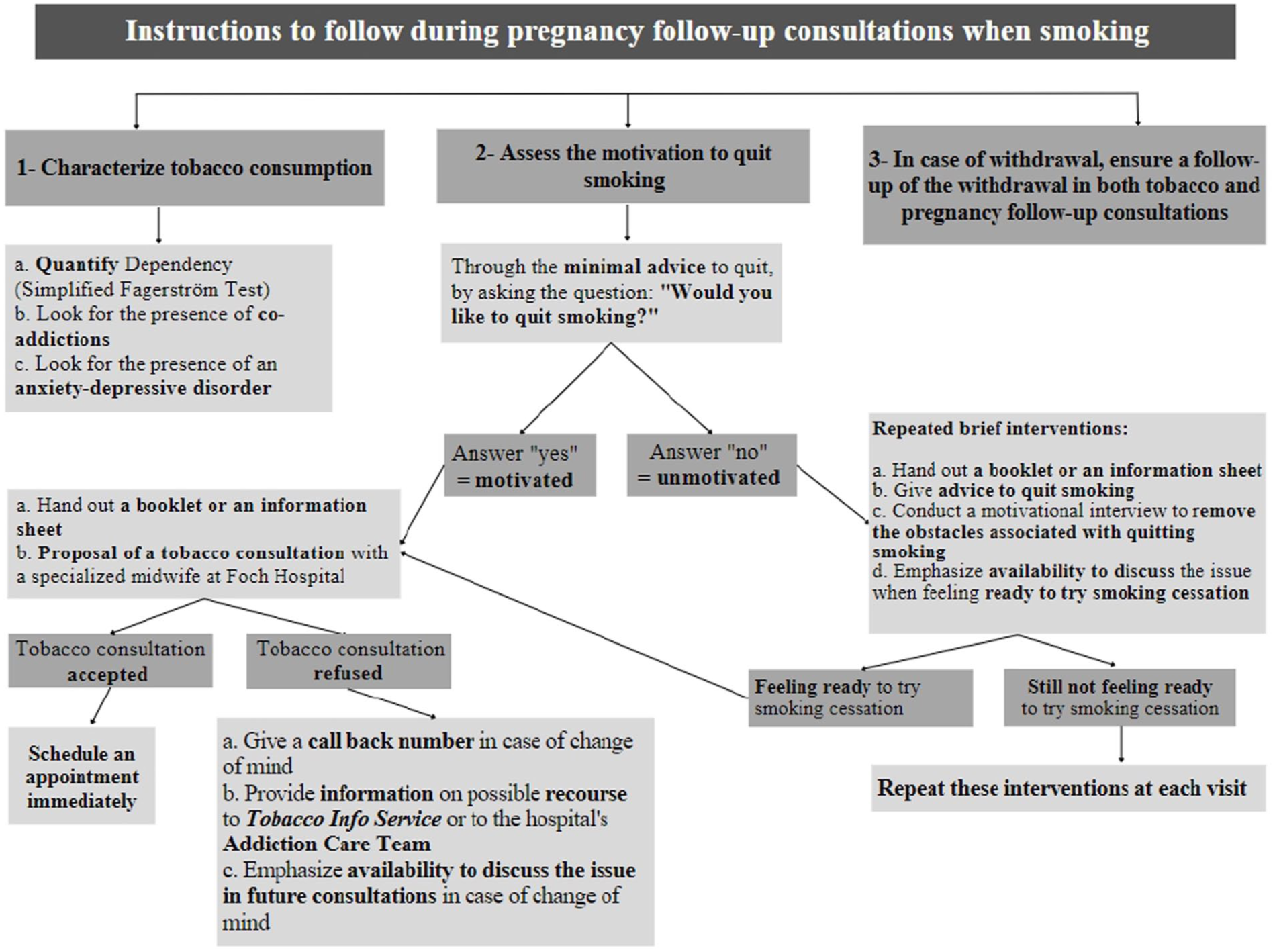
Proposal of a flowchart outlining the instructions to be followed by midwives during pregnancy follow-up consultations when pregnant women report smoking.
Discussion
This qualitative study was designed with a practice-oriented perspective, aiming not only to describe midwives’ experiences but also to inform the development of context-specific recommendations to improve smoking cessation support during pregnancy. Rather than seeking theoretical generalization, our findings highlight how individual skills, organizational constraints, and care pathways interact in a real-world maternity setting to shape the implementation of national recommendations. By grounding the analysis in routine clinical practice within a single Mother–Child Unit, this study provides actionable insights into modifiable levers at the local level, including training needs, organizational structures, and coordination with addiction care services. The COM-B model and the TDF were used as analytical lenses to structure the interpretation of barriers and facilitators, thereby supporting the translation of qualitative findings into practical recommendations (Supplemental Table S4).
In this qualitative research involving French midwives, the participants highlighted their emphasis on educating about the dangers of smoking, while acknowledging a deficit in practical communication skills. Their understanding, although consistent with the current HAS’s guidelines, is not up-to-date. Additionally, several midwives face multiple obstacles, including time constraints, patients’ past negative experiences with NRT, and concerns about its safety.
Interpreted through the COM-B framework, our findings suggest that several modifiable levers may support improved implementation of smoking cessation support during pregnancy. 17 First, the limited knowledge of national recommendations and low confidence in prescribing NRT primarily reflect gaps in capability, supporting the need for targeted training and practical workshops for midwives. 13 Second, organizational barriers such as time constraints, lack of continuity of care, and limited coordination with addiction services point to restricted opportunity, highlighting the importance of structured care pathways, dedicated smoking cessation consultations, and improved interprofessional communication.22,23 Third, variability in engagement with smoking cessation discussions, often conditional on perceived patient motivation, relates to motivation and underscores the value of brief, repeated interventions and supportive tools designed to facilitate non-judgmental dialogue. Together, these elements illustrate how aligning training, organizational change, and supportive resources may address complementary COM-B domains and enhance the feasibility of smoking cessation support in routine maternity care. 24 To enhance transparency, a mapping between key empirical findings, COM-B/TDF domains, and corresponding recommendations is provided in the Supplemental Table S3.
Our findings align with and extend recent research on professional socialization and smoking cessation support in healthcare training contexts. For example, a recent study in France found that midwifery students were less likely than medical students to intend to discuss smoking with their patients, an effect attributed to differences in professional socialization and role expectations. 25 This resonates with our results, where some midwives described hesitation or low confidence in addressing smoking, suggesting that professional norms and training pathways influence how smoking cessation is prioritized in routine care. Beyond individual attitudes, our data highlight how organizational constraints and care pathways further shape these professional behaviors. Taken together, this literature and our findings underscore the importance of addressing both socialization processes in health professions education and structural supports in clinical settings to enhance consistent smoking cessation engagement.
Echoing the findings of this study, a recent systematic review that consolidated data from eight qualitative studies in high-income countries underscored the necessity for healthcare providers to improve their approach in discussing smoking. This improvement aims to ensure that such conversations do not harm their relation with female patients. 15 Furthermore, healthcare providers acknowledged the importance of addressing smoking cessation support beyond the healthcare setting, recognizing its relevance in the wider social environment. 15
Our study similarly reflects a gap in knowledge and practice, evidenced by the minimal use of tools by French midwives to address smoking during pregnancy. This underutilization was corroborated by patients, as 53% reported not receiving any information on the benefits of quitting smoking, and 77% did not receive an informational brochure. 26 Additionally, another study found that 62% of gynecologists and 79% of midwives never offered smoking cessation support. 27 Effective tools for smoking cessation include explaining the health risks of smoking for both the mother and child, highlighting the benefits of quitting at any stage during pregnancy, and setting a quit date. The communication of these messages should be clear and non-judgmental to avoid guilt or hostility. 28 Therefore, it is crucial to enhance the knowledge and skills of professionals, including midwives, who interact with pregnant women, enabling them to identify and address tobacco use early in pregnancy. Bryce et al. also suggest the implementation of a smoking cessation program for healthcare professionals during pregnancy, 28 which would involve “training, advice, and protocols for providing information, consistent advice, and support to pregnant women.” Such a program, currently absent in France, could be introduced to French midwives through specialist tobacco units.
Nearly all French midwives knew about their ability to prescribe NRT. Despite this prescribing right being available in France since 2016, only about one-third of the surveyed midwives realized they could prescribe NRT to those in the pregnant woman’s support circle during pregnancy, as well as to those in the child’s network during postnatal care. Furthermore, the primary challenge encountered by French midwives (65%) in assisting pregnant women to quit smoking was identified as the lack of motivation in the patients.1,29
Healthcare professionals, such as midwives, play a major role in advising and supporting women in the face of unhealthy behaviors. Therefore, it is recommended to act as early as possible during pregnancy. 30 The educational program for patients (EPPs) should be a focal point for establishing a personalized trust relationship, allowing, if necessary, the referral of pregnant smokers to other professionals in the network.31,32 Early intervention by a multidisciplinary and multi-professional team, working in collaboration with perinatal and addiction networks, seems crucial. 33 The coordination between addiction structures, psychiatric services, perinatal networks, and city–hospital networks is essential for the coordination of perinatal and addiction care. 34 Indeed, obstetricians, general practitioners, midwives, tobacco specialists, addiction specialists, psychiatrists, psychologists, and social workers must intervene, gradually and at the right time, in a coordinated and differentiated care approach. However, professionals must be vigilant regarding the quality and proper nature of intra- and inter-institutional transmissions, as well as the continuity of care.15,30,35
Interviews with midwives reveal disparities in care and their expectations. Indeed, the diversity of their statements is generally the result of experience acquired by the midwife. 36 Knowledge gained in the field is an evolving experiential knowledge over the course of a career, thus providing ease, special interest, and facilitating discussions with patients, especially on difficult topics. 37 However, healthcare professionals should always communicate relevant information based on literature in a context of constantly evolving knowledge.14,15,24 Therefore, it is crucial for healthcare professionals to train in the modalities of smoking cessation management during pregnancy and to continuously update their knowledge and professional skills.
The interactions during a pregnancy are generally conducted by midwives and have been reinforced over time (EPP, prenatal prevention check-up, etc.). Unfortunately, the time dedicated to consultations, particularly for prevention messages, is getting shorter.38,39 It is therefore essential to optimize this time through clear and precise booklets and prevention messages. 37 The midwives interviewed reported using very few paper and computer supports, despite the significant existence of institutional materials. However, all professionals interviewed agreed on the importance of such information supports and wished to rely on such documents to improve their clinical practice. It thus seems essential to meet this need by co-constructing supports adapted to the needs and scientifically validated, with the aim of improving understanding and appropriation of information by the involved teams. This co-construction approach of a guide/booklet by the teams would improve the adoption of the smoking cessation prevention discourse and would consequently increase the level of knowledge of pregnant women who received this information. 40
Importantly, the recommendations proposed are not intended as national-level guidelines, but as locally applicable, practice-oriented proposals derived from a single maternity unit and should therefore be interpreted with caution beyond similar contexts. This study did not aim to follow the full Behavior Change Wheel intervention development process, but rather to use COM-B and TDF as interpretative frameworks to support exploratory, locally applicable recommendations.
Limitations
This study has several limitations that should be acknowledged. First, it was conducted in a single maternity hospital, and the findings reflect the organizational context and professional practices of one Mother–Child Unit. As such, the results are not intended to be statistically generalizable to all maternity settings in France. Rather, the aim was to provide an in-depth, context-specific understanding of routine practices and organizational constraints, with a view to informing local practice improvement. Second, participation was voluntary, and several midwives declined to be interviewed due to a self-reported lack of knowledge regarding smoking cessation during pregnancy. This may have introduced a selection bias, whereby the perspectives captured predominantly reflect midwives who were already sensitized or interested in the topic. However, this finding highlights an important structural issue, namely, gaps in training and confidence, which is consistent with the themes identified in the interviews and reinforces the relevance of the recommendations proposed. Third, as with all qualitative research based on self-reported data, the possibility of social desirability bias cannot be excluded, particularly given that the interviewer was also a midwife. To mitigate this risk, interviews were conducted in a non-judgmental manner, anonymized, and analyzed independently by two researchers using an established analytical framework. Finally, while the COM-B model and the TDF informed the analytical approach, these frameworks were used as interpretative lenses rather than as prescriptive intervention-development tools. Consequently, the recommendations derived from this study should be viewed as exploratory and practice-oriented, intended to support local implementation and hypothesis generation rather than to serve as national-level guidelines.
Conclusion
This qualitative study provides a practice-oriented insight into how midwives experience and manage smoking cessation during pregnancy within a maternity care setting. Rather than highlighting a lack of willingness, our findings underscore the combined influence of limited training, organizational constraints, and fragmented care pathways on the implementation of smoking cessation support in routine practice. By adopting an implementation-focused perspective informed by the COM-B framework, this study identifies concrete, modifiable levers at the local level, including strengthening midwives’ capabilities through targeted training, improving organizational opportunities via structured care pathways, and supporting motivation through practical tools that facilitate repeated, non-judgmental discussions with pregnant women. The recommendations proposed should be viewed as exploratory and context-specific, intended to support local quality improvement initiatives rather than to serve as national guidelines. Future research could extend this work by incorporating the perspectives of other healthcare professionals involved in antenatal care, as well as pregnant women themselves, to further inform the design and evaluation of scalable smoking cessation interventions during pregnancy.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261427550 – Supplemental material for Management of tobacco smoking among pregnant women: A qualitative study with French midwives to inform local practice recommendations
Supplemental material, sj-docx-1-whe-10.1177_17455057261427550 for Management of tobacco smoking among pregnant women: A qualitative study with French midwives to inform local practice recommendations by Marianne Alhage, Maxence Arutkin, Pierre-François Ceccaldi, Loïc Josseran, Jean-Marc Ayoubi and Alexandre Vallée in Women's Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057261427550 – Supplemental material for Management of tobacco smoking among pregnant women: A qualitative study with French midwives to inform local practice recommendations
Supplemental material, sj-pdf-2-whe-10.1177_17455057261427550 for Management of tobacco smoking among pregnant women: A qualitative study with French midwives to inform local practice recommendations by Marianne Alhage, Maxence Arutkin, Pierre-François Ceccaldi, Loïc Josseran, Jean-Marc Ayoubi and Alexandre Vallée in Women's Health
Footnotes
Acknowledgements
None.
Ethical considerations
The study was approved by the Foch IRB: IRB00012437 (approval number: 23-02-06) on 2 June 2023. Non-opposed consent was obtained from all participants. In accordance with French regulations for non-interventional qualitative research, a non-opposed consent procedure was used. Participants received written information about the study objectives, procedures, and their rights, including the right to refuse participation or withdraw at any time. Verbal consent was obtained prior to each interview.
Consent to participate
Consent was considered implied when participants agreed to take part in the interview and did not express any opposition.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.