
Abstract
Background:
Uninsured, low-income Spanish-speaking women face systemic barriers to accessing gynecologic care, especially within Fort Worth, Texas. Because of this health disparity, we elected to evaluate screening outcomes of patients receiving care at La Clínica de las Mujeres (LCDM), a student-run clinic (SRC) providing free, culturally competent care to this population in Fort Worth, Texas.
Objectives:
To assess the structure and utilization of an SRC on cancer screening adherence among uninsured, Spanish-speaking women in Fort Worth, Texas.
Design:
Retrospective descriptive pre-post study.
Methods:
Chart review of patients seen at LCDM from August 2022 to September 2024 was conducted. Data included 147 clinical encounters with 114 individual patients, assessing demographics, screening history, services, and referrals. McNemar’s test assessed changes in screening adherence.
Results:
Patients (mean age: 47.5 years; 95.6% Hispanic) primarily resided in underserved zip codes (77.2% in 76110). Pre-intervention, 46% adhered to Pap smear guidelines and 64% to mammography guidelines. Post-intervention adherence approaches complete compliance among those with available post-intervention data (Pap χ²[1] = 66.0, p < 0.0001; Mammogram χ²[1] = 27.0, p < 0.0001). Services included pelvic ultrasounds (n = 20), specialist referrals (n = 11), and contraceptive access (n = 12).
Conclusions:
LCDM was associated with significant improvements in gynecologic preventive care adherence for uninsured Spanish-speaking populations in Fort Worth, Texas. Student-run models may help address critical gaps in accessibility to women’s health services and mitigate systemic barriers to care for underserved populations.
Introduction
Uninsured, low-income, Spanish-speaking women face significant barriers to accessing gynecologic care due to factors such as ethnicity, immigration status, language barriers, and social determinants of health.1,2 Cultural norms, including embarrassment and fear about health and cancer, as well as limited English proficiency and inadequate health literacy in Spanish, have been associated with poorer understanding of screening recommendations and lower uptake of cervical cancer screening, even when services are available in Spanish.3,4 In addition, undocumented women report significantly more obstacles to screening and lower knowledge of preventive services compared with documented women. 5 These barriers contribute to disparities in preventive care utilization and poorer health outcomes among this population. Student-run clinics (SRCs) have emerged as an important resource to address these disparities by providing care to underserved populations throughout the United States.6 –8
La Clínica de las Mujeres (LCDM) is a monthly, student-run gynecology clinic in Fort Worth, Texas, which provides free care to uninsured Spanish-speaking women under the supervision of licensed physicians. The clinic utilizes Community-Based Participatory Research (CBPR) principles to ensure culturally relevant care by involving Spanish-speaking community members in its development and implementation. 9 Evidence shows that CBPR can lead to sustainable health interventions that are more effective and culturally appropriate for underserved populations. 10
SRCs have been shown to improve access to preventive care, health outcomes, and patient satisfaction while providing valuable experiential medical education for students.7,8 A systematic review by Xiao et al. found that SRCs can significantly increase breast and cervical cancer screening rates among underserved populations. 6 Additionally, Simpson and Long highlighted the importance of these clinics as contributors to both patient care and medical education.8,11 This underscores the potential of SRCs to address critical preventive care needs in underserved populations and supports the importance of initiatives like this study in evaluating and improving women’s health services in these settings. In addition, language-concordant care, where providers and patients share the same primary language, has been associated with improved patient satisfaction, adherence to treatment plans, and overall health outcomes. 12 This is particularly relevant for the growing Hispanic population in Texas and other parts of the United States.
However, there is limited research specifically focused on SRCs that target Spanish-speaking women in Texas and limited research on patient’s satisfaction with SRCs. 2 By focusing on a population that faces multiple barriers to care, our study provides insights into effective strategies for reducing health disparities through community engagement and thereby improving access to culturally competent care of the underserved and uninsured women of our community. The primary objective of this study is to evaluate the association between care at LCDM and adherence to gynecologic cancer screening guidelines among uninsured, Spanish-speaking women in Fort Worth, Texas.
Introduction to Mercy Clinic and LCDM
Mercy Clinic is located in Fort Worth, Texas, serving uninsured adults in zip codes 76110, 76104, and 76115. Patients qualify based on household incomes not exceeding 200% of the federal poverty level, which is defined as no income greater than $31,300 for a single individual or $64,300 for a family of 4 based on the 2025 guidelines. 13 Mercy Clinic provides a range of services, including preventive care, acute care, and chronic disease management. LCDM is a specialized women’s health service within Mercy Clinic, which is an SRC supervised by volunteer physicians that provides gynecologic healthcare to uninsured women residing in the delineated zip codes. Services at LCDM are made possible through the generous donation of time, expertise, and materials from dedicated volunteer providers, as well as ongoing support and resources from Mercy Clinic.
Operational structure of LCDM
LCDM functions as an ancillary clinic that operates on the first Saturday of each month, with patients referred from Mercy Clinic’s primary care services. Two upper-level (third or fourth year) medical students oversee clinic operations, including scheduling volunteer providers and student teams. On clinic days, one to three volunteer providers are present alongside student volunteers organized into multiple teams consisting of one upper-level student and one or two lower-level students. At least one student must demonstrate Spanish proficiency to serve as an interpreter during visits.
Upper-level students, under the guidance of an experienced, supervising volunteer physician, conduct patient interviews, perform exams, and perform minor procedures such as Pap smears. The supervising volunteer physician provides real-time feedback during examinations to ensure safe and effective patient care. Sensitive procedures requiring additional expertise (e.g., polypectomy, endometrial biopsy, Intrauterine Device insertion, etc.) are performed by the physician.
Administrative tasks such as patient reminders, result follow-ups, imaging coordination, and specialist referrals are managed by Mercy Clinic staff and clinic managers. For abnormal findings, overseeing students collaborate with supervising volunteer providers and clinic managers to develop appropriate care plans. Positive screening results for cervical or breast cancer are referred to the Moncrief Cancer Center through a pre-established partnership for underserved patients. For cases requiring additional specialist care beyond Mercy Clinic’s capabilities, referrals are made to Project Access Tarrant County—a healthcare initiative supported by the Tarrant County Medical Society that connects uninsured patients with a network of volunteer providers.
On average, LCDM sees about 10 patients per clinic session—4 presenting with gynecologic complaints and the remainder for general well-woman exams. Gynecologic visits often involve complex or prolonged procedures such as polypectomy, endometrial biopsy, or IUD insertions. Each clinic session at LCDM begins with a didactic lecture led by a volunteer supervising physician for student volunteers, focusing on common gynecologic conditions or other relevant health topics. These sessions are tailored to address the types of gynecologic concerns identified in the patient list for that day, ensuring that both students and providers are prepared to deliver informed, patient-centered care.
Methods
This study was a retrospective descriptive pre–post analysis . All patient data were handled in compliance with Health Insurance Portability and Accountability Act (HIPAA) regulations. Eligible participants included non-pregnant females aged 18–99 years who attended LCDM for a minimum of one visit between August 2022 and September 2024, resided in zip codes 76110, 76115, or 76104 as it is an eligibility requirement to be seen at Mercy Clinic, and had a household income at or below 200% of the national poverty level; individuals with household incomes exceeding this threshold were excluded. A comprehensive chart review was performed for all patients meeting criteria, and data collected from medical record documentation included patient demographics, number of encounters, chief complaints, history of cervical and breast cancer screening, gynecologic services provided (such as Pap smears, pelvic exams, and contraceptive counseling), and specialist referrals. To ensure accuracy and consistency, data were systematically abstracted from electronic medical records using a standardized data abstraction tool developed by the research team. Descriptive statistics were used to summarize all demographic and clinical variables. Continuous variables, such as age, were reported as means with standard deviations, while categorical variables were presented as frequencies and percentages. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 14
Statistical analysis
To evaluate changes in adherence to cervical and breast cancer screening guidelines following establishment of care at LCDM, we conducted a paired analysis comparing screening status before and after clinic enrollment. Pre-intervention adherence was defined as screening status documented prior to the initial LCDM visit. Post-intervention adherence was defined as screening status documented at or immediately following the index clinic visit, based on results of tests ordered and completed through LCDM. Only patients with complete paired pre- and post-intervention screening data were included in McNemar’s test analyses. For Pap smear adherence, 114 patients contributed paired data. For mammogram adherence, 78 age-eligible patients contributed paired data.
Adherence was defined according to the American College of Obstetricians and Gynecologists (ACOG) guidelines for Pap smears and mammograms based on patient age and screening interval. Because the data represented paired binary outcomes (i.e., adherent vs. non-adherent) for the same individuals at two time points, McNemar’s test was used to assess whether the observed changes in adherence were statistically significant, with results reported as χ² test statistics with 1° of freedom. The level of statistical significance for this analysis was alpha = 0.05. Analyses of screening adherence were restricted to patients with both pre- and post-intervention screening information available. Missing data were handled using listwise deletion. Patients with incomplete information for a given variable were excluded from that specific analysis but remained eligible for other analyses if their data were available. Of the 147 total clinic encounters, 114 unique patients had complete paired adherence data for cervical cancer screening and were included in the Pap smear analysis. For breast cancer screening, 78 patients met age eligibility criteria for mammography and had complete paired pre- and post-intervention data. No imputation was performed, as there were no missing adherence data for the paired analyses.
Results
Over 25 months, LCDM saw 114 unique patients across 15 clinic sessions, resulting in a total of 147 clinical encounters. During this period, 36 medical students and 9 providers volunteered their time. On average, patients attended 1.3 visits during this timeframe.
Patient demographics are summarized in Table 1. The mean age of patients was 47.5 years, with ages ranging from 21 to 72 years. Nearly all patients (95.6%) identified as Hispanic, while the remaining 4.4% identified as Asian. A majority (93.8%) reported Spanish as their primary language.
Summary of demographic characteristics for patients seen at LCDM.

LCDM: La Clínica de las Mujeres; SD: standard deviation.
Gynecologic needs and services
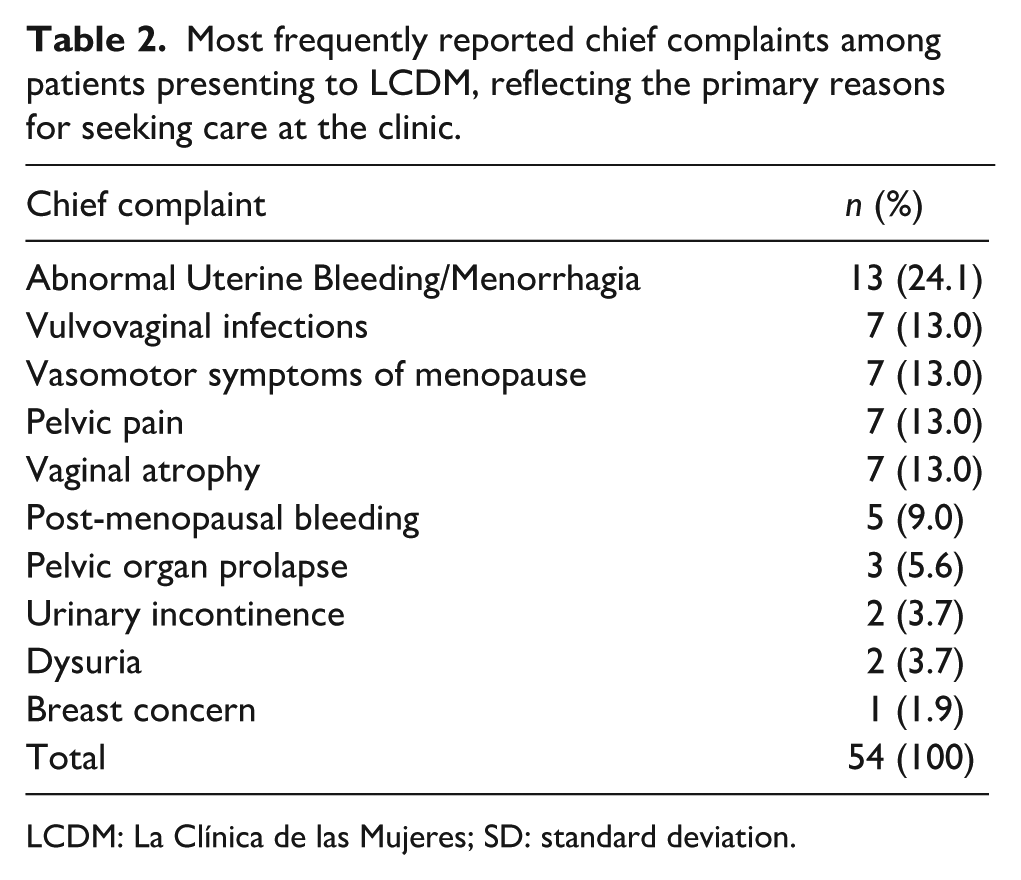
The numbers of gynecologic complaints addressed in clinical encounters are presented in Table 2. Most common chief complaints included Menorrhagia/Abnormal Uterine Bleeding (24.1%), vulvovaginal infections (13.0%), pelvic pain (13.0%), atrophic vaginitis (13.0%), vasomotor symptoms of menopause (13.0%), post-menopausal bleeding (9.0%), pelvic organ prolapse (5.6%), urinary incontinence (3.7%), dysuria (3.7%), and breast concerns (1.9%). The numbers of procedures and laboratory tests performed, and specialist referrals are shown in Table 3. Of note, LCDM providers performed 102 Pap smears, 3 endometrial biopsies, and 3 cervical polypectomies, all of which were sent for pathologic analysis. Regarding specialist referrals, five patients were referred to Moncrief Cancer Center for abnormal screening Pap smears and/or mammogram results. Eleven patients were referred to Project Access Tarrant County for indications including pelvic organ prolapse, menorrhagia, sleep apnea, umbilical hernia, and dermatologic concerns.
Most frequently reported chief complaints among patients presenting to LCDM, reflecting the primary reasons for seeking care at the clinic.
LCDM: La Clínica de las Mujeres; SD: standard deviation.
Common interventions/referrals.

LCDM: La Clínica de las Mujeres; SD: standard deviation.
Gynecologic outcomes and adherence to screening guidelines
Prior to establishing care with LCDM, only 46% of patients were adherent to ACOG cervical cancer screening recommendations (53/114; 95% CI: 37%–55%; Table 4). Of the remaining patients, 32% were within 4–5 years since their last Pap smear, 8.7% were within 6–10 years, 5.2% were within 11–15 years, and 7% were within 16–20 years (Figure 1). For mammograms, 64% were adherent to ACOG mammogram guidelines for age-eligible women prior to being seen in the clinic (49/78; 95% CI: 53%–74%; Table 4). Of the remaining patients, 21% were within 3–5 years since their last mammogram, 1.3% were within 6–10 years, 3.9% were within 11–20 years, and 11.7% had never had a screening mammogram (Figure 1).
Paired pre–post screening adherence status.

CI: confidence interval.

Time since last cervical and breast cancer screening among patients establishing care at La Clínica de las Mujeres.
Finally, patients demonstrated a statistically significant improvement in adherence to ACOG-recommended screening guidelines for both Pap smears (χ²[1] = 66.0, p < 0.0001) and mammograms (χ²[1] = 27.0, p < 0.0001) between pre- and post-clinic measurements (Figure 2).
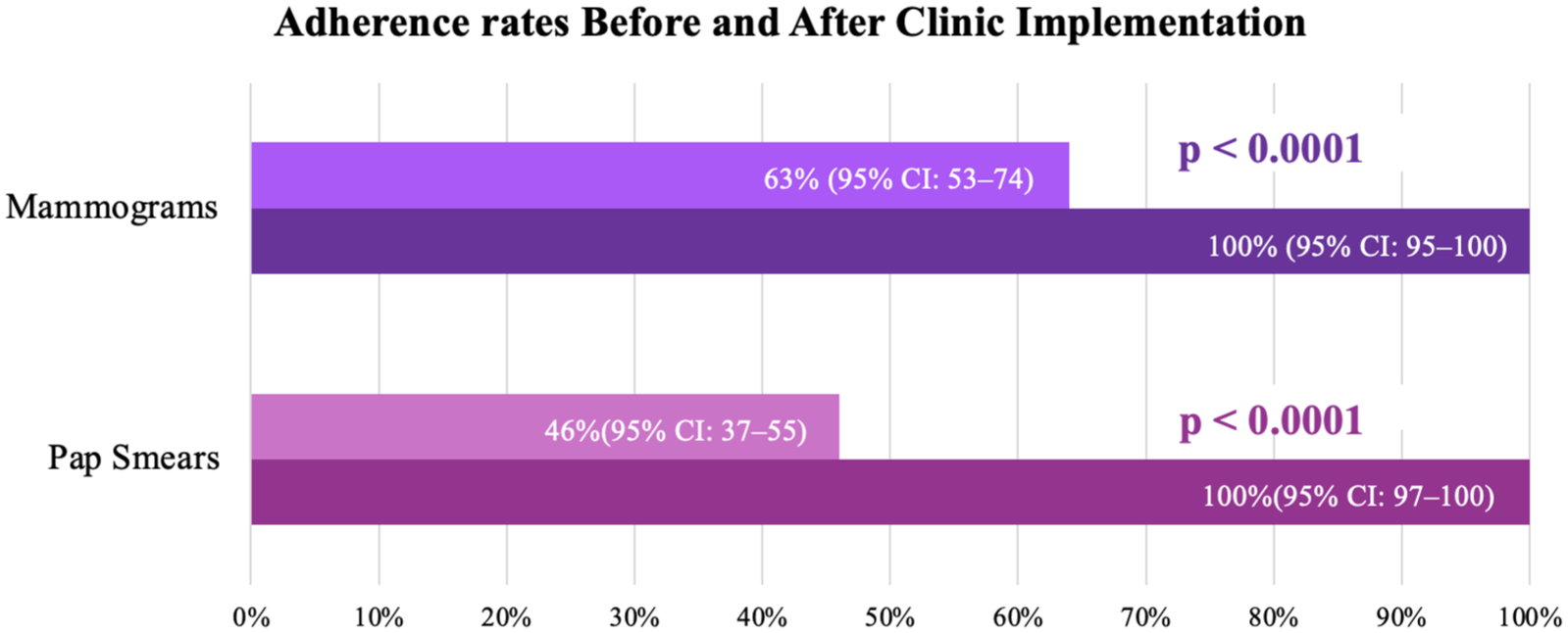
Adherence rates to Pap smears and mammogram before and after implementation of La Clinica de las Mujeres.
Discussion
The findings from LCDM illustrate the potential for student-run free clinics in addressing healthcare disparities among underserved populations, particularly among uninsured, Spanish-speaking women. Prior to the institution of this clinic, the healthcare provided to this particular population in the Fort Worth community was discontinuous, incomplete, and fell short of providing them with appropriate, comprehensive medical care.
LCDM provides additional opportunities for patients to access preventive and specialized care, addressing a wide range of gynecologic complaints and facilitating necessary referrals for advanced interventions if required. The improvement in adherence to both cervical cancer and breast cancer screening observed in this study suggests that care at LCDM may help address gaps in preventive care among uninsured, Spanish-speaking women. Prior to establishing care, a substantial proportion of patients were overdue for routine cancer screenings. Following clinic enrollment, improved adherence to ACOG guidelines for both cervical and breast cancer screening was demonstrated among those with available post-intervention data. These adherence patterns are consistent with a potential beneficial role for targeted interventions such as LCDM and support the hypothesis that such clinics may help reduce disparities in cancer screening within underserved populations. In addition, these results show the importance of integrating culturally competent care and language accessibility into clinic operations, which may have contributed to the observed outcomes.
Furthermore, LCDM serves as a model for leveraging student-driven initiatives to expand healthcare access while simultaneously providing additional low-resource clinical exposure for medical students. The involvement of medical students and volunteer providers not only addressed immediate patient needs but also fostered a deeper understanding of the social determinants of health among trainees. This dual benefit—improving patient care while cultivating future healthcare leaders—highlights the potential for SRCs to contribute to both public health and medical education. As demonstrated in other SRCs across the United States, such initiatives can inspire long-term commitments to serving underserved communities and addressing systemic inequities in healthcare delivery.7,8,11
Limitations
This study has several limitations, including its retrospective design and short observation period, which limits the ability to assess long-term outcomes, and the small sample size, which may affect generalizability and precision. There also may be selection bias related to systematic differences between patients who attend free clinics and those who do not. Additionally, operational challenges during the early stages of the clinic’s establishment may have influenced the data collected. Language barriers and cultural differences, while mitigated by Spanish-speaking volunteers, may still have impacted patient communication and care delivery. Resource constraints inherent to SRCs may limit the scope and frequency of services provided.
Finally, as a descriptive, observational study, our analysis cannot fully control for unobserved variables that may influence outcomes (e.g., changes in patient motivation, external healthcare access, secular trends, or broader community health initiatives). In addition, this study lacked a comparison group and used a descriptive pre–post design, causal inference regarding the clinic’s effect on screening adherence is limited. Thus, our findings should be interpreted as associations rather than evidence of direct causation.
To build on the success of LCDM, Mercy Clinic and other student-led clinics in Fort Worth could consider expanding specialty services tailored to underserved populations. By establishing additional SRC focused on high-demand areas such as dermatology, cardiology, and mental health, these clinics could address critical gaps in healthcare and provide comprehensive care to the community.
Conclusion
This study found that care at an SRC was associated with improved access to gynecologic care and higher adherence to screening guidelines among uninsured, Spanish-speaking women, suggesting a potential role for such clinics in addressing critical healthcare gaps and reducing health disparities within this underserved population. By facilitating preventive care such as cervical and breast cancer screening, the clinic may contribute to improved health outcomes over time. Furthermore, this study underscores the potential of SRCs to address unmet healthcare needs while fostering future healthcare providers’ commitment to serving marginalized communities. Altogether, it exemplifies how SRCs may promote health equity and enhance access to care, providing a model for future initiatives aimed at reducing healthcare disparities.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261424823 – Supplemental material for Structure, utilization, and screening adherence of a student-run women’s health clinic for uninsured Spanish-speaking women: A descriptive analysis
Supplemental material, sj-pdf-1-whe-10.1177_17455057261424823 for Structure, utilization, and screening adherence of a student-run women’s health clinic for uninsured Spanish-speaking women: A descriptive analysis by Alicia M. Faszholz, Vanessa Lozano and Jacqueline Garda in Women's Health
Footnotes
Acknowledgements
The editorial assistance of Gregory L. Kearns, PharmD, PhD, FAAP is gratefully acknowledged as is the support received from the Anne Burnett Marion School of Medicine at Texas Christian University and the Baylor Scott and White All Saints Medical Center in Fort Worth, TX.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board at Texas Christian University (#2024-282) on October 21, 2024.
Consent to participate
The need for written informed consent was waived.
Consent for publication
Consent for publication of patient data was not required as the study used de-identified, retrospective data with no patient images or individually identifiable information. The IRB waived the need for written consent in accordance with institutional and national guidelines.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset supporting the findings of this study is available from the corresponding author upon reasonable request and with permission from the relevant clinical institutions where the data were collected.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.