
Abstract
Background:
Diaper insecurity, unmet need for infant/child diapers, is a form of material deprivation associated with worse maternal mental health, including higher levels of stress, anxiety, and depression.
Objectives:
To examine retrospective reports of mothers’ experiences of diaper insecurity and coping strategies as they related to maternal physical and mental health, health behaviors, and social interaction.
Design:
This study used semi-structured, in-depth interviews with 70 mothers who lacked enough diapers. A thematic analysis using abductive coding was conducted to identify related factors connecting diaper insecurity and mothers’ health outcomes.
Methods:
Mothers who self-identified as experiencing diaper insecurity were interviewed about reasons they struggled to access diapers, coping strategies, and perceived effects on their financial situations, social relationships, and well-being.
Results:
Qualitative analysis identified three themes centered around mothers’ experiences of diaper insecurity: (1) common ways of managing diaper insecurity, such as missing work, school, or medical appointments and having to forgo other basic needs, shopping, and socializing, which can mean less income, less access to health care, and fewer social interactions; (2) additional physical, cognitive, and emotional labor associated with managing diaper insecurity that contributes to worse physical and mental health; and (3) maternal shame associated with an inability to provide a basic need of early childcare and fear of stigma that hinders parental self-efficacy and sense of self-control.
Conclusion:
Beyond its association with other factors, including low income and social isolation, known to negatively affect psychological well-being, lack of access to enough diapers may contribute to maternal stress, anxiety, and depression. Interviews with mothers revealed the mental, physical, and social toll of diaper insecurity and point to public diaper support as a possible pathway for supporting women’s health.
Keywords
Introduction
Four in 10 children in the United States live in households that struggle to afford basic needs, including food, housing, and medical expenses. 1 Families raising the youngest children – infants and toddlers who wear diapers – tend to struggle more because they are most likely to live in poverty. 2 A particularly pressing form of basic needs deprivation facing these families is diaper insecurity, not having enough diapers to keep children dry, comfortable, and healthy without sacrificing other essentials, a problem reported by up to half of American mothers with young children.3 –9 Families struggling with diaper insecurity are also more likely to struggle with other forms of deprivation such as food scarcity and housing insecurity,9,10 and parents’ efforts to meet their children’s diaper needs often lead to skimping on other essentials.
Lacking diapers can have serious and widespread consequences for infants’ and toddlers’ health and development. Parents facing diaper insecurity often must stretch diaper supplies, including using diapers that no longer fit, creating makeshift diapers, having children go diaper free, reusing dried diapers, or leaving the same diaper on for days.6,10,11 Ill-fitting diapers, using diapers made from non-breathable materials, and infrequent diaper changes can increase children’s risk for urinary tract infections, diaper dermatitis or “diaper rash,” and yeast infections in the diaper area.12,13 All three conditions are primary reasons children go to pediatricians and emergency rooms, 14 and they can become so severe as to require hospitalization. Infants and toddlers without enough clean, comfortable diapers can also experience sleep disruptions and developmental delays, such as later crawling or walking. 15
In addition to impacts on children, diaper insecurity and related coping strategies also have negative effects on parents. Quantitative research on diaper insecurity has found that lacking enough diapers is a form of material deprivation specifically associated with worse maternal mental health outcomes, including higher levels of stress, anxiety, and depression.6,9 Smith et al. suggested several possible explanations for this. Diaper insecurity may be associated with other factors, such as low income and social isolation, that are known to negatively affect psychological well-being; diaper insecurity and maternal mental health problems may share common causes, such as children’s health issues or economic challenges; or diaper insecurity alone may negatively impact mothers’ health and well-being. 6
This prior research identifying the association between diaper insecurity and negative maternal mental health outcomes points to the need for additional research on mothers’ lived experiences of diaper insecurity as a case of how limited access to basic needs impacts women’s health. Given diapers’ central role in early childcare, diaper insecurity is likely to have greater effects on parents’, especially women’s, well-being. Women are more likely to provide childcare and a greater proportion of care for young children, 16 make the majority of household purchasing decisions, 17 and perform cognitive labor associated with anticipating and monitoring family members’ needs. 18 This study therefore aimed to understand lived experiences and perceived effects of managing diaper insecurity among women who were primary caregivers of young children.
Materials and methods
From January 2018 to September 2019, I interviewed 70 women who had experienced diaper insecurity. I utilized purposive sampling strategies and recruited previously unknown to me respondents through sharing my contact information via family service providers, including medical offices, clinics, and hospitals, WIC (Special Supplemental Nutrition Program for Women, Infants, and Children) offices, and social media forums for parents seeking basic needs assistance. Those who self-identified as struggling to access diapers and who had primary responsibilities for a child in diapers, including those who were pregnant, qualified for the study. Seven respondents were recruited via snowball sampling.
After recruiting 70 women and 2 men using these methods, I targeted recruitment efforts at fathers by distributing study flyers through fatherhood programs, diaper banks, and social service agencies that served men. Only one additional father contacted me about the study, and he asked his wife most of the questions during the interview. Unsuccessful attempts to recruit more fathers, despite targeted efforts, point to the highly gendered nature of managing diaper insecurity, which likely falls predominantly on women in their capacity as mothers and primary caregivers of young children. Given this, I chose to concentrate analysis on women’s experiences of diaper insecurity and excluded data from the three men interviewees to intentionally focus on mothers’ experiences.
In-depth qualitative interviews took place over the phone and lasted 30–70 min, with most lasting approximately 1 h. I asked mothers about their family and financial situations; diapering practices; experiences of diaper insecurity; strategies for accessing diapers; and demographic characteristics (see Supplemental Appendix 1 for the full interview guide). I sent respondents each $25 cash in recognition of the value of their time. The Committee for the Protection of Human Subjects (IRB) at California State University, Fresno, reviewed and approved the study (Protocol #2018-844).
Data analysis
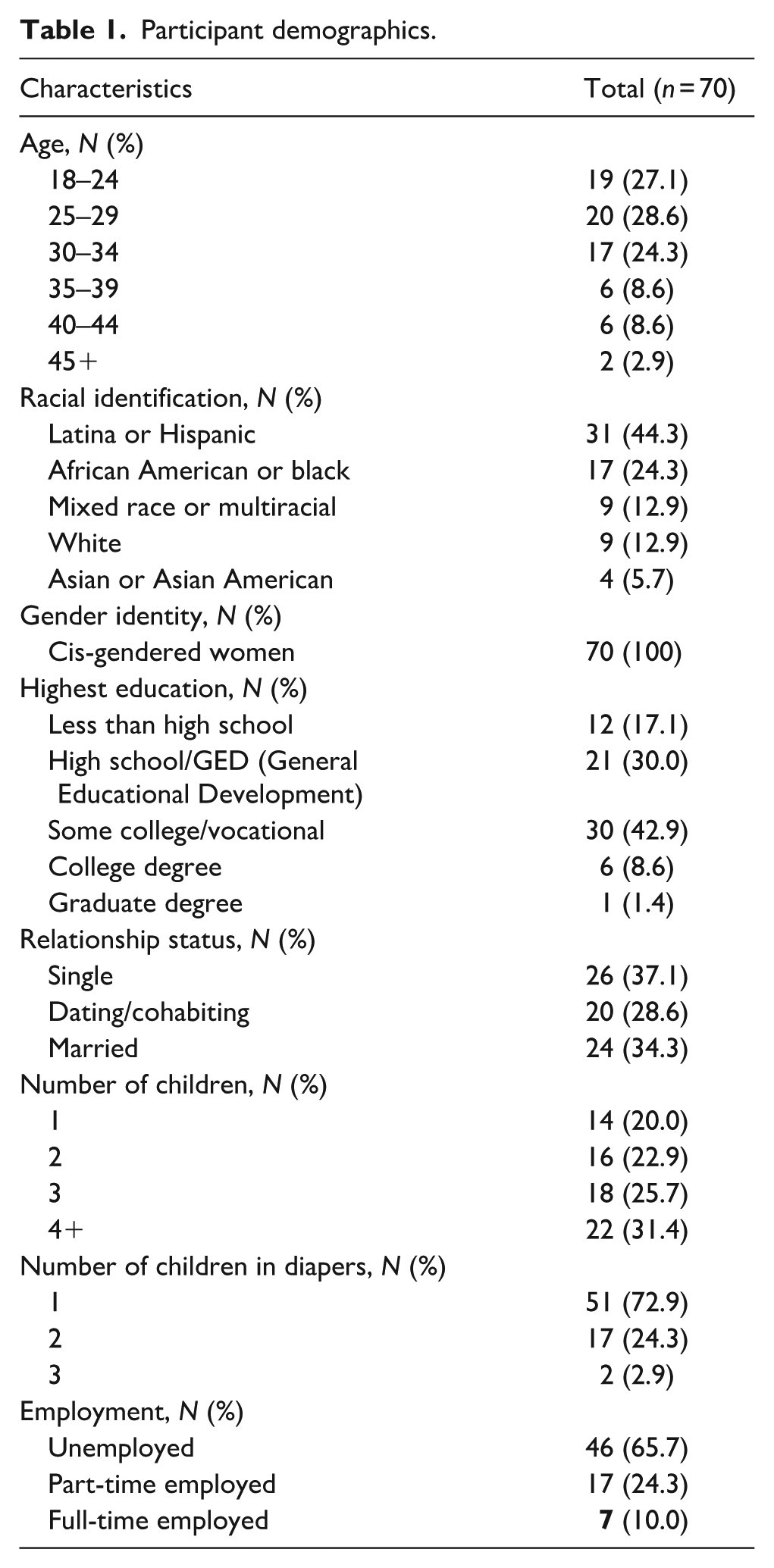
The median age of the 70 mothers I interviewed was 29 years, and most were women of color. Based on the official poverty threshold at the time of the interviews, almost all were living in poverty. 19 Mothers reported spending, on average, $66 (ranging from $22 to $175) per month on diapers, which was 8% of the mean reported household income. Participants’ demographic characteristics are presented in Table 1. All mothers resided in California at the time of interviews.
Participant demographics.
Using an abductive analytical approach that combines deductive and inductive strategies, 20 I utilized knowledge of previous literature on mothers’ experiences of diaper insecurity to devise research questions and compose the interview guide. To confirm narrative accuracy and credibility of the data, while interviewing mothers I used probes for more detailed explanations, iterative questioning to corroborate answers, and on-the-spot member checks of both descriptive and interpretive validity.
With mothers’ explicit permission and consent, I digitally recorded the interviews and took detailed notes. All interviews were transcribed in full, and I wrote extensive descriptive, thematic, and methodological notes. Utilizing word processing and spreadsheet software and concept-mapping techniques while employing a flexible coding process, I then developed thematic findings and explanations that emerged inductively from the data. First, I coded for broad topics by applying index codes and a priori attributes (e.g., use of diaper-stretching strategies, missed work due to lacking diapers, and forgoing other basic needs) to each paired transcript and memo, which allowed me to generate cross-case memos and a set of analytic codes. Second, I applied these analytic codes and generated new inductive attributes (e.g., diaper insecurity and coping strategy impacts on mothers’ mental health and parental self-efficacy) by comparing respondents’ references to these themes across the body of data. Finally, to ensure that accounts of the data met the threshold for theoretical validity and cross-case reliability, I reviewed the data for alternative explanations and negative cases.
Drawing on my training in and previous experience with qualitative research methodologies and based on standards for in-depth qualitative interviewing studies, an a priori sample size of at least 50 respondents was initially planned. However, recruitment and data collection continued until both data saturation and inductive thematic saturation were reached. 21 The completion of 70 interviews was the point at which responses aligned with answers from previous interviews, data had become repetitive, and no new codes or themes emerged from subsequent interviews.
As a white, affluent woman researcher interviewing mostly low-income women of color, I was mindful of how personal characteristics and social distance potentially shaped the interview encounters. My name, affiliation, and contact information noted on recruitment materials readily signaled my gender, educational background, and occupation. However, because I intentionally opted for audio-only telephone interviews for reasons of access, inclusion, and rapport, respondents did not have visual data to gauge my race, age, or other characteristics. Respondents often inquired verbally about my age but rarely asked about my race or ethnicity (perhaps due to my name or linguistic signaling). The question mothers asked most was whether I, too, was a parent and how old my child or children were. Disclosing to respondents that I had a child in the middle of toilet training who still wore diapers was key to establishing rapport. Although we were mostly outsiders to the other’s social positions and experiences, we connected through shared insider status as mothers of children in diapers. 22
In navigating both social distance and shared parental status, I communicated to respondents that they were experiential experts and that my goals were to listen to and understand their stories of diaper insecurity without judgment; convey their stories and perspectives accurately, objectively, and respectfully; and protect their privacy. Thus, all names are pseudonyms and identifying details have been excluded. The reporting of this study conforms to the consolidated criteria for reporting qualitative research (COREQ) checklist for interviews (see Supplemental Appendix 2 for the completed checklist). 23
Results
This analysis identified three primary themes in how mothers explained their experiences of diaper insecurity as negatively impacting their mental health and well-being. First, common ways of managing diaper insecurity, including missing work, school, or medical appointments and having to forgo other basic needs, shopping, and socializing, often resulted in less income, less access to health care, and fewer social interactions for mothers. Second, mothers described the additional physical, cognitive, and emotional labor associated with managing diaper insecurity as contributing to poorer physical and mental health. Finally, mothers shared that shame associated with an inability to provide a primary basic need of early childcare and fear of stigma hindered their parental self-efficacy and sense of self-control, leading to depression and anxiety.
“When we don’t have diapers, we just don’t go out”: maternal sacrifices of diaper insecurity
Mothers’ efforts to cope with not having enough diapers affected how they interacted with their children and how they managed their social lives and work schedules. A third of mothers in the current study shared with me that they worked fewer hours and/or reduced how much time their children spent in childcare because of lacking diapers. Alicia, a Latina, 22-year-old mother of two, said, There have been times I couldn’t go to work. I didn’t have gas because I needed to buy my son diapers instead of going to work. I used a sick day for that, almost lost my job over it.
Over half of the mothers I interviewed had foregone running errands, attending social events, or leaving their homes because of diaper insecurity. These tactics were often necessary when mothers had completely run out of diapers and became common strategies for saving diapers when children needed to be in public, leading to feelings of social isolation. Fatima, a black, 36-year-old mother of two, shared: When we have to go out, she puts on a diaper. When we’re at home, she’s just been no diaper. When we don’t have diapers, we just don’t go out. No diapers, no doctor visit.
Likewise, Jocelyn, a black, 32-year-old mother of two, recently had a high-risk pregnancy during a period of intense stress exacerbated by diaper insecurity. She explained why she rarely left the house due to lacking diapers: It makes you feel bad not being able to just go out and get the stuff for your kids when they need it. If my baby needs something, I can’t just go open my wallet and get $20 and go purchase stuff, so that makes me depressed. I’m trying potty training to get rid of the diapers. So, between it all, I just don’t leave the house unless I absolutely have to. . . . I don’t get my hair or nails done, none of that. I just stay in the house and spend money on the kids.
Like Alicia, Fatima, and Jocelyn, many mothers described rarely leaving their homes, missing work and medical appointments, and not going grocery shopping or socializing because they lacked diapers. Staying home more readily allowed them to use common diaper-stretching strategies, such as having children go diaper free, creating makeshift diapers using other household materials, and using the same diaper for longer. Mothers saved their limited disposables for time their infants spent in public or childcare and otherwise tried to avoid being in public where their diapering habits were subject to greater social scrutiny. As Aurelia, a Latina, 25-year-old mother of three, noted: It’s just safer if a kid doesn’t wear a diaper at home. . . . You still stress over it, like ‘I don’t have enough diapers,’ and that stress affects your health, but at least other people aren’t watching. . . . That wears on you and wears you out. . . . It has really affected my physical and mental health. You just stress over it because you’re going back and forth in your mind thinking, “How am I gonna do it? How am I gonna do it?”
The exasperation and fatigue in Aurelia’s voice were palpable, underscoring the stress of constantly weighing a lack of diapers against the need to leave the house for work, shopping, and her own mental well-being.
Another common strategy mothers used for coping with diaper insecurity was sacrificing their own basic needs so that they could afford diapers for their children. Half of mothers talked about not buying their own period products, toilet paper, medicine, underwear, clothing, or shoes, while a quarter reported going without food or eating cheaper foods to buy diapers. Ashley, a Latina, 18-year-old mother of one, shared, Lots of the time I don’t eat a whole day, or sometimes I’ll just eat one part of the day because I’m trying to save money for diapers and I’m so stressed.
Similarly, Kiera, a multiracial, 23-year-old mother of one, explained, By the end of the month, we literally have nothing, no food, no money, low diapers. They’ll be three or four days where I’ll go without eating, just drink water. It makes me angry and sad, and not eating adds to the stress.
Mothers like Ashley and Kiera paid for diapers in part using currency of their own hunger, stress, and discomfort.
Diapers were also costly in this way for Lila, a multiracial, 24-year-old mother of three, who sold her blood plasma twice weekly to afford diapers for her two youngest children. Lila said, I was going two times a week so I could get the $25 and then the $40. I did it for three, almost four months, donated blood. My boyfriend made me stop because he was worried it wasn’t good for me. It was hard because my hemoglobin always seemed to be so low. I was trying to eat kale, boiled eggs, oatmeal, orange juice trying to make sure I was high [in hemoglobin] before I went. I was turned down once because I was two points too low. It was so stressful like, “How am I going to get these diapers if I can’t get the money for the blood?” I was breaking down crying because I didn’t know what I was going to do.
Lila’s boyfriend convinced her to stop selling her blood plasma for diaper money after he noticed severe problems with her energy levels, sleep, and mood.
Mothers shared that they did everything they could to buffer their children from any ill effects of diaper insecurity, largely by taking its burdens upon themselves. Yet, the sacrificial strategies they necessarily used to access and stretch diapers tended to have negative financial, social, emotional, and physical costs. These costs included the following: lost income; less access to medical care; negative moods and stress associated with reduced food intake; less control over their time and schedules; and reduced social interaction resulting from seclusion to private spaces where they could more readily cope with lacking diapers. Considering how needs are material, such as food and medicine, as well as psychological and social – like a sense of agency and the ability to interact with others in collective spaces for work, worship, friendship, and health care – managing diaper insecurity led to mothers missing out on a variety of necessities essential for their well-being as they understood it.
“The diaper thing, it’s killing me”: how managing diaper scarcity affects maternal mental health
According to mothers, managing diaper insecurity also negatively impacted their health by requiring excessive physical, cognitive, and emotional labor that taxed their psychological resources. Although I did not explicitly ask mothers about mental health impacts of experiencing and managing diaper need, nearly two in three (N = 46) described diaper insecurity as directly linked to experiences of “anxiety”; “depression” or “depressive symptoms”; “trauma” or “PTSD”; “worry,” “stress,” or “grief”; negative self-esteem or self-image, and/or sleep disruptions.
Once reason for this is that many of the strategies mothers used to cope with diaper insecurity involved exacting attention to diaper supplies, such as carefully tracking the number of diapers on hand and exactly how long those diapers were likely to last. This high degree of specificity and calculating, saving, and stretching limited diaper supplies as far as possible required a great deal of effort and energy. Maria, Latina, 30, and a mother of four, explained, I count every diaper, write it down, track every little thing, so I know how much money and how long each box will last. Diapers is the number one concern for me right now, so I have to think about this stuff in this way. I can’t go over my daily limit.
Mothers especially feared getting dangerously close to using their last available diaper and the impossible choices that would ensue. Jessica, a white, 37-year-old mother of five, explained, It’s that feeling when you’re down to your last two diapers, you’re waiting for your check to come tomorrow, and your baby is a little bit wet, but you don’t want to change them right now because you might run out of that last diaper. That and we don’t have gas in the car until tomorrow, and I can’t go to the store to use the little gas I have to buy diapers. I’m always thinking about diapers, making sure the babies have diapers, or if they only have one diaper left, when I can get to the store. It’s always kicking in the back on my brain. Worrying about it becomes second nature.
Toni, Latina, 29, and a mother of four, similarly shared, One day, we were down to two diapers. I didn’t get paid until the next day, so I was doing everything to make those two diapers last until I could get paid, get to the store, get her diapers, and change her then and there. . . . When she had on that last diaper, I was like, “Please, please don’t poop, we can make it, you know?” The diaper thing, it’s killing me.
Using a final diaper was its own source of distress that triggered mothers’ feelings of despondency. Joanna, Afro-Latina, 18, and a mother of one, told me, I psych myself out when he’s on the last diaper. I’m already a mess emotionally. I just had a baby. I felt like I was going crazy in the head, my emotions were everywhere. Diapers and the money situation are a big trigger for me. I can change him only when he really needs to be changed, not when he’s barely wet, just to save on diapers. I think, “It’s okay, he can go like 30 more minutes.” I’m embarrassed because that’s my baby. . . . It takes a big toll on my overall mental health. . . .When I’m in the zone with him, and he’s just the light of my life, then I do of course get that peak of happiness, but that’s not very often. But if I’m having a bad day, the diapers are running really low, it’s harder to interact with him, to get my mind off things.
Joanna poignantly captured the psychological toll of managing diaper scarcity, especially during the maternal postpartum period when infants require the most diaper changes – around 10–15 per day – and skin is particularly delicate and prone to rashes.
Molly, black, 31, and a mother of two, likewise described the mental toll of daily effort and energy required to manage diaper insecurity. When we’re at home, I let them go without diapers, and one time, I even stretched my daughter’s medicine for diapers. I’m currently down to my last pack of diapers now, and I’m thinking I have a shelf I may be able to sell. . . . I’m stressed out a lot. It definitely takes a toll on [my husband and kids]. I try not to let them see it, but sometimes it’s unavoidable. Last month, I went through a bad depression for a week. It was non-stop crying because all I was thinking about was money. “How am I gonna buy diapers this month? How I’m gonna buy the food and diapers this month?”
For Molly, coping with diaper scarcity involved managing, not only diapers, but also maternal stress and strain on family relationships created by constant worry over how to stretch the household budget to cover diapers and other basic needs.
Mothers’ diaper stress was particularly acute when concerns about sick children coincided with diaper insecurity. Nora, a Latina, 23-year-old mother of two, shared that she agonized a lot more about the diapers when the kids get sick because I think, “This is like the fifth diaper he just went through. I’m down to eight diapers.” I never thought I’d have to worry about counting every last diaper all the time, about my kids not having enough. It weighs on you and brings you down.
Diana, 29, white, and a mother of five, described similar unrelenting concerns. I just pray and hope the kids don’t get sick, that by the time I get paid, I can get the diapers right away. . . . We have to wait for the diaper to get very, very full as it’s nearing the point of leaking, and then change them right away. It wears you out having to worry about every last diaper.
Like Nora and Diana who used the language of diaper scarcity “weighing on you” and “wearing you out,” many mothers described incessant anxiety about being down to their last diapers. They experienced diaper insecurity as a particularly stressful form of deprivation that they felt in their bodies and minds, a feeling that constantly occupied their thoughts and led to feelings of depression “bringing you down.”
“I feel like I’m a bad parent when diapers run low”: how diaper insecurity undermines maternal self-efficacy
Mothers also shared that diaper insecurity led to feelings of having failed as a provider and caregiver when the work of managing limited diaper supplies and having too few diapers undermined their parental confidence and self-efficacy. Melissa, a Hmong, 33-year-old mother of three, vividly recalled one anxiety attack brought on by a shopping trip for $100 worth of diapers. She stocked up and bought cheaper diapers in bulk when she had money, but even this caused stress because she worried her daughter would outgrow that size before she could use them all. She further explained, You think you’re okay when you’re lifting your baby, and you look at her. You’re like, “I’m okay, sometimes I think you need more than I can give, but you don’t.” But then you’re holding the baby and all of a sudden, you’re not enough. There were moments when I didn’t want to hold my baby because of my depression. In those moments, diapers always come into mind, like, “Oh, did I get your diapers? Do I have enough? Did I use too many? Oh my gosh, I don’t actually have enough. Or I have too much of the old size, but I don’t have any bigger ones. I have to finish the smaller ones before I can afford new ones.” It’s all so triggering. The diaper stuff is always on my mind.
Mothers also described how self-doubt connected to diaper insecurity led to feelings of hopelessness and triggered or exacerbated preexisting mental health challenges. Brenda, an Asian American, 25-year-old mother of three, shared Sometimes I feel hopeless, like I can’t do much at all. But I know I’ve tried to provide as much as I can for my kids, times when I’ve gone without or would push a bill out because my son really needed diapers, and I had nobody and nothing else. My [post-traumatic stress disorder] really comes out over the diapers. As much as I need electricity, to keep my kids out of the dark, I need even more to make sure they’re comfortable, so they won’t see my struggle.
Part of that struggle was coping with the judgment and stigma, both from others and internalized, mothers feared when they did not have enough diapers. As Toni explained to me, I feel like I’m a bad parent when diapers run low because it’s like I’m not a good provider. . . . I’ve had anxiety attacks worrying about whether people think I’m a bad mom if the baby has a saggy diaper. That’s why I can’t buy the cheap ones. Two pees and they drop.
Toni was among several mothers who shared with me that they purchased more expensive diapers and changed diapers more frequently, thereby worsening diaper insecurity, because they were afraid that a child seen in a soiled diaper signaled that their mother was unfit.
Two in three mothers I interviewed had borrowed diapers or money explicitly intended to buy diapers from others in their social networks, including family, friends, coworkers, and neighbors. Asking family or friends for diapers or diaper money was also the most reported diaper need coping strategy in other research on diaper insecurity. 9 Yet, mothers confided that they were reluctant to ask for diaper help and usually only did so as a last resort in the direst situations. Aversion to asking for help was rooted in mothers’ identities as self-reliant parents committed to sacrificing and stretching for their children.
Shaped by cultural narratives of self-sufficiency and parental responsibility, requests for diaper assistance came at a psychological cost to mothers’ pride, sense of independence, and parental self-efficacy. Audra, a white, 32-year-old mother of five, said, It’s sad to need diapers. You don’t want to feel like you’re failing as a parent.
The embarrassment associated with asking for diaper help, even, and sometimes especially, from others they knew well, prevented many mothers from asking at all. As Toni shared with me, I will never ask my mom for diaper money again because she doesn’t get it. Neither does my sister. They look down on me about it. It gets thrown in my face. I can’t live down that I asked them for diapers.
Mothers like Audra and Toni worried that others attributed their diaper insecurity to bad budgeting and not prioritizing their children’s needs.
Carrie, a Latina, 33-year-old mother of four, also described the judgment she and other mothers encountered when asking for diaper help, including questions about their childbearing motivations and commitments. “‘Why do you have kids if you can’t provide for them?’ people ask. You see all these things on social media, shaming mothers for asking for things they need for their baby, but at least I’m doing what I got to do to get the diapers.”
Similar concerns prevented some mothers from seeking diaper assistance from diaper distribution services and organizations. Not only did it require that they leave their homes and travel in public spaces, making managing diaper insecurity more difficult, it also often involved providing documentation and information they were reluctant to share with others from whom they feared judgment. Natasha, a black, 35-year-old mother of four, described diapers as a daily struggle, but I don’t want to put my business out there. People can see certain people like us, and they look down on us and start talking bad because we can’t afford good [diapers]. . . . We need programs to help with the [diapers], but just don’t look down on us for needing help.
While half of mothers who had received diapers from organizations reported positive and supportive experiences, the other half discussed experiences like Natasha’s that resulted in feelings of stigma or judgment. Even in the absence of enacted stigma, discrimination or unfair treatment from others, mothers struggling with diaper insecurity often still experienced felt stigma, the internalized shame and expectation of discrimination that prevented mothers from seeking help with diapers, undercutting their self-esteem and feelings of parental self-efficacy. 24
Discussion
Prior research suggested several possible pathways by which diaper insecurity could be linked to poorer maternal mental health, including diaper insecurity exacerbating low income and social isolation, sharing common causes such as health or financial issues, and experiences of diaper insecurity directly impacting mothers’ health and well-being. 6 My in-depth qualitative interviews with mothers about their lived experiences of diaper insecurity suggest that all three mechanisms are likely to blame.
Recent literature finds evidence of negative physical, emotional, social, and economic consequences of diaper insecurity.9,25 Parents who cannot provide diapers for daycare miss, on average, 4 days of work or school per month, risking lost wages, lost jobs, and lost opportunities for upward mobility. 26 The findings of this analysis focused on diaper insecurity’s impacts specifically on maternal health and well-being align with this previous research indicating that lacking diapers and common diaper insecurity coping strategies directly or indirectly lead to or exacerbate many of the challenges poor and low-income mothers face. These challenges include food insecurity and other forms of basic needs deprivation; social isolation and missed opportunities for accessing health care, childcare, and employment; and increased physical and cognitive labor needed to manage scarcity and stigma associated with lacking basic needs.
As described by economist Sendhil Mullainathan and psychologist Eldar Shafir, managing material deprivation depletes individuals’ emotional energy. Scarcity of any kind – too little money, time, or human connection – overloads mental capacity, or what Mullainathan and Shafir call bandwidth. 27 Like a physical muscle, pressures on and overuse of bandwidth strain cognitive abilities, leading to negative mental and physical health outcomes. Deprivation, disconnection, and discrimination associated with diaper insecurity all tax mothers’ already limited bandwidth, which can compromise parental self-efficacy and contribute to poorer physical and mental health outcomes through a variety of biological, psychological, and environmental pathways known to be associated with depression and anxiety.28,29 Interviews with mothers revealed that these include, but are not limited to, fatigue and inadequate nutrition and sleep; stress, low self-esteem, rumination, and negative emotions and self-concept; and role strain, social exclusion, and lack of social support.
Implications for policy and practice
Diaper insecurity and challenges associated with it are consequences of the financial and social precarity that characterizes much of parenting in the United States. Given limited public provisions and social support for meeting children’s basic needs, diaper expenses are among the many reasons that parents with infants and toddlers face high caregiving costs. However, fiscal and safety net policies in the United States, including those specifically intended to help low-income and poor mothers with young children, do not always recognize diapers as a basic need. Diapers are not systematically covered by the largest public assistance programs, including WIC, and direct cash aid assistance is rarely sufficient to afford diapers in addition to other basic needs. 30 With few exceptions, state Medicaid programs provide diapers only as a qualifying medical expense for children over a certain age (at least 3 years) medically diagnosed as incontinent. Because diapers are not recognized as a qualified medical expense for most children, they are still taxed in many states at rates ranging from 2.5% to 7.5%. 31
Diaper distribution organizations, including many diaper banks that serve maternal and infant health programs, are a crucial source of support for diaper-desperate families. In 2016, diaper banks distributed more than 50 million diapers to over a quarter of a million children across the United States, meeting only 4% of the estimated diaper need across the country. 32 Despite increasing service capacity and greater public funding in recent years, diaper banks and basic needs banks that distribute diapers mostly rely on in-kind and private monetary donations, resulting in insufficient funding and capacity to meet needs across their service areas.
The findings of this research reinforce the importance of understanding diaper insecurity as a form of basic needs deprivation and adverse social determinant of both child and maternal health and well-being, as well as an environmental factor that may contribute to physical, emotional, and social causes of worse maternal mental health. As such, diapers should be recognized as a basic need by pediatric, obstetric, and other healthcare providers and in programs and policies that seek to support and improve child and maternal health.
Several state and federal bills have proposed classifying diapers as a medical necessity to lay the policy foundation for greater coverage of diaper expenses through income-based programs like Medicaid. Unfortunately, such bills have not yet gained sufficient political traction. Nevertheless, many continue to advocate for diaper policies and public funding for diaper distribution organizations and infant and maternal health programs to provide diapers specifically as a basic need support that enhances the development of children and the physical and mental health of their mothers.
Limitations
This study has several limitations. I did not recruit a nationally representative sample of respondents currently caring for children who wear diapers, but rather a purposive sample of parents who identified as not having enough diapers for children in their care. The interview guide used was neither validated nor pilot-tested, and the analysis was conducted by a single coder. Moreover, focusing only on women’s experiences of managing diaper insecurity necessarily discounted men’s experiences. Study findings may therefore have limited generalizability to all those experiencing diaper insecurity and should be subject to further validation. Future research should also incorporate men’s perspectives to provide a more comprehensive understanding of how diaper insecurity impacts parenting and families more broadly.
Additionally, I relied on respondents’ self-reported accounts of diaper insecurity as contributing to negative maternal mental health outcomes, rather than any official medical diagnoses of anxiety, depression, and related conditions. Qualitative research has inherent limitations in identifying correlations and influencing factors. However, it is particularly well-suited for studying experiences and understandings of those experiences in context. As designed, the study was unable to ascertain to what extent other factors, such as food insecurity or housing instability, may have directly or indirectly contributed to the challenges mothers described. Future research should continue to explore how diaper insecurity may directly contribute to adverse maternal health outcomes.
Conclusion
Complementing prior quantitative research on correlations between diaper insecurity and negative maternal mental health outcomes, this research offers an in-depth, qualitative understanding of the experiences and perceptions of mothers who struggle with diaper insecurity as a form of basic needs deprivation that mothers themselves understand as negatively impacting their physical and mental health. Results suggest that, beyond its association with other factors, such as low income and social isolation, that are known to negatively affect physical and psychological well-being, lack of access to enough diapers likely contributes to and exacerbates maternal stress, anxiety, and depression. Interviews with mothers revealed the physical, emotional, and social toll of diaper insecurity and point to public support for diaper distribution and recognizing diapers as a medically necessary basic need as possible pathways for improving women’s health and well-being.
Given that mental and physical health challenges arise from a confluence of individual, interpersonal, and structural factors rooted in physiological, social, and economic dynamics, among others, it is unlikely that diaper insecurity independently causes or explains maternal health problems. Furthermore, as mothers interviewed for this research could attest, diaper insecurity is rarely experienced in isolation from other financial stressors, time pressures, and lacking other needs. If diaper insecurity is one of many challenges low-income mothers face, it is unlikely that a targeted intervention such as more systematic diaper funding or distribution would lead to significant improvements in maternal health. However, addressing one type of deprivation known to be linked to lacking other basic needs and poorer maternal health outcomes would help address, if not resolve, diaper insecurity–related stressors that mothers experienced and described as negatively affecting their physical and mental health.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261424037 – Supplemental material for Depression of being “down to my last diaper”: A qualitative descriptive study of associations between diaper insecurity and maternal health
Supplemental material, sj-docx-1-whe-10.1177_17455057261424037 for Depression of being “down to my last diaper”: A qualitative descriptive study of associations between diaper insecurity and maternal health by Jennifer Randles in Women's Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057261424037 – Supplemental material for Depression of being “down to my last diaper”: A qualitative descriptive study of associations between diaper insecurity and maternal health
Supplemental material, sj-pdf-2-whe-10.1177_17455057261424037 for Depression of being “down to my last diaper”: A qualitative descriptive study of associations between diaper insecurity and maternal health by Jennifer Randles in Women's Health
Footnotes
Acknowledgements
The author appreciates participants’ willingness to share their valuable time and stories for this research.
Ethical Considerations
The Committee for the Protection of Human Subjects (IRB) at California State University, Fresno, reviewed and approved interviews for this study (Protocol #2018-844) on January 22, 2018.
Consent to Participate
Participants received and reviewed written consent documentation and gave verbal consent prior to interviews. Verbal consent was determined to be appropriate due to the virtual nature of the interviews. Consent was recorded in a password-protected and encrypted file stored on an institutional drive that was accessible only by the principal investigator.
Consent for publication
Not applicable.
Author contributions
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: American Sociological Association Fund for the Advancement of the Discipline and the College of Social Sciences at California State University, Fresno.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.