
Abstract
Background:
Transgender (trans) women living with HIV often face barriers to accessing inclusive and comprehensive primary and HIV care.
Objectives:
We aimed to (1) describe differences in trans women’s disclosure of their trans identity and comfort discussing trans identity and trans-specific healthcare needs, based on physician type, and (2) report on the prevalence of negative trans-specific experiences with HIV physicians and any provider-related factors associated with comfort.
Design:
Data of trans participants in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS) were analyzed across three waves (2013–2018).
Methods:
Descriptive statistics explored disclosure of trans identity and comfort discussing trans-specific healthcare needs with family physicians versus HIV physicians. Fisher’s exact tests of association explored the relationship between provider-related factors and self-reported comfort. Prevalence of negative trans-specific experiences with HIV physicians was reported.
Results:
At baseline, of 54 trans women, 39 (72.2%) had a physician who supervised their HIV care in the year preceding (HIV physician). Among this subset, 94.9% had disclosed their trans identity and 82.1% reported feeling comfortable discussing trans-specific healthcare needs with this physician. Of the 27 (50.0%) who reported having a regular family physician other than their HIV care provider, 92.6% had disclosed their trans identity and 88.9% were comfortable discussing trans-specific healthcare needs. The most prevalent negative trans-specific experience with HIV physicians reported cumulatively was being told by the physician that they did not know enough about trans-related care to provide care (16.7%).
Conclusion:
Our findings demonstrate a high prevalence of disclosure of trans identity to physicians among our trans participants. Our findings suggest trans women have similar comfort discussing trans-specific healthcare needs with their family and HIV physicians; however, negative experiences with HIV providers indicate the need for gender-affirming, trans-specific provider training.
Introduction
Transgender (trans) women are disproportionally affected by HIV globally, and it has been estimated that they are 66 times more likely to have acquired HIV as compared with other individuals over 15 years of age.1–3 Such a high prevalence of seropositivity in this population can be attributed, in part, to a syndemic of co-occurring health and psychosocial factors, such as stigma and violence, that are intersectional, interacting, and may increase vulnerability to HIV infection.4–6 In Canada, trans women living with HIV often face barriers to accessing inclusive and comprehensive primary health and HIV care, including enacted stigma in the provision of direct care, cisnormativity in sexual health services, and a lack of provider knowledge, training, and experience working with trans populations. 7 Intersecting sociodemographic factors may present barriers that further limit access to inclusive and comprehensive primary and HIV care for marginalized populations, such as the intersection of anti-trans stigma and racism among trans women of color living with HIV. These experiences may be better understood through the multiple minority stress model, whereby intersecting social stresses may lead to poorer health outcomes and reduced uptake of healthcare services.8–11
Positive patient-provider relationships are key to bolstering healthcare utilization and positive physical and mental health outcomes in trans individuals regardless of HIV status. 12 The voluntary disclosure of trans identity to healthcare providers precedes the co-development of gender-affirming relationships. 13 However, barriers to disclosure, such as the fear of discrimination and stigma, anxiety, and concerns regarding patient privacy, may hinder this co-development.14–16 For trans patients living with HIV, discomfort discussing trans health issues with family physicians may also hinder their engagement in necessary HIV care and the broader care cascade. 17 Conversely, comfort discussing gender-related health issues with a healthcare provider is associated with improved HIV prevention and treatment outcomes, including viral suppression. 18
Among women living with HIV, HIV-related stigma is associated with a lower likelihood of antiretroviral therapy (ART) initiation and suboptimal ART adherence. 19 Stigma related to both HIV seropositivity and trans identity intersects to negatively impact access to and comfort with primary and HIV care in trans women living with HIV.20,21 Healthcare providers may enact trans- and HIV-related stigma in the provision of care for trans women living with HIV, which in turn may contribute to a feeling of mistrust of medical professionals in this population.22,23
To improve access to trans-inclusive and culturally sensitive HIV prevention, care, and support programs in Canada, we must better understand the current landscape of patient-provider relationships between trans women living with HIV and their family physicians and HIV care providers. There exists a dearth of literature on the prevalence of disclosure and comfort with primary and HIV care providers among trans women living with HIV. Therefore, the objectives of this study are to (1) describe differences in trans women’s disclosure of their trans identity and comfort discussing trans identity and trans-specific healthcare needs, based on physician type, and (2) report on the prevalence of negative trans-specific experiences with HIV physicians and any provider-related factors associated with comfort.
Methods
Study design and participants
This is a secondary analysis of data from The Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). CHIWOS was a multi-site prospective cohort study that followed 1422 women living with HIV across British Columbia, Ontario, and Quebec from 2013 to 2018. All participants were 16 years of age or older, had been diagnosed with HIV, and self-identified as women. 24 The trans women subset (n = 54) included participants who, at baseline, indicated being assigned male at birth and reported women or trans women for their current gender identity, or being assigned intersex at birth and reported trans woman for their current gender identity. Participants were excluded if they indicated being assigned female at birth, or if they indicated being assigned intersex at birth and reported woman for their current gender identity. To best align with a community-based participatory approach, all recruitment and data collection in CHIWOS were conducted by Canadian women living with HIV trained as peer research associates (PRAs).25,26
CHIWOS used a non-random, purposive sampling frame that utilized PRA personal networks, community-based and AIDS service organizations, HIV clinics, online resources, community advisory board members, and physical recruitment materials, such as posters and flyers. 24 Participants were followed longitudinally through three waves of structured web-based surveys. These surveys used validated questions and scales, when available, and test-retest reliability of the questionnaire measures was assessed among 30 participants who completed the questionnaire twice. 24 This study uses the baseline and longitudinal survey data collected from October 2013 to May 2015 (wave 1), September 2015 to January 2017 (wave 2), and March 2017 to September 2018 (wave 3). Most survey interviews were conducted in person in English or French in a confidential setting, and some were conducted over the phone or Skype. Following completion of the survey, participants received $50 in remuneration. Study questionnaires are available as Supplemental Material to this article.
Ethics
All study participants provided written informed consent prior to enrollment. Ethics approval was obtained from the research ethics boards (REBs) of the University of British Columbia/Providence Health Centre, Simon Fraser University, Women’s College Hospital, and the McGill University Health Centre. Study sites with independent REBs obtained approval independently prior to commencing enrollment. 24 The ethics approval number from the REBs of the McGill University Health Centre is 11-102-GEN (Supplemental Appendix B).
Setting
In Canada, HIV care is publicly funded and primarily delivered through a combination of hospital-based specialty and community clinics. HIV clinicians are clinicians who acquired a specific HIV expertise motivated by their special interest in this practice, and it includes some infectious disease specialists (not all), some family physicians, and physicians trained in other specialties. The practice across all physicians considered HIV clinicians is very similar (regardless of their training), but may vary as to whether they also provide primary care for other issues or not. However, HIV care is not part of the training for family physicians, and unless they sought HIV-specific training to become HIV clinicians as defined above, general stream family physicians may provide general primary care to people living with HIV, but not HIV-specific care. Some people living with HIV are thus followed by a HIV clinician only; some are followed by a HIV clinician and a “general practice” family physician. ART is available at no cost or low cost through provincial and territorial drug programs. Multidisciplinary teams often support care delivery, incorporating physicians, nurses, social workers, and peer navigators to address both medical and psychosocial needs.
Measures
Participant characteristics including age, sexual orientation, residence (urban versus rural), housing status, previous incarceration, and years living with HIV were included to better describe the sociodemographic positionality of trans women living with HIV across several provinces in Canada. Statistics Canada defines an urban residence as a location with a population equal to or greater than 30,000. 27 Stable housing was defined as dwelling in an apartment, house, self-contained room in a house or apartment, or a group home. 28
Participants were defined as having an HIV physician if they indicated having received HIV care primarily from one physician in the year preceding the completion of the survey. The “HIV doctor” was identified through the following questions: “Which of the following healthcare providers primarily looks after your HIV medical care*? We will now refer to this person as your HIV doctor.” These HIV physicians had a variety of training backgrounds, such as infectious diseases and family medicine. Participants were then defined as having a family physician if they answer yes to the following question: “Do you have a regular family doctor (other than your HIV doctor)?” Our study questionnaire contained separate questions regarding the care provided by the HIV clinician, and the care provided by the family physician. Disclosure of trans identity to family physicians was assessed with the question, “Does your current family doctor know about your trans identity and experience?” Disclosure of trans identity to HIV physicians was similarly assessed through the question “Does your HIV doctor know about your trans identity and experience?” Response categories for both questions included “Yes, I told my family/HIV doctor,” “Yes, my family/HIV doctor asked about my history,” “Yes, my family/HIV doctor was informed of my trans identity without my consent,” “No, it hasn’t come up,” “No, I don’t feel comfortable telling my family/HIV doctor,” and options for those who did not know or who preferred not to answer.
Comfort discussing trans identity and trans-specific healthcare needs with family physicians was assessed through the question “How comfortable are you discussing your trans-specific healthcare needs with your family doctor?” Comfort discussing trans identity and trans-specific healthcare needs with HIV physicians was similarly assessed through the question “How comfortable are you discussing your trans identity and trans-specific healthcare needs with your HIV doctor?” Participants responded using a 4-point Likert scale ranging from “Very comfortable,” to “Very uncomfortable,” with options for those who did not know or who preferred not to answer. Participants were also asked to report the gender and training of their HIV physician.
To investigate enacted negative trans-specific experiences with HIV physicians, participants were asked “Has your HIV doctor ever. . .?” and were provided with a list of 13–15 response options, including “refused to discuss trans-related health concerns,” “discouraged you from exploring your gender,” and “insisted on examining parts of your body that were not relevant to your care.” Responses to these items were summed into a total cumulative prevalence.
Statistical analysis
Disclosure of trans identity to family and HIV physicians and comfort discussing trans identity and trans-specific healthcare needs with family and HIV physicians were analyzed using descriptive statistics, and change over time is reported descriptively to provide further insight. For HIV physicians only, and due to the small sample size, Fisher’s exact tests, rather than chi-square tests, were performed to determine any statistically significant associations between provider-related characteristics, such as the gender and training of the HIV physician, and comfort discussing trans identity and trans-specific healthcare needs. Odds ratios (OR) with associated confidence intervals (CI) and p-values are reported for these analyses. Comfort was dichotomized to facilitate the creation of 2 × 2 tables for Fisher’s exact tests of association. “Very comfortable” and “Comfortable” were combined to create the “Comfortable” group, and “Uncomfortable” and “Very Uncomfortable” were combined to create the “Uncomfortable” group. The cumulative prevalence of negative experiences with HIV doctors is summarized using percentages. All statistical analyses were performed using R-studio (version 2023.06.0+421). The reporting of this study conforms to the STROBE statement. 29
Results
Participants
The median age at baseline was 41 (interquartile range (IQR): 18–71; Table 1). Most participants were assigned male at birth (96.3%). In terms of sexuality, 51.9% of participants identified as heterosexual, and 44.4% identified as LBQQ2S (lesbian, bisexual, queer, questioning, or two-spirit). Most participants resided in an urban area (98.1%), reported stable housing (74.1%), were Canadian citizens (83.3%), and earned less than $20,000 annually (88.9%). 42.6% had been previously incarcerated, with 5.6% experiencing incarceration within the past year. The racial and/or ethnic composition of the subset was 37.0% Indigenous, 35.2% White, 9.3% African/Caribbean/Black, and 18.5% another race/ethnicity. The median age at the time of HIV diagnosis was 30 (IQR: 0–54), and most participants first accessed HIV care within 4 months of their diagnosis (59.3%).
Baseline characteristics of trans women living with HIV participating in the CHIWOS study (n = 54).

IQR: interquartile range; LBQQ2S: lesbian, bisexual, queer, questioning, and two-spirit; DK/PNTA: don’t know/prefer not to answer; CHIWOS: Canadian HIV Women’s Sexual and Reproductive Health Cohort Study.
Disclosure of trans identity to family and HIV physicians
The prevalence of disclosure of trans identity to family physicians and HIV physicians across all three study waves is illustrated in Figure 1. At baseline, of the 54 participants in the trans subset, 72.2% (n = 39) reported having a physician who supervised their HIV care within the previous year. Of these, 94.9% (n = 37) had disclosed their trans identity to this HIV physician. Of 36 respondents in wave 2, 97.2% (n = 35) had disclosed their trans identity to their HIV physician, and of 25 respondents in wave 3, 100.0% (n = 25) had disclosed their trans identity. At baseline, 50.0% (n = 27) of participants reported having a family physician other than their HIV care provider. Of these, 92.6% (n = 25) had disclosed their trans identity to their family physician. Among the 21 respondents in wave 2 and wave 3, 100.0% (n = 21) had disclosed their trans identity to their family physician.

Percent stacked bar charts of disclosure of trans identity to family and HIV physicians.
Comfort discussing trans identity and trans-specific healthcare needs with family and HIV physicians
The prevalence of self-reported comfort discussing trans identity and trans-specific healthcare needs with family and HIV physicians is illustrated in Figure 2. At baseline, among the 39 participants who reported having a regular HIV physician, 82.1% (n = 32) reported comfort discussing their trans identity and trans-specific healthcare needs with this physician. At wave 2, of 36 respondents, 66.7% reported comfort, and at wave 3, of 25 respondents, 92.0% reported comfort. Among the participants who reported having a regular family physician other than their HIV care provider at baseline, 88.9% (n = 24) reported comfort discussing their trans identity and trans-specific healthcare needs with this physician. At wave 2, among the 21 respondents with a family physician, 90.5% reported comfort which increased to 95.2% at wave 3.
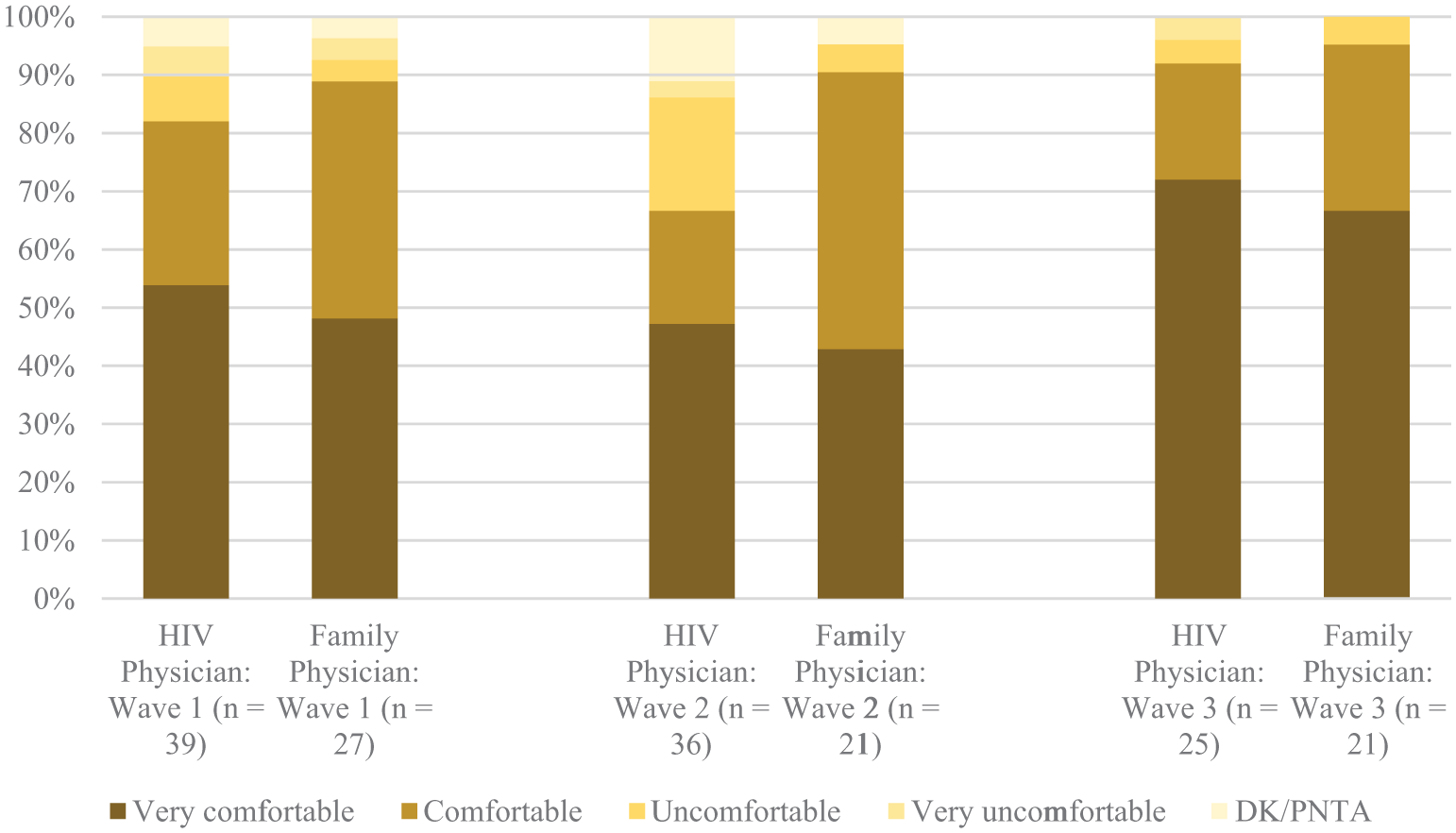
Percent stacked bar chart of comfort discussing trans identity and trans-specific healthcare needs with HIV and family physicians.
Provider-related factors influencing comfort
No statistically significant associations between provider-related factors and comfort discussing trans identity and trans-specific healthcare needs were found. However, when considering the OR estimates as suggesting a possible association, having a woman as an HIV physician (compared to a man HIV physician), or having an HIV clinician trained as a family physician (compared to an HIV clinician trained as an infectious disease specialist) may be associated with greater comfort discussing trans identity and trans-specific healthcare needs at baseline (OR: 1.55; 95% CI: 0.128–85.5; and OR: 1.61; 95% CI: 0.0643–118, respectively). Mosaic plots of the 2 × 2 tables used in Fisher’s exact tests can be found in Figure 3.

Mosaic plots of (a) gender (n = 37) and (b) training (n = 14) of HIV physician versus comfort discussing trans identity and trans-specific healthcare needs at baseline.
Negative trans-specific experiences with HIV physicians
The cumulative prevalence of negative trans-specific experiences with HIV physicians is detailed in Table 2. Most participants did not experience any of the listed negative trans-specific experiences with HIV physicians. However, the three most common experiences were (1) being told by their HIV physician that they did not know enough about trans-related care to provide care (16.7%), (2) their HIV physician thinking the gender listed on their ID or forms was a mistake (9.3%), and (3) their HIV physician refusing to examine parts of their body because they are trans (9.3%).
Cumulative prevalence of negative trans-specific experiences with HIV physicians (n = 54).

Discussion
To create a culturally competent, affirming environment, trans women living with HIV must be empowered to disclose their trans identity and feel comfort discussing their trans identity and trans-specific healthcare needs with healthcare providers. 8 In order to do so, providers must create a context of safety and affirmation in their practice. To our knowledge, this study is the first to compare trans women living with HIV’s disclosure of trans identity and their comfort discussing trans identity and trans-specific healthcare needs with family and HIV physicians in Canada. We found that most trans women in CHIWOS had disclosed their trans identity to family and HIV physicians, and most were comfortable discussing trans-specific healthcare needs with both family and HIV physicians. This proportion increased over the course of follow-up in the study.
Trans-related stigma is known to impact healthcare access for trans women. According to a previous study on healthcare avoidance among trans women in Argentina, 27.4% of whom self-reported HIV infection, trans women who have experienced stigma in healthcare settings were more than three times more likely to avoid accessing care in the future compared to those who had not. 30 Some of the negative trans-specific experiences that were reported by participants in CHIWOS are examples of trans-related stigma enacted by HIV care providers (e.g., HIV care providers discouraging participants from exploring their gender identity and HIV care providers using hurtful language to discuss participants’ trans identity). However, this barrier is not unique to trans women living with HIV; similar findings with sexual minority women accessing sexual and reproductive health care and with sexual minority men accessing preventive HIV care demonstrate a link between negative experiences and healthcare avoidance.31,32
Despite the low overall prevalence of negative trans-specific experiences with HIV physicians, the most prevalent negative experience with HIV physicians was that their HIV physician told them that they did not know enough about trans-related care to provide them care. These results are consistent with those of the Trans PULSE Project, where 29.1% of participants on the transfeminine spectrum reported their family physicians did not know enough about trans-related care to provide them care. 17 To reduce health inequities and negative experiences with both family and HIV physicians, it is imperative that undergraduate medical and residency programs integrate more comprehensive trans-specific training into their standard curricula. Rather than through a singular exposure, trans health care may be best taught through a shift to longitudinally integrated and clinical skills based pedagogical interventions from attitude and awareness-based interventions. 33 Given the higher reported comfort of trans women living with HIV with HIV outreach and program staff who also identify as trans, barriers to disclosure and patient comfort for trans women living with HIV may be ameliorated by increasing the number of trans physicians, primary care providers, and community workers practicing gender-affirming primary and HIV care. 8
Given the reported instances of trans-related stigma, and to further understand and address the prevalence of enacted stigma in the provision of care for trans women with HIV, intersectional stigma frameworks must be integrated into interventions to improve primary and HIV care outcomes. 34 Examples of these interventions include integrating screening for and addressing psychosocial syndemic conditions in existing HIV care interventions, fostering resilience by increasing solidarity within communities of trans women living with HIV, and even implementing multi-method arts-based strategies to build mutual connection among community members.35,36 Signals from research taking place following the onset of the COVID-19 pandemic indicate that barriers to HIV care for trans women may have been exacerbated, particularly for those with multiple intersecting marginalized identities, such as racialized trans women. 37 Future research must consider the implications of global health events on access to care for increasingly marginalized populations.
Limitations
While a diversity of trans women living with HIV are represented in our study, the non-random, purposive sampling strategy utilized by the research team may have resulted in an overrepresentation of trans women living with HIV who were already engaged in care. Although the multi-site design of CHIWOS further allowed for a diversity of trans women living with HIV to be represented in our analysis, it must be noted that rates of disclosure of trans identity and comfort discussing trans-specific healthcare needs with providers likely vary throughout Canada and globally. Trans women living with HIV who face higher levels of stigma and discrimination from healthcare providers may be underrepresented due to healthcare avoidance resulting from previous negative experiences. Despite the efforts of the research team, the small sample of trans women living with HIV may have been underpowered to detect statistically significant associations between provider-related factors and comfort, so our results and conclusions should be interpreted with caution. Most of the interest in this article stemmed from reporting descriptive results on a generally underrepresented population who was included in CHIWOS, and we did not conduct a power analysis prior to performing the analyses. As the most common negative trans-specific experience with HIV physicians was that they were denied care, the type of care refused may have been interpreted differently by participants (e.g., HIV care versus trans-specific care). Also, only negative experience with HIV physicians were reported, and there were no questions investigating positive experiences with these physicians, nor for positive or negative experiences with family physicians. The dichotomization of family physician and HIV physician may present some conceptual difficulties, as some HIV clinicians may also be trained as family physicians and provide primary care for other issues, but the family physicians were specifically identified as not being their HIV doctor in the CHIWOS questionnaire. As is often the case with trans women living with HIV in healthcare and research settings, over the three study waves, retention decreased and resulted in fewer respondents who provided data to address the objectives of this analysis. 38 The longitudinal flow of participant responses to our primary research objectives can be found in Supplemental Appendix A and is illustrated by several Sankey diagrams. Participants also may have not reported disclosure and comfort with physicians due to a lack of comfort with research staff. Furthermore, CHIWOS engaged women living with HIV living only in British Columbia, Ontario, and Quebec, and was unable to capture the experiences of women living with HIV who resided outside of these three provinces. 24 Given that most trans women participants resided in urban centers, these findings may not be generalizable to populations of trans women with HIV living in smaller cities, towns, or rural areas within these three provinces. More research engaging larger samples of trans women living with HIV, and other study designs utilizing qualitative or mixed methods such as conducted by Johnson et al. in Southeast United States, 39 must be undertaken in Canada and globally to better understand the barriers and facilitators to disclosure and comfort.
Conclusion
Our findings suggest that trans women living with HIV in Canada have similar comfort discussing their trans identity and trans-specific healthcare needs with family and HIV physicians. Overall, we found a high degree of disclosure and comfort discussing trans identity and trans-specific healthcare needs with family and HIV physicians. Given the reported instances of negative trans-specific experiences with HIV physicians, there remains a need for gender-affirming, trans-specific training for HIV care providers. Further research, especially qualitative research, may help researchers and clinicians better understand the barriers to disclosure and comfort with family and HIV physicians.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251406944 – Supplemental material for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada
Supplemental material, sj-pdf-1-whe-10.1177_17455057251406944 for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada by Bluma Kleiner, Carmen H. Logie, Pierre-Paul Tellier, Seerat Chawla, Ashley Lacombe-Duncan, Yasmeen Persad, Lashanda Skerritt, Ann N. Burchell, Mona Loutfy, Angela Kaida and Alexandra de Pokomandy in Women's Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057251406944 – Supplemental material for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada
Supplemental material, sj-pdf-2-whe-10.1177_17455057251406944 for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada by Bluma Kleiner, Carmen H. Logie, Pierre-Paul Tellier, Seerat Chawla, Ashley Lacombe-Duncan, Yasmeen Persad, Lashanda Skerritt, Ann N. Burchell, Mona Loutfy, Angela Kaida and Alexandra de Pokomandy in Women's Health
Supplemental Material
sj-pdf-3-whe-10.1177_17455057251406944 – Supplemental material for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada
Supplemental material, sj-pdf-3-whe-10.1177_17455057251406944 for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada by Bluma Kleiner, Carmen H. Logie, Pierre-Paul Tellier, Seerat Chawla, Ashley Lacombe-Duncan, Yasmeen Persad, Lashanda Skerritt, Ann N. Burchell, Mona Loutfy, Angela Kaida and Alexandra de Pokomandy in Women's Health
Supplemental Material
sj-pdf-4-whe-10.1177_17455057251406944 – Supplemental material for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada
Supplemental material, sj-pdf-4-whe-10.1177_17455057251406944 for Disclosure, comfort, and negative experiences with HIV care providers among transgender women living with HIV in Canada: Findings from a prospective cohort study of women living with HIV in Canada by Bluma Kleiner, Carmen H. Logie, Pierre-Paul Tellier, Seerat Chawla, Ashley Lacombe-Duncan, Yasmeen Persad, Lashanda Skerritt, Ann N. Burchell, Mona Loutfy, Angela Kaida and Alexandra de Pokomandy in Women's Health
Footnotes
Acknowledgements
The CHIWOS Research Team would like to thank women living with HIV for their contributions to this study. We also thank the national team of co-investigators, collaborators, and Peer Research Associates and acknowledge the national Steering Committee, our three provincial Community Advisory Boards, the National CHIWOS Aboriginal Advisory Board, and all our partnering organizations for supporting the study. CHIWOS Research Team: Rahma Abdul-Noor (Women’s College Research Institute), Aranka Anema (Harvard Medical School), Jonathan Angel (Ottawa Hospital Research Institute), Dada Mamvula Bakombo (McGill University Health Centre), Fatimatou Barry (Women’s College Research Institute), Greta Bauer (University of Western Ontario), Kerrigan Beaver (Women’s College Research Institute), Marc Boucher (CHU Ste-Justine), Isabelle Boucoiran (CHU Ste-Justine), Jason Brophy (Children’s Hospital of Eastern Ontario), Lori Brotto (University of British Columbia), Ann N. Burchell (St, Michael’s Hospital), Claudette Cardinal (Simon Fraser University), Allison Carter (Kirby Institute), Lynne Cioppa (Women’s College Research Institute), Tracey Conway (Women’s College Research Institute), José Côté (Centre Hospitalier de l’Université de Montréal), Jasmine Cotnam (Canadian Aboriginal AIDS Network), Cori d’Ambrumenil (AIDS Vancouver Island), Janice Dayle (McGill University Health Centre), Erin Ding (British Columbia Centre for Excellence in HIV/AIDS), Danièle Dubuc (McGill University Health Centre), Janice Duddy (Pacific AIDS Network), Mylène Fernet (Université du Québec à Montréal), Annette Fraleigh (Women’s College Research Institute), Peggy Frank (Simon Fraser University), Brenda Gagnier (Women’s College Research Institute), Marilou Gagnon (University of Victoria), Jacqueline Gahagan (Dalhousie University), Claudine Gasingirwa (Women’s College Research Institute), Nada Gataric (British Columbia Centre for Excellence in HIV/AIDS), Rebecca Gormley (British Columbia Centre for Excellence in HIV/AIDS), Saara Greene (McMaster University), Danielle Groleau (McGill University), Charlotte Guerlotté (COCQ-SIDA), Trevor Hart (Ryerson University), Catherine Hankins (McGill University), Emily Heer (Alberta Health Services), Robert S. Hogg (Simon Fraser University), Terry Howard (Glasshouse Consultants), Shazia Islam (Women’s College Research Institute), Joseph Jean-Gilles (GAP-VIES), Hermione Jefferis (AIDS Vancouver Island), Evin Jones (Pacific AIDS Network), Charu Kaushic (McMaster University), Mina Kazemi (Women’s College Research Institute), Mary Kestler (Oak Tree Clinic BCWH), Maxime Kiboyogo (McGill University Health Centre), Marina Klein (McGill University Health Centre), Nadine Kronfli (McGill University Health Centre), Gladys Kwaramba (Women’s College Research Institute), Gary Lacasse (Canadian AIDS Society), Ashley Lacombe-Duncan (University of Michigan), Melanie Lee (Simon Fraser University), Rebecca Lee (CIHR Canadian HIV Trials Network), Jenny Li (British Columbia Centre for Excellence in HIV/AIDS), Viviane Lima (British Columbia Centre for Excellence in HIV/AIDS), Elisa Lloyd-Smith (Vancouver General Hospital), Carmen Logie (University of Toronto), Evelyn Maan (Oak Tree Clinic), Valérie Martel-Lafrenière (Centre Hospitalier de l’Université de Montréal), Carrie Martin (Canadian Aboriginal AIDS Network), Renee Masching (Canadian Aboriginal AIDS Network), Lyne Massie (Université du Québec à Montréal), Melissa Medjuck (formerly of the Positive Women’s Network), Brigitte Ménard (McGill University Health Centre), Cari L. Miller (formerly of Simon Fraser University), Judy Mitchell (Positive Living North), Gerardo Mondragon (British Columbia Centre for Excellence), Deborah Money (Faculty of Medicine at UBC), Ken Monteith (COCQ-SIDA), Marvelous Muchenje (Women’s Health in Women’s Hands CHC), Florida Mukandamutsa (CASM), Mary Ndung’u (African Partnership Against AIDS), Valerie Nicholson (Simon Fraser University), Kelly O’Brien (University of Toronto), Nadia O’Brien (McGill University Health Centre and McGill University), Gina Ogilvie (University of British Columbia), Susanna Ogunnaike-Cooke (Public Health Agency of Canada), Joanne Otis (Université du Québec à Montréal), Rebeccah Parry (Simon Fraser University), Sophie Patterson (Simon Fraser University), Angela Paul (Positive Living North), Doris Peltier (Canadian Aboriginal AIDS Network), Neora Pick (Oak Tree Clinic BCWH), Alie Pierre (McGill University Health Centre), Jeff Powis (Michael Garron Hospital), Karène Proulx-Boucher (McGill University Health Centre), Corinna Quan (Windsor Regional Hospital), Jesleen Rana (Women’s Health in Women’s Hands CHC), Eric Roth (University of Victoria), Danielle Rouleau (Centre Hospitalier de l’Université de Montréal), Geneviève Rouleau (Centre Hospitalier de l’Université de Montréal), Sergio Rueda (Centre for Addiction and Metal Health), Kate Salters (British Columbia Centre for Excellence in HIV/AIDS), Margarite Sanchez (ViVA), Roger Sandre (Haven Clinic), Jacquie Sas (CIHR Canadian HIV Trials Network), Édénia Savoie (McGill University Health Centre), Paul Sereda (British Columbia Centre for Excellence in HIV/AIDS), Stephanie Smith (Women’s College Research Institute), Marcie Summers (formerly of the Positive Women’s Network), Wangari Tharao (Women’s Health in Women’s Hands CHC), Christina Tom (Simon Fraser University), Cécile Tremblay (Centre Hospitalier de l’Université de Montréal), Jason Trigg (British Columbia Centre for Excellence in HIV/AIDS), Sylvie Trottier (Centre Hospitalier Universitaire de Québec), Angela Underhill (Women’s College Research Institute), Anne Wagner (Ryerson University), Sharon Walmsley (University Health Network), Clara Wang (British Columbia Centre for Excellence in HIV/AIDS), Kath Webster (Simon Fraser University), Wendy Wobeser (Queen’s University), Denise Wozniak (Positive Living Society of British Columbia), Mark H. Yudin (St. Michael’s Hospital), Wendy Zhang (British Columbia Centre for Excellence in HIV/AIDS), Julia Zhu (British Columbia Centre for Excellence in HIV/AIDS), and all other CHIWOS Research Team Members who wish to remain anonymous. Alexandra de Pokomandy’s project manager at the Research Institute of the McGill University Health Centre, Sofia Danna, submitted the article.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CHIWOS was funded by the Canadian Institutes of Health Research (CIHR), the CIHR Canadian HIV Trials Network (CTN 262), the Ontario HIV Treatment Network (OHTN), and the Academic Health Science Centres (AHSC) Alternative Funding Plans (AFP) Innovation. ANB and AK received salary support from CIHR. AdP was supported by a salary award (Research Scholar) from the Fonds de recherche du Québec – Santé (FRQ-S). CHL was supported by the Canada Research Chairs Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The de-identified datasets generated and analyzed during the current study are not publicly available as we do not have community or REB approval to do so. Data are available from the Women’s College Research Institute Women and HIV Research Program Data Access Coordinator for researchers and students who meet the criteria for access to confidential data. The current Data Access Coordinator is Angela Underhill, and she can be reached at ![]() ) which includes the requirement that the ICMJE authorship criteria be met by all authors.
) which includes the requirement that the ICMJE authorship criteria be met by all authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.