
Abstract
Transgender and gender-diverse (TGD) persons represent a small but growing population in the United States. Accessing inclusive, equitable, and evidence-based healthcare remains a challenge for this patient population. Many TGD persons seek gender-affirming care, including gender-affirming hormonal therapy (GAHT) and gender-affirming surgery (GAS), to help ameliorate the physical and mental aspects of their gender incongruence. Both GAHT and GAS induce clinically important histopathologic and anatomic changes in breast tissue. Consequently, breast care in TGD persons has become an increasingly recognized topic of importance in gender-affirming care. However, there remains a scarce but growing base of literature specifically addressing the unique healthcare needs of breast care in TGD patients. This article will review how to establish trusting patient–provider relationships for TGD patients, gender inclusivity in breast clinics and imaging centers, the influence of GAHT and GAS on breast tissue, breast cancer screening recommendations and barriers, and breast cancer risk and treatment considerations in TGD persons.
Keywords
Introduction
Over the past decade, a growing percentage of the population self-reports as transgender and gender-diverse (TGD), and currently, approximately 0.5%–1.6% of American adults identify as TGD.1,2 The terminology TGD encompasses individuals whose gender identity is different from the sex they were assigned at birth. It should be noted that sex assigned at birth generally includes female, male, or intersex and is primarily based upon genital anatomy and/or chromosomal makeup. This contrasts with gender identity, consisting of a spectrum with each end of the spectrum representing the gender dichotomy of femininity or masculinity. Persons whose sex assigned at birth is the same as their gender identity are called cisgender.3,4 A glossary of terms is detailed in Table 1. While the authors acknowledge the diversity of the gender spectrum, for the purposes of this review article, when referencing previously published studies, the terminology chosen by the authors in each specific study will be used. TGD persons may receive gender-affirming therapies, such as gender-affirming surgery (GAS) and gender-affirming hormone therapy (GAHT), resulting in improved psychosocial well-being and lower rates of depression and self-harm.5 –7 Notably, gender-affirming therapies can influence the anatomical and histopathologic makeup of a person’s fibroglandular breast tissue.8,9 In this review article, we examine the current data on breast care considerations for TGD persons, highlight topics, and discuss opportunities for future work to guide evidence-based and equitable breast care for persons of all genders.
Gender terminology.

Establishing trusting healthcare relationships
To optimize the patient experience and ensure comfort in the clinical environment, healthcare providers must be trained in culturally sensitive terminology and invested in creating inclusive and gender-affirming environments, all while addressing their personal biases. 10 One of the first steps is correctly using a patient’s personal pronouns and chosen name during patient interactions. Accurately representing and documenting each patient’s gender identity in the electronic medical record and during interprofessional communication is critical. Inconsistencies in patient pronouns and names across team members and records result in medical distrust, patient frustration, and an undue burden to patients to correct and educate healthcare professionals, which only further perpetuates healthcare barriers many TGD persons face. 11 Regarding breast care specifically, medical terminology must be specific and accurate in the medical record, but also inclusive during patient interactions. For example, some transmasculine patients may prefer the term “chest” instead of “breast,” as the latter may feel incongruent with their masculine identity. For many marginalized populations, welcoming and inclusive clinical care environments can help establish trust between patients and providers, subsequently improving the quality of care. 12 Providing gender-neutral intake forms and signage as well as gender-inclusive private and lavatory areas also promotes an inclusive environment for TGD patients. 13
Beyond terminology, providers must endeavor to build trusting partnerships with TGD patients. Strong patient–provider relationships are achieved through the practice of cultural humility, improving TGD representation and visibility in healthcare, and healthcare provider education on gender diversity. 14 In a large-scale national survey, one in three TGD patients reported having a negative interaction with a healthcare provider because of their gender identity, illustrating the importance of improving patient–provider relationships. 15 Cultural humility focuses on healthcare provider self-reflection and self-critique, allowing for continual healthcare provider improvement and individualized patient interactions, consequently improving patient–provider relationships.16,17 Greater reported patient satisfaction and improved health outcomes have been noted when patients from racial minority backgrounds are cared for by a diverse healthcare team.18,19 In keeping with this notion that minority representation matters for patients, it would follow that increasing TGD representation in healthcare would help improve patient–provider relationships for TGD patients.
Lastly, lack of provider education is a commonly cited challenge by both healthcare providers and patients when it comes to optimizing TGD patient–provider interactions.20 –22 It is imperative to implement education cross-professionally and early in the education process. Many medical schools do not have adequate cultural competency interventions, particularly regarding providing care for TGD populations.23,24 Though formal education has not been shown to eliminate transphobic beliefs held by some healthcare providers, it is an important step in eliminating bias toward TGD patients and building successful patient–provider relationships. 25 In summary, to successfully establish trusting healthcare relationships with TGD patients, efforts must be made to utilize inclusive gender-affirming language, promote cultural humility, strengthen healthcare provider education, and increase the representation of TGD people in the medical profession.
Gender inclusivity in breast clinics and imaging centers
The feminization, or “pinkification,” of breast cancer has long been a successful strategy to improve breast cancer screening and awareness for cisgender women, but it has also come to dominate the atmosphere at many breast cancer centers. 26 As a result, the values and expectations of both cisgender men and TGD individuals with breast cancer are not adequately met in these settings. TGD individuals diagnosed with breast cancer are often forced to seek care at facilities named and designed exclusively for women.27,28 A review of 40 breast imaging centers nationally in 2019 found that 15% displayed pink graphics, 12.5% used the term “women’s center,” and none mentioned transgender services on the imaging center site. 28 Cisgender male patients report feeling unwelcomed in these settings, where both other patients and staff question their presence as patients. 29 Individuals who feel their values, expectations, and needs are not accurately represented in patient-centered questionnaires report lower utilization which can lead to worse outcomes overall.30,31 More specifically in breast imaging centers, patient intake forms often are not relevant to persons assigned male sex at birth; for example, questions pertaining to a patient’s last menstrual period. 27
TGD individuals report persistent negative experiences in healthcare settings and commonly report an inability to access gender-affirming spaces or gender-appropriate facilities.15,32 The layout of physician practices and breast care centers has been identified as a significant barrier to care for TGD patients seeking breast care. 33 A 2020 survey of TGD patients, found that 71% of respondents had at least one negative breast imaging encounter. 34 In breast center waiting rooms, 90% of male presenting patients report they experience extreme or severe embarrassment while awaiting care compared to 50% of women. 35 For both cisgender men and transmasculine patients seeking breast care, the stigma of being a non-female presenting individual in the breast care setting has significant negative effects on patient experience and outcomes. 35 Beyond the aesthetics of facilities, the pinkification of breast care can influence providers’ attitudes toward male-presenting patients. Men have reported gendered treatment by members of the care team and even “being treated as a woman,” a phenomenon that can be particularly damaging for transmasculine patients.29,36 A 2018 survey of breast imaging facilities found that most facilities (78.5%) had gender-neutral patient bathrooms; however, 22% had physical spaces with dominant pink hues and 26% of intake forms automatically populated with female phrases/pronouns. 37 Considering these reported pitfalls, breast clinics and breast imaging centers can improve gender inclusivity by creating gender-neutral physical spaces, deemphasizing the feminine association with breast cancer, and utilizing gender-inclusive patient intake forms.
Breast considerations and gender-affirming hormone therapy
Mammary tissue development is similar in prepubertal males and females. During typical puberty in cisgender girls, further breast development occurs under the influence of estrogen with the formation of ducts, lobules, and acini. 38 For cisgender boys, further mammary development is arrested during typical puberty under the influence of testosterone. 39 In the mature male breast, only primitive ducts, stromal elements, and fat tissue are typically observed. 40 Due to the differing mammary structures between mature cisgender males and females, the incidence of benign and malignant breast pathology occurring in each group is substantially different.
GAHT is a critical aspect of medical gender affirmation for many TGD individuals, with approximately 98% of respondents on GAHT in the 2022 US Transgender Survey reporting that they were “a little or a lot more satisfied” with their life on GAHT. 41 Feminizing GAHT induces the development of female sex characteristics, which includes breast development, and reduces male secondary sex characteristics.8,42 A standard feminizing GAHT regimen includes estrogen (estradiol) and often an antiandrogen (most commonly spironolactone) to suppress endogenous testosterone. Other less commonly used antiandrogens include finasteride, cyproterone acetate, and gonadotropin-releasing hormone agonists.42,43 Despite limited studies on the role of progesterone in feminizing GAHT regimens, some patients and providers have noted anecdotal improvements in breast development, mood, and libido when including progesterone as part of their feminizing hormone therapy.42,44 Breast development begins 3–6 months after the initiation of feminizing GAHT with full effect within 2–3 years. 45 However, the degree of breast development is heterogeneous among TGD persons on estradiol. 46 And, most patients are unlikely to achieve Tanner stage V breast development despite adequate GAHT regimens.47,48 The heterogeneity of breast tissue development is theorized to be secondary to a combination of genetic and epigenetic breast tissue hormone responsiveness and variations in GAHT regimens.46,49 Despite the variable degree of breast development amongst TGD persons assigned male at birth (TGD AMB), feminizing GAHT with estrogen will result in breast tissue parenchyma which is histologically identical to cisgender females including the formation of ducts, lobules, and acini, and therefore should not be referred to as gynecomastia. 50 Consequently, TGD AMB persons on feminizing GAHT can present with a diverse array of both benign and malignant breast pathology rarely seen in cisgender men and commonly demonstrated in cisgender women.51,52
Masculinizing GAHT primarily utilizes testosterone which induces male secondary sex characteristics and reduces female secondary sex characteristics. 42 Progestins may also be used to reduce menses. Serum testosterone levels in the mid-to-normal male range and serum estradiol levels in the post-menopausal female range are typically observed for TGD individuals assigned female at birth (TGD AFB) on masculinizing GAHT. 45 Serum estradiol levels may stay elevated above the normal male range due to peripheral aromatization of circulating testosterone. 53 Reduced glandular tissue and increased fibrous connective tissue have been observed in TGD individuals on long-term androgens, similar to that of post-menopausal women.54 –57 However, fibrocystic changes often observed in post-menopausal women are rarely seen in TGD individuals on testosterone. 54 Additionally, a recent study examined 314 breast specimens from transgender men on testosterone who had undergone gender-affirming chest masculinization surgery. The breast specimens demonstrated decreased lobular density, a higher degree of lobular atrophy, and a lower incidence of cysts, apocrine metaplasia, calcifications, columnar cell change, and atypia compared to cisgender women. 56
Breast considerations and gender-affirming top surgery
The number of TGD persons seeking gender-affirming operations has significantly increased in the setting of a growing population of TGD individuals and improved insurance coverage following the implementation of the Affordable Care Act in 2016.58 –60 The most commonly performed gender-affirming operations are gender-affirming breast/chest surgery, colloquially called “top surgery.” 59 Top surgery in persons assigned female or intersex at birth who have breasts is called “gender-affirming chest masculinization surgery (GACMS)” or sometimes “gender-affirming mastectomy.”12,61,62 Persons assigned male or intersex at birth who desire a chest with breasts may choose to undergo breast augmentation, usually with breast implant placement. 63 In this section, we discuss healthcare provider and patient considerations for persons who undergo either GACMS or gender-affirming breast augmentation.
Gender-affirming chest masculinization surgery
The most commonly performed GAS in TGD AFB persons is GACMS. 59 In this operation, most of the fibroglandular breast tissue is removed along with reduction of the skin envelope to give the chest a masculine and/or flat appearance (Figure 1). This can often be done with preservation of the nipple–areolar complex which may be reduced in size or shape at the time of surgery to provide balance between the skin to nipple–areolar complex ratio.64,65 Emerging data suggest that the amount of fibroglandular breast tissue removed at the time of GACMS varies between surgeons and between patients and that the amount left behind or surgically removed is largely dependent upon the patient’s body habitus to preserve an anatomically desirable chest contour.12,62 Thus, GACMS is not generally considered to be equivalent to oncologic risk-reducing mastectomies, which aim to remove as much breast tissue as possible to maximally reduce future breast cancer risk.12,66,67

Examples of gender-affirming top surgery. Before (a) and after (b) chest masculinization surgery. Before (c) and after (d) breast augmentation.
TGD persons considering GACMS should be counseled that while it may decrease a person’s risk for breast cancer, it does not completely negate the risk for future breast cancer development.61,66,68,69 Therefore, surgeons should consider performing a breast cancer risk assessment using validated tools such as the Gail and Tyrer–Cuzick models and consider genetic counseling with possible genetic testing for a pathogenic germline variant for those persons with a history suggestive of a hereditary cancer syndrome.70 –72 Understanding future breast cancer risk is imperative to support patients in their decision for GACMS or to undergo oncologic risk-reducing mastectomies. 66 A recent study demonstrated the majority of TGD AFB patients who were considering GACMS and found to be at an elevated risk for breast cancer decided to move forward with oncologic risk-reducing mastectomies rather than GACMS alone signifying how an individual’s breast cancer risk can guide their decision. 73 Additionally, TGD AFB persons who decide to undergo oncologic risk-reducing mastectomies should be aware that current guidelines recommend routine chest examination to detect breast cancer development along the chest wall or skin flap, but no routine imaging is currently recommended at this time.74 –76
Whether TGD persons undergo GACMS or oncologic risk-reducing mastectomies, it is imperative that all tissue removed at the time of surgery be appropriately oriented and undergo full pathological examination. Retrospective cohort studies have identified that atypical breast lesions have been found in GACMS tissue specimens, even if patients have been on gender-affirming testosterone therapy, which may increase the risk for future breast cancer development if residual fibroglandular breast tissue is left behind after GACMS.57,77,78 While rare, there are incidences of ductal carcinoma in situ or early-stage breast cancer incidentally identified on surgical pathology after GACMS.57,79 Because of these findings, it is essential that all persons who meet current breast cancer screening guidelines undergo screening imaging prior to GACMS to ensure the correct operation and treatment are provided to patients.80,81 If an incidental cancer is found at GACMS, current care for cisgender patients applies and additional surgery may include completion mastectomy to obtain negative margins and surgical axillary nodal staging. 82
Gender-affirming breast augmentation
Gender-affirming breast augmentation is often desired by transfeminine individuals, most commonly due to insufficient breast development with feminizing GAHT alone. 52 Breast augmentation is typically performed with the placement of bilateral silicone or saline implants either posterior (retropectoral) or anterior (prepectoral) to the pectoralis musculature (Figure 1). Most recent estimates suggest approximately 60%–80% of transgender women consider or undergo breast augmentation.44,52 Although most are satisfied with their results, 33% reported health complaints attributed to breast implants. 52 Imaging evaluation of breast implants in TGD individuals is identical to that of cisgender women. 83 Evaluation for silicone implant rupture can be performed with breast ultrasonography or breast magnetic resonance imaging (MRI). Although saline implant rupture is typically diagnosed clinically based on physical signs, diagnostic breast imaging can be performed if clinical exam findings are inconclusive. 84 Patients with silicone breast implants should undergo breast MRI surveillance starting 5–6 years after implantation and then every 2–3 years thereafter to exclude rupture. 85 Furthermore, clinicians and patients should be aware that textured implants are specifically associated with breast implant-associated large cell lymphoma (BIA-ALCL), a non-Hodgkin lymphoma, and several case reports of BIA-ALCL have been reported in TGD persons.86 –89
Historically, TGD individuals have often sought gender-affirming care outside of the established medical system. Although prohibited in the United States, some TGD AMB individuals may undergo breast augmentation with free injection of particles or fillers such as silicone, liquid paraffin mineral oil, and polyacrylamide hydrogel.90,91 TGD individuals injected with free particles may develop mastodynia, palpable lumps, contour deformity, and skin changes including induration and hyperpigmentation.90,92 Free particle injections have been noted to result in granulomas and fibrosis, obscuring normal breast parenchyma on mammography and breast ultrasonography, and consequently potentially masking an underlying malignancy. 93 Therefore, for this group of patients, breast MRI is helpful for the detection of malignancy, which can be more easily differentiated from free silicone based on specific imaging enhancement and signal characteristics.94,95
Breast cancer screening considerations
Breast cancer is one of the most common malignancies in the United States. Approximately 12.9% of cisgender women and 0.13% of cisgender men will develop breast cancer during their lifetime. 96 The lifetime risk of breast cancer in TGD individuals is not known as there have been no comprehensive prospective longitudinal studies in this population and the influence of GAHT and gender-affirming chest reconstruction on breast cancer development is poorly understood. Screening mammography is considered the gold standard breast cancer screening modality by the United States Preventive Services Task Force (USPSTF), the American Cancer Society (ACS), and the American College of Radiology, requiring screening coverage by insurance providers under US federal law. However, neither the USPSTF nor ACS have produced breast cancer screening guidelines for TGD individuals as of 2024. Likely secondary to a lack of clear guidelines, recent studies have demonstrated lower breast cancer screening rates of TGD individuals compared to cisgender women.97 –99
The current limited evidence base regarding the incidence and characteristics of breast cancer for TGD individuals on estrogen therapy is slowly growing. Although the incidence of breast cancer for TGD individuals is unknown, it likely lies between that of cisgender men and women. Most data on breast cancer in TGD is based on case reports and case series; however, three cohort studies from the past decade offer some insight into breast cancer in TGD persons. Data from the American College of Surgeons’ National Cancer Database (NCDB) identified 35 TGD patients from a cohort of nearly 12 million persons from 2003 to 2016. 100 The NCDB cohort data did not identify a difference in stage at diagnosis or survival; however, given their small cohort of TGD persons with breast cancer, 95% confidence intervals were quite wide and limited the statistical interpretation of their findings. 100 A cohort study of over 5,000 TGD individuals in the Veterans Administration Hospital System found only 10 TGD breast cancer patients; however, the authors think that many patients were missed, given documenting errors and the culture within their hospital system throughout the cohort. 101 de Blok et al. examined a cohort of 2,260 transgender women and 1,229 transgender men in the Netherlands who received GAHT from a retrospective national dataset. 52 This retrospective cohort study calculated the incidence of invasive and non-invasive breast cancers and notably found a 46-fold higher risk of breast cancer in transgender women compared to cisgender men, but a 0.3-fold lower rate compared to cisgender women. 52 In transgender men, the incidence of invasive breast cancer was lower (0.2 standardized incidence ratio) compared to cisgender women, but higher compared to cisgender men. 52 Also, of note in this study, the median age of breast cancer diagnosis was lower compared to cisgender women and a higher-than-expected proportion of breast cancers in transgender women displayed HER2 receptor status. However, given the homogenous patient population (>90% White and average weight), the applicability of these findings to other populations is unclear.
Despite limited data in this patient demographic, there have been several breast cancer screening guidelines published for TGD patients, relying upon expert consensus, retrospective cohort studies, and extrapolation from cisgender populations. Consequently, there is variation in breast cancer screening recommendations amongst the organizations with published guidelines. Multiple health care organizations including the American College of Radiology, University of California San Francisco, World Professional Association of Transgender Health, Fenway Health, the Endocrine Society, and the International Journal of Gynecologic Cancer have published breast cancer screening recommendations for TGD patients.42,83,102 –105 These recommendations are detailed in Tables 2 and 3. Despite slight variations in recommendations from each organization, several common themes emerge from the guidelines summarized below:
Transgender women at average risk of breast cancer with ⩾5 years of GAHT should follow the same local screening recommendations as cisgender women.
Transgender women at average risk of breast cancer with <5 years of GAHT should not undergo routine screening mammography.
Transgender men without GACMS should follow the same local screening recommendation as cisgender women based on their personal risk profile.
Transgender men who have undergone GACMS should consider annual physical chest exams. Screening mammography is not routinely recommended at this time.
Selected breast cancer screening recommendations for transgender women.

WPATH: World Professional Association of Transgender Health; UCSF: University of California San Francisco; TGD: transgender and gender-diverse; BC: breast cancer; GAHT: gender-affirming hormone therapy.
Selected breast cancer screening recommendations for transgender men.
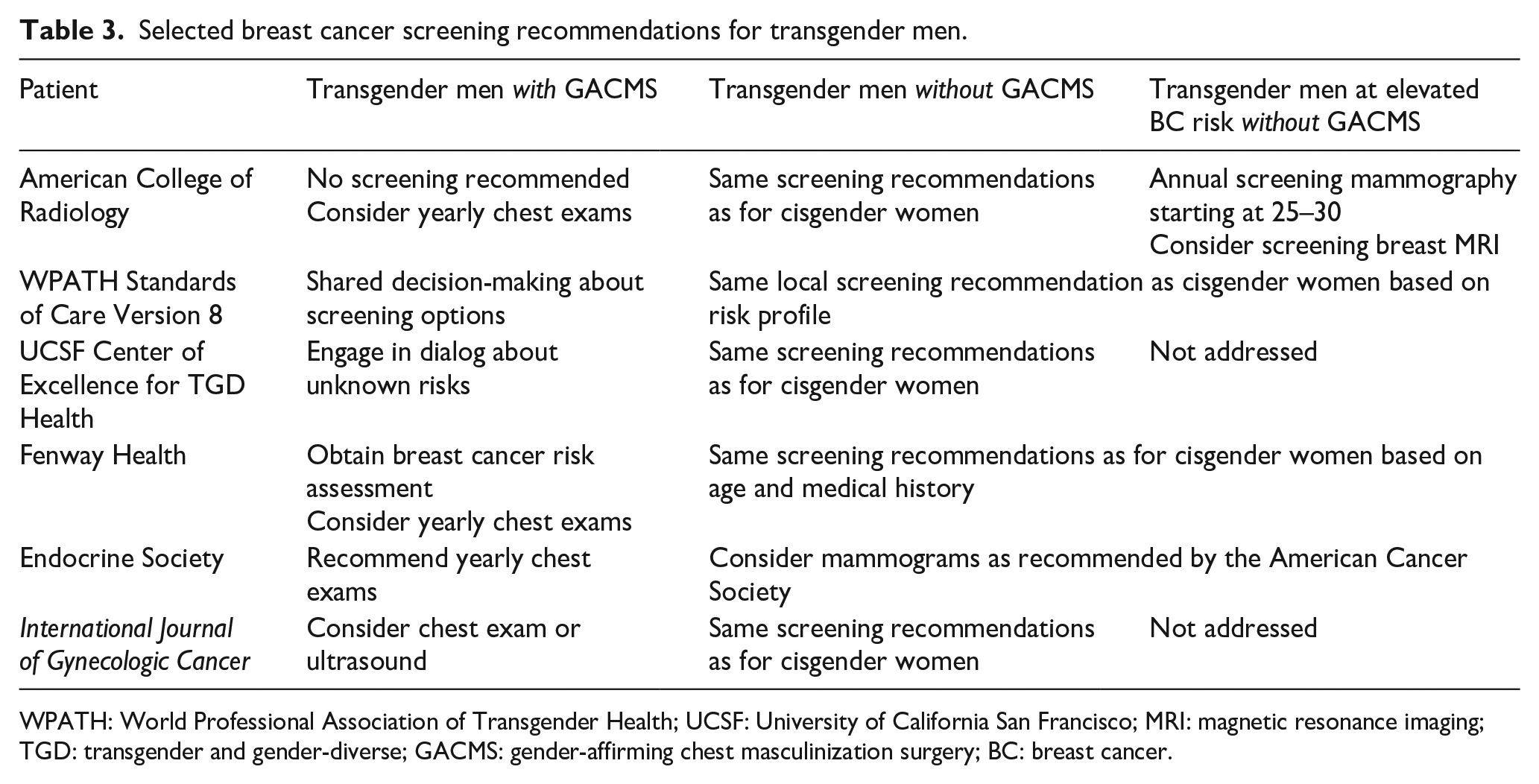
WPATH: World Professional Association of Transgender Health; UCSF: University of California San Francisco; MRI: magnetic resonance imaging; TGD: transgender and gender-diverse; GACMS: gender-affirming chest masculinization surgery; BC: breast cancer.
Multiple barriers to accessing screening mammography exist for TGD persons. While a third of TGD persons report concern regarding breast cancer development, many are unaware of their risk and screening options, or what are considered best practices.106,107 Many lack access to adequate health insurance and for those who are insured, only a small percentage of United States insurance policies provide gender neutral and/or inclusive screening mammography coverage. 108 A lack of provider knowledge regarding breast cancer screening recommendations for TGD patients also likely contributes to TGD breast cancer disparities. A recent survey of primary care practitioners found only 35% of respondents were aware of breast cancer screening recommendations for TGD patients. 109 Another survey of breast imaging radiology practices found that only 33% followed screening recommendations for transgender women on GAHT. 110 And lastly, many TGD patients endorse negative imaging encounters when undergoing screening. More specifically, a 2019 survey of TGD patients found that 33% reported unexpected emotional discomfort with mammography exams and 49% with ultrasound exams, which comprise the bulk of breast cancer screening imaging services. 34
Breast cancer treatment considerations
While breast cancer is one of the most common cancers seen in cisgender women, there is limited published data on breast cancer risk and outcomes in TGD persons, largely due to historic societal marginalization leading to a lack of self-reporting gender and lack of gender data collection in tumor registries, cohort studies, and clinical trials.111 –115 For TGD AFB persons who develop breast cancer, the decision for breast-conserving surgery versus mastectomy, with or without post-mastectomy breast reconstruction, is impacted by gender identity. A single-institution cohort study recently identified that transgender men more frequently choose to undergo mastectomy without post-mastectomy breast reconstruction compared to cisgender women. 116 Thus, surgeons should be mindful of discussing all options with TGD persons who develop breast cancer and work with plastic surgeons and other team members to ensure that the surgical breast cancer team supports the patient’s gender identity, including how adjuvant radiation therapy may alter physical appearance and cosmetic outcomes.
Perhaps the most significant, but least studied area of breast cancer treatment in TGD persons is how GAHT may influence locoregional and/or distant recurrent for estrogen receptor (ER) and/or progesterone receptor (PR) positive breast cancer—particularly amongst transfeminine persons on GAHT with estrogen. Standard treatment for ER and/or PR-positive breast cancer entails 5–10 years of endocrine therapy, which depletes an individuals’ endogenous levels of estrogen and progesterone. 82 This is typically with tamoxifen for men and premenopausal women or aromatase inhibitors for post-menopausal women. Thus, for TGD persons on GAHT with estrogen and/or progesterone, with ER and/or PR-positive breast cancer, the current consensus is to consider stopping GAHT given the potential for hormones to stimulate tumor regrowth and/or spread. Similarly, many breast cancers express the androgen receptor (AR), which is stimulated by testosterone, and thus testing for this receptor may be considered for TGD persons on gender-affirming testosterone. 117 Also of note, testosterone can be aromatized to estradiol, which could have an impact on ER+ cancers as well. Again, while no outcome data exists, it is reasonable to consider stopping testosterone therapy given the potential risk of breast cancer recurrence. However, the benefit of stopping GAHT for TGD patients with an ER, PR, and/or AR positive breast cancer must be balanced with the risk of negatively impacting the patient’s mental well-being and neuroendocrine function, particularly in TGD patients who have undergone gonadectomy with minimal endogenous sex hormone production. Recent survey data did find that 30% of TGD persons reported they would not be willing to consider stopping gender-affirming therapy if they were to develop a hormone-receptor positive breast cancer which highlights future opportunities for research on outcomes. 107
Study limitations
PubMed was the primary search engine for research in this publication, which allowed for a comprehensive review of breast care considerations in TGD persons. Literature not found in PubMed may not have been included and is one source of bias and limitation to this study. Overall, there is limited knowledge regarding breast care and breast cancer in TGD persons, creating an opportunity for more research to be conducted.
Conclusion
Breast care considerations for TGD persons is an increasingly recognized important topic of inquiry in gender-affirming care. Both GAHT and gender-affirming top surgery can substantially impact the risk of breast cancer in TGD individuals. Consequently, it is critical to understand both the histopathologic and anatomic considerations of these gender-affirming interventions to better inform breast cancer risk, optimize breast cancer screening recommendations, and improve breast cancer treatment outcomes for this historically marginalized patient population. Achieving these goals will not be possible unless an inclusive healthcare environment and trusting patient–provider relationships are adequately maintained by utilizing gender-affirming language, promoting cultural humility, strengthening healthcare provider education, and increasing TGD representation in healthcare. Although the body of evidence pertaining to breast cancer in TGD patients is slowly growing, there remain many unanswered questions and future opportunities for further investigation: In transfeminine persons, a deeper understanding of how estradiol dose, duration of treatment, and progesterone use affects breast cancer risk; in transmasculine persons, a better assessment of breast cancer risk after GACMS; and for all TGD persons, further investigation into high-risk individuals (BRCA 1/2 mutation, strong family history of breast cancer, etc.), taking into account GAHT and gender-affirming top surgery, is urgently needed.