
Abstract
Background:
Menstrual cycles are a natural part of many people’s health, yet are subject to stigma and misinformation, which can affect the experience of menstrual-related symptoms and overall well-being.
Objectives:
The study explored how perceptions of the menstrual cycle are associated with symptom severity and their impact on daily life, including work, social activities, and intimate relationships.
Design:
A cross-sectional observational study.
Methods:
An anonymised online survey, distributed through social media, email, and newsletters. Participants aged 18 and older who menstruated in the previous 12 months were included. Demographic data, menstrual cycle characteristics, and self-reported symptom severity were collected. Perceptions of menstruation were measured using a 5-point Likert scale. Nonparametric statistical tests, including Kruskal–Wallis, chi-square, and Spearman’s rank-order correlation, were used for data analysis.
Results:
In total, 4735 responses were included in the analysis. Positive perceptions of menstruation were associated with lower reported pain levels and reduced disruption to daily activities, including work and academic performance. Notably, 90.71% reported that menstrual symptoms disrupted their work, with 31.8% taking time off in the past 12 months. Intimate relationships were affected for 84.31% of participants, with significant correlations between comfort in seeking support from partners and the disruption of intimacy (rs(8) = −0.117; p < 0.001). Participants who viewed menstruation positively experienced fewer mental health symptoms, such as depression and anxiety, compared to those with negative perceptions. The study found that positive perceptions of the menstrual cycle were associated with less severe symptoms and a reduced impact on daily activities.
Conclusions:
The findings suggest an association between menstrual perceptions in shaping the experience of symptoms and their broader psychosocial impacts. Enhancing menstrual health literacy and promoting positive perceptions could improve individual health outcomes and societal attitudes. Future public health policies should integrate menstrual health education and supportive workplace policies to enhance the quality of life for those who menstruate.
Registration:
Not applicable.
Introduction
Over the course of a lifetime, a woman will experience ~450 menstrual cycles. 1 This complex physiological process prepares the female body for a potential pregnancy and repeats on average every 28 days. 2 However, menstrual cycles are subject to both inter- and intra-person variability, which affects both the cycle length and symptoms.3–5
Menstrual health is defined as complete physical, mental, and social well-being in relation to the menstrual cycle. 6 This definition emphasises that the menstrual cycle is more than just a biological process, but something that can significantly influence various aspects of health, well-being, and daily life,7–9 and many suggest the menstrual cycle should be considered a vital sign of overall health.10,11 While the menstrual cycle affects health, it can also be disrupted by environmental and lifestyle factors such as stress, nutrition, exercise, and sleep.12–16 Physical health aspects impacted by the menstrual cycle include pain, 9 abnormal uterine bleeding,7,17 and unpredictable cycles, 18 all of which are known to affect daily activities and quality of life.5,7,17–19 Menstrual-related conditions, like endometriosis and polycystic ovary syndrome (PCOS), can further impact quality of life.20,21 Individuals with endometriosis, for instance, frequently experience debilitating pelvic pain, fatigue, and gastrointestinal issues, all of which can reduce their ability to participate in work, social activities, and exercise.20,21 Similarly, PCOS can lead to irregular periods, infertility, weight gain, and increased risk of metabolic disorders, further affecting physical health and self-esteem.20,21 Additionally, the menstrual cycle affects mental well-being, contributing to mood, cognitive function,22,23 premenstrual syndrome, and premenstrual dysphoric disorder, which involve symptoms such as mood swings, irritability, and depression.24–26 These symptoms can interfere with day-to-day activities, leading to reduced participation in exercise, 27 diminished academic or professional performance,28–30 and withdrawal from social activities, 31 with a total estimated health burden equal to 3.835 years of disability adjusted life years. 32 Research also shows that certain phases of the menstrual cycle may exacerbate underlying psychological conditions or emotional distress, further illustrating the close interplay between mental health and menstrual experiences. 33
Despite the universality of the menstrual cycle for women, it is subject to stigma and harmful norms, which often delay or prevent women from seeking support, which in turn can cause worsening of symptoms.34–36 Perceptions of menstruation are shaped by culture,37,38 education, 39 and personal experiences6,28,40 and can influence an individual’s experience of their own cycle. Munro et al. 41 found that both positive and negative perceptions affected students’ confidence in managing their cycle. Similarly, Kennett et al. found that college students with positive perceptions and better coping strategies were more likely to maintain daily activities, despite intense menstrual symptoms, compared to those with negative perceptions. 42 Furthermore, it was shown that women reported reduced premenstrual cycle symptoms when enrolled in peer support programmes aimed at positively framing their perception of the menstrual cycle. 43
Studying the relationship between the perception of, and the experience of the menstrual cycle, addresses not only the physical element but also examines both the psychological and social aspects of menstrual health. Understanding this relationship could therefore provide valuable insights for improved health outcomes at an individual level, and potentially enhance health policy and interventions at a public health level, ultimately leading to improved management strategies and better quality of life.
This study aims to explore the association between perception of the menstrual cycle and how women experience it, including its impact on daily life. We assess how different attitudes towards menstruation correlate with physical and mental symptoms associated with the cycle, and how it interferes with social, intimate, and occupational activities. Through this research, we hope to better inform public health and education that promote a healthier, more integrated approach to managing the menstrual cycle.
Methods
Study aim
The primary aim of the study was to investigate whether perceptions of the menstrual cycle are associated with the severity of menstrual symptoms. The study also investigated if perception and understanding of the menstrual cycle were associated with the level of disruption their symptoms caused to their work and employment, social activities, and intimate relationships.
Design and setting
This study is a cross-sectional observational study, conducted through an anonymised online survey. The survey was created using Qualtrics and distributed on multiple channels to maximise reach, including the social media, email subscriber list, and newsletter of The Food Medic, a health education platform with global reach. It remained open for 2 weeks between March and April 2024. No formal power analysis was conducted prior to data collection, as this was an exploratory cross-sectional study.
Prior to giving consent, participants were asked to read a participant information sheet. To be eligible for the study, participants must be aged 18 years or older, have menstruated in the previous 12 months, and have given their consent to participate. Women who were currently pregnant were excluded from the study. Incomplete survey responses were excluded from the final analysis.
Survey design
The questionnaire was purpose-designed, as existing validated tools did not fully capture the multidimensional constructs we aimed to measure, including to comprehensively assess menstrual symptom severity, perceived impact on quality of life, employment/study, intimate relationships, and attitudes towards menstruation. However, the design of the survey was informed by established literature, clinical experience, and previously validated instruments, including the Menstrual Symptom Questionnaire (MSQ) 44 and the Menstrual Attitude Questionnaire (MAQ), 45 which guided the development of sections related to symptom severity, perception, and psychosocial impact. The final questionnaire was reviewed internally for content relevance and clarity prior to deployment.
Data collection
The survey collected demographic information, including gender identity, educational background, general health status, and country of residence. Menstrual cycle characteristics and history of reproductive health conditions were also recorded. Severity of symptoms were rated on a scale of 1–10 and values were described as follows: 1–2 = very mild (barely noticeable); 3–4 = mild (noticeable but can be ignored much of the time); 5–6 = moderate (distracting and cannot ignore for more than a few minutes); 7–8 = severe (distressing and significantly interferes with most daily activities. Concentration and task performance are considerably affected); 9–10 = very severe (intense and debilitating, unable to perform almost all activities).
+++Perceptions and attitudes towards the menstrual cycle were assessed using a five-point Likert scale. Central tendency of Likert data was determined using the median.
Participants were grouped into three categories based on their perceptions of menstruation, categorised as having positive, neutral, or negative perceptions, based on their responses to a series of positively and negatively framed Likert-scale items. This classification was used to explore associations with symptom severity and psychosocial outcomes.
Other variables such as general health, diagnosis status, and menstrual cycle history were collected using multiple-choice or categorical response formats. Participants were asked to self-rate their current knowledge of the menstrual cycle using a single-item question: “How would you rate the quality of education or information you have about the menstrual cycle now?” Additionally, they completed a five-item multiple-choice quiz designed to objectively assess menstrual cycle knowledge. Each correct answer was awarded one point, yielding a total score out of five. Knowledge levels were categorised as follows: 0–1 = poor knowledge, 2–3 = some knowledge, and 4–5 = good knowledge.
A copy of the complete questionnaire is included in the Supplemental Material.
Statistical analysis
Nonparametric tests were selected as the most appropriate approach for this analysis due to the non-normal distribution of the data and the ordinal nature of several key variables. A Kruskal–Wallis test was used to determine pain differences across different perception groups due to the sample size. Associations between categorical variables were examined using chi-square tests, and the effect size of significant associations was measured with Cramer’s V. A Spearman’s rank order correlation was used to evaluate relationships between ordinal variables, including data derived from five-point Likert scale items. Mean ± SD is reported. A p value of 0.05 was considered significant. Analysis was carried out using BMI SPSS (version 29.0.2.0).
Reporting standards
Reporting of this cross-sectional study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational research. 46 The completed STROBE checklist has been included as Supplemental Material.
Ethics approval and consent to participate
This study was reviewed and approved by an internal ethics review board (ref. FMRERB/2025/001) for ethical compliance and conducted in adherence to internationally recognised ethical and legal standards, including the principles of the Declaration of Helsinki. All participants were presented with a detailed information sheet outlining the study’s purpose, procedures, potential risks and benefits, data handling, and confidentiality. Informed electronic consent was obtained through a series of questions confirming eligibility, understanding, voluntary participation, and agreement for their anonymised responses to be used in research publications. No personally identifiable information was collected, and all data were fully anonymised and handled in accordance with the General Data Protection Regulation (GDPR).
Results
Demographics and participant characteristics
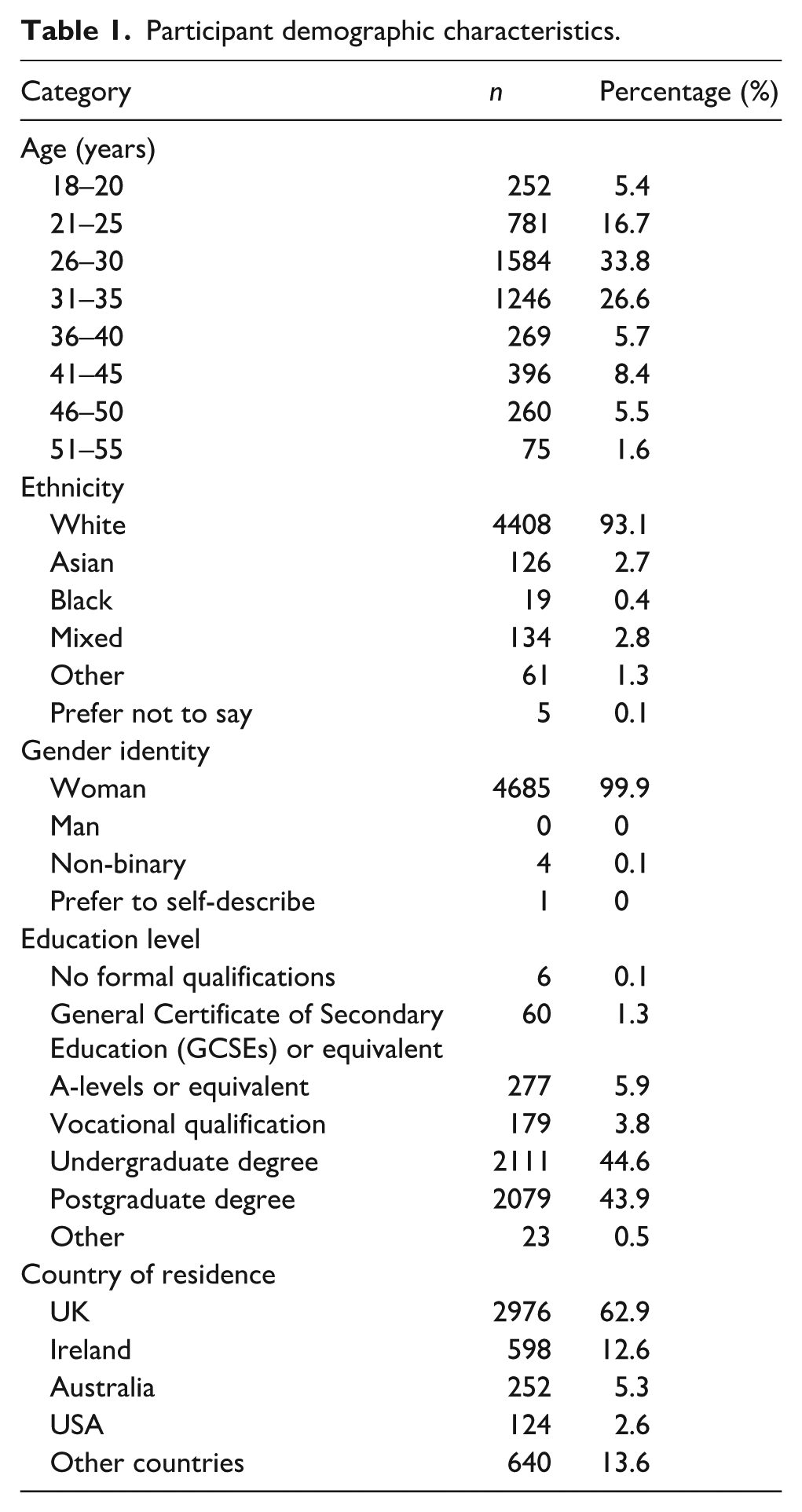
There were 6446 responses to the survey, 1711 of which were incomplete and therefore excluded, leaving a total of 4735 responses in the final analysis. The majority of participants were between the ages of 21 and 35, with the largest groups being 26–30 (n = 1584) and 31–35 (n = 1246). The sample included a diversity of ethnic groups and was predominantly White (93.1%), followed by mixed ethnicity (2.8%), Asian (2.7%), Black/African/Caribbean (0.4%), and other (1.3%). Almost all (n = 4685; 99.9%) of respondents identified as women; the remainder identified as non-binary or transgender male. The majority of participants identified as heterosexual (93.1%) or bisexual (5.1%). Just over three-quarters of participants were in a relationship (46.7%) or married (29.9%). The remainder were single (21.6%) or undisclosed. The educational background of participants was highly skewed towards higher education with 44.6% holding an undergraduate university degree and 43.9% holding a postgraduate degree, 3.8% held a higher diploma, and the remainder held a school degree (7.1%) or was undisclosed (0.6%). Participant demographics are outlined in Table 1.
Participant demographic characteristics.
Menstrual cycle characteristics and pre-existing health conditions
The median age of menarche was 12 years old (n = 1223; 25.8%). Cycle lengths were reported as regular (between 21 and 35 days) by 3709 participants (78.3%), short and irregular (<21 days) by 129 (2.7%), and long and irregular (more than 35 days) by 425 (9.0%). In total, 406 participants (8.6%) described their menstrual cycle regularity as being managed by their use of contraception. Menstrual flow was described as moderate by 49.6% of participants, while 38.5% described their bleeding as heavy.
About 67.4% of participants had no medical history of reproductive health conditions. However, 10.6% had a previous diagnosis of PCOS and 5.6% had endometriosis. A full breakdown of previous diagnoses can be found in Table 2. Menstrual cramps were common, affecting 57.3% (n = 2715) of participants every cycle, 29.8% (n = 1413) some cycles, and the remainder experiencing cramps rarely (11.0%; n = 521) or never (1.8%; n = 86). The median pain score for cramps was 6.7 (SD ± 2.2). The most commonly reported symptom was bloating, affecting 96.92% (n = 4589) of participants, and 13.2% (n = 606) reported that it interferes with daily activities and considerably affects task performance (Figure 1).
Respondents with previous diagnoses.
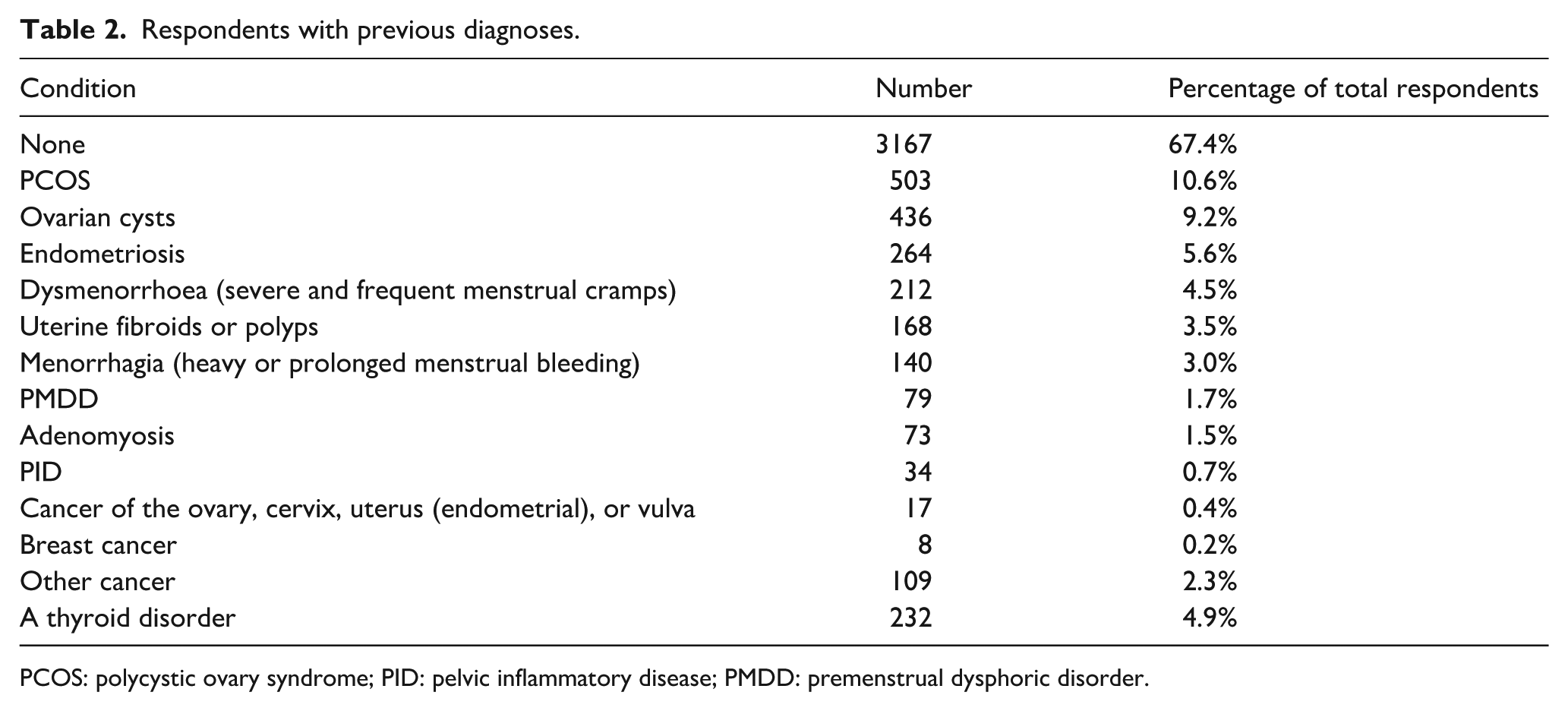
PCOS: polycystic ovary syndrome; PID: pelvic inflammatory disease; PMDD: premenstrual dysphoric disorder.

Frequency and severity of menstrual cycle related symptoms.
The most commonly reported psychological symptom was irritability, reported by 95.63% (n = 4528), 20.8% of which reported it interferes with daily activities and considerably affects task performance. Figure 1 shows the frequency and severity of all menstrual-related symptoms. The level of disruption to daily activity is also described.
Perceptions summary
The survey results on perceptions and attitudes towards menstruation are detailed in Figure 2. The central tendency was to strongly agree that menstruation is viewed as a natural aspect of life. There was a central tendency to agree that menstruation acts as a bothersome interruption in daily life and negatively affects mood and behaviour. Conversely, the majority strongly disagreed with the statement that menstruation is a taboo subject but also strongly disagreed with the idea that education about menstruation is adequate.

Perceptions and attitudes towards menstruation.
Symptom management
For pain management, most respondents (81.8%; n = 3875) used over-the-counter pain relief, while 67.8% (n = 3210) used heat therapy. Other reported methods include physical exercise (47.7%; n = 2258), relaxation techniques (e.g. meditation, deep breathing; 20.2%; n = 955), dietary changes or supplements (17.7%; n = 840), herbal remedies or supplements (9.9%; n = 468), prescription medication (9.8%; n = 464), or other (3.4%; n = 162).
A Spearman’s rank-order correlation was used to determine whether participants who felt more comfortable seeking support from healthcare professionals reported higher satisfaction with the support they received and greater satisfaction with their current symptom management strategies. There was a positive correlation between comfort in seeking support from healthcare professionals and satisfaction with the support received, which was statistically significant (rs(8) = 0.640, p < 0.001). There was also a positive correlation between comfort in seeking support and satisfaction with management strategies (rs(8) = 0.215, p < 0.001). Furthermore, participants who are most comfortable seeking support from healthcare professionals reported lower mean disruption from symptoms than those who felt least comfortable, respectively, for headaches (2.27 ± 1.25 versus 2.45 ± 1.21 ; p = 0.15), back pain ( 2.03 ± 1.10 versus 2.47 ± 1.27; p < 0.001), pelvic pain (2.32 ± 1.24 versus 2.66 ± 1.37; p = 0.001), diarrhoea (2.00 ± 1.14 versus 2.19 ± 1.19; p = 0.011), leg pain (1.93 ± 1.11 versus 2.23 ± 1.28; p = 0.046), decreased sleep quality (2.45 ± 1.26 versus 2.81 ± 1.27; p < 0.001), irritability (2.43 ± 1.21 versus 2.73 ± 1.24; p < 0.001), mood changes (2.48 ± 1.29 versus 2.80 ± 1.26; p < 0.001), anxiety (2.69 ± 1.32 versus 2.86 ± 1.30; p = 0.028), low mood (2.48 ± 1.28 versus 2.80 ± 1.30; p < 0.001), depression (2.29 ± 1.33 versus 2.70 ± 1.39; p < 0.001), fatigue (2.76 ± 1.29 versus 3.15 ± 1.23; p < 0.001), concentration difficulty (2.60 ± 1.27 versus 2.83 ± 1.26; p = 0.008), feeling overwhelmed (2.48 ± 1.28 versus 2.85 ± 1.31; p < 0.001), and tearfulness (2.25 ± 1.28 versus 2.50 ± 1.36; p = 0.004).
Lastly, participants who viewed menstruation as a positive aspect of their life rated their period pain 18% lower (5.74 ± 2.29 versus 6.98 ± 2.13; p < 0.001) than those who do not view menstruation as a positive aspect of their lives.
Mental health impact
A large majority report mental health symptoms in relation to their menstrual cycle, which is detailed in Figure 1. Participants who agreed with statements that framed the menstrual cycle negatively reported more mental health symptoms than those with who disagreed with the same statements. On the other hand, participants who agreed that they feel empowered by their menstrual cycle, experience significantly less severe symptoms during menstruation compared to those who disagreed that they feel empowered by their cycle. While this association was not true for feelings of worthlessness or guilt or irritability, the effect was seen for tearfulness and spells of crying, feeling overwhelmed, social withdrawal, difficulty concentrating, depression, low mood, anxiety, and mood swings.
A significant negative correlation was observed between participants’ comfort in discussing menstruation with friends and family, and the frequency of cancelling or avoiding social engagements due to menstrual symptoms. Specifically, those more comfortable discussing menstruation were less likely to avoid social interactions (rs(8) = −0.105, p < 0.001).
Menstrual health knowledge and education
To explore if higher levels of knowledge about menstruation are associated with different menstrual experiences, we asked participants to rank their own knowledge as poor (n = 281), some (n = 847), or good knowledge (n = 3607). We also assessed participants’ actual knowledge and rated their knowledge as poor (n = 263), some (n = 1679), or good knowledge (n = 2669).
Participants who self-rate their knowledge of the menstrual cycle higher are significantly more likely to have positive perceptions of menstruation and to agree that menstruation is an empowering experience compared to those who self-rate their menstrual knowledge as poor (p < 0.001). However, although the associations are significant, the effect size is weak (Cramer’s V < 0.2).
To explore whether knowledge about menstruation was associated with menstrual experiences, we asked participants both to self-rate their level of menstrual knowledge and to complete a brief five-question quiz assessing factual knowledge of the menstrual cycle. Based on quiz results, participants were categorised as having poor (0–1), some (2–3), or good (4–5) knowledge. These categories were used alongside self-rated knowledge for comparative analysis. Mean symptom severity scores did not differ significantly based on either quiz-based knowledge scores or self-reported knowledge levels of the menstrual cycle. There is also no association between knowledge scores and the reported disruption to daily activities resulting from symptoms, with the exception of acne/oily skin, changes to appetite, irritability, and mood changes, all of which were reported as less disruptive to daily activities when participants scored highly (Figure 3).

Distribution of participants by self-perceived and quiz-based menstrual knowledge levels.
Participants who self-rated their knowledge as high did report less disruption than people who perceived their knowledge to be poor for the following symptoms, respectively, bloating (2.15 ± 1.11 versus 2.48 ± 1.21; p < 0.001), nausea/vomiting (1.86 ± 1.13 versus 2.04 ± 1.28; p = 0.031), breast pain (1.67 ± 0.93 versus 1.91 ± 1.11; p = 0.004), changes to appetite (1.9 ± 1.02 versus 2.08 ± 1.13; p = 0.031), fatigue (2.85 ± 1.22 versus 3.08 ± 1.27; p = 0.008), depression (2.49 ± 1.32 versus 2.76 ± 1.44; p = 0.025), low mood (2.56 ± 1.24 versus 2.84 ± 1.34; p = 0.003), anxiety (2.66 ± 1.24 versus 2.86 ± 1.33; p = 0.044), mood changes (2.55 ± 1.22 versus 2.78 ± 1.31; p = 0.008), irritability (2.50 ± 1.20 versus 2.7 ± 1.27; p = 0.021), decreased sleep quality (2.56 ± 1.20 versus 2.78 ± 1.27; p = 0.035), leg pain (2.03 ± 1.18 versus 2.31 ± 1.26; p = 0.029), headaches (2.27 ± 1.17 versus 2.53 ± 1.24; p = 0.01), migraines (2.98 ± 1.45 versus 3.13 ± 1.39; p = 0.026), feeling overwhelmed (2.62 ± 1.26 versus 2.93 ± 1.32; p = 0.002), tearfulness and spells of crying (2.30 ± 1.24 versus 2.54 ± 1.39; p = 0.024).
Work and employment
The impact on work and academic performance was observed, with 90.71% (n = 3665) of participants reporting disruption due to menstrual symptoms, and 22.6% of those report the impact to be severe (n = 625; 17.1%) or very severe (n = 203, 5.5%). Thirty-one point eight percent of participants report taking time off work or university to manage their menstrual symptoms in the past 12 months, with 16.0% (n = 758) missing 1–2 days, 10.5% (n = 488) missing 3–5 days, 3.3% (n = 157) missing 6–10 days, and 2.2% (n = 103) missing 10 or more days. When they do take time off work, 18.9% (n = 895) report it as a sick day, 9.2% (n = 435) work from home, 0.8% (n = 37) use annual leave, and 1.1% (n = 52) take unpaid leave. Most respondents felt their employer did not understand how their menstrual symptoms impact them, with 64.0% (n = 2023) reporting their employer’s understanding as not well at all, and 18.7% (n = 592) reporting they understood somewhat well. Only 6.7% of participants felt that their employers understood the impact of menstrual symptoms very well (n = 147) and extremely well (n = 60). In total, 11.3% (n = 535) were somewhat uncomfortable seeking support from their employer when they experienced symptoms, and 62.6% (n = 2966) were very uncomfortable. Only 2.5% (n = 118) and 1.6% (n = 77) were somewhat or very comfortable seeking support from their employer, respectively.
Intimate relationships
Menstrual symptoms disrupted intimate relationships for 84.31% of respondents, with 30.9% reporting a severe or very severe impact. In total, 77.8% (n = 3687) say that menstrual cycle symptoms affected intimacy with their partner in the last 12 months. There was a significant negative correlation (rs(8) = −0.117; p < 0.001) observed between participants’ comfort in seeking support for menstrual cycle symptoms and the impact on intimacy in the last 12 months. Specifically, those who agreed they were comfortable getting support from their partners were less likely to have intimacy disrupted by their symptoms.
Discussion
This study provides valuable insights into the association between perceptions and attitudes towards the menstrual cycle and their impact on various aspects of life, including employment and intimate relationships. The findings indicate that the way individuals perceive their menstrual cycle may be associated with their experience of menstrual-related symptoms and their broader psychosocial well-being.
Previous literature has highlighted the role of psychological support in managing menstrual symptoms. For instance, psychological interventions aimed at empowering women by reframing their narratives around premenstrual symptoms have demonstrated effectiveness comparable to pharmacological treatments such as selective serotonin reuptake inhibitors in addressing mental health-related symptoms. 47 Our findings align with this body of research, suggesting that participants with positive perceptions of their menstrual cycle report lower pain levels and improved mental health during menstruation. While prior research has often described how personal experiences shape menstrual perceptions, our findings suggest that perceptions may also be related to how symptoms are experienced and interpreted. Given the cross-sectional nature of our data, we cannot determine the direction of this relationship and the association may be bidirectional or mutually reinforcing. The possibility of reverse causation should also be considered, where lower pain levels and better mental health might contribute to more positive perceptions of the menstrual cycle. This interpretation is consistent with the growing body of research suggesting that positive menstrual experiences are often accompanied with less menstrual pain and better general health behaviours, and can mitigate the adverse effects of menstrual symptoms.41–43,48–51 Conversely, prior research has also shown that certain phases of the menstrual cycle can intensify psychological symptoms and exacerbate underlying mental health conditions, supporting the complex interaction between physical and emotional experiences of menstruation. 33
Our study demonstrated that participants who viewed menstruation positively experienced less severe symptoms, and that this in turn had a reduced impact on their daily activities. Previous studies have highlighted how menstruation and menstrual symptoms reduces participation in activities due to embarrassment or concern that they would fail to conceal their menstrual period or symptoms.52–54 Our study also observed that menstrual cycle symptoms affect work performance, with 90.71% of participants reporting disruptions. Notably, one in three participants reported taking time off work or university to manage symptoms in the last year, with some taking up to 5 days. Additionally, when participants did take time off, 2.5% used annual leave and 3.5% took unpaid leave. This mirrors findings from other studies that have reported significant impacts on productivity and work attendance due to menstrual symptoms.12,41–43 From an economic standpoint, menstrual symptoms lead to significant productivity losses, costing ~$4333/person annually in the United States and about ¥491.1 billion annually in Japan.55,56 Moreover, presenteeism due to menstrual-related symptoms has been shown to amount to 9 days of productivity loss for women annually. 19 Although our findings found no association between how well people felt their employer understood the impact of their menstrual cycle and how much they rated menstrual-related disruption to their work performance, other studies have found that extent to which employees disclose their menstrual pain to their leaders affects presenteeism. 57 It has previously been recommended that flexible work arrangements may reduce presenteeism, as this will allow affected individuals to adjust their work hours or work from home to reduce the impact of their symptoms on productivity.19,57 Increasing awareness and implementing supportive workplace policies has also been proposed to benefit both employees and employers by improving productivity 58 ; however, more research is needed to understand the effect of these changes once brought into practice.
We found the comfort level in discussing menstrual health with friends, family, or healthcare providers emerged as a critical factor. Participants who felt comfortable seeking support reported fewer disruptions from menstrual symptoms and greater satisfaction with their symptom management strategies. However, it is not unusual for people to feel dismissed by healthcare workers when seeking support for menstrual-related symptoms or conditions. 59 There is also evidence to suggest that when patients have positive interactions with healthcare, it reduces the impact of their cycle-related symptoms and they are more likely to receive effective pain management plans.52,60–62 This underscores the importance of supportive and accessible healthcare services in managing menstrual health effectively, as our findings and previous research have both found positive healthcare experiences to improve the impact from the menstrual cycle.
Another significant finding of our research was the impact of menstrual cycle symptoms on intimate relationships. A majority of participants reported that menstrual symptoms negatively affected intimacy, which is consistent with previous studies.61,63–66 Lonkhuijzen et al. found that negative attitudes towards menstruation often lead to reduced sexual activity during menstruation. 63 Our study extends this understanding by demonstrating that those who felt supported by their partners experienced less disruption in their intimate relationships, highlighting the role of partner support in mitigating the adverse effects of menstrual symptoms on intimacy. This is similar to findings by Allen and Goldberg, who reported that people engaging in intimacy during menstruation often view it as a normal aspect of a committed relationship. 64 Furthermore, research by Romans et al. suggests that social support plays a more significant role in influencing mood across the menstrual cycle than hormonal fluctuations alone. 67 Notably, couples therapy has been found to be more effective than individual therapy or waitlist control in improving relationships and alleviating premenstrual distress. 47 These findings underscore the importance of a supportive social environment in managing the psychological and relational impacts of menstrual symptoms.
Lastly, our findings support the need for comprehensive menstrual health education. Participants who perceived themselves as having higher levels of menstrual knowledge reported more positive experiences and less disruption from menstrual symptoms. This finding supports the need for comprehensive menstrual health education that not only addresses the biological aspects but also challenges the stigma and misconceptions surrounding menstruation, similar to the recommendations laid out by Hennegan et al. 6 It is not uncommon for people to feel they have not been given accurate or sufficient education on the menstrual cycle.28,68–70 As our findings suggest that improving menstrual health knowledge also improves how people experience their cycles, it underscores the importance of education and menstrual health literacy in shaping menstrual experiences. This is echoed in recent evaluations of educational interventions, which demonstrated improved menstrual perceptions and reduced mood-related symptoms among adolescents following targeted menstrual health education. 71
Limitations
When interpreting the findings of this study, there are several limitations which should be considered.
No prospective sample size calculation was performed. While the large sample enhances the statistical power of the findings, this limits precision in determining whether the study was adequately powered for all subgroup analyses or associations. This study is subject to both selection and information bias, which are common in self-reported, cross-sectional online surveys. Selection bias may have occurred during recruitment, as the survey was distributed through social media and newsletters related to The Food Medic – a platform that actively advocates for women’s health. This likely attracted a sample, that is, more health-literate, interested in menstrual health, and not fully representative of the general population. Furthermore, the study sample was skewed towards a predominantly White, highly educated population, limiting the generalisability of the findings. The limited racial diversity likely reflects the audience reach of the digital platforms used, rather than true differences in interest or prevalence of menstrual health issues. While understanding these structural contributors is important, exploring these structural factors was beyond the scope of this exploratory study. While the high number of respondents emphasises that there is a large appetite from people to share their experiences, future research should aim to recruit a more diverse sample as menstrual experiences and perceptions may vary significantly across different ethnic and cultural groups.37,38,68 Although demographic data were collected, subgroup analyses (e.g. by age, race, education, or nationality) were not conducted due to limited diversity within some sub-groups and the study’s exploratory nature. Future research should explore these influences, including age, in more representative samples. Information bias may also be present due to the reliance on self-reported data, which is subject to recall bias, leading to over or under-reporting of symptoms and impact. These sources of bias should be considered when interpreting the results.
A further limitation is that the questionnaire was purpose-designed and has not yet undergone formal validation. While its development was informed by validated tools (e.g. MSQ, MAQ) and relevant literature, future research should aim to validate the instrument’s reliability and construct validity, to enhance the robustness of the findings and improve comparability with other studies.
A further consideration is that the cross-sectional design of the study limits the ability to infer causality between menstrual perceptions and the severity of menstrual symptoms. Longitudinal studies would be necessary to establish causal relationships and understand how perceptions may change over time and impact symptoms. Finally, the use of nonparametric tests due to the non-normal distribution of the data, while appropriate, may limit the statistical power of the analysis.
Additionally, the survey did not collect detailed data on previous or current hormonal contraceptive use. This decision was made to minimise recall bias and avoid the complexity of accurately capturing varied contraceptive histories. Future research focussed specifically on hormonal contraceptive use may be better suited to explore its relationship with menstrual symptoms and perceptions.
Despite these limitations, this study provides valuable insights into the role of menstrual perceptions in the experience of the menstrual cycle and highlights the need for further research to explore these relationships in more depth.
Conclusions
In conclusion, this study highlights an association between menstrual perceptions on the experience of menstrual symptoms, as well as their broader impact on work, relationships, and well-being. While the direction of this relationship cannot be established from the current data, the findings raise important considerations for how attitudes towards menstruation may interact with symptom reporting and lived experiences. Promoting positive perceptions and increasing menstrual health knowledge may support better individual health outcomes, as well as societal attitudes towards menstruation. Future policies should prioritise integrating menstrual health into public health agendas to ensure adequate support and education. Such efforts could lead to improved well-being and productivity for those who menstruate, ultimately enhancing their quality of life.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251399893 – Supplemental material for Exploring the role of menstrual perceptions on health, well-being, and daily functioning
Supplemental material, sj-docx-1-whe-10.1177_17455057251399893 for Exploring the role of menstrual perceptions on health, well-being, and daily functioning by Bríd Ní Dhonnabháin and Hazel Wallace in Women's Health
Footnotes
Acknowledgements
None
Ethical considerations
This study protocol was reviewed and approved by an internal ethics review board (ref. FMRERB/2025/001).
Consent to participate
Participants signed a consent form prior to taking the study’s online survey. Written informed consent was obtained electronically from all participants prior to survey initiation. Consent included confirmation of eligibility, understanding of the participant information sheet, and voluntary agreement to participate.
Consent for publication
Written informed consent was obtained from all subjects involved in the study.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Hazel Wallace is the founder of The Food Medic Ltd, who carried out the research.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available to ensure the privacy of the patients participating in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.