
Abstract
Background:
The COVID-19 pandemic created unique challenges for perinatal individuals in New York City, particularly in neighborhoods with predominantly Black and Latino populations.
Objectives:
The aim of this study was to explore the mental and emotional health experiences of postpartum individuals residing in North and Central Brooklyn, East and Central Harlem, and the South Bronx neighborhoods during the COVID-19 pandemic.
Design:
A qualitative study design was used, emphasizing the lived experiences of postpartum women throughout the pandemic.
Methods:
In-depth interviews were conducted with 41 women, who gave birth between March 2020 and March 2022, in English and Spanish. Data were collected through telephone calls, between July and August 2023. A thematic analytical approach was applied.
Results:
Most participants reported experiencing the emotional changes that are commonly cited during the postpartum period, such as feelings of stress, anxiety, and depression. However, these feelings felt heightened and exacerbated as repercussions of the pandemic. Some shared the negative impact of the pandemic, such as isolation, fear of the virus, changes in healthcare protocols and the loss of social support. Others elevated the joys experienced due to their status as a new parent and the unanticipated benefits of the pandemic, specifically, increased maternal bonding time and opportunities to create healthier social networks.
Conclusion:
This study highlights important gaps in maternal health services during emergencies and underscores the need for policies addressing structural inequities, enhancing social support systems, and expanding access to perinatal mental health services. Investments in paid family leave, affordable childcare, telehealth, and expansion of the perinatal health workforce are critical to improving birth and postpartum outcomes, particularly for populations living in disinvested neighborhoods. Emergency response planning must prioritize the physiological and psychological safety of perinatal individuals to ensure equitable health outcomes.
Plain Language Summary
The COVID-19 pandemic created new challenges for people who gave birth, especially in New York City neighborhoods where many Black and Latino families live. In this study, 41 women who had recently given birth were interviewed in English and Spanish over the phone during the summer of 2023. The goal was to better understand how the pandemic affected their emotional health and overall experience after giving birth. Many women shared that they felt stress, anxiety, or depression after having their baby. These feelings were stronger because of the pandemic. Women shared how hard it was to be isolated from others, to worry about getting sick, and to deal with changes in how they received healthcare. They also talked about the loss of support from family, friends, and healthcare professionals. At the same time, some women found moments of joy. Some felt closer to their baby and enjoyed extra bonding time. Others used this time to build stronger, healthier social connections. This study shows that the pandemic made the postpartum period more difficult for many women. It also shows how important support is for emotional health. Study findings suggest that we need better policies to support new mothers, such as paid family leave, affordable childcare, mental health care, and stronger social support systems. This is especially true for communities that have fewer resources. Preparing for future emergencies must include protecting the health and well-being of people who are pregnant or have recently given birth.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) pandemic presented unique challenges for perinatal individuals residing in New York City (NYC). Shortly after identifying its first case of COVID-19, NYC became an epicenter of the outbreak in the United States, with more than 200,000 confirmed cases between March and May 2020. 1 During this time, uncertainty around the physiological effects of the virus, as well as lack of testing resources and limited treatment capacity, led to the implementation of various policies aimed at reducing rates of infection. 2 This was especially relevant for perinatal individuals, many of whom spend time in medical settings for prenatal care, labor and birth, and postpartum care. For example, some NYC hospitals limited the ability for support persons (e.g., partners, doulas, family, and friends) to be in the birthing room for a brief period of time. 3 While these protocols were quickly reversed, many perinatal individuals and their families experienced undue stress because of these changes. 4
While the impact of COVID-19 was difficult for most NYC residents, the pandemic disproportionately affected residents in neighborhoods with predominately Black and Latino populations.5–7 Three majority Black and Latino neighborhood clusters in North and Central Brooklyn, East and Central Harlem, and the South Bronx, where the NYC Department of Health and Mental Hygiene (NYC Health Department) has had a long-standing physical presence, experienced high risk of severe disease. From February 2020 to October 2021, these three areas experienced higher than average COVID-19-related hospitalization rates and age-adjusted death rates compared to NYC overall. 8 These inequities stem from structural and long-standing racist policies and practices that have negatively affected community health and have contributed to other persistent racial and social inequities including housing conditions, employment circumstances, and underlying diseases that increase the risk of contracting and having a severe reaction to COVID-19 infection. Structural racism has been defined as the “totality of ways in which societies foster discrimination, via mutually reinforcing systems that in turn reinforce discriminatory beliefs, values, and distribution of resources.” 9 Specifically, neighborhood disinvestment and policies like redlining have segregated NYC’s residential communities and conditioned access to resources, including wealth, by race. To address health inequities caused by these historical and contemporary injustices, the three Bureaus of Neighborhood Health (BNHs), located in the aforementioned neighborhoods and operated by the NYC Health Department, led this research project as part of a neighborhood strategy to address and uplift needs of these communities.
One community health priority of the BNHs is to reduce inequities in maternal and infant health outcomes between residents living in BNH neighborhoods and the rest of NYC. According to data from the NYC Health Department’s 2021 Vital Statistics, the prevalence of low infant birthweight (<2500 g) among those living in BNH neighborhoods was higher compared to NYC overall (Brooklyn: 10.9%; Harlem 10.2%; Bronx: 10.5% versus NYC: 9.0%). Babies born to residents in the BNH neighborhoods are also at higher risk of preterm birth (<37 weeks gestation) compared to babies born in NYC overall (Brooklyn: 12.2%; Harlem: 11.6%; Bronx: 11.8% versus NYC: 9.9%). 10 From 2019 to 2021, the infant mortality rates in the Brooklyn, Harlem, and Bronx BNH neighborhoods were 5.3, 6.7, and 5.4 per 100,000 live births, respectively, versus 3.7 per 100,000 live births in all of NYC. Additionally, postpartum women living in these neighborhoods demonstrate higher levels of depression symptomology (Brooklyn: 11.2%; Harlem: 15.2%; Bronx: 10.7% versus NYC: 6.9%). 11 While the full impact of the COVID-19 pandemic on birth outcomes among BNH residents has yet to be determined, it is apparent that the pandemic exacerbated challenges faced by perinatal women, including increased levels of stress, anxiety, and depression.12,13 Overall, the COVID-19 pandemic has been uniquely challenging on the mental health of all NYC residents.14–17 However, perinatal women were particularly susceptible to the negative effects of the pandemic.
Although fears related to pregnancy and birth can be considered rather common, 18 one study revealed that higher levels of fear due to COVID-19 were associated with increased odds of depression and anxiety among pregnant women. 17 Fear of COVID-19 during pregnancy has also been associated with lower infant birthweight and reduced gestational age at birth. 19 The pandemic was also disruptive to those in their postpartum period and new parents. Many studies have documented the challenges of the transition to parenthood that many people face.20,21 These challenges include families often juggling the demands of dealing with a newborn, breastfeeding challenges, changes in their support system, financial stressors, and other challenges pertaining to parenthood.22,23 Therefore, the COVID-19 pandemic response policies, including the “New York State on PAUSE” executive order and recommendations for social distancing, posed challenges to expectant and postpartum mothers, increasing isolation during a time when social support structures are crucial for the well-being of this group and their newborns.24,25 This is especially pertinent due to the association between lack of social support and increased risk of postpartum depression (PPD).26,27 The impact of the pandemic on PPD is well documented. 28 Specifically, the prevalence of PPD during the pandemic was found to be much higher globally at 34% when compared to prepandemic rates, ranging from 9.5% in higher-income countries to 25.5% in lower-income countries. 29 One study found that 36% of postpartum women in the United States reported feelings of depression during the COVID-19 pandemic, compared to 17% before the pandemic. 30
Globally, many studies have shared the COVID-19 pandemic experiences of pregnant and postpartum women, including the impact of healthcare resource reductions, changes with utilization of maternal and infant health care, and the social and emotional impact of the pandemic on mothers and their families.31–35 However, the specific experiences of perinatal individuals in neighborhoods most impacted by conditions of the pandemic remains undocumented in literature. This study fills a gap in knowledge by focusing on the mental and emotional health of postpartum women in BNH neighborhoods, whose experiences during the pandemic have not been systematically studied.
Methods
This explorative qualitative study included individual semistructured in-depth interviews with 41 participants conducted between July and August 2023. Eligibility criteria included having experienced a live birth and being a resident of North and Central Brooklyn, South Bronx, or East and Central Harlem between March 2020 and March 2022. Those who were eligible also had to speak English or Spanish for the interviews. Those who were under the age of 18 were excluded from the study. The purpose of these interviews was to better understand the experiences of BNH residents with their clinical care during the pandemic, specifically on the impact that the pandemic had on birthing and postnatal care; breastfeeding practices; emotional well-being; COVID-19 vaccine considerations; and other factors related to their overall postpartum experience. Findings related to the mental and emotional health impact of the pandemic are presented in this article. The consolidated criteria for reporting qualitative research (COREQ) checklist were used in the preparation of this manuscript (Supplemental material). 36
Sampling and recruitment
To capture a variety of experiences and perspectives across the three BNH neighborhoods, we utilized quota and snowball sampling approaches. Specifically, we aimed to conduct 10–15 interviews per BNH with a goal of reaching saturation across all neighborhoods, for a total of 30–45 interviews. Saturation was operationalized as the point at which no new insights were identified in successive interviews. Participants were recruited through electronic flyers that were emailed through existing NYC Health Department community partner networks, posted in the local NYC Health Department buildings, and disseminated to local partners in the wider community who interact with people who had recently given birth. The study team also distributed physical flyers in community spaces frequented by families such as parks, farmers markets, and other community events. Those who were interested in participating in the study were asked to call the number listed on the flyer to determine eligibility. Potential participants were screened by a member of the research team in their preferred language of English or Spanish, and if eligible they were invited to orally consent to the study and participate in a demographic survey. Participants were subsequently scheduled for an interview. All eligible participants who were scheduled for interviews completed them, therefore no refusal or dropouts occurred. This study was approved by the NYC Department of Health and Mental Hygiene IRB (#22-022), and all participants provided audio-recorded verbal informed consent. Procedures followed relevant ethical guidelines and regulations.
Data collection
Interviews were conducted by telephone. With the participants’ permission, all interviews were audio-recorded. Interviews ranged from 45 to 60 min. At the end of the interviews, each participant received a $50 gift card to thank them for participating which was either mailed to them or picked up at the local Health Department building. The initial draft of a semistructured interview guide was developed by the two lead researchers (BB and LS) based on the study aims and existing literature. Both researchers have prior experience conducting in-depth interviews and one has expertise specifically in maternal health content. Feedback on this draft was obtained from the full research team, who bring varied qualifications including qualitative expertise, research on the impacts of the COVID-19 pandemic, and maternal health. A revised guide reflecting edits from the research team was shared with research colleagues in a division of the NYC Health Department dedicated to maternal and child health topics for content expertise, and their edits were subsequently incorporated to create a final version. Specifically, the guide included questions in five domains: (1) participant experiences giving birth, (2) postpartum care experiences, (3) infant feeding experiences, (4) what is working well throughout the postpartum period, and (5) the current needs of participants (Table 1). Although the questions were kept constant throughout the interview process, probes were iteratively revised based on early interviews to ensure clarity for participants.
Interview Guide Questions.
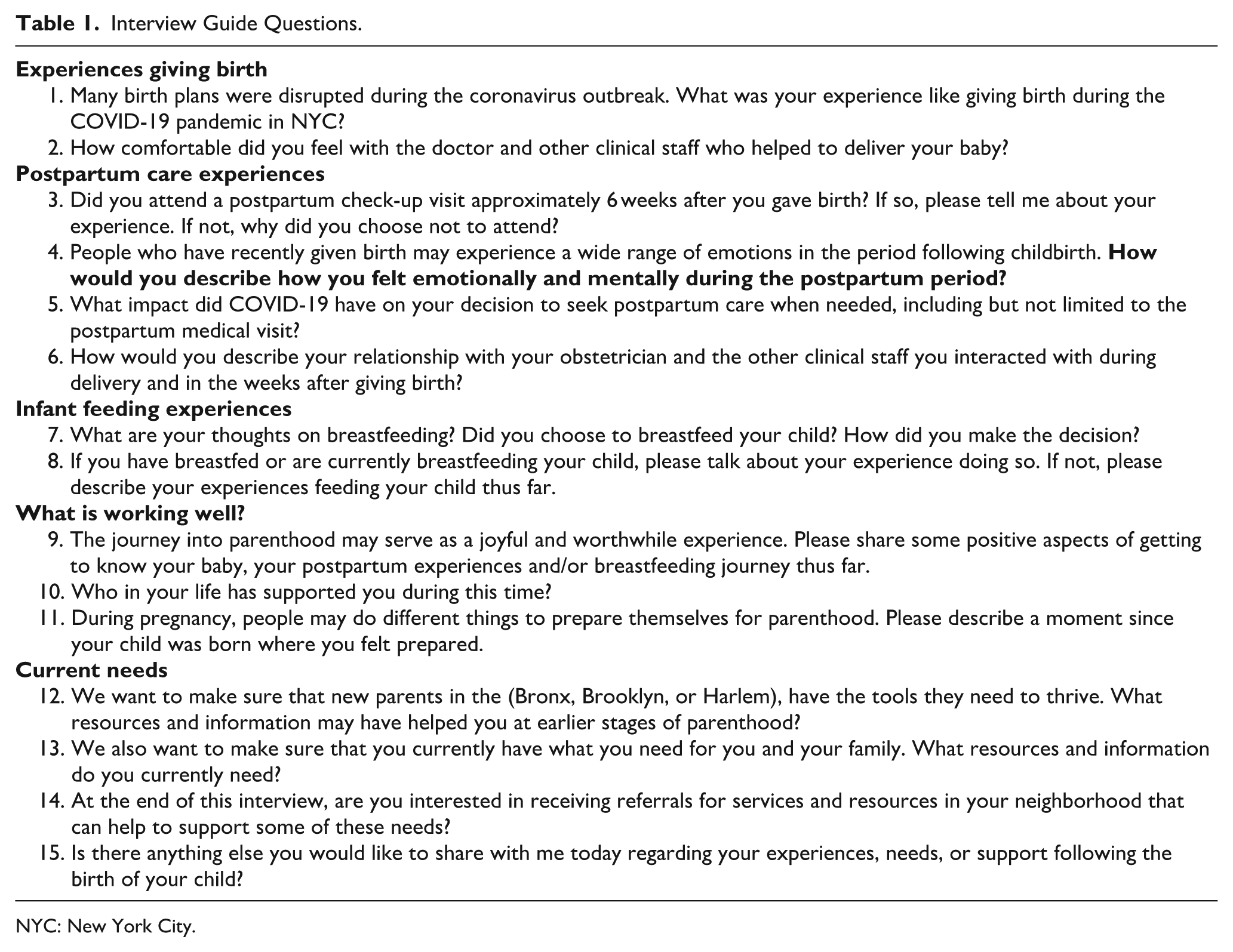
NYC: New York City.
Interviews were conducted by 10 members (SD, JP, JV, LS, BB, FD, VG, BJ, SA, and RD) of the research study team, who worked in 1 of the 3 BNH neighborhoods. It is important to note that no members of the research team had prior relationships with study participants. All interviewers received qualitative research training in masters’ or doctoral programs or from NYC Health Department experts. Spanish-speaking interviewers were native speakers and fluent in the language.
Researchers continually reflected on how their own experiences and identities influenced data collection, analysis, and interpretation. Similar to the study population, all interviewers identified their gender as cisgender women, except for BB, who identified as a cisgender man. All but three team members, LS, AW, and CN, identified as Black/African American or Hispanic. All study team members worked or lived in NYC, with some members of the team being residents of the neighborhoods from which participants were recruited. Two members of the research team, LS and CN gave birth in NYC during the COVID-19 pandemic. The study team was also aware of the social, health and economic inequities, and resultant challenges faced by our study population, as that was the basis of our work in these neighborhoods. As researchers working for the advancement of health equity in these neighborhoods, and as residents of these neighborhoods, the team was heavily invested in the subject matter of this study, particularly during COVID-19, which exacerbated the inequities observed in these neighborhoods. Specifically, the lead author (SD), who conducted some of the interviews, identifies as a Black woman and is a maternal health researcher specializing in birth equity. This positionality shaped the interview process, particularly in how rapport was built with participants with similar backgrounds and how follow-up questions were asked. While this shared identity may have supported more open dialogue during interviews, the study team remained attentive to the risk of assumptions based on perceived shared experiences. All researchers used a similar type of approach with their respective experiences and identities.
Audio recordings were uploaded to TRINT, a NYC Health Department approved automatic cloud-based transcription software, for verbatim transcription. Transcripts in Spanish were translated into English. All transcribed interviews were reviewed by interviewers for accuracy.
Data analysis
All transcripts were analyzed thematically using a combination of inductive and deductive approaches. Data were managed using ATLAS.ti software. Three members of the study team (SD, BB and BJ) each coded a sample of transcripts from participants living in each of the three BNH neighborhoods. These initial codes were generated both inductively from the data and deductively based on the interview guide and study objectives. Through regular peer debriefing meetings, the three coders compared their analyses, discussed points of disagreement, and refined a preliminary codebook through consensus. The remaining transcripts were then coded by additional team members (RJ, LS, SA, FD, and VG), who were purposefully assigned transcripts from participants outside of the BNH catchment area in which they worked to reduce familiarity bias, as some members served as interviewers. The coding schema was then refined through regular and consistent meetings with the larger coding team. To ensure that potential biases were identified, and thematic interpretation was consistent, team members presented analytic memos, questioned one another’s assumptions, and refined code definitions through collaborative discussion.
This iterative process also facilitated the grouping of codes into thematic categories, where emerging themes and subthemes were identified, which led to the development of a final thematic framework. Themes were considered by borough of residence, but findings presented in this article did not differ by borough. Additionally, elements of content analysis were inductively incorporated to capture frequency of salient themes where appropriate. An audit trail was maintained throughout the study to document coding frameworks, theme development, and analytic decisions.
Results
All participants identified as cisgender women and with the exception of one participant, all women in our study identified as either Black/African American or Hispanic/Latino. Additional sociodemographic characteristics of participants are shown in Table 2.
Participants’ sociodemographic characteristics (N = 41).

A total of 48 people responded to the flyer and were interested in participating in the study. Among the 48, 41 (85%) were eligible.
Four themes related to mental and emotional health emerged, including (1) isolation, pandemic anxiety, and the anticipated burden of medical racism; (2) joy of parenthood and bonding during the pandemic; (3) reshaping social connections in the postpartum period; and (4) effects of social support received (Table 3).
Thematic structure.

Isolation, pandemic anxiety, and the anticipated burden of medical racism
Twenty-six out of the 41 women shared experiences dealing with stress, anxiety, and depression shortly after the birth of their baby. While some denoted their feelings as being temporary, others shared what they believed were the main contributors to this stress, such as difficulties with postpartum recovery, lack of adequate postpartum mental health preparation and concerns about their infant’s well-being.
Fear of COVID-19 transmission
Many discussed how the added element of living through a pandemic introduced another level of stress and fear. Specifically, one woman (P19) detailed how “being scared and hearing people die every day” contributed to a high level of anxiety during her postpartum period. Due to the COVID-19 pandemic, participants’ concerns about their newborns acquiring the virus caused them to take precautions that would ensure their infant’s safety, but these precautions further isolated them as new parents.
I was just very overprotective because of COVID, so I didn’t let no one meet her. And then after that, she turned, I think it was about like seven, eight weeks, I allowed people to come one at a time. But you had to get tested for COVID. I was so scared of it, ‘cause I didn’t want her to get it. (P26)
During the initial rollout of the COVID-19 vaccine, a few women discussed their concerns with taking the vaccine due to their uncertainty about potential effects on their baby’s health and development. A woman (P15) who gave birth to her baby earlier in the pandemic stated that “I didn’t want to get the COVID vaccine when I was pregnant.” Another participant expressed experiencing fear that having taken the vaccine during pregnancy could have negative consequences for her baby: “[I was] scared. . . because I thought maybe my baby is not doing well or something like that because I got the COVID vaccine” (P37). Conversely, improvements in protective measures bolstered mental health for some women. One woman (P18) described feeling safer and less anxious during the pandemic when the COVID vaccine became available: I would have had a different mentality that everything was going to be okay, but I didn’t feel that way. Now, since then it’s good that the vaccine is there and all that, I already feel safer. (P18)
Anticipated medical racism as a preemptive stressor
Black women expressed a heightened level of awareness about the potential for medical racism to impact their birthing experience and put them at higher risk for maternal mortality. A few even mentioned the high-profile NYC cases of women who died in 2020 due to complications from an emergency C-section or receiving an epidural in facilities located in their neighborhoods.
37
The fear of experiencing childbirth during the pandemic compounded by the fear of race-based mistreatment from clinicians led to changes in their birth plans. After seeking out information on hospitals and reviewing maternal health-related statistics, one participant chose a specific center outside of her neighborhood based on the level of care given: I wanted to go to a place that was out of my neighborhood because before I gave birth to her, a lady, I heard a girl died while trying, while in childbirth basically due to the health system that wasn’t really that good for Black people. I was trying to research the stats and you know treatment and care of where I went because, I wasn’t necessarily planning on going to that one. Because it was far out of my reach, but I took a cab there. So that’s pretty much it, and the concern of when someone dies in childbirth due to lack of care and lack of concern. So, yeah, so that was cause for trepidation [. . .] They even painted a mural on the wall, of a girl. I forgot her name. It was really big at the moment. That was just really scary, and it was messing with me. I will admit it was a big thing. And makes you concerned about if you would get good health care, or if the people there were racist and not doing everything they could. (P19)
Joy of parenthood and bonding during the pandemic
Some women expressed the joys of learning to be a parent through the caretaking of their newborn. While they acknowledged stressors associated with the role of motherhood, they described being proud of their resiliency and ability to overcome these challenges. Giving birth during a pandemic allowed some participants additional time to bond with their new child because of the various policies that encouraged or required residents to stay at home or shelter in place. One woman stated that “the bonding part was really nice. I stayed home with my baby for like six months due to COVID, so I was happy about that” (P23).
When the women were asked about the positive aspects of parenting, many became notably more animated. Most described the joy they experienced in getting to know their new baby, including positive feelings associated with watching the baby grow, and feeling needed by and connected to their new baby. Some women shared specific aspects of their child’s personality that they found special. One woman (P21) described excitement in watching her baby explore new things and seeing their curiosity. Another explained, Of course, the whole, her existence is like positive, look at the outcome. Beautiful. And then she’s like my best friend. She lights up my life, my world. [. . .] I’ve always had anxiety and battled depression all my life. With my upbringing and everything, I have like the perfect gift, like she is the best thing that’s ever happened to me. (P8)
Reshaping social connections in the postpartum period
Some women reported feeling isolated and alone throughout the perinatal period. Due to both self-imposed restrictions and citywide policies, these women stayed home and isolated from their support network.
Loss of traditional in-person support
During the postpartum period, participants attributed the feelings of isolation, depression, and being overwhelmed to a lack of adequate support. One woman (P18) explained that “no nurse could come to the house. It’s just my husband’s support, but sometimes he had to work, so that’s how I spent it alone and I was kind of anxious because I couldn’t go out. Then I had a cesarean section, so it was very difficult for me to breastfeed my baby [without help].”
Reassessing and restructuring existing relationships
Many women found themselves restructuring their social networks during this period. This was largely due to pandemic-related needs, seeking support to recover from birth, or gaining new perspectives due to parenthood. A few women reconnected with estranged family members as a means of strengthening their social network. Conversely, the isolation brought by the pandemic facilitated opportunities where some participants could establish new boundaries with friends or family members they no longer wished to be in their child’s life, altogether improving family dynamics.
Two women reported utilizing domestic and gender-based violence support services (DVSS; specifically through the shelter system) during their pregnancies as a steppingstone to finding safe, permanent housing for them and their children. One of these women described how she established firmer boundaries with her family of origin: So, I’ll shorten the conversation. I visit them when I want to visit them. So, like, I don’t have the open-door policy anymore like how I used to. I was completely vulnerable to them and this is what they did. So now, you know, I have my own space and my own apartment, 2 beds, and you know they have their own room, and I have my own room. (P11)
The other used DVSS to escape intimate partner violence. In coordination with her physician, she was able to utilize the telemedicine resources that were made widely available during the pandemic to have remote prenatal visits from a safe place. She said: I really expressed to my doctor that, you know, I was in an abusive situation. I was going to lose my apartment and I had to go into the shelter[. . .]I finally moved out of the shelter. . . like a couple days ago and I had been there, . . . since I was six months pregnant in September. . ..[. . .] it was like, it was a lot of stuff. Like, I lost my apartment, you know, my situation with my daughter’s father was extremely toxic and extremely violent. And I was just like, I was going nuts. I was going nuts but I did the right thing and I asked for help. (P5)
Effects of social support received
All but one woman (P38) reported receiving some form of social support during their postpartum period. Some elaborated on how the actions of individuals within their social support system would impact their mental health. Specifically, receipt of social support was seen to be protective against depression, anxiety, and other forms of distress. Reported social supports were classified as tangible, emotional, and informational support.
Tangible support
Tangible resources and services were the most frequently reported type of support received throughout the perinatal period, and included money, food, transportation to medical appointments, baby showers, babysitting or childcare help, and help with domestic work. Prior to giving birth, baby showers allowed friends and family members to bond with and celebrate the expectant mother. Baby showers were seen as a symbolic display of emotional support and allowed the participant to receive needed tangible goods (e.g., diapers, clothing, breast pumps), which saved money and time. Some participants expressed feelings of joy and happiness when recounting memories of their showers. One woman shared: My twin sister was always there for me. She did a surprise baby shower for me. That was happiness. That was the best thing. I don’t know what to say like [. . .] That was the best, happiest day in my life. (P40)
During the postpartum period, some families had a maternal figure (e.g., the woman’s mother, partner’s mother) who moved in their residence to aid the participant during recovery, help with the baby, and reduce other stressors. Accepting babysitting offers from trusted friends and family members provided the participant with time alone to engage in self-care. One woman acknowledged that having people readily available to babysit was a privilege that was often not accessible to other mothers: They [my friends] have been there from day one. They definitely helped me. And if I need to do a date night, they would definitely have no problem watching the baby. Or, if I just need a babysitter because I have to go to work or I have to have a meeting there. You know, they’re always there for me and helpful and supportive [. . .] Um, they definitely been very helpful and supportive and [that] benefits me because if I feel like I need to do a self-care activity, I’m able to. Unlike other people that I know . . .I have friends who have had kids and they don’t have nobody to watch their kid if they wanted to just take a walk in the park for a day or something like that. So I feel very, I’m very grateful for that and just happy that I do have a support system compared to other mothers who don’t really have nobody in their corner. (P36)
Emotional support
Women discussed the strategies they used to address feelings of depression or diagnosed PPD, which included receiving words of encouragement, affirmations, and psychotherapy. Participants who received this type of support were better able to cope with their emotions and stressful experiences. One woman mentioned using a psychotherapy mobile application to talk to a therapist and psychiatrist: My ACS [NYC Administration for Children’s Services] caseworker, she told me about the app [Talkspace]. It’s an app you could talk to a live therapist and psychiatrist on there. I was talking to them on there. So that played a part in me overcoming that emotional rollercoaster, too. So, I had used that for a little while. For about three months. (P1)
Another woman mentioned receiving emotional support from a breastfeeding support group that provided virtual sessions during the pandemic: So, I was in Baby Cafe. They were really, like, supportive and helpful, like days when I wanted to talk about things, they were always there. And yeah, they were just always there for me when I wanted to talk. (P14)
Informational support
Informational support usually came in the form of having access to a knowledgeable person or literature. For instance, one woman noted that, “when I was pregnant, my midwife connected me with a family nurse that I still speak to [to] this day. She’s also the one that connected [me] to the doula. I feel, she’s very attentive to me” (P9). Women who received informational support noted its benefits, but a lack of informational support was mentioned by eight women who noted that adequate mental health resources were not offered to them. Most felt they did not receive a thorough mental health assessment during the postpartum check-up visit and were not offered appropriate mental health resources: Well, I imagine [mental health resources] would be useful because they [would] give us therapy or something, but since she never told me anything, well, no, I didn’t know. (P37)
Discussion
Findings from this study illustrate how the COVID-19 pandemic affected the experiences of residents in North and Central Brooklyn, South Bronx, and East and Central Harlem who gave birth between March 2020 and March 2022. During the postpartum period, women are at high risk of experiencing depression, anxiety, and other instances of emotional distress.38,39 Similar to these findings, most women in our study reported feelings of stress, anxiety, and depression shortly after giving birth. Additionally, they explained ways in which these feelings were heightened by the challenges and uncertainty of giving birth during a pandemic. These results provide substantive depth to prior quantitative research documenting increased prevalence of depression and anxiety symptomology among perinatal women during the COVID-19 pandemic. 40
Policies intended to curb disease transmission had unintended consequences on the mental health of perinatal individuals. COVID-related hospital policies from 2020 through 2022 were unpredictable, inconsistent, and fast-changing, which was distressing to many people seeking healthcare, especially in the first 3 months of the pandemic when the virus was novel, and transmission was poorly understood.41–43 Other studies have elucidated on how the sudden changes to birth plans during the pandemic can be distressing and traumatic. 44 The experience of birth trauma can have some lasting physiological and emotional effects that can negatively impact the postpartum experience and is associated with an increased risk of PPD.45,46 While years have passed since the advent of the COVID-19 pandemic, it is important that future studies focus on understanding the long-lasting and augmented effects of a traumatic perinatal experience brought about by this global pandemic or other similar public health emergencies. This can include examining attitudes toward planning for subsequent pregnancies, changes in birth plans with subsequent pregnancies, and increased use of mental health support.
Social distancing and stay-at-home orders contributed to feelings of isolation and loneliness during a time when social support structures are crucial for the well-being of this group and newborns. 24 Our findings also support prior research which indicates that higher social support helped mitigate mental health-related distress.47,48 Social isolation has been cited as a predetermining factor for perinatal and postpartum mood and anxiety disorders 49 which worsened during the COVID-19 pandemic.31,50–52 Globally, studies on mental health during the COVID-19 pandemic found that perinatal women overall are more vulnerable to developing mental disorders during quarantine periods.53,54
These women were also confronted with a unique set of challenges and concerns, such as fear of the severity of disease, transmission of infection to newborns, and adverse disease outcomes for their newborns. In addition to worrying that their newborns might contract COVID-19 after birth, some women described a reluctance to be vaccinated during their pregnancy for the same reason. During the pandemic, the lack of certainty about how the vaccine might affect their child’s growth, health, and development has been noted to be a common reason for vaccine refusal for pregnant women.55,56 The sentiments demonstrated in our study seem to persist. The uptake rates for the COVID-19 and bivalent booster vaccines are still lower among Black and Latina pregnant women compared to their White and Asian counterparts and the general population. 57 On the other hand, other women in our study expressed that the availability of vaccines helped them to feel safer and less anxious. It is important to note that adequate vaccine education from a maternal healthcare provider is needed to alleviate fears and improve motivation for vaccine compliance.58,59
Among some Black participants, the fear of giving birth during a pandemic was exacerbated by the potential for medical racism, such as implicit or explicit race-based mistreatment by a clinician, which could increase the risk of death during or after childbirth. Studies have shown that the perceived experience of racial discrimination has been linked to an increased likelihood of a preterm birth, low birthweight, delays in antenatal care, and lack of trust in medical providers. 60 Experiences of emotional distress due to racism has also been associated with an increased prevalence of PPD among women of color. 61 Many Black pregnant women are aware of the additional risks associated with medical racism. While stressful, the added knowledge can empower some women to take more control of their birth plans. At least one woman in our study avoided giving birth at a particular health facility in her neighborhood due to such fears.
While the women in our study shared the deleterious effects of experiencing childbirth and postpartum during a pandemic, many shared benefits as well. Some women expressed that they were able to leverage COVID-19 isolation recommendations to limit interaction with certain individuals. Others were able to be reconnected with previously estranged family members. While many studies identified the disruptions to interpersonal relationships between romantic partners, family, and friends,24,62,63 findings from this study are unique because women shared that changes in their social networks were attributed to pandemic-specific needs, unmet support, and recovery needs after giving birth, and to new perspectives gained through parenthood.
Certain pandemic-era policies, such as stay-at-home orders, allowed women to have additional bonding time with their child compared with conventional parental work-leave options. Although other studies have shown a reduction of mother–infant bonding due to the pandemic,64,65 further examination of this positive effect is needed. While purposed to mitigate the spread of COVID-19, certain practices, such as telemedicine services, telework, and other means of virtual communication seemed to serve as a protective factor toward the women’s physiological and mental health throughout the postpartum period. Returning to the example of P5, above, this woman utilized telemedicine services to safely access medical care during a domestic violence crisis while pregnant. Although this can be considered an emergency circumstance, domestic violence during pregnancy is a common and dangerous occurrence, 66 and is theorized to have been increased globally during the COVID-19 pandemic. 67 This care delivery method demonstrated that flexible arrangements for medical care can be viable, productive, and desired during all pregnancy and birth experiences, not just during a public health emergency.
Overall, this study sheds light on the unique challenges faced by women already experiencing heightened stress, depression, and birth-related trauma during the COVID-19 pandemic, emphasizing the urgent need for targeted and expanded support to help them heal from the additional burdens brought about by the crisis. While existing literature has extensively documented the importance of prioritizing vulnerable populations, such as individuals living in poverty,68,69 incarcerated populations, 70 and other marginalized communities71,72 during public health emergencies, this study adds to the growing body of evidence calling for specific attention to perinatal individuals. These findings also suggest that tailored interventions, including access to doula care, robust social support networks, mental health services, and adaptable healthcare delivery models, are essential to address the unintended consequences of emergency conditions and policies. By implementing these strategies, healthcare systems can better support the physical and emotional well-being of birthing individuals, ultimately helping to mitigate the long-term effects of compounded trauma during public health crises.
NYC health department response
The BNHs have historically cultivated expertise and programming to address inequities in maternal health, sexual and reproductive health, chronic disease prevention and treatment, among other areas. Due to the COVID-19 pandemic, various health inequities were exacerbated, and several programs were responsive to arising needs.
With maternal health and birth equity being a citywide priority, an expansion of the NYC Health Department’s Healthy Start Brooklyn “By My Side” birth support program into the Citywide Doula Initiative (CDI) occurred in March 2022. The CDI provides free doula care within neighborhoods across the city that were recognized as having the most disproportionate COVID-19 and other related health outcomes. Those who live in a shelter, are in foster care, have no other labor support, are giving birth for the first time, had a previous traumatic birth experience, or have a high-risk medical condition are prioritized. The CDI also trains community members to become doulas, and they support hospitals in becoming more doula-friendly since doula care is associated with many positive birth outcomes for mother and baby. This level of support is vital for a safe and positive experience during pregnancy and birth. 73
There was also an increase in targeted mental health support for birthing families, along with general support for the community. The NYC Health Department’s Family Wellness Suites are physical spaces in Tremont, East Harlem, and Brownsville where families can receive physical supplies, services, health education, breastfeeding support, and connections to community resources. All aforementioned programs assess expectant and current mothers and fathers for perinatal mood and anxiety disorders (PMADs) to make referrals to professional support when necessary. Within the BNHs, staffing and professional development also increased to address needs for perinatal individuals. This included onboarding a mental health clinician to provide direct support, certified lactation counselors to expand breastfeeding support, and health educators to provide more informational support in various topic areas. Additionally, support groups around breastfeeding, perinatal mental health, and others also expanded to provide more educational and social support for mothers and families living in BNH neighborhoods. In response to the pandemic, many previously offered and expanded programming turned to providing services virtually to avoid disruptions with care. Throughout the NYC Health Department, other divisions are also leading the way to expand mental and behavioral health support for perinatal individuals.
Apart from direct service delivery, the BNHs have collaborated with internal and external stakeholders, including hospital systems and community-based organizations, to collectively strategize to prevent morbidity and mortality related to pregnancy, specifically for Black women and perinatal individuals, who experience the worst inequities in outcomes and care. This has included discussions and planning for collective actions around perinatal mental and behavioral health service capacity and care, policies, and models of reimbursement to improve the pregnancy and birthing experience, and how to effectively address structural racism within systems of care.
Strengths and limitations
The qualitative approach and methodology used in this study can be considered a strength. This allowed a group of postpartum women the opportunity to share their experiences with the birth of their child, postpartum care, emotional well-being, parenting, social support, and current needs through in-depth interviews. This is important because all these topics are interrelated and have a great impact on the postpartum experience. Conducting these interviews over the phone addressed accessibility barriers and expanded the number of eligible people who could participate in this study. Another strength is reflected within our study team, who actively live and/or work within the neighborhoods of our study participants. Additionally, many of the study team members have similar racial and ethnic identities with the women in our study and two team members experienced pregnancy during the pandemic. However, it is important to note that while some team members shared similar identities, practices with reflexivity were continuously incorporated throughout the research process to prevent biases.
This study has several limitations. First, the interview guide was not piloted prior to data collection. However, it is important to note that the questions were informed by existing literature and reviewed by the study team and researchers with maternal health expertise. Additionally, the semistructured format of the interview guide provided team members with the flexibility to ask probing questions. Second, member checking was not conducted with study participants due to the sensitive nature of the discussions on postpartum health experiences during the COVID-19 pandemic. Overall, the study team did not recontact participants to minimize burden. However, the credibility of study findings was achieved through team-based discussions and triangulation across multiple coders. Third, findings from this study may include social desirability bias, especially with discussions on emotional and mental health for this population. In consideration that study team members are employees of the NYC Health Department, some women may have not felt comfortable with sharing their past or current mental health status for fear of judgment or penalization. Although perinatal individuals of any gender were allowed in the study, all participants self-identified as cisgender women, which reduced capability to understand intersecting marginalized gender identities. Finally, interviews were only conducted in English and Spanish. Some of the residents in our BNH neighborhoods speak other languages, including, Haitian Creole, French, Urdu and Mandarin Chinese. They might have had experiences distinct from the study group.
Conclusion
While this study highlights the emotional and social support experiences of women who gave birth during the COVID-19 pandemic, it also shines a light on the gaps in maternal health services and resources that can occur during another emergency response of this magnitude. Several policies can support equitable birth and postpartum outcomes for women and their babies, specifically more investment and attention to policies that provide additional support for parents such as paid family leave, affordable childcare, and teleworking options. Additionally, there needs to be a focus on policy to improve the social determinants of health of perinatal individuals such as those around food insecurity, community and interpersonal violence, affordable housing, access to quality education, and economic inequities. To address perinatal mental health or PMADs, there needs to be policies to protect perinatal individuals who seek support for a mental health or substance use condition and to eliminate any punitive measures around seeking services. There also is a need to ensure that institutions, especially healthcare systems, implement systems of accountability to ensure the physiological and psychological safety of pregnant and postpartum women during times within and outside of an emergency.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251398252 – Supplemental material for The emotional and social impact of COVID-19 on postpartum women: A qualitative analysis on the experiences of women who gave birth during the pandemic in New York City
Supplemental material, sj-pdf-1-whe-10.1177_17455057251398252 for The emotional and social impact of COVID-19 on postpartum women: A qualitative analysis on the experiences of women who gave birth during the pandemic in New York City by Sheena Dorvil, Rose Jimenez, Jennifer Pierre, Jocelyn Valdez, Stephanie Arbelaez, Lauren J. Shiman, Adam Wohlman, Brandon Brooks, Fatoumata Diallo and Christina I. Nieves in Women's Health
Footnotes
Acknowledgements
The authors thank the participants for sharing their experiences. The authors would also like to thank Rachel Dannefer, Bonnie Jim, Valentina Giraldo, Ilish Neely, Keira Sutton-Agnew, and Zulma Novoa for their assistance with study recruitment and data collection. Finally, the authors acknowledge Michelle Morse, Zahirah McNatt, Padmore John, and Anita Reyes for their support and leadership of the Bureaus of Neighborhood Health, Center for Health Equity and Community Wellness at the NYC Health Department.
ORCID iDs
Ethics Considerations
This study was approved by the New York City Department of Health and Mental Hygiene Institutional Review Board (IRB: #22-022).
Consent to Participate
All participants were informed of the study and provided their audio-recorded verbal informed consent to take part in the study. All study procedures were carried out in accordance with relevant guidelines and regulations.
Consent for publication
All participants provided informed consent for their anonymized data to be used in this publication. No identifiable information has been included, and all efforts have been made to ensure confidentiality and privacy in reporting the findings.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the New York City Department of Health and Mental Hygiene.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are not publicly available to maintain participants’ confidentiality.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.