
Abstract
Background:
Uterine fibroids (UFs) are the most common benign tumours of the uterus and are often asymptomatic. However, there is a high incidence of symptomatic fibroids among Black women, with many presenting late for treatment.
Objective:
We examined the patterns and risk factors associated with the late presentation of UF in Black women.
Designs:
Mixed methods study design: A quantitative and qualitative approach.
Methods:
An interviewer-administered questionnaire was used to obtain information about the late presentation of UF from 138 women at the Gynaecology clinic of the University College Hospital, Ibadan, Nigeria. For the qualitative component, in-depth interviews were conducted with eight women experiencing symptomatic fibroids. The odds of late presentation were analysed across socio-demographic, obstetrics and clinical characteristics, along with the type of diagnosis, using logistic regression with a statistical significance level set at p < 0.05. Qualitative data were examined through an inductive thematic analysis, focusing on emerging themes.
Results:
The mean age of participants was 36.80± 7.24 years, with a significant proportion (62.3%) presenting late, more than 6 months after the onset of symptoms and 65.1% having multiple UFs. Factors associated with late presentation included age (AOR = 4.000; 95% CI 0.086–0.0730), parity (AOR = 3.299; 95% CI 1.150–9.464) and presenting with subfertility or infertility (AOR = 0.070; 95% CI 0.020–0.249). The qualitative findings highlighted how situational factors such as inadequate knowledge of the condition, aversion to surgery, negligence, cultural misconception and financial constraints contributed to late presentation.
Conclusion:
A significant number of women, particularly older and nulliparous individuals, sought care late for symptomatic UFs. Increased sensitization and targeted educational interventions are needed to encourage early presentation and timely treatment. Implementing effective health strategies that address the reasons for late presentations will improve health outcomes for women with symptomatic fibroids.
Plain language summary
Many African women, especially in Nigeria, often wait too long to get treatment for UF. These growths are common and can cause serious problems that affect quality of life. However, the reasons for this delayed presentation are not fully understood, making it harder to improve treatment and care.
The research team studied why women in urban Nigeria seek treatment late for UF. The goal was to understand better why some women don’t visit the doctor even when they have symptoms. To gain deeper insights, we interviewed women experiencing these symptoms.
Information was gathered from 138 women through questionnaires, and in-depth interviews were conducted with eight women. The average age of those with symptomatic fibroids was approximately 37 years. Key findings showed that older age, infertility issues, and the number of pregnancies were linked to delays in treatment. Many women lacked knowledge about fibroids, were afraid of surgery, held certain cultural and religious beliefs, and faced financial challenges, all of which contributed to their delays in seeking care. By combining the analysis with personal stories, we gained a clearer understanding of the difficulties these women face.
These results indicate that many women, especially older and those who have never given birth, are not receiving timely care for symptomatic fibroids. Better awareness and educational programmes are needed to encourage early treatment, which could improve their health outcomes and reduce complications. Additionally, the findings equip healthcare providers with insights into the factors leading to late presentation for treatment, enabling them to identify at-risk groups and create more effective support strategies and interventions.
Introduction
Uterine fibroids (UFs) are benign smooth muscle tumours and are the most common neoplasms affecting women of reproductive years 1 with their prevalence ranging from 28.3%–31.6% in Nigeria.2,3 Approximately 7% of women with UF are asymptomatic, likely leading to an underestimation of the true prevalence, as these cases often go unreported. 4 UFs are categorized according to their location: subserosa fibroids extend outward from the uterus, intramural fibroids develop within the myometrium and submucosal fibroids protrude into the uterine cavity. 5 Symptoms of UF include heavy menstruation, severe anaemia, abdominal mass and discomfort, pelvic pain and pressure, sub-fertility and infertility. 6 Other reproductive risks associated with UF include; impaired fertility, miscarriage, pregnancy-related deaths, increased preterm labour and delivery, delivery complications and increased risk of caesarean delivery.7–9 In sub-Saharan Africa, the barriers to treatment of UF are often related to the lack of access to adequate healthcare facilities, lack of well-trained health providers, poor quality of health services and issues of finance for treatment. 6
The pattern of presentation of UF is changing, as a recent study reported that fibroid is common among women aged 50 and above, post-menopausal women and having no live births. 10 However, there is a higher UF prevalence among women from the ages of 21 to 35 than women in the older age group. 2 Other factors predisposing women to UF include biological (genetic mutation like MED 12, epigenetic factors as observed in monozygotic twins, endogenous and exogenous hormonal factor, obesity),10,11 socio-demographic (age, race), reproductive (time since last birth, parity) and individual lifestyles (smoking, diet, alcohol consumption).1,12 In addition, socio-economic factors, especially education and income, affect access to, and the type of healthcare services received for benign diseases like UF. 13 For women in most African societies, societal values and norms cause stigmatization and misinformation with superstitious beliefs, often leading to delayed presentation, late diagnosis and treatment for UF. 14
The treatment of UF is based on the symptoms, size, rate of growth and desire for fertility, and treatment options include expectant management, medical therapy, uterine artery embolization and surgery like myomectomy and hysterectomy. 15 Previous studies have focused on racial dynamics, symptoms and treatment of UF, with little information on the timing of presentation, which can determine the type of treatment and care.6,15,16 This study, therefore, examines the current patterns of presentation of UF about timing, as well as the factors that predispose women with symptomatic UF to present late for treatment at a healthcare facility.
Methods
Study area and design
This study utilized a convergent mixed methods design to collect information from women diagnosed with symptomatic UF at the University College Hospital (UCH), Ibadan, Nigeria. By integrating both qualitative and quantitative techniques, this study provides a comprehensive understanding of UF, capturing a broad range of women’s experiences and perspectives, thereby enhancing insights into the risk factors and reasons for late presentation. UCH is a government tertiary healthcare facility located in the urban city of Ibadan, Nigeria. It provides approximately 4500 gynaecological consultations every year across 5 subspecialties: Urogynaecology, Gynaecologic Oncology, Fetomaternal Medicine, Infertility and Assisted Conception, and Fertility Research and Endocrinology.
Study participants
The study population was patients diagnosed with symptomatic UF from 2019 to 2021 who attended the gynaecology clinic of UCH, Ibadan, Nigeria.
Inclusion criteria
Women in the reproductive age group with symptomatic fibroids who have completed at least secondary school education presenting at UCH who gave their consent were eligible to participate in this study.
Exclusion criteria
The study excluded pregnant women with co-existing UF, acutely ill women, those with recurrent UF, and those less than 20 and older than 49 years of age.
Data collection
The quantitative study captured symptomatic patients with clinical and ultrasound diagnoses of UF from 2019 to 2021 who presented in the gynaecological clinic, whereas the in-depth interview (IDI) participants were patients diagnosed in 2021. To ensure validity, the quantitative questionnaire was pre-tested for clarity and understanding, which also enhanced the reliability and accuracy of the data collected. A total of 241 patients presented during the study period; 138 patients were purposively selected to maximize variation and ensure that the selected participants had valuable insights to contribute (Figure 1 – study flow diagram). They were also selected based on the inclusion criteria. Firstly, a structured questionnaire was administered to the participants to collect data on socio-demographic characteristics, clinical symptoms and duration from the onset of symptoms to the presentation of symptomatic UF (Supplemental Appendix 1). Secondly, IDI lasting 60–90 min were conducted using semi-structured interview guide adapted from previous studies.17–19 (Supplemental Appendix 2). The semi-structured interview guide was pre-tested on 2 participants (10% of the initially planned 12–15 participants) to enhance clarity and contextual appropriateness of the questions. These interviews explored their perceptions, knowledge, patterns and factors associated with the late presentation of symptomatic UF. All interviews were conducted by a trained MSc Sociology student in a quiet room within the clinic to ensure confidentiality and create a comfortable environment for open discussion. After conducting eight interviews with no new insights emerging, data saturation was achieved indicating the information was rich enough to answer the research question.20,21 Interviews were audio-recorded with participant consent, and field notes were taken during and immediately after each session to capture non-verbal cues and contextual details. Transcripts were not returned to participants for comment or correction, and no participant checking of findings was conducted. The medical records were also reviewed to extract relevant data, which added depth and reliability to the quantitative findings. Information extracted includes ultrasound findings, clinical signs and symptoms and treatment received (if any). The reporting of the qualitative aspect of this study conforms to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Supplemental Appendix 3). 22 The quantitative aspect follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Appendix 4). 23

Study flow diagram.
Sample size calculation
The sample size was calculated using the Kish and Leslie formula for a single proportion. Based on a 6.83% prevalence of UF in a South-Western Nigerian population study, 4 95% confidence interval and 5% margin of error, the minimum sample size was derived. Accounting for a 10% non-response rate, a final sample size of 138 was used.
Statistical analysis
The quantitative data were analysed using IBM Statistical Package for Social Science (SPSS) Statistics for Windows version 25.0 (IBM Corp., Armonk, NY, USA). Descriptive and inferential statistics were used to determine the factors associated with late presentation with the significance level set at p < 0.05. The odds ratio and 95% confidence interval were reported. Fisher’s exact test was reported when the expected frequency in any cell of the contingency table was less than 5.
The qualitative data were analysed using inductive, narrative and thematic content analysis approaches. The transcripts were used to develop a preliminary codebook, which was continuously refined as new themes emerged during the coding process conducted by two of the researchers until the final codebook was generated. Thematic analysis was employed to identify themes within the data, resulting in a final set of descriptive categories.
Outcome variable
The outcome variable of this study was the late presentation of UF.
Independent variables
Socio-demographic characteristics
Obstetric characteristics
Type of diagnosis
Clinical characteristics (signs and symptoms)
Contextual factors identified in the qualitative data
Operational definition
Early presentation refers to the patient’s first instance of seeking healthcare within 6 months of the onset of symptoms, whereas late presentation refers to seeking healthcare for symptoms beyond 6 months after their onset. 24
Types of diagnosis are categorized into two: Intentional and Incidental check-ups. Intentional check-up/diagnosis is classified as a diagnosis when the primary reason for presenting at a healthcare facility is related to fibroid symptom(s), whereas incidental diagnosis is defined as a diagnosis made during a presentation for a different ailment. Clinical diagnosis refers to the patients’ symptoms based on evaluation of the clinical findings, whereas ultrasound diagnosis was based on radiological report of presence of UF including size, location and numbers.
Ethics information
Ethical approval was obtained from the Ethics Committee of the University of Ibadan/University College Hospital (UI/EC/21/0055). Written consents were obtained from the study participants after fully disclosing the study objectives and purpose. Confidentiality was assured as names were not required from the participants and data de-identified. The IDIs were conducted by a female MSc Sociology student with training in qualitative research and interview techniques. No prior relationship was established with participants before recruitment, minimizing potential bias in responses and maintaining objectivity throughout the data collection process.
Results
One hundred and thirty-eight women participated in the quantitative aspect of the study, whereas eight women participated in the qualitative study. Table 1 summarizes the socio-demographic data of the IDI participants.
Socio-demographic of the in-depth interviews participants.

Of the 138 women, approximately 80% of the women were Christians, married (82.6%) and had tertiary education (81.2%). Half (50.7%) of the participants are within the 30–39 age category, and 34.1% were self-employed (Table 2).
Socio-demographic characteristics of participants.

SD: standard deviation.
The pattern of presentation and treatment received by diagnosed patients was examined and presented in Table 3. Approximately two-thirds presented late (62.3%), with 81.2% of diagnoses made during an intentional check-up. Most patients (95.7%) had no family history of UF, and over half of the population (60.1%) had fibroids in multiple locations at the time of presentation. Among those with single-location fibroids, intramural fibroids were the most common (43.6%). The most common symptoms reported were abdominal/pelvic pain (53.4%) and subfertility/infertility (36.1%). Surgical treatment was the most common treatment received by the participants, with only a small number of women (0.7%) undergoing endometrial polypectomy.
Patterns of presentation and treatment.

Multiple response.
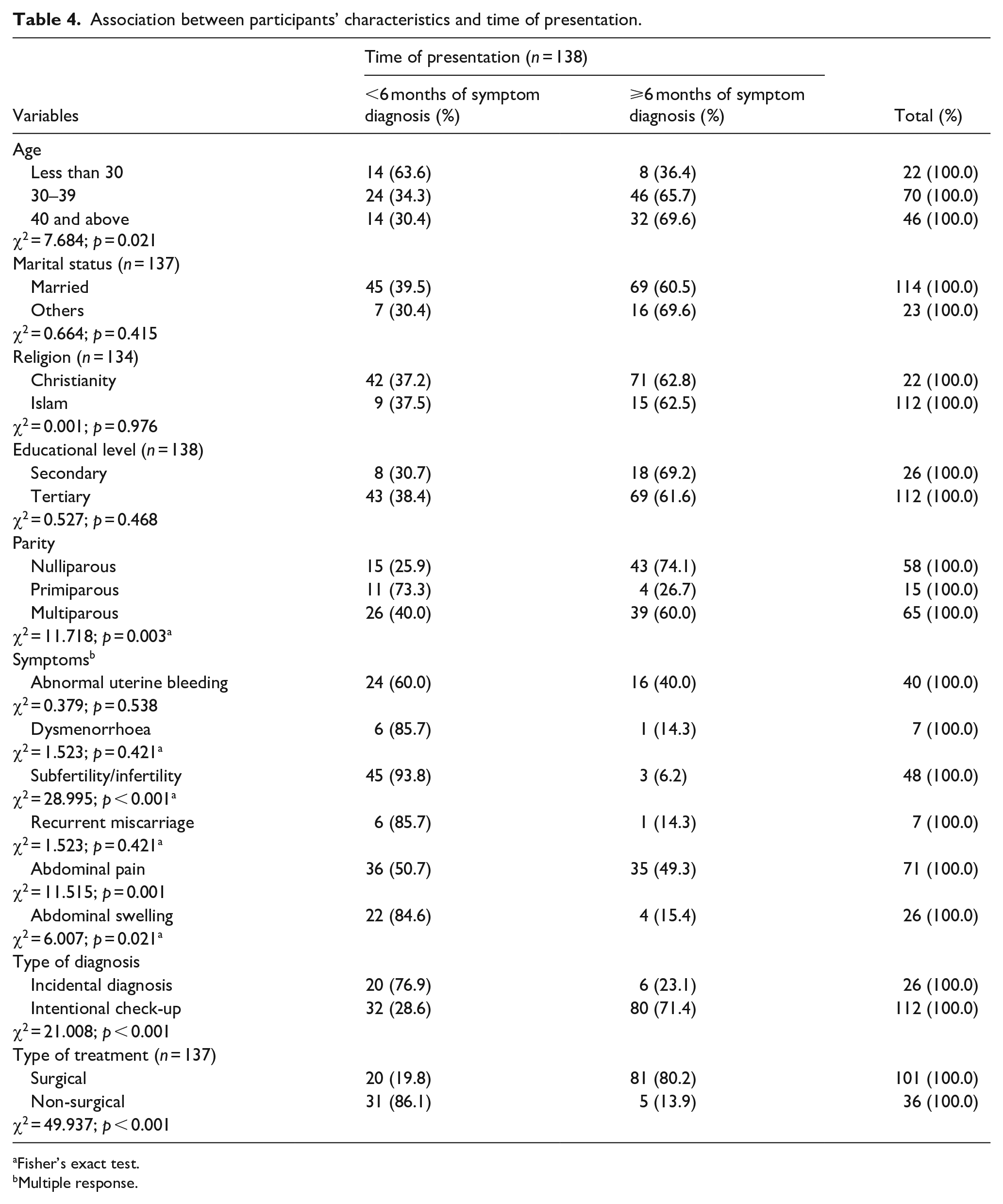
The prevalence of late presentation was higher among women ⩾40 years than those younger (<30 years and 30–39 years), (69.6% versus 65.7% versus 36.4%; p = 0.021) and in those with intentional check-ups than incidental diagnosis (71.4% versus 23.1%; p < 0.001). A significant proportion of the nulliparous women presented late compared to multiparous and primiparous women (74.1% versus 60.0% versus 26.7%; p = 0.003). Despite the late presentation, a significant proportion of women (64.2%) received treatment promptly. Most of those who underwent surgical treatment presented late compared to those receiving non-surgical treatment (80.2% versus 13.9%; p < 0.001; Table 4).
Association between participants’ characteristics and time of presentation.
Fisher’s exact test.
Multiple response.
Table 5 shows the adjusted and unadjusted odds ratio of the time of presentation of UF. Variables such as age, parity, symptom (subfertility/infertility) and type of treatment received were examined as predictors of late presentation for UF management. Women aged 40 years and above were four times more likely to present late for UF treatment compared to those 39 years and younger (AOR = 4.000; 95% CI 0.086–0.0730). The nulliparous women were three times more likely to present late for treatment than multiparous women (AOR = 3.299; 95% CI 1.150–9.464). Additionally, those experiencing subfertility or infertility were approximately 14 times less likely to present late for treatment compared to those without symptoms (AOR = 0.070; 95% CI 0.020–0.249). Women who received surgical treatment were 25 times more likely to present late for UF treatment (AOR = 25.230; 95% CI 6.895–92.326).
Predictors of late presentation of uterine fibroids.

In the qualitative analysis, three key themes emerged: inadequate knowledge of the condition, aversion to surgery and financial constraints. These factors significantly contribute to women presenting late at healthcare facilities. Participants shared contextual reasons that influenced their delayed care-seeking behaviour, offering insights into the challenges they faced.
Inadequate knowledge of the condition and cultural misconception
Many women expressed feelings of confusion and helplessness which reflects the lack of understanding about their condition and the appropriate steps to seek care. Cultural beliefs about women’s sexuality and health can also overshadow the actual medical issues at hand further complicating her health-seeking behaviour. This cultural inclination also promotes the use of home remedies – herbs rather than seeking medical care. In addition, the intersection of spirituality and health particularly the stigma associated with strong religious beliefs about conditions like fibroids can significantly influence how women perceive and manage their health.
‘I didn’t know what to do, I was just packing myself and getting soaking. You know what? let me tell you something, when my father discovered that I was having heavy bleeding you know what he said, the man said, my father, my own father he said boya o se family planning ni (maybe she did family planning) and my mother was even telling him that what will I do family planning for, my dad told my mum that do you think she can stay so long like that without having sex with a man, though she is unmarried, she cannot even stay so long like that without having sex and I am not married, see that kind of ideology. . .Nothing, I was just taking ewe ogbo with milk. They call something ewe ogbo, when you add it with milk it will give you more blood that is it. . . It is common everywhere just pluck, after plucking you squeeze the juice and add milk to it. . .’ [IDI, 42 years, Teacher] ‘. . .you know the way they (people) see it outside the world, people say it is spiritual, in fact, churches have affected so many things, maybe they think you have a spiritual husband making love in the dream and all those things. . .Fibroid is a bad omen’ [IDI, 38 years, Unemployed]
Aversion to surgery
Many participants expressed a deep-seated fear of surgical procedures, often rooted in cultural beliefs, personal experiences and societal perceptions. This fear can lead to a reluctance to seek timely medical intervention, as women weigh the potential risks of surgery against their current health status. Additionally, societal attitudes contribute to this fear, particularly among single women, who may avoid surgery due to concerns about visible scars that could impact their chances of finding a partner.
‘Now I have seen people who are not married that have got large abdominal mass and say this cannot be fibroid and once they are diagnosed the fear is I don’t want to get operated on, I don’t want anybody to put a knife on my stomach while I am yet to get married, so that will now determine, to me that is what I observe as a person. . . Because they feel once there is a mark on your stomach your husband will ask you, are you sure you are having your uterus intact because that will be the fear. Whatsoever must have led you to do such operation, it might be that your uterus has been taken away, must I go through the risk, the extent of risking my life and get married to you and we are waiting for the fruit of the womb, so that is the fear. . .’. [IDI, 42 years old, Nurse] ‘. . .maybe people are thinking at the end of the day, it will be surgery case or being worried about all that surgery involves’. [IDI, 38 years old, Civil Servant]
Financial constraints
Some women indicated in their interviews that they sought care late due to an inability to afford the necessary surgery for their condition. Participants shared experiences of having to borrow money to cover hospital bills, indicating that they needed time to secure funds before seeking treatment.
‘Negligence, let me say money again. . . I was trying to package myself for money because I know that UCH that is where I am going because that is where I did the first one, so UCH I am coming, and I have to package myself with money, so I was now planning. So, my husband helps me borrow (get) some amount, so for me to start with. . .’. [IDI, 39 years old, Civil servant]
The responses above affirmed that women’s social and cultural environment as well as their economic condition affect the time of presentation.
Discussion
This study examines the patterns of presentation of UF and the factors that contribute to late presentation. Factors associated with late presentation of symptomatic fibroids include age, parity, clinical symptoms, type of diagnosis, aversion to surgery, negligence, treatment costs, low educational status, inadequate knowledge of the condition and lack of social support. Most women diagnosed with UF are less than 40 years old, multiparous and married. However, a study in the United States found that fibroid cases were more prevalent among older women of 45 years and above. 9 In some studies, UF is more commonly diagnosed in nulliparous women, whereas our study found a higher diagnosis rate among multiparous women, despite evidence suggesting that multiparity is generally associated with a reduced risk of UF. 10 This discrepancy may be attributed to differences in population characteristics, as well as cultural and societal factors. Multiparous women may be more willing to discuss health issues, leading to a higher diagnosis rate. Additionally, they are likely to be older, which increases their risk of developing UF. 10
Almost all the women reported no family history of UF, which is quite different from the findings in some studies that suggest family history influences the timing of presentation.14,25 This discrepancy may be attributed to a cultural silence surrounding UF; some participants mentioned that they are secretive about their condition and do not discuss it with others, which may make them unaware of their likely family history. Despite experiencing several symptoms, most of the respondents still presented late, with the diagnosis made when they intentionally presented for check-ups because of the worrisome symptoms. This is probably because some women wait until their fibroids have grown large enough to cause debilitating health issues, such as severe bleeding and anaemia. 26 Some women believed their symptoms were not serious and thought they could manage and cope with them. Others take analgesics and self-prescribed medications to relieve their symptoms until their condition worsens or they experience complications before seeking hospital care.
Intentional check-ups and surgical treatment were associated with late presentation, which is expected since most of our study respondents were symptomatic and likely sought care when their symptoms became worrisome. The finding that most diagnoses occurred during intentional check-ups further emphasizes that identifying fibroids typically requires an in-person visit to a healthcare provider or facility equipped with ultrasound technology. 27 Additionally, concerns about treatment costs and aversion to surgery may have contributed to delays in seeking care. The qualitative data from our study indicated that financial burdens, negligence, inadequate knowledge and aversion to surgery are significant risk factors for late presentation which is in keeping with findings from previous studies.1,17
Our study findings of inadequate knowledge and absence of a confidant as risk factors for late presentation were consistent with other studies. A review article identified lack of knowledge and misinformation from family and friends contributes to women’s delays in seeking early intervention. 14 This supports the report that many women with UF lack the support needed to manage their condition, with only a few seeking assistance from healthcare professionals. 26
Literacy, along with cultural and societal beliefs, significantly influences understanding of symptoms and healthcare-seeking behaviour. In this study, the level of knowledge among relatives, such as parents, was associated with health-seeking behaviours. Some women may conceal their feelings, as less informed family and friends often hold superstitious beliefs about the causes and management of fibroids. For instance, one participant shared, ‘I didn’t know what to do; I was just soaking myself. When my father discovered I was having heavy bleeding, he said, “Maybe she did family planning” and insisted that I couldn’t stay unmarried without having sex for so long’. This highlights how inadequate knowledge, and cultural beliefs can lead women to self-manage their conditions instead of seeking appropriate medical care.
Most of the respondents in this study presented late, corroborating other findings that women experienced UF symptoms for years before diagnosis. 16 Being 40 years or older and nulliparous were predictors of late presentation for fibroid treatment. The finding that a significant association exists between age greater or equal to 40 years and UF in the multiple logistic regression model corroborates with the report by Stewart et al. 1 In addition, Zimmermann et al. reported that the prevalence of UF increased by age, especially in women >40 years in 8 different countries; Brazil, Canada, France, Germany, Italy, South Korea, the United Kingdom and the United States. 28 This finding was attributed to variations in a country’s access to the healthcare system and healthcare provision. In Li et al. study, it was revealed that globally, women aged 35–39 years and older have an increased risk of UF and attributed their finding to the women’s origin or descent linking this with changing economic development, lifestyles and diets. 29 In addition to the above reasons, our findings may be attributed to previously asymptomatic fibroids growing bigger and becoming more prominent with age and increased exposure to sex steroid hormones. 10 In contrast, a study by Millien et al. found no association with age. 18 In this study, women aged 40 and above may have attributed fibroid symptoms to natural ageing processes, which could delay their seeking prompt healthcare, leading to late presentation for treatment. Additionally, some women might view symptoms like menstrual irregularities as typical, which can influence the timing of their presentation, especially among nulliparous women. 25 The perception that surgery is the most commonly used and effective treatment for UF, despite its potential costs, may also contribute to delays in seeking care.3,30,31 This underscores the finding that financial constraints were frequently cited as a reason for delayed treatment in this study. However, those having subfertility/infertility, a delay in conception, were less likely to present late for treatment. We observed that those with symptoms of subfertility/infertility were 14 times less likely to present late for treatment. This could be because fertility defines womanhood and marriage success in most African societies.
Limitations and strengths
This facility-based study is limited to women who sought care at the hospital, which may restrict the generalizability of the findings. Obesity, a potential risk factor for UF due to hormonal imbalances, was not assessed in the study. Additionally, although the semi-structured interview guide was adapted from previous studies, it was not formally validated, therefore we could not confirm whether the women’s reported perceptions accurately reflected their clinical understanding or health-seeking behaviours related to late presentation. However, the qualitative findings offer valuable insights and deepen the understanding of why women delay seeking care despite experiencing symptoms, whereas the quantitative results offer reliable data with a detailed description of the patterns of presentation and factors associated with the late presentation of UF. Overall, the study equips healthcare providers with the knowledge of the factors contributing to late presentation, allowing for the identification of at-risk populations and tailoring of interventions. It can also inform strategies to improve patient–provider communication, enhance early diagnosis and ultimately improve the quality of life and treatment outcomes for women with fibroids.
Conclusion
This study identifies several reasons for the late presentation of women seeking treatment for symptomatic UF. They have limited knowledge about fibroids, self-medicate and cope until symptoms become worrisome or complications arise while prioritizing cultural and societal beliefs. Early diagnosis and treatment are crucial for reducing complications and healthcare costs. Therefore, both hospital and community-based initiatives should educate women about the symptoms of UF and the importance of seeking timely medical care. Advocacy efforts should focus on public awareness campaigns, addressing financial barriers such as promoting broader health insurance coverage and fostering support networks to mitigate delays in receiving treatment.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251367143 – Supplemental material for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study
Supplemental material, sj-docx-1-whe-10.1177_17455057251367143 for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study by Ayoola J. Fakunmoju, Olufunke A. Fayehun and Oluwasomidoyin O. Bello in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251367143 – Supplemental material for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study
Supplemental material, sj-docx-2-whe-10.1177_17455057251367143 for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study by Ayoola J. Fakunmoju, Olufunke A. Fayehun and Oluwasomidoyin O. Bello in Women's Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251367143 – Supplemental material for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study
Supplemental material, sj-docx-3-whe-10.1177_17455057251367143 for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study by Ayoola J. Fakunmoju, Olufunke A. Fayehun and Oluwasomidoyin O. Bello in Women's Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057251367143 – Supplemental material for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study
Supplemental material, sj-docx-4-whe-10.1177_17455057251367143 for Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: A mixed method study by Ayoola J. Fakunmoju, Olufunke A. Fayehun and Oluwasomidoyin O. Bello in Women's Health
Footnotes
Acknowledgements
None.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of the University of Ibadan/University College Hospital (UI/EC/21/0055).
Consent to participate
Written consents were obtained from the study participants after fully disclosing the study objectives and procedures. Confidentiality was assured as names were not required from the participants.
Consent for publication
Not applicable. This study did not involve the publication of identifiable personal data, images or case details that would require participant or guardian consent for publication.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data supporting this study’s findings are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.