
Abstract
Background:
The increasing rate of cesarean section births is a global concern, including in Tanzania, where cesarean section births account for 11% of live births. Following a cesarean section, mothers are commonly discharged early to reduce ward congestion; as a result, they are required to receive care at home. However, evidence indicates that mothers receive limited or no information on post-cesarean section home care, which increases the risk of complications.
Objective:
To assess knowledge of home care after cesarean section birth among postpartum mothers in Central Tanzania.
Design:
An analytical cross-sectional study.
Methods:
This study involved 467 randomly selected post-cesarean section mothers, assessed 24–48 h after birth. Participants’ knowledge was evaluated using 60 items that covered essential home care, nutrition, and postnatal services utilization, as well as sexual and reproductive health. Data analysis was conducted using SPSS (version 27).
Results:
Overall, 63% of post-cesarean section mothers demonstrated adequate knowledge of essential healthcare needs, whereas 55% exhibited an inadequate knowledge of nutritional needs and the utilization of post-natal services. However, 93% had inadequate knowledge regarding sexual and reproductive healthcare. Being employed, residing in Dodoma, and having higher education attainment were significantly associated with adequate knowledge of essential healthcare needs, as well as meeting sexual and reproductive health, nutritional, and post-natal service utilization needs. Post-cesarean section mothers with only one prior cesarean section were less likely to possess adequate knowledge about essential healthcare needs and sexual and reproductive healthcare.
Conclusion:
Generally, the knowledge of home care after cesarean section births is inadequate, especially regarding sexual and reproductive healthcare. Comprehensive and standardized health education on home care after cesarean section births is essential for improving knowledge of home care among post-caesarean section mothers and enhancing their recovery.
Introduction
The increased rate of cesarean section (CS) births is a worldwide concern. 1 CS counts for more than one in five (21%) of all childbirths. 2 The rate is expected to rise in the coming decades, with nearly a third of all births anticipated to be conducted by CS. 2 In Tanzania, 11% of live newborns were delivered by CS, with the majority (30%) performed in private sector facilities, 28% in religious/voluntary sector facilities, 13% in health facilities, and the smallest 12% in public facilities, other percentages were not mentioned in the report. 3 The CS births are expected to increase following Tanzanian government efforts to promote access to emergency obstetric services, which have resulted in more than 400 health facilities being upgraded to provide access to cesarean births and blood transfusions Comprehensive Emergency Obstetric and Newbon Care (CEmONC). 4
Mothers after CS births are commonly discharged early to decongest the post-CS wards. This early discharge results in post-CS mothers benefiting less from hospital care and being exposed to home care earlier. 5 Therefore, mothers’ knowledge of home care after CS is essential in guiding them on their recovery. Contrary to high-income countries (nations with a high gross national income per capita, as classified by international organizations such as the World Bank) where mothers are commonly visited at home by healthcare providers for care, 6 this practice is uncommon in Tanzania. 7 Mothers and their babies are required to visit the postnatal clinic 7 days after CS. 8 This time is well known to be when most of the complications after childbirth occur, one of them being surgical site infection (SSI). 8 Therefore, knowledge of home care after a CS is necessary to ensure a smooth recovery and avoid complications. 7
Evidence suggests that little or no information is given to post-CS mothers by healthcare providers on care at home following CS births. 9 Available guidelines have contradicting recommendations on home care after CS, 9 leading to the provision of inconsistent and inadequate information by healthcare providers to post-CS mothers. 10 This is challenging in a low-income country like Tanzania, where a context-specific post-CS home care guide is not available. Therefore, studying home care knowledge of postpartum mothers after CS is important to inform the baseline understanding before the establishment of intervention. This study describes postpartum mothers’ knowledge of home care after CS birth in central Tanzania.
Objectives
Broad objective
To assess knowledge of home care after CS births among postpartum mothers in Central Tanzania.
Specific objectives
To assess the prevalence of knowledge on home care after CS birth among postpartum mothers in Central Tanzania.
To assess the predictors of knowledge on home care after CS births among postpartum mothers in Central Tanzania.
Methods
Study design
This analytical cross-sectional study examined the relationship between home care knowledge and the associated factors. This study was conducted in the two regional referral hospitals in the central zone of Tanzania, Dodoma Regional Referral Hospital and Singida Regional Referral Hospital, which had higher rates of both SSI 11 and CS births. 7 In addition, these hospitals provide CEmONC services. The study was conducted between March and June 2022.
Study population
This study enrolled mothers who gave birth by CS and were 24–48 h postpartum. This timeframe was selected because mothers are likely to have less postoperative pain and still be in the wards before they are discharged home. To be included in the study, mothers had to be able to walk post-surgery (ambulate) and have given birth to a live baby by CS in the study setting. Mothers of premature babies or those requiring prolonged hospitalizations were excluded from the study. All participants provided written consent after receiving detailed information about the study’s aim, procedures, and their right to withdraw at any time.
For illiterate participants, a thumbprint replaced a signature. Participants under 18 years of age provided verbal assent, and their legal guardians provided the necessary signatures.
Sample size estimation
The sample size for this study was estimated based on the ongoing quasi-experimental study evaluating the effectiveness of the post-CS home care guide in preventing SSI. 7 Based on the established inclusion criteria, the 467 mothers were randomly selected from the post-CS wards after being identified by the nurses in charge. Each qualified mother was assigned an identification number. These numbers were written on a piece of article, folded, and placed in a box. Selection was conducted through a lottery system with numbers drawn randomly from the box. To maintain equal selection probability, drawn numbers were returned to the box after each selection. The random sampling approach ensured that all eligible mothers had an equal chance of participation while minimizing selection bias.
Data collection tool and method
The pre-tested structured questionnaire was developed based on established components of post-CS home care guidelines. These components included nutrition, wound care, exercise, hygiene, family planning, post-natal service utilization, sexual activities, and mental healthcare. In addition, the questionnaire assessed mothers’ demographic characteristics and economic status. Economic status was assessed using eight question items adapted from the Tanzania Demographic and Health Survey. 12
An interviewer-administered questionnaire was used to collect data from post-CS mothers through Kobo Toolbox, a digital data collection software designed for data collection using a tablet or smartphone. The first author and three research assistants conducted all interviews 24–48 h after the CS, whereas the post-CS mothers were resting in bed. At this time, ambulation had already been initiated, and mothers were able to sit up and breastfeed their infants. The beds were screened to maintain privacy and avoid interruptions from ward activities. Specifically, data collection took place between March and May 2024.
Piloting of the tool
To ensure the validity and reliability of the questionnaire used to assess mothers’ knowledge of home care after hospital discharge, a pre-test was conducted with 50 post-CS mothers, representing 10% of the total sample size at Morogoro Regional Referral Hospital (MRRH). 13 The MRRH was chosen as it is a different site from where the main study was conducted. 14 Data analysis was performed using Statistical Package for Social Sciences (SPSS version 25). The pre-test findings informed both principal component analysis (PCA) and scale analysis. For PCA, a factor loading threshold of 0.50 was applied, as recommended by previous studies. 15 The internal consistency of the tool was ensured by evaluating it using Cronbach’s alpha, with a cut-off point value of α ⩾0.60 to ensure homogeneity. Data cleaning and completeness were verified by examining the frequencies of items per variable. 15
The content validity was ensured by adopting and modifying tools from credible sources12,16 and further reviewed by the third author, a quantitative research expert. None of the included items were removed during manual data cleaning, as all demonstrated variance. A total of 60 items were subjected to exploratory factor analysis, with a Kaiser-Meyer-Olkin (KMO) value of ⩾0.5 and a significance level of ⩽0.05. An item weight was set at ⩾0.3 as recommended by previous scholars, 15 and all items met this criterion and were retained for further analysis. To assess internal reliability, scale analysis was conducted on 60 items. The results showed that no item had zero or near-zero covariance, indicating that all items were suitable for further analysis. Moreover, the second (quantitative research expert) and third author reviewed the tool and suggested editorial changes. However, no items were added or removed as a result of their review.
Measurement of variables
Dependent variable
Knowledge of home care among post-CS mothers.
Independent variables
Age of the mother: The chronological age of the mother at the time of the survey.
Education level: The highest level of education attained by the mother.
Occupation: The current employment status or job role of the mother.
Marital status: The current marital situation of the mother (e.g. single, married, divorced).
Caregiver: Identification of who primarily cares for the mother and/or the newborn.
Number of births: The total number of births (parity) experienced by the mother.
History of CS: This variable has three options: 0 (no previous history of cesarean birth), 1 (one previous cesarean birth), 2 (two previous cesarean births).
Number of antenatal clinic (ANC) visits: The total number of antenatal care visits attended by a mother during the pregnancy.
Tribe: Category 1: native tribes (specifically Gogo and Rangi) and category 2: immigrant tribes (all other tribes).
Analysis
The analysis was performed using SPSS (version 27). Descriptive statistics were used to summarize participants’ demographic characteristics, estimate the prevalence of knowledge, and describe patterns related to home care knowledge.
Knowledge was assessed across three domains: essential home care for post-CS mothers, knowledge of nutrition and postnatal services utilization and knowledge of sexual and reproductive health. Mothers who scored above 50% in each domain were considered to have adequate knowledge in that respective category.
To examine the relationship between independent variables and the categorical-dependent variables for each knowledge domain, chi-square tests and multiple logistic regression analyses were performed. A 95% confidence interval and a 5% margin of error (0.05) were used to determine statistical significance.
Reporting guide
The reporting of this study adheres to the STROBE statement for cross-sectional studies (Supplemental Material). 17
Results
The study involved 467 post-CS mothers. About three-quarters (74.5%) were aged between 20 and 34 years, and a few (11.1%) were aged 16–19 years. Nearly half of the participants (47.8%) had completed primary education. The majority of mothers had experienced two to four pregnancies (55.3%) and two to four childbirths (53.7%). Most of the participants (80.7%) had attended more than four antenatal care visits, and nearly half of the mothers (47.1%) had a history of one prior CS, as shown in Table 1.
Sociodemographic characteristics of the study participants (N = 467).

ANC: antenatal clinic.
Prevalence of home care knowledge among post-CS mothers
The majority of participants (63%) had adequate knowledge of essential healthcare needs. However, more than half (55.5%) demonstrated inadequate knowledge of nutritional needs and postnatal service utilization. A substantial proportion of participants (92.9%) had inadequate knowledge regarding sexual and reproductive healthcare, as shown in Table 2.
Prevalence of knowledge on home care among post-CS mothers (N = 467).

Association between demographic characteristics and knowledge of essential healthcare needs
The knowledge of essential healthcare needs among post-CS mothers was significantly associated with region of residence, education level, occupation, tribe, and the number of previous CS. In contrast, no significant associations were found with age, marital status, type of caregiver, number of pregnancies, number of births, or number of ANC visits, as shown in Table 3.
Relationship between knowledge for domain 1, 2, and 3; and the demographic characteristics of post-CS mothers.
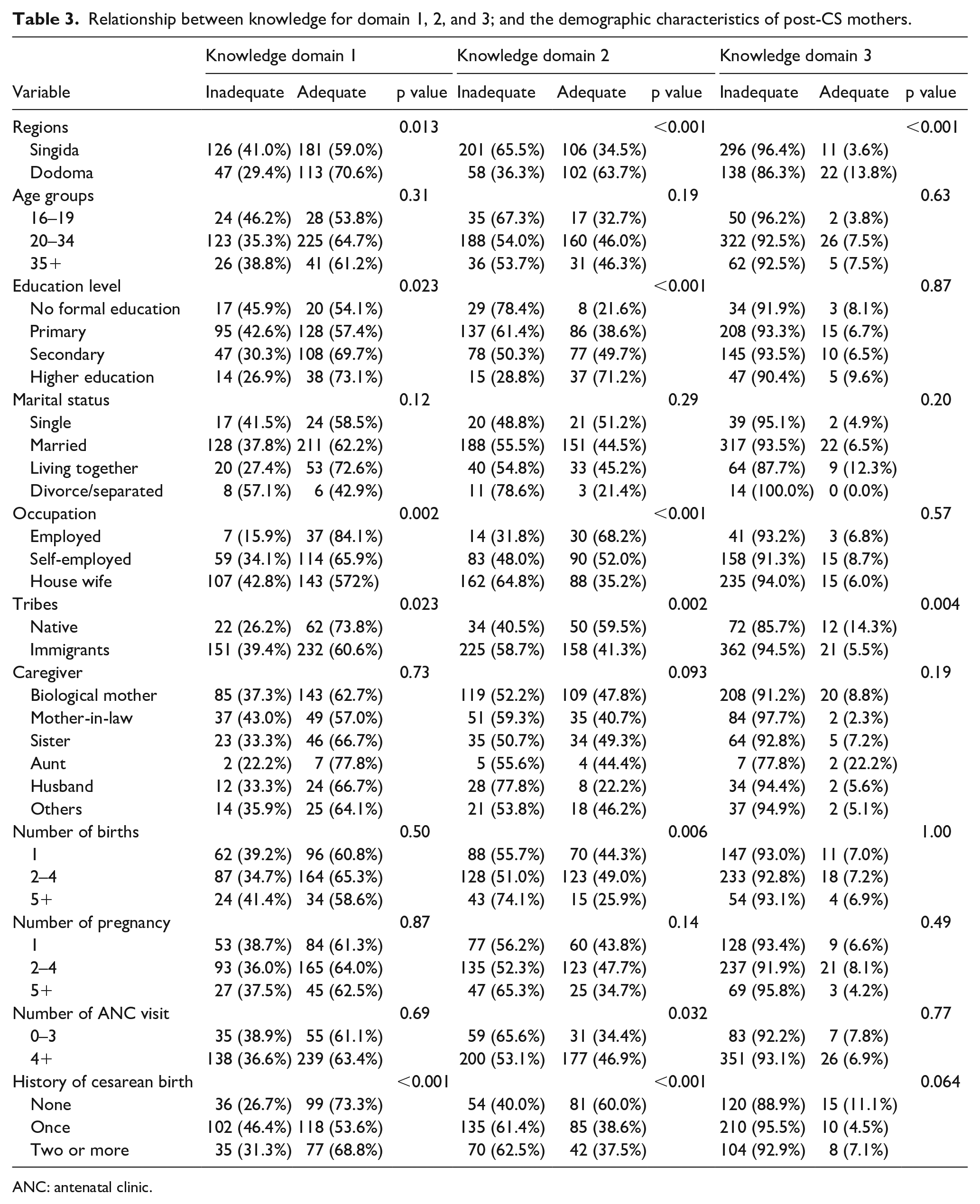
ANC: antenatal clinic.
Association between demographic characteristics and knowledge of nutritional needs and postnatal care service utilization
Knowledge of nutritional needs and postnatal care service utilization among post-CS mothers was significantly associated with region of residence, education level, maternal occupation, tribe, number of ANC visits, and the number of CS a woman had. However, no significant association was found with age, marital status, type of caregiver, or number of pregnancies, as shown in Table 3.
Association between demographic characteristics and knowledge of sexual and reproductive healthcare
Knowledge of sexual and reproductive healthcare among post-CS mothers was significantly associated with region of residence and tribe. The number of cesarean births a woman has had shown a marginal association with knowledge of sexual and reproductive healthcare needs. Other factors, such as age, education level, occupation, marital status, type of caregiver, number of pregnancies, number of ANC visits, and number of births, were analyzed but did not show any association with knowledge of sexual and reproductive healthcare, as presented in Table 3.
Factors associated with adequate knowledge of the essential healthcare needs of post-mothers and newborn care
This study found that employed mothers had slightly higher knowledge of essential healthcare needs after CS compared to housewives, when other factors are controlled (Adjusted Odds Ratio-AOR 1.10 (95% CI: 0.67–1.80)). In addition, mothers with a prior history of CS were less likely to have adequate knowledge of essential healthcare needs (AOR 0.51 (95% CI: 0.31–0.85)), as presented in Table 4.
Results of logistic regression model for factors associated with adequate knowledge for domain 1, 2, and 3 of post-CS mothers.

ANC: antenatal clinic; CS: cesarean section.
Factors associated with adequate knowledge of nutritional needs and postnatal care service utilization
Mothers residing in the Dodoma region, and with higher education levels, were independently associated with adequate knowledge of nutrition needs and postnatal service utilization. Mothers from Dodoma were more than twice as likely to have adequate knowledge of nutritional needs and postnatal care service utilization (AOR 2.17 (95% CI: 1.33–3.51)). In addition, mothers with higher education levels were significantly more likely (over seven times) to have adequate knowledge compared to mothers with no formal education (AOR 7.66 (95% CI: 2.32–25. 30)). In contrast, mothers with at least one previous CS were less likely to have adequate knowledge of nutritional needs and postnatal care service utilization (AOR 0.45 (95% CI: 0.23–0.88)), as shown in Table 4.
Factors associated with adequate knowledge of sexual and reproductive healthcare needs
Residing in the Dodoma region was found to have a borderline association with having adequate knowledge of sexual and reproductive healthcare needs among post-CS mothers, compared to those from the Singida region (AOR 3.33 (95% CI: 1.42–7.80)). Other factors, including education level and number of cesarean births, marital status, occupation, tribe, type of caregiver, age, number of ANC visits, and number of births, were also analyzed but showed no significant association with knowledge of sexual and reproductive healthcare needs, as shown in Table 4.
Discussion
This cross-sectional study aimed to assess mothers’ knowledge of home care after CS. The findings revealed a generally low level of knowledge among post-CS mothers, especially regarding sexual and reproductive healthcare. Adolescents constituted the smallest subgroup in the study population. Despite the small sample size of adolescent mothers, no significant association was found between adolescent age and low knowledge of post-CS home care. This challenges the assumption that younger age limits understanding of home care practices. The findings align with a study conducted in sub-Saharan Africa, 18 which reported that adolescents who receive targeted education can improve their postpartum knowledge and practices. Similarly, a study in Indonesia demonstrated that reproductive health education interventions can significantly enhance adolescents’ knowledge. 19 In this study, adolescent mothers exhibited higher levels of knowledge comparable to their older counterparts. This underscores the effectiveness of comprehensive, standardized, evidence-based education, such as home care guides for mothers of all age groups. Instead of viewing age as a risk factor, this study emphasizes the importance of delivering age-inclusive, evidence-based education to support recovery and improve the home care experience for all postpartum mothers.
In this study, the majority of mothers (63%) demonstrated adequate knowledge of essential healthcare, including wound care, perineal care, body hygiene, and mental healthcare. These findings differ from those reported by Peter and Seif; and Elsayed et al., where the majority of post-CS mothers exhibited poor knowledge of essential healthcare, particularly in the area of wound care.20,21 The discrepancy in findings may be attributed to differences in the assessment tools used. In the present study, the tool evaluated the overall home care knowledge of post-CS mothers rather than focusing solely on wound care, as was the case in other studies. In addition, the timing of participants’ selection may have influenced results. The previous studies assessed mothers attending antenatal visits during subsequent pregnancy following a CS, whereas the current study assessed mothers within 24–48 h after their CS delivery.
This study also found that employed mothers had greater knowledge of essential healthcare post-CS compared to unemployed mothers. This may be attributed to the fact that most employed mothers tend to be more educated and therefore possess better knowledge of essential life skills than unemployed mothers. 4 Moreover, employment status often reflects economic status, which can influence access to health information and resources related to post-CS home care. 22
Furthermore, the study also revealed that mothers with a prior history of CS were less likely to have adequate knowledge of essential healthcare after CS compared to those with no prior history of CS. This suggests that having previously undergone a CS does not necessarily ensure better knowledge of home care. It indicates that essential post-CS health is still inadequately provided to mothers during hospital stay. 23 This gap may indicate a lack of sufficient education on essential healthcare needs within the community, including among mothers who have previously delivered through CS. 10
In addition, this study found that more than half of post-CS mothers had inadequate knowledge of nutritional needs and postnatal care services utilization. Similar findings were reported in a study by Peter et al., which identified limited knowledge among post-CS mothers regarding the role of nutrition in wound healing. 20 Nutrition, particularly adequate protein intake, is critical for wound healing, as protein deficiency impairs the proliferative phase by disrupting angiogenesis, fibroblast proliferation, and collagen production, ultimately reducing connective tissue formation. 24 Cultural beliefs and myths surrounding pregnancy and childbirth often contribute to dietary restrictions that may hinder recovery. 22 For example, a study by Bathula et al. 25 on the nutritional experiences of postpartum mothers found that dietary restrictions were commonly practiced during the first 15 days after childbirth. The same study reported that although most mothers consumed excessive amounts of iron‑rich foods, they avoided fruits and protein‑rich foods such as meat, eggs, and fish.
Moreover, the current study reported that post-CS mothers residing in Dodoma had greater knowledge of nutritional needs and postnatal care services utilization compared to those from Singida. This disparity may be attributed to the rapid development of Dodoma, following its designation as the capital city of Tanzania. The resulting influx of people for business and employment has likely enhanced access to health information and services compared to Singida. 26 Similar findings were reported in a study by Beraki et al. in Eritrea, which showed that mothers from urban areas were twice as likely to be knowledgeable about postnatal care services compared to those from rural areas. 27 This difference is likely due to greater access to health information and services in urban or more developed regions.
Mothers with higher education levels were also more likely to possess knowledge of nutritional needs and postnatal care services utilization than those without formal education. Consistent findings were reported by Nchimbi and Joho in Tanzania, who assessed knowledge of puerperal sepsis and self-care practices among postpartum mothers. 28 The study found that mothers with higher education were significantly more likely to understand how to prevent puerperal sepsis than those without formal education. 28 Likewise, Peter et al. reported inadequate wound care knowledge among post-CS mothers was more prevalent among those with no formal education compared to mothers with higher levels of education. 20 Similarly, a study by Bearki et al. in Eritrea found that mothers with secondary and higher education demonstrated greater knowledge of postnatal care service utilization than those with lower education levels. 27 These findings suggest that education levels may enhance mothers’ access to health information and improve their understanding of essential care practices. In today’s digital and information-driven world, women with higher education are more likely to be familiar with basic nutritional needs, such as balanced diets and food groups, compared to those with limited or no formal education.
Furthermore, this study found that mothers with a prior history of CS were less likely to have adequate knowledge of nutritional needs and postnatal service utilization compared to those without a previous CS. This finding suggests that education on nutrition and postnatal service utilization is inadequately provided to post-CS mothers, even among those who have previously undergone the procedure. Evidence indicates that knowledge is a strong predictor of postnatal care utilization.29,30 Therefore, investing in maternal education on nutrition and postnatal services is critical to improving both nutritional practices and attendance at postnatal clinics.
Moreover, the study revealed that the majority of post-CS mothers had inadequate knowledge of sexual and reproductive healthcare. This aspect of health is essential at all stages of life, particularly during pregnancy and childbirth, when physiological changes may impact sexual well-being. According to the Tanzania Ministry of Health’s postpartum guide, women are advised to resume sexual activity only after three conditions are met: perineal healing, lochia has stopped, and mental readiness. 31 Previous studies have reported that the mode of delivery is not a significant predictor of sexual recovery 32 or sexual dysfunction in women. 33 Therefore, all post-partum mothers, regardless of their delivery method, should be knowledgeable about sexual and reproductive health. In contrast to this study’s findings, a study by Beraki et al. in Eritrea found that 46.5% of postpartum mothers were aware of the appropriate time to resume sexual activity after childbirth. 27 These findings underscore the need to explore further the knowledge of post-CS mothers regarding home care, as identifying these knowledge gaps is crucial for designing effective, targeted interventions that support maternal health recovery after childbirth.
Limitations of the study
Although this is one of the few studies assessing post-cesarean mothers’ knowledge of home care after hospital discharge, research on this topic remains scarce. To strengthen the discussion, we included studies from diverse global sources, including those focusing on mothers who have had spontaneous vaginal deliveries. Additionally, recall bias is a potential limitation, as participants were asked to report their home care experiences retrospectively. To minimize this, a piloted, structured questionnaire was used to ensure clarity and accuracy in responses. Nevertheless, the findings should be interpreted with this limitation in mind.
Conclusion
Generally, post-cesarean mothers demonstrated limited knowledge of home care, especially in sexual and reproductive healthcare needs after birth. Given the increasing global rates of CS births, it is crucial for mothers to be well informed about post-CS care to prevent both short and long-term complications, such as SSIs. There is a great need to provide comprehensive and standardized health education on post-CS home care to support mothers and caregivers during recovery. This is especially important as early hospital discharges may leave mothers inadequately prepared, highlighting the necessity for improved health education to enhance their knowledge and self-care practices.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251365372 – Supplemental material for Knowledge of post-cesarean home care among postpartum mothers in Central Tanzania: Baseline findings from a quasi-experimental study
Supplemental material, sj-docx-1-whe-10.1177_17455057251365372 for Knowledge of post-cesarean home care among postpartum mothers in Central Tanzania: Baseline findings from a quasi-experimental study by Mwajuma Bakari Mdoe, Stephen Mathew Kibusi and Lilian Teddy Mselle in Women's Health
Footnotes
Acknowledgements
The authors appreciate the post-CS mothers and nurse midwives of DRRH and SRRH for their contributions to this study. Additionally, the authors would like to acknowledge the University of Dodoma for funding this study.
Ethical considerations
The Institutional Review Board of Muhimbili University of Health and Allied Sciences approved the study (ref no.: MUHAS-REC-05-2021-647).
Consent to participate
Respondents provided written consent after being informed about the aim of the study, the procedures, and their right to withdraw at any time. For respondents who were illiterate, a thumbprint was accepted as a substitute for a signature. Additionally, since eight minors were involved, they provided verbal consent while their legal representatives provided the necessary signatures.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Dodoma has funded this study for the doctoral program. However, the funder had no role in the study design, data collection, data analysis, or article writing and publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data of this study are under the Muhimbili University of Health and Allied Sciences, they will be available upon request to the office of Deputy Vice-Chancellor–Chancellor Academic, research, and Consultancy through email:
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.