
Abstract
Background:
One of the primary reasons for an increase in cesarean sections is obstetricians’ uncertainty about labor trial safety following a previous cesarean section. The success rate of vaginal birth after cesarean section with a single cesarean scar is greater than 50%. However, to the best of our knowledge, there is a scarcity of information on the determinants of vaginal birth after cesarean delivery in the study area. As a result, the purpose of this study was to identify predictors of successful vaginal birth after cesarean delivery in public hospitals in Eastern Ethiopia.
Methods:
A nested case–control study design was used within a prospective follow-up study conducted from June to October 2020. A total of 220 women who tried vaginal birth after cesarean delivery was included, 110 cases and 110 controls. Cases were women with one previous cesarean section scar and successfully proceed with vaginal delivery. The controls were those with an earlier cesarean section scar and delivered by emergency cesarean section after trial of labor. A pre-tested structured questionnaire was used to gather the information. Multiple logistic regression is used to identify the determinants for the success of vaginal birth after cesarean section; odds ratio with its 95% CI are used to report the findings.
Results:
We found that living in rural areas (AOR = 2.28; 95% CI (1.85, 12.41)), having a current antenatal care follow-up (AOR = 3.20; 95% CI (1.15, 8.87)) and partograph monitoring of labor (AOR = 4.26; 95% CI (1.90, 9.57)) had a positive association with successful vaginal birth after cesarean section. In contrast, the presence of meconium-stained amniotic liquor (AOR = 0.10; 95% CI (0.01, 0.75)) and history of stillbirth (AOR = 0.07; 95% CI (0.02, 0.53)) reducing the chance of success of the trial.
Conclusion:
Past obstetric history, such as stillbirth, history of labor trial after primary cesarean section, and prior vaginal birth, were significant predictors for achieving vaginal birth after cesarean section. Antenatal care visit, and partograph follow-up were the current obstetric characteristics positively associated with the trial of labor.
Keywords
Introduction
A trial of labor after cesarean (TOLAC) is a trial of labor for the current pregnancy to achieve a vaginal birth after a previous cesarean section scar (VBAC). 1 Over the last several years, the cesarean section (CS) rate has increased in the world. 2 Most obstetricians are unsure about the safety of the trial of VBAC, and women are also unwilling to accept the risk associated with the trial of VBAC. As a result, women who had previous CS scar underwent repeat CS which is the primary cause of an increased cesarean delivery rate.3,4 However, studies indicated that VBAC’s success rate among women with one CS scar is more than 50% with minimal complication.5–9
Maternal morbidity and future pregnancy complications are reduced with the success of VBAC. Furthermore, a successful VBAC lowers the risk of surgical complications and the length of hospital stay. 10 Repeated CS is associated with increased obstetric complications, such as hysterectomy, blood transfusions, adhesions, and surgical injury. Placenta previa occurrence increases from 10/1000 deliveries in one CS to 28/1000 with three CS deliveries. 11 VBAC is one approach to control the rate of CS and decreased maternal complications related to repeated CS. It also to obtain large families as the plan. 10
The risk of morbidity is higher in failed VBAC; several studies indicated that patients with a failed vaginal birth after cesarean have higher uterine rupture rates, hysterectomy, blood transfusions, chorioamnionitis, postpartum hemorrhage, and neonatal morbidities.12,13
Guidelines for VBAC indicate that TOLAC offers women with no contraindications and one previous transverse low-segment cesarean. The decision should be based on the standard approach to reduce the risk associated with the TOLAC. 14 The chance of achieving a vaginal birth is influenced by many factors, such as prior vaginal birth, low maternal BMI, rupture of membrane at admission, high parity, the recurrent indication of CS, and cervical dilatation.5,9,15–20
In Ethiopia, like other countries, the preferred delivery mode for pregnant women who have a cesarean delivery history is the CS, which increased the CS rate. Some studies in Addis Ababa, Ethiopia reported that the success rate of VBAC is the same as other sub-Saharan regions, which is > 50%, with several factors associated with success VBAC.21–23 Understanding predictors under a different setting benefits the clinician to recognize and decide if CS should proceed based on women’s labor progress. However, to the best of our knowledge, there is a scarcity of information on the determinants of VBAC in the study area. As a result, the goal of this study was to identify predictors of successful vaginal birth after cesarean delivery in public hospitals in Eastern Ethiopia.
Method
Study design, setting, and period
A nested case–control study (NCC) design within a prospective follow-up study was conducted on selected hospitals from the Harari region, Dire Dawa, and East Hararghe—namely, Hiwot Fana, Jugal Hospital, Dil Chora Hospital, and Bisidimo Hospital from June to October 2020. A total of 2246 laboring women were included in the prospective follow-up maternal survey; these women, 210 women, were recruited for this study after the delivery. Cases were women with one previous CS scar and successfully proceed with vaginal birth. The controls were those with an earlier CS scar and delivered by emergency CS after trial of labor.
Source and study population
This study’s source population was all women who have the previous scar and attend delivery at selected hospitals. Women with one previous CS scar and tried for a vaginal birth for current pregnancy were the study population. According to the selected hospitals’ protocol, the women who had more than one CS scar should undergo elective CS. Therefore, a trial of labor is allowed for the women who had only one previous scar.
Inclusion and exclusion criteria
Sampling techniques and sample size determination
The sample size is calculated by assuming a 95% confidence interval, power of 80%, based on a case–control study done at Addis Ababa; the presence of amniotic fluid used as a predictor. Unexposed with outcome 29%, exposed with outcome 47% and OR = 2.20, R = 1:1, 22 the final sample size is 231. A 1:1 case to control ratio was used; the sample size is divided into 115 for the cases and 116 for controls with a 5% non-response rate. The participants were consequently selected as having the previous scar and trying a vaginal birth. The sample size was proportionally allocated to each hospital by considering client flow in the prior months. 24 Finally, 220 women with only one previous CS scar tried vaginal delivery were included. Of these, 110 succeeded in vaginal delivery, whereas 110 tried labor but failed vaginal delivery and underwent emergency CS. Therefore, all women who had previous CS scars and tried labor enrolled during the study period were included.
Participants recruitment
Women recruited in the follow-up study and previous CS scars were invited to participate in the research. All information about the study was explained to the participants according to their understanding level using local languages. After obtaining written informed consent, recruitment was carried during delivery. In the follow-up maternal survey, 359 women had previous CS scar; 297 had one previous CS. However, 225 women had one CS tried vaginal birth, and 220 were volunteers.
Data retrieval and collection
A pre-tested structured questionnaire translated into the local language (Amharic Afaan-Oromo and Somali) was used to gather the information. It was developed from other literature.22,25–28 The Ethiopia DHS wealth index questionnaire was used to assess the wealth of the women. 29 Maternal characteristics registered on admission were retrieved from the entrance and enrollment sheet, including socio-demographic and maternal information. In addition, factors related to the success or failure of vaginal birth were recorded using the outcome registration sheet. Besides, maternal and fetal sheets were used to record maternal and fetal characteristics. The maternal section includes previous success VBAC, history of stillbirth (a baby who dies after 28 weeks of pregnancy, but before or during birth, is classified as a stillbirth), 30 the indication of primary CS, prior vaginal delivery, cervical dilatation, station of presenting part, premature rupture of the membrane (PROM), presence of meconium aspiration amniotic fluid, and place of labor initiated. The neonatal characteristics include sex, gestational age, birth weight, and Apgar score. The information was gathered by trained BSc midwives recruited from the selected hospitals.
Data quality assurance
A pre-test was conducted by taking 5% of the sample size at Haramaya hospital, which is not part of the study, and training was offered for data collectors, and the detailed illustration is indicated elsewhere. 24
Data management and analysis
Data were entered using the Epi-Data version.3.1 and later exported to STATA version 14 for analysis. Descriptive analysis was presented using tables and figures. The relationship between the dependent variables, success or failure of vaginal birth after trial of labor, and independent variables, such as socio-demographic factors, past, current, and labor-delivery history, was determined by a chi-square test or Fisher’s exact test with 95% confidence intervals (CI) and p < 0.05. Using crude and adjusted logistic regression, explanatory variables were identified.
Ethical consideration
Ethical clearance was obtained from the Institutional Health Research Ethical Review Committee (Ref. no. IHRERC/107/2020), a Health and Medical Science college, Haramaya University. The purpose, procedure and duration, possible risks, and benefits of the study explain using the local language. Then individual informed, voluntary, written, and signed consent was obtained from each participant
Results
Socio-demographic characteristics of the women
A total of 359 had previous CS scar, and 220 women who had tried vaginal birth after one CS were included in this study, 110 cases and 110 controls. The majority of participants were in the age category of 25–34 years (68.64%), lived in urban areas (65.00%), and had a minimum of primary education (35.77%) (Table 1).
Socio-demographic characteristics of participants in the trial of labor study at public hospitals, Eastern Ethiopia, 2020.
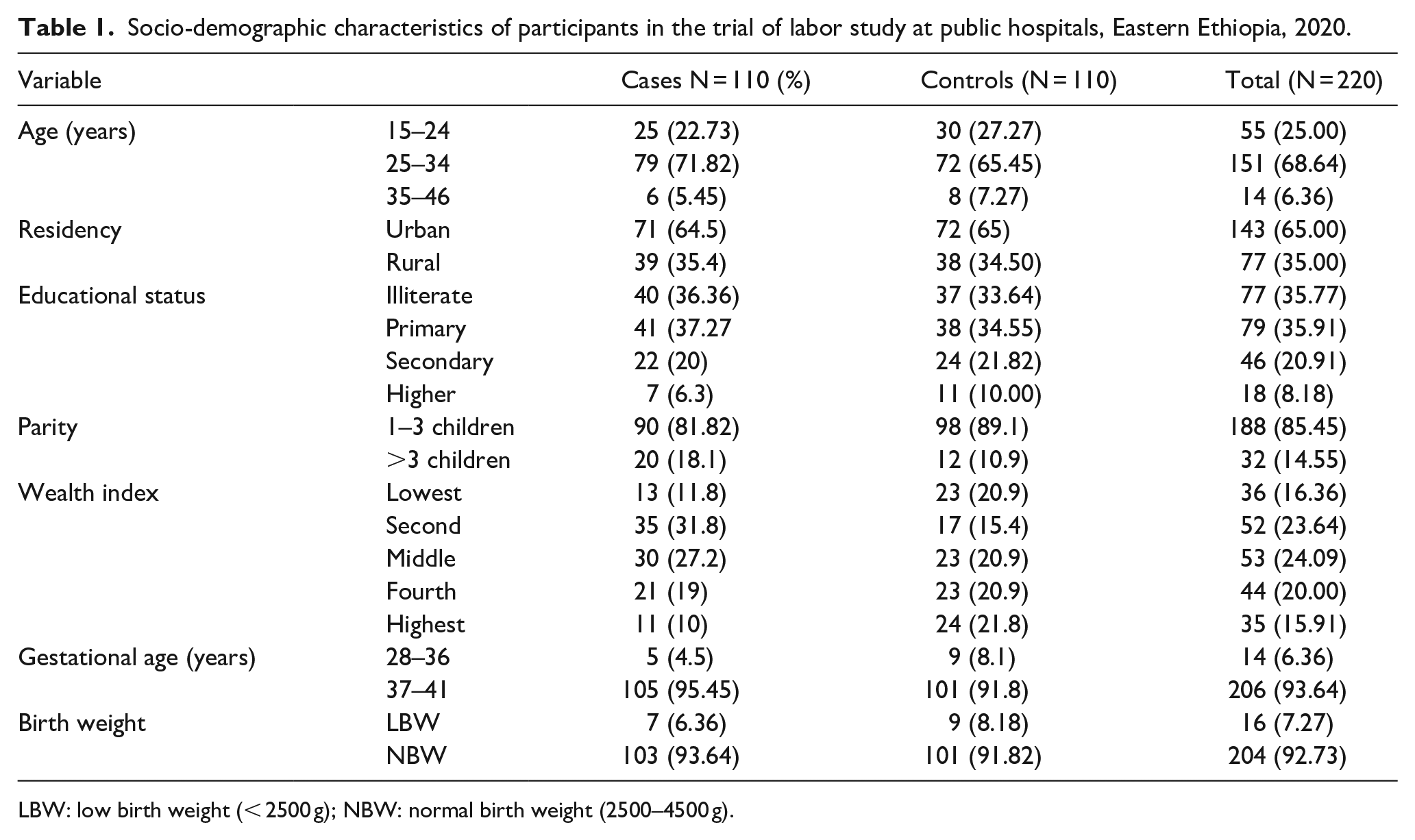
LBW: low birth weight (< 2500 g); NBW: normal birth weight (2500–4500 g).
Past and current obstetric characteristics of the women
Regarding previous delivery history, nearest to one-fourth of the women (23%) had a history of labor trial after previous CS, accounting for 35% of cases and 14% of controls. Prior vaginal birth was successful in 90.2% of those who attempted VBAC in the past. More than half of the cases and 23% of the controls had a history of vaginal birth prior to CS. History of stillbirth was discovered in 7% of the participants.
For current pregnancy, 59% of the cases were followed by partograph. The majority 84% among the cases and 75% among the controls followed antenatal care (ANC) (Table 2).
Obstetric characteristics of participants in the trial of labor study at public hospitals, Eastern Ethiopia, 2020.

CS: Cesarean Section; ANC: Antenatal Care.
Regarding mode of delivery for cases, 101 gave birth by spontaneous vaginal delivery, and the rest were born through instrumental delivery.
The common CS indication for previous CS (primary CS) was obstructed labor for both groups, but it was higher in the control group (29% versus 20%) (Table 3).
Primary CS indications among participants in the trial of labor study at public hospitals, Eastern Ethiopia, 2020.

CS: Cesarean Section; PROM: Premature Rupture of the Membrane.
The most typical CS delivery indication for current pregnancy (Control group) was obstructed labor (24.55%) followed by non-reassuring fetal heart rate (Figure 1).
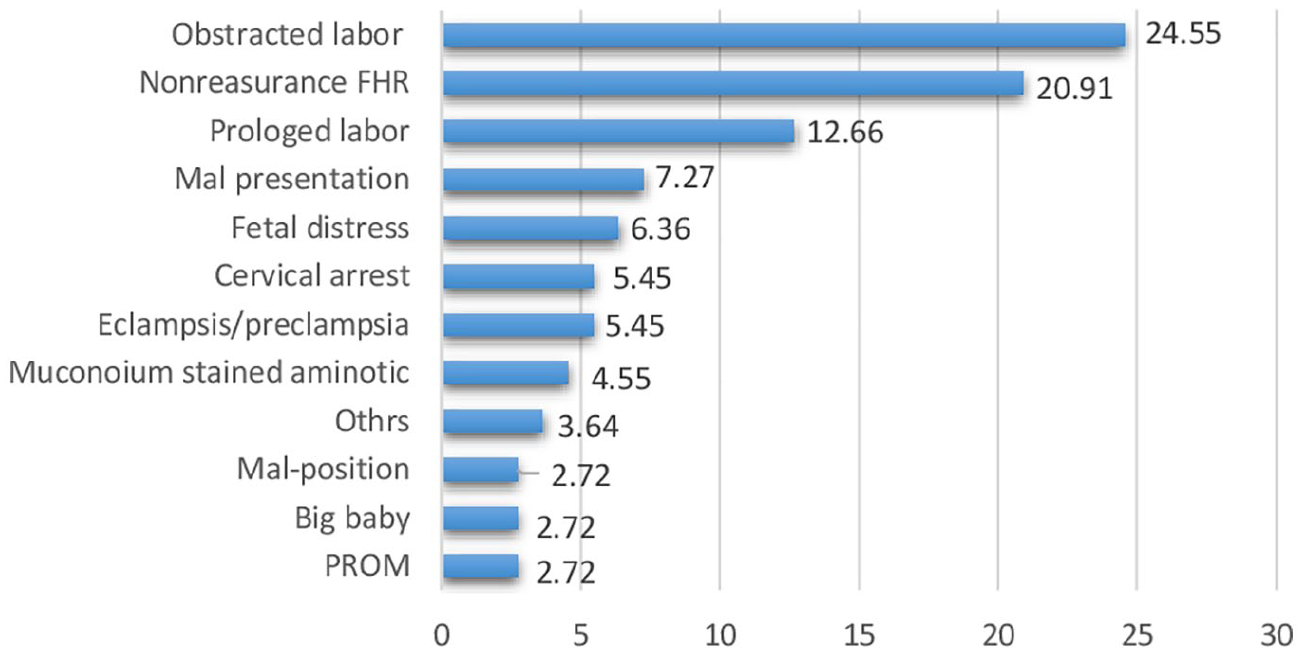
Indications of CS for the current pregnancy, trial of labor study at public hospitals in Eastern Ethiopia, 2020.
Predictors of the trial of scar after cesarean delivery
Living in rural residents had a significant association with the success of VBAC (AOR = 2.28; 95% CI (1.85, 12.41)). The women from the second to fourth wealth index have a higher chance of success VBAC. History of stillbirth (AOR = 0.07; 95% CI (0.02, 0.53)) was related to failed VBAC. The women who had a history of labor trial after primary CS (AOR = 3.52; 95% CI (1.34, 9.27)) and had a prior vaginal birth had a higher chance of success with VBAC (AOR = 2.97; 95% CI (1.07, 8.27)). Having ANC for current pregnancy increased the opportunity for a successful vaginal birth (AOR = 3.20; 95% CI (1.15, 8.87)). Regarding current delivery, the success of VBAC was less in the presence of meconium-stained amniotic liquor (AOR = 0.10; 95% CI (0.01, 0.75)). The women with cervical dilatation of 6–8 cm at admission have higher VBAC chances (AOR = 7.88; 95% CI (2.17, 28.55)). Whereas the women with the station of presenting part above ischial spine (−3 and −2) at admission have less opportunity to give birth by vaginal delivery after previous CS. Following the women with partograph had a positive association with success of vaginal birth (AOR = 4.26; 95% CI (1.90, 9.57)) (Table 4).
Determinants of success VBAC, the labor study trail at public hospitals, Eastern Ethiopia, 2020.
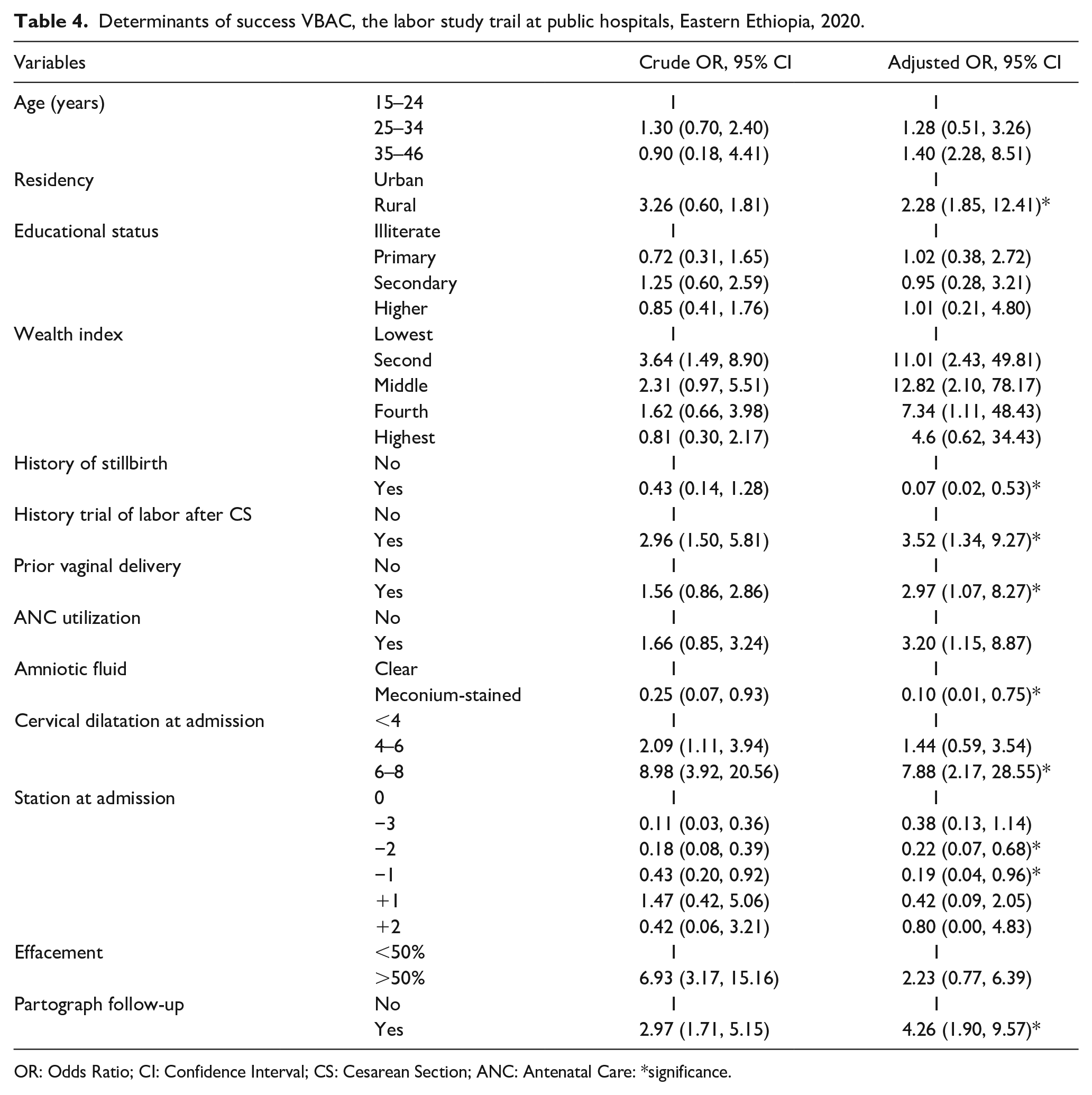
OR: Odds Ratio; CI: Confidence Interval; CS: Cesarean Section; ANC: Antenatal Care: *significance.
Discussion
VBAC is recognized as an alternative choice of subsequent natural delivery for women with a history of CS. It is also one approach to control the increase CS rate and complications related to repeat CS.
This study included 220 women who had prior CS scar and tried vaginal birth for their current pregnancy. Half of the women were failed VBAC, and the typical reason for current CS was obstructed labor (24.55%) followed by non-reassurance fetal heart rate. Several studies showed that these are the most common indication for CS delivery.31,32 In addition, history of stillbirth, history of labor trial after primary CS, prior vaginal birth, ANC, and cervical dilation were found predictors with VBAC.
Congruent to other studies,22,33 the women who had a stillbirth history were less likely to achieve VBAC’s success. This might have arisen from the assumption that the previous stillbirth history is the risk for recurrent stillbirth, 34 and CS is considered the safe mode of delivery. Similarly, the presence of meconium-stained amniotic liquor reduces the opportunity for success of VBAC by 94%; this corresponds with other studies that showed it was associated with failed VBAC.22,23 The occurrence of meconium-stained amniotic liquor is the risk for meconium aspiration syndrome. Women who attend ANC were 3.5 times more likely to achieve VBAC compared to their counterparts. This could be explained as ANC in pregnancy after a cesarean delivery is based on a risk assessment and enables the women to decide about the mode of delivery for the current pregnancy. 35 Congruent with other studies,22,23,28,36 this study indicates that the women who had a history of labor trial after CS were five times more likely to succeed in VBAC and have prior vaginal delivery before CS increased the chance of success by fourfold. This might arise from having vaginal birth experience decreased women stress to attend vaginal delivery.
The station of presenting parts −3 and −2 declined the success of VBAC by 78% and 81%, respectively. This corresponding with other studies that showed vertex −2 or higher had highly significant adjusted odds for failed TOLAC. 25 Likewise, the women followed by partograph four times more likely to achieve VBAC compared to their counterparts. This is explained by the fact that the women who followed the partograph had a better chance of detecting complications and receiving early treatment. The problem is that women who are not followed by the tool may be detected late, and the management will be CS delivery.
This study was part of a prospective follow-up study; all maternal information is taken before delivery. Hence, there is a high possibility of retrieving all necessary data without missing it. However, some past obstetric history and previous CS-related information were based on maternal recall, so it is not highly reliable and not included. Besides, a pre-pregnancy BMI was a significant predictor in other studies for the success of VBAC, yet in our research, this was not included as it was not possible to retrieve.
Conclusion
Past obstetric history, such as stillbirth, history of labor trial after primary CS, and prior vaginal birth, was the significant predictor for achieving VBAC. ANC and partograph follow-up were current obstetric characteristics that were positively associated with success of VBAC, respectively. Laboring women should be identified carefully for VBAC, considering these for the fetus and the women’s safety. Particular attention should be given to ANC and partograph follow-up. Encouraging the women to try vaginal birth during antenatal care utilization will increase the success rate, and this should be actively considered during ANC follow-up.
Footnotes
Acknowledgements
The authors thank Haramaya University, College of Health and Medical Sciences, for funding. They also thank data collectors and health professionals who work at the obstetric ward for their unreserved commitment and support.
Authors’ contributions
M.T. designed the study, participated in data collection, and analyzed and interpreted the results under the supervisor of N.A., K.T.R., and L.G. They (N.A., K.T.R., and L.G) also reviewed the draft result and approved the final result. All authors read and approved the final article.
Availability of data and materials
All the data of this study are available from the corresponding author on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is part of a PhD thesis, and the author(s) disclosed that Haramaya University provided financial support for data collection as part of higher education research sponsorship.