
Abstract
Background:
Despite growing awareness of the need for better healthcare and research focused on women, sex-based inequalities persist, resulting in poorer health outcomes for women. Particularly, women with congenital bleeding disorders (CBDs) receive less care, are underrepresented in research, and experience diagnostic delays compared to men with CBDs, despite both exhibiting symptoms.
Objectives:
To identify lived experiences and care needs of women with CBDs.
Design:
A qualitative study, including focus groups and semi-structured interviews.
Methods:
Women were eligible to participate if they were between 18 and 40 years old, diagnosed with a CBD, and able to speak Dutch. Focus groups or semi-structured interviews about the themes (1) healthcare, (2) social functioning, (3) work and education, and (4) sexuality and intimacy were conducted in person or online, based on women’s preference. Thematic analysis was conducted in MAXQDA.
Results:
Twenty-eight women with a CBD participated. In general, as well as in primary healthcare settings, women experienced a lack of knowledge among healthcare providers and a tendency to downplay their symptoms. Furthermore, the women expressed limited awareness among healthcare professionals (HCPs) regarding the impact of CBDs on mental health, particularly during specific life phases (e.g., transition to high school). Women described the need to schedule social activities around their menstruation cycle and emphasized how heavy and prolonged menstrual bleeding negatively affected their work and education. Feelings of insecurity and shame were reported, primarily related to menstruation. Additionally, insecurity due to bruises and bleeding affects women’s sexuality. Lastly, a lack of information regarding pregnancy and delivery was reported.
Conclusion:
Improved symptom recognition and a better understanding of the impact of CBDs on the daily life and mental health of women is needed. Accessible informational materials for both women and HCPs, as well as platforms for sharing experiences, may help facilitate this process.
Introduction
Despite global recognition of the need to improve healthcare and research focused on women, sex and gender inequalities persist (e.g., sex-biased research), resulting in poorer health outcomes for women.1,2 A patient population affected by this inequality is women with a congenital bleeding disorder (CBD).3,4 The term CBD refers to a group of conditions of the blood clotting system associated with prolonged and excessive bleeding symptoms that may occur spontaneously or following trauma or surgery. There are different types of CBDs that are caused by the deficiency of specific clotting factors, including hemophilia A and B (FVIII and FIX deficiency) where clotting factor levels <40% define a woman with hemophilia, and levels >40% define a hemophilia carrier who may have mild symptoms. 5 Other bleeding disorders include von Willebrand’s Disease (vWD; types based on von Willebrand Factor deficiency), platelet disorders, and rare coagulation factor deficiencies. 6 Hemophilia, among the most studied and known CBD, is inherited through the X-chromosome and therefore predominantly affects men. 7 This led to a research focus on male patients, and the misconception that women with hemophilia are asymptomatic.5,8 Women with CBDs may experience symptoms that are rarely recognized as abnormal, or a CBD may not be considered during diagnostic testing. 9 Consequently, women with CBDs often face exclusion from research,5,8 diagnostic delays, 10 insufficient care5,8, and inappropriate treatments (e.g., undergoing hysterectomy for heavy menstrual bleeding before a CBD diagnosis and exploration of alternative treatments 11 ).
Despite being underrecognized, the symptoms experienced by women with CBDs can significantly impact daily life. These include heavy or prolonged menstrual bleeding,8,9,12 bleeding as a result of ovulation, postpartum hemorrhage,8,9 heavy or prolonged nosebleeds, easy bruising, prolonged bleeds after surgeries or dental procedures,9,13 gastrointestinal bleeding,9,12 and muscle or joint bleeds. 9 Qualitative studies on the lived experiences of the impact of these symptoms in women with CBD are rare, 10 did not focus solely on women 14 or focus on specific situations, for instance reproduction. 15 Previous questionnaire-based research showed the profound negative impact of a CBD on various aspects of daily life. For instance, women with CBD refrained from social activities or were absent from work because of their menstruation, 16 experienced lower physical functioning in comparison to women without CBD, 17 and faced challenges during pregnancy and other reproductive phases.8,18 Another related and important aspect of daily life is sexual functioning, which may also be negatively affected by symptoms of a CBD such as heavy menstrual bleeding. However, research on sexual functioning in women with CBD is limited. 16
Given the reduced attention to the symptoms and complaints that women with CBDs may experience, and the potential impact on their daily lives, 8 , 16–18 raising awareness and improving care for women with CBD is essential. This study focuses on (young) adult women (i.e., aged 18–40 years) with CBDs because this phase is characterized by the formation of personal identity, social integration, exploration of sexuality, development of romantic relationships, considerations about starting a family, and career development.19,20 Additionally, focusing on this age group facilitates meaningful discussions in focus groups, whereas older women may have different experiences requiring a different study approach (e.g., taking menopause into account 21 ).The current qualitative study aimed at identifying and understanding the lived experiences and care needs of women with CBDs regarding different aspects of daily life.
Methods
Participants and procedure
Eligible participants were Dutch-speaking women between 18 and 40 years of age and diagnosed with a CBD (e.g., hemophilia carrier, vWD, or Glanzmann thrombasthenia) and known at a Hemophilia Treatment Center (HTC). An exclusion criterion was having an acquired bleeding disorder. Patients who are registered at the HTC of Amsterdam UMC received an invitation letter and the Dutch Hemophilia Patient Association (Nederlandse Vereniging voor Hemofilie Patiënten; voor iedereen met een erfelijke stollingsstoornis (NVHP)) issued a call on its platforms, inviting women to participate in a 2-h focus group or 1-h semi-structured interview, depending on the woman’s preference. Written informed consent was provided by all participants before participation. After participation, women received a €10 gift card. Data were collected between May 2022 and January 2023, continuing until enough overlapping insights were gathered among participants, providing sufficient depth to address the study’s aim (data sufficiency). 22 Approval of the Medical Ethics Committee of Amsterdam UMC was obtained (W22_164 # 22.213). The consolidated criteria for reporting qualitative studies checklist (COREQ) was used as the standardized reporting framework for this study. 23
Characteristics of participants
Sociodemographic (e.g., relationship status, age, education) and clinical data (e.g., diagnosis, clotting factor percentage, comorbidity) were collected through a self-created self-report questionnaire. Information on clinical data was supplemented by data from medical records if participants consented. This was only possible for patients from the Amsterdam UMC. The questionnaire also asked about feelings of restrictions in daily life due to CBD using two items: one with yes/no questions on various bleeding problems in daily life, and one yes/sometimes/no question on the extend of feeling restricted by bleeding problems overall. Participants could provide further clarification on the second question in an open text box.
Focus group and semi-structured interview
The focus groups (two to five participants per focus group) or semi-structured interviews were conducted in person at the Amsterdam UMC or online, based on the woman’s preference. Each focus group was led by two researchers (TvG (psychologist/PhD student), LT (psychologist/post-doctoral researcher)), where TvG was the interviewer and LT the observer who took fieldnotes. Semi-structured interviews were conducted one-on-one (TvG). Both interviewers are female, experienced in qualitative interview techniques and had no professional patient–provider relationship with the participating women. During the first two focus groups, a patient advocate from the patient association, NVHP, was present as a key participant to initiate discussions by sharing her and other women’s experiences. To create a safe and non-judgmental environment, the focus groups and interviews started with underlining the importance of keeping personal information confidential. After that, the aim of the study was explained, which focused on four aspects of daily life: (1) healthcare, (2) social functioning, (3) work and education, and (4) sexuality and intimacy. The importance of these themes was based on literature5,8,16,17 and expert experience (MD). A conversation guide was developed to cover these themes. The conversation guide provided structured prompts and guidance throughout the focus groups and interviews to help the interviewers maintain a comfortable and open dialog. Additionally, open-ended follow-up questions were included to ensure important aspects were addressed, while allowing flexibility to adapt to the flow of the discussion and keep the focus on the four themes. During the focus group discussions, the participating women first wrote their thoughts about the four themes on post-its or a digital equivalent, which were organized by content and subsequently discussed in the group. This was an effective way to enhance engagement, elicit opinions from all participants about a sensitive topic and improve understanding of different perceptions. 24 During semi-structured interviews, only open-ended questions from the interview guide were used. To ensure data met the study’s aim, the content of semi-structured interviews and focus groups was periodically evaluated within the larger study team.
Analyses
The IBM Statistical Package for Social Sciences (SPSS) version 28.0 was used to conduct descriptive analyses to characterize the participants. The focus groups and interviews were audio recorded, transcribed verbatim and analyzed in MAXQDA Plus 2022 (by VERBI software) using thematic analysis, which included several steps: (1) familiarizing with the data and highlighting relevant text fragments, (2) grouping relevant text fragments to generate initial codes, (3) sorting the different codes into the pre-themes and identifying subthemes, (4) reviewing and discussing themes, and (5) defining the final themes. 25 If necessary, adjustment or additions were made to the pre-defined themes that formed the conversation guide. Two researchers (TvG, LT) conducted the analysis, where one researcher (TvG) analyzed all transcripts and 17% was double coded and analyzed independently (LT). Analyses were discussed in the larger study team and consensus on the final themes was reached. Finally, two patient advocates (vWD (age 38 years) and carrier of hemophilia A (age 53 years)) were asked to provide feedback regarding the interpretation and completeness of the results to further ensure that the findings accurately reflect patients’ experiences, 26 particularly within the women with a CBD community. The subthemes are reported in an order that reflects their discussion frequency.
Results
Participants
In total, 28 women with CBD participated in 6 focus groups and 12 semi-structured interviews. Their mean age was 29.4 years (range 19–40). Nine of the participating women are hemophilia A or B carrier, and two have hemophilia with a clotting factor under 40%. Eight women have vWD, and four women have other rare factor deficiencies. One woman has Glanzmann thrombasthenia, and two women have a combined diagnosis (see Table 1).
Participant characteristics (N = 28).

NVHP: Nederlandse Vereniging voor Hemofilie Patiënten; voor iedereen met een erfelijke stollingsstoornis; SD: standard deviation.
No participants aged 18 years.
Glanzmann thrombasthenia.
“Other” were two women who have two bleeding disorders combined.
Chronic lung disease, neurological disorder, digestive disorder (n = 2), dermatological condition, hematologic disorder other than CBD.
Participants highest and completed level of education. Education level was categorized according to ISCED levels: Primary education (ISCED level 1), Secondary education (ISCED levels 2 and 3), Tertiary education (ISCED levels 6 and 7).
Based on the questionnaire completed before the focus groups or interviews, more than half (57%) of the participating women (sometimes) felt restricted because of their bleeding tendency. They felt limitations due to heavy menstruations, nosebleeds, bleeds after surgery, or during their postpartum phase. They reported having to be constantly alert and careful, for example at work, during sport and holidays.
Qualitative data of the focus groups/interviews
Healthcare
Regarding healthcare, four themes were identified: (1) knowledge of healthcare professionals (HCPs), (2) outpatient care, (3) treatment, and (4) mental health awareness. A selection of associated quotes is presented in Table 2.
Overview of the identified themes and associated quotes regarding healthcare.

All quotes were translated into English. HTC: Hemophilia Treatment Center.
Most women reported a lack of knowledge about CBDs among HCPs working outside the HTC. In particular, they felt that general practitioners were unfamiliar with bleeding disorders in women and therefore, often did not recognize symptoms (e.g., heavy menstruation) or downplayed them, resulting in a delayed diagnosis. Some women with a CBD had received care at a general hospital, where they or their family felt a continuous need to remain alert to ensure appropriate treatment and medication were provided. Additionally, some women with a CBD reported managing their care independently. For example, by using tranexamic acid pills after surgery, without consulting an HCP.
Most participating women did not have regularly scheduled outpatient care at an HTC. Most women felt that regular visits, for example, once every 1 or 2 years, would be sufficient as they had no or limited complaints. Only a few women with a CBD reported preferring more frequent outpatient visits. Furthermore, most women with a CBD know how to reach out to the HTC if needed and find it easy to do so. The HTC is described as a welcoming place. Some women with a CBD mentioned that they prefer multidisciplinary care (e.g., including psychologists, gynecologists, social workers) and information adapted to each patient’s specific phase of life (e.g., transitioning to high school, family planning phase).
Only a few women with CBD receive scheduled treatment. These women reported that planning intravenous injections before school or injecting themselves can be difficult and that (additional) treatment during menstruation is necessary. They also noted that treatment allowed them to have a “normal” life. Other women with CBD sometimes use a nasal spray or pills (tranexamic acid) in case of minor bleeds, during their menstruation, or after surgery. Importantly, the women report that the most used treatment for heavy menstruation are hormonal contraceptives, such as oral contraceptive pills or intra uterine devices (IUDs), and women report to be compliant with these treatments. Women perceived these treatments as helpful, but some expressed reluctance to use these hormonal options and a preference for more information about options of non-hormonal treatments.
A need for increased mental health awareness was mentioned by some of the participating women with CBD. They noted that HCPs often solely focus on medical aspects and overlook the impact of bleeding disorders on their daily life and mental health. The women need providers to ask the right questions, assess needs, and follow-up or ask more detailed questions. Some women with CBD highlighted the need to raise awareness about the mental health of young girls and women, particularly at the start of their menstruation, to ensure they are adequately prepared.
Social functioning
From discussions about how CBDs can influence social functioning, five themes were identified: (1) disclosure about diagnosis in social interactions, (2) understanding and support from others, (3) effect on family, (4) engaging in social activities, and (5) feeling insecure/ashamed. A selection of associated quotes is presented in Table 3.
Overview of the identified themes and associated quotes regarding social functioning.
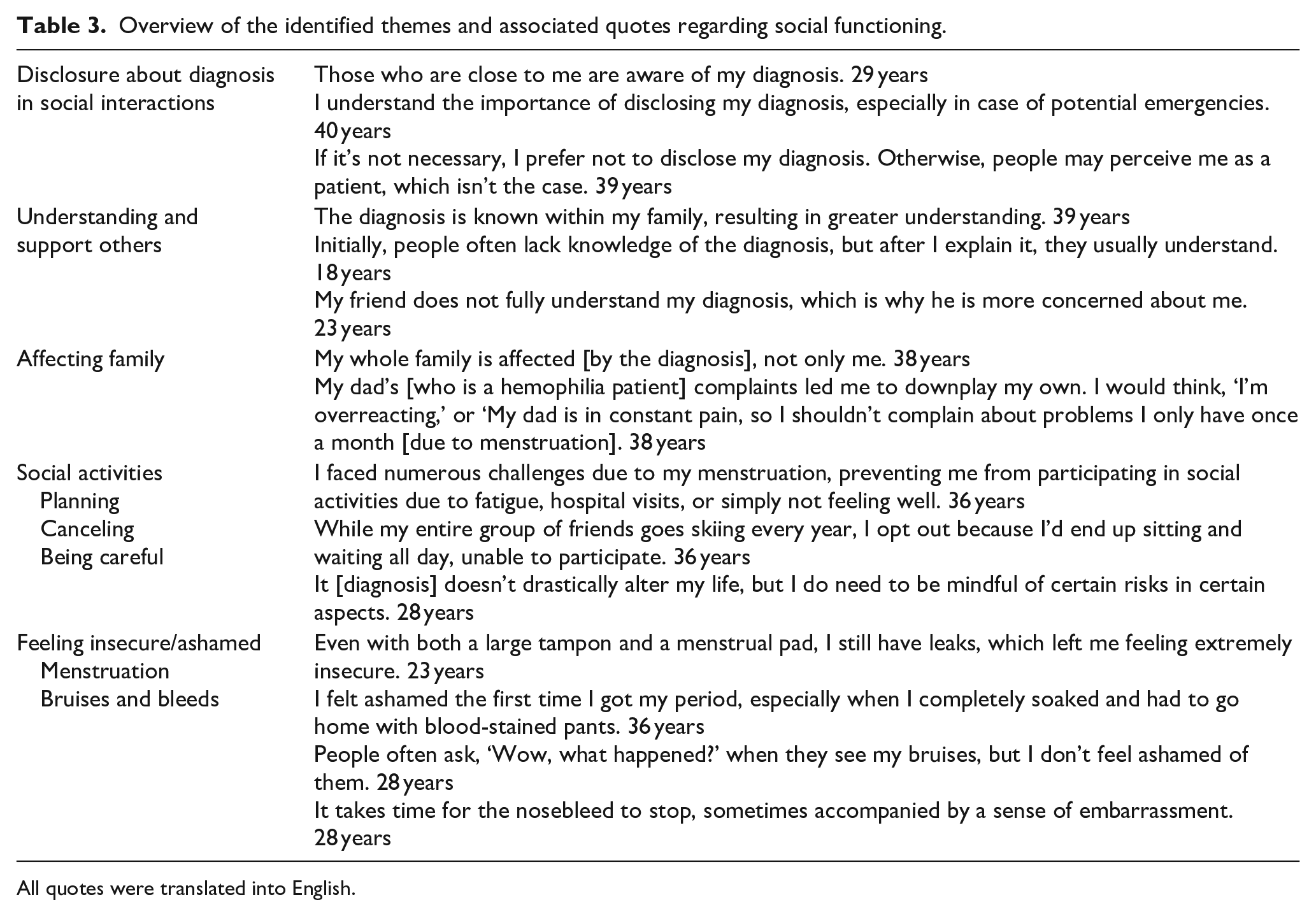
All quotes were translated into English.
Most women with CBD reported they only disclose their diagnosis to people within their close social circle (e.g., family and friends). Disclosure to others is typically motivated by practical considerations (e.g., knowing emergency procedures). Disclosure often happens naturally, when the topic arises in conversations. Most participants stated they do not find it difficult to disclose their diagnosis. Nevertheless, a few women expressed difficulty due to concerns about being perceived differently by their peers. Some women chose to not disclose their CBD, as they are not affected by any symptoms in their daily lives.
Most women felt they received understanding and support from others, and that people close to them understand their diagnosis well. Particularly family members tend to understand their situation well as they often share the same diagnosis and related consequences. For instance, sharing experiences with a sibling results in a stronger connection and feeling supported. Some women mentioned that explaining their diagnosis is necessary for others to understand its implications and that a lack of understanding can lead to misunderstandings or overprotectiveness.
During focus groups it became evident that a bleeding disorder not only influences the women with a CBD individually but also affects their families. Family members may feel anxious or become overprotective toward the women, especially if a male relative shares the diagnosis and experiences many complications. This was particularly the case for hemophilia patients, since symptoms in men tend to be more severe due to the inheritance of hemophilia through the X-chromosome. Conversely, because of the severity of symptoms in male family members, women’s complaints may be downplayed. They are often seen as “only” being a carrier of the disease.
Negative impact on engaging in social activities was reported in three ways: planning, canceling, and being careful. First, some women with a CBD mentioned consciously planning their activities beyond their menstruation. Reasons for such planning include the fear of period leaks, fatigue resulting from low iron levels, or cramps. Second, a heavy menstruation was often a reason to cancel activities. Other reasons were hospital visits, bleeds, or too risky activities. Lastly, some women with a CBD mentioned they were extra careful during social activities such as sports or travels, due to concerns about bleeding and bruising.
Feeling insecure or ashamed can be the result of heavy menstruation, bruises, or bleeds and negatively affects social functioning. Most women with a CBD reported fearing period leaks. Regarding bruises, some women with a CBD mentioned being aware of the visibility of their bruises but not feeling ashamed about it, despite people reacting negatively to bruises. Few women with a CBD reported experiencing spontaneous and heavy nosebleeds, leading to feelings of shame in social situations.
Work and education
Regarding the aspect work and education, four themes were identified: (1) understanding and support at work/school, (2) disclosure about diagnosis at work/school, (3) impact of menstruation, and (4) career choice and occupation. A selection of associated quotes is presented in Table 4.
Overview of the identified themes and associated quotes regarding work and education.

All quotes were translated into English.
Most women with CBD reported understanding and support from colleagues and employers at work, or teachers and classmates at school/university. Support manifested in various forms, including flexible work arrangements such as working from home or adjusting shifts (e.g., for hospital visits or during menstruation). However, some women encountered problems with employers and teachers who restricted toilet visits to break times or denied days off during heavy menstruation. Some women with CBD also encountered challenges with teachers who did not understand the difficulty of keeping up in class when having low iron levels, or teachers who did not permit skipping gym classes.
As also discussed in previous aspects of daily life, disclosure about the diagnosis also played a role at work/school. Yet, women with CBD were more reluctant to disclose their diagnosis to colleagues, employers, teachers, and classmates. Some women chose to share information about emergency procedures only. Alternatively, some women with CBD disclosed their diagnosis, often prompted by questions about bruises or when using crutches. Furthermore, few women with CBD mentioned that the decision to disclose depended on the workplace atmosphere, and they found it easier to disclose to female colleagues or employers.
Impact of menstruation on work and education was mentioned by many participating women with CBD. As discussed in previous sections on daily life, menstruation and the risk of period leaks often led to feelings of insecurity and shame at work or school. Additionally, low iron levels and even fainting were reported as factors negatively affecting work and school performance. Pain, such as menstrual cramps, sometimes made attending work of school impossible. Some women even stated that without hormonal contraception to suppress menstruation, work would be impossible for them.
Few women with CBD indicated that their diagnosis influenced their career choice and occupation. They recognized that certain physically demanding jobs are unfeasible, such as jobs involving long working hours of standing. Other women with CBD mentioned being mindful of risks at work and taking steps to avoid potentially risky situations. Lastly, a few women with a CBD expressed an interest of working in health and healthcare due to their personal experiences with their diagnosis.
Sexuality and intimacy
Five themes, related to sexuality and intimacy, were identified: (1) feeling insecure/ashamed, (2) communication with HCP, (3) easy bruising and bleeds, (4) partners’ understanding and support, and (5) disclosure about diagnosis in relationship/dating life. Most women mentioned to identify as heterosexual. A selection of associated quotes is presented in Table 5.
Overview of the identified themes and associated quotes regarding sexuality and intimacy.
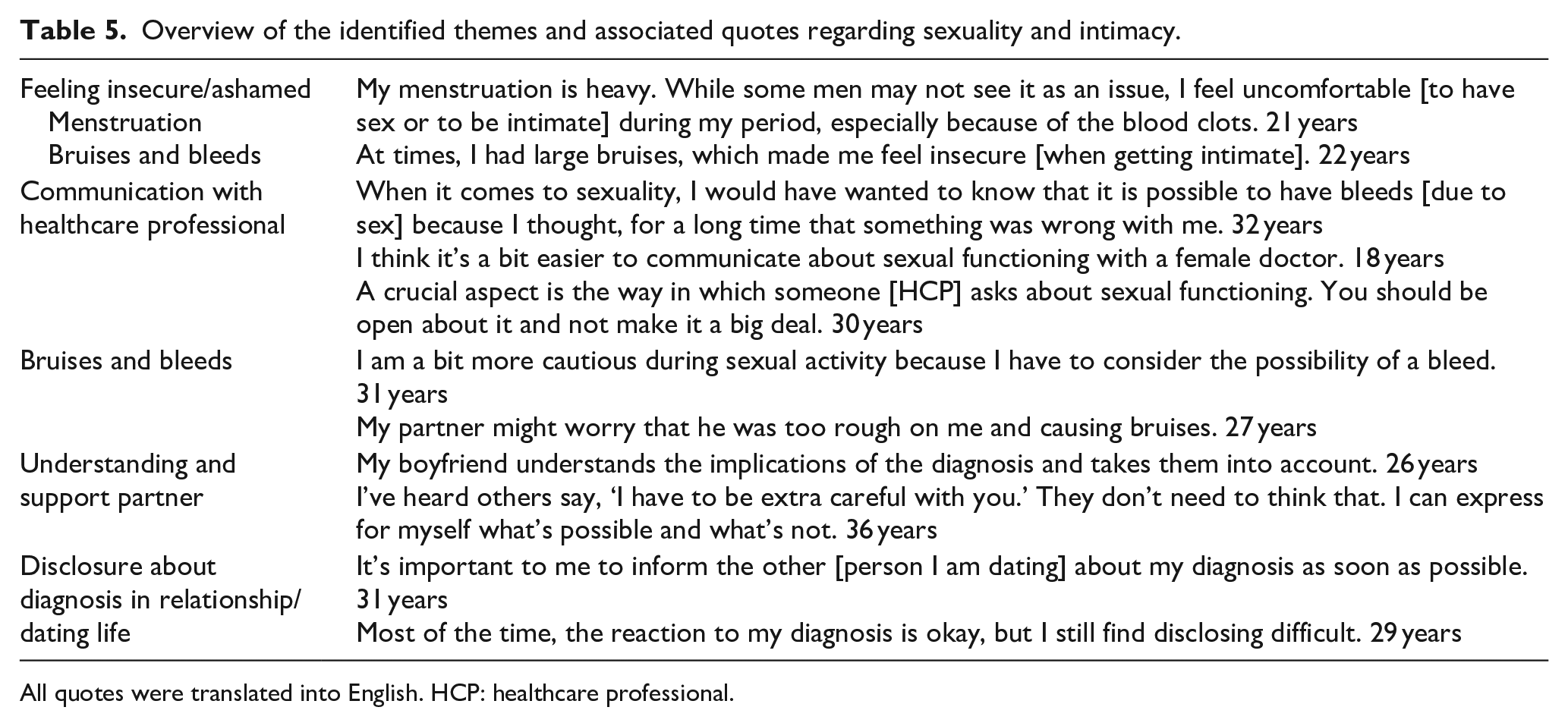
All quotes were translated into English. HCP: healthcare professional.
Most women with a CBD reported feeling insecure or ashamed about engaging in sexual activity due to their heavy menstruation. Most women with CBD refrained from sexual activity during their prolonged menstruation because of concerns about blood loss, lack of sex drive, or a partner’s discomfort with menstruation. Additionally, for some women, the unpredictability of their cycle and the unexpected onset of menstruation contributed to feelings of shame. Vaginal bleeding outside the normal menstrual period was also common, further exacerbating feelings of insecurity around sexual activity or intimacy.
Several women with CBD emphasized the importance of open communication with an HCP regarding sexual function. Currently, there is a lack of communication and information, leading to women with a CBD being unaware of the possibility of bleeding following vaginal penetrative sex. Most of the women with a CBD stated that HCPs should initiate sexual health-related discussions. Some also mentioned their preference for a female HCP or a nurse addressing sexual functioning. Furthermore, most women with a CBD recognized the sensitivity of the topic and underscored the importance of the HCP’s attitude in discussing and normalizing the topic.
Bruising and bleeds may be a result of being sexually active. For example, penetrative sex could result in bleeding, which led to some women with CBD being anxious about being sexually active or worried because they initially did not understand the cause of the bleed. Some women with CBD mentioned there were periods in which they avoided sexual activity to prevent bleeding. Furthermore, some women with CBD mentioned they had bruises or a sore feeling as a result of being sexually active. However, this did not hinder them from being sexually active again. Few women with CBD expressed feelings of guilt toward their partners about having to deal with their bruises.
Most women with CBD reported their partner is understanding and supportive regarding their bleeding disorder. Partners often take the diagnosis into account and remain calm in case of a bleed. Some women with a CBD mentioned their partner is overly cautious, which they do not appreciate.
Disclosure about the diagnosis when dating was also discussed. Most women with CBD mentioned being open about their diagnosis, with some choosing to disclose at the beginning of a relationship, whereas others waited until it came up naturally in conversations. A few women with CBD stated they did not disclose their diagnosis because they are not affected by symptoms of the bleeding disorder and some expressed nervousness about disclosing due to concerns about potential reactions from partners.
Reproductive choices and pregnancy
Despite not being a topic from the conversation guide, the women also elaborated on their reproductive choices and pregnancies, including: (1) information provision, (2) concerns, and (3) genetics. A selection of associated quotes is presented in Table 6.
Overview of the identified themes and associated focus group and interview quotes regarding reproduction choices and pregnancy.
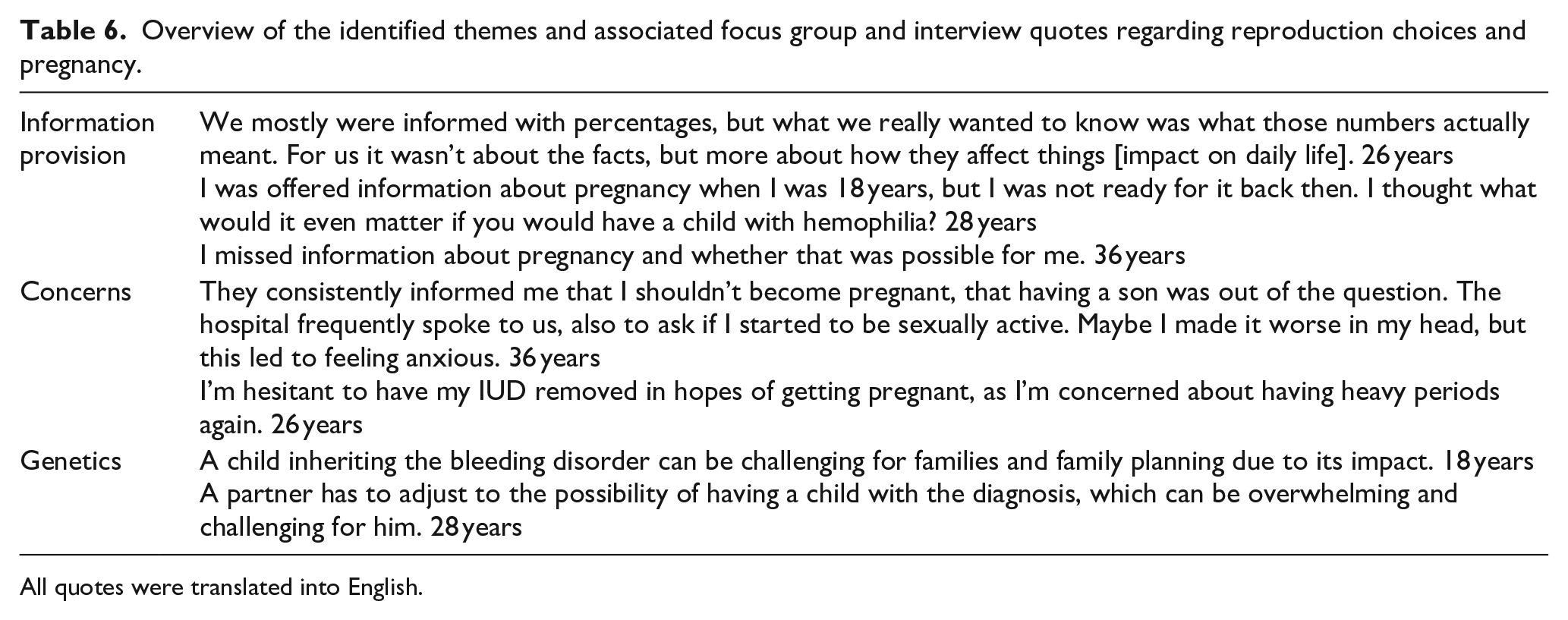
All quotes were translated into English.
Most of the women with CBD reported a lack of clear information regarding reproduction, genetic aspects, and the safety of pregnancies and giving birth. Information was often unclear or only provided once. In addition, women experienced poor timing of information delivery—either too early (e.g., 18 years) or too late (e.g., shortly before trying to conceive or when already pregnant). Furthermore, women expressed a need for improved and repeated information, more frequent check-ups at the HTC, and the opportunity to share experiences with other women. A minority of the women with CBD felt well-informed and supported by HCPs.
Concerns regarding pregnancy were reported by many of the women with CBD, which also affected their reproductive choices (i.e., being anxious about trying to conceive, feeling the necessity to do prenatal tests). Concerns about menstruation, when trying to conceive and not using contraceptives, were mentioned and withheld some women from trying to get pregnant. Some women with a CBD stated that when they received information from the HCP about pregnancies and deliveries (e.g., needing a medicalized delivery) this led to feeling anxious and nervous. Few of the, mostly younger, women even mentioned they are anxious about unintentionally getting pregnant because of their CBD and are therefore nervous when having intercourse.
Regarding genetics, most women with a CBD knew about the risks. Some women mentioned a child with a bleeding disorder may affect them as a parent or the family, due to the need for extra care for that child. Furthermore, some women with a CBD reported the potential impact of inheritance on their partners, meaning that their partners must consider the possibility of having a child with a CBD and learn about what it entails. Few women described they had a partner who reacted negatively to the possibility of having a child with a bleeding disorder.
Patient advocate perspective
The two patient advocates recognized the identified themes from their own experiences and experiences from other patients (e.g., shared during events of the NVHP), especially the impact on mental health and the importance of being aware of the life phase of the women with a CBD. Furthermore, the patient advocates recognized the importance of communication about possible difficulties during sexuality and intimacy. However, they also acknowledged the risk that information about possible difficulties may cause additional feelings of anxiety or worries regarding sexual activity. Lastly, the patient advocates stated they understand the concerns of a heavy menstruation when not using contraceptives. However, this could be resolved when heavy menstruation would be treated with other treatments such as coagulation factor.
Discussion
The current study highlights the need for greater awareness and tailored support for women with CBDs, as well as peer support. We found that CBD has a negative impact on women’s daily lives, while also revealing feelings of insecurity and shame, thereby extending previous research.8,16–18 The participating women reported that their symptoms were often downplayed in primary care and general hospitals, and there was a lack of awareness regarding the impact of CBDs on mental health, particularly during specific life phases (e.g., transition to high school or adolescence). Difficulties experienced by women during these phases of life have also been reported previously, 27 showing lower health-related quality of life scores in adolescent girls, which may be attributed to adolescence being a period characterized by insecurities and the onset of menstruation.
Women participating in our study also reported the need to plan social activities and adjust their work/education around their symptoms. These findings are consistent with those of another qualitative study involving young adult women with CBD, whose age range closely matched that of our participants. 14 Furthermore, our results correspond with a questionnaire-based study that found poorer scores on work and education functioning, which were attributed to heavy menstruation. 28 Most women in the current study reported to use contraceptives to manage their heavy menstruation. However, as noted by the patient advocates, it may also be beneficial to consider coagulation factor treatment, to not only manage menstrual bleeding but also prevent excessive blood loss with resulting iron deficiency. Such treatment could be especially helpful for those planning to have children.
Next to the impact of heavy menstruation on daily life, women in our study reported experiencing intermenstrual bleeding. This aligns with previous research indicating that irregular bleeds or spotting between menstrual cycles is common among women with CBDs.29,30 However, these studies emphasize the need for more research. Although an IUD may help prevent or reduce these bleeds, it can also cause irregular bleeds or spotting as a side effect. 31 In our study, most women reported using contraceptives to manage their heavy menstrual bleeding, but we did not investigate treatment or strategies for managing intermenstrual bleeding. We think considering coagulation factor treatment could be helpful in managing both intermenstrual and heavy menstrual bleeding.
Additionally, the women expressed a lack of knowledge and information regarding sexuality and intimacy; some women with a CBD did not know that bleeding after penetration is possible, leading to insecurity and shame. A lack of knowledge and information regarding reproductive choices and pregnancy was also reported. Since the impact on reproductive choices and pregnancy has been thoroughly studied previously, 15 this theme was initially not included in the conversation guide. However, the impact of a CBD on reproductive choices and pregnancy, along with the lack of knowledge and information on these topics, was frequently reported by the participating women and subsequently added as a theme. This highlights the need for improved care through timely preparation and better communication, as supported by previous research. 18
There are some initiatives to increase the awareness toward women with CBDs in healthcare. The initiation of a new nomenclature in which the categories are severe, moderate, or mild hemophilia or, symptomatic versus asymptomatic hemophilia carrier instead of just hemophilia carrier fulfills in the need for better medical care for these women. 5 Additionally, one of the Principles of Care (an initiative of the Women and Bleeding Disorders Working Group of the European Association for Haemophilia and Allied Disorders and the European Haemophilia Consortium) states to involve women with CBDs in registries, clinical research, and innovation. 4 The findings of the current study, particularly the findings regarding providers and care needs, underline the importance of such initiatives. Yet, more research is needed to help HCPs offer better care, information provision, and education to women with a CBD. 32 Especially more awareness in primary care would result in better health outcomes for women. 33 Women with a CBD in this study reported that general practitioners are often unfamiliar with bleeding disorders and tend to downplay symptoms. When general practitioners recognize symptoms of bleeding disorders, it can help in diagnosing women with a CBD early and offering the right care. This includes referring women to HTCs, where their specific needs can be addressed. Additionally, a proactive approach by HCPs from HTCs towards women with CBDs could be beneficial. For example, through regular contact, HTCs could reduce barriers for women with CBDs to seek and receive appropriate care.
It is understandable not every HCP feels competent enough to inform or address every aspect a woman with a CBD might be impacted on. Therefore, a multidisciplinary approach and referral to specialized professionals is necessary. For example, aspects of the mental impact of a CBD may be best addressed by a psychologist, sexuality and intimacy by psychologists or sexologists, and referrals to gynecologists may be indicated for questions about reproductive choices and pregnancy. A training on how to discuss sensitive topics, like sexuality and intimacy, could also be helpful. Additionally, providing informational material (e.g., leaflets or links to informative video/animation) could be an accessible way of informing and educating both women with a CBD and HCPs. An educational and insightful checklist to provide insight in the heaviness and duration of the menstruation, and if this is in the normal range could be useful. An example of such a checklist is the 7-2-1 rule or menstruation symptom check.34,35 A valuable resource for the women with a CBD themselves is to have contact with and learning from other women with a CBD, for example through a patient association. During the focus groups, the participating women mentioned the value of hearing about experiences of other women with the same condition.
HCPs in the HTCs were already reported to be warm and welcoming and care in an HTC is preferred over general care given their expertise. Care with awareness for the impact of a bleeding disorder on mental health is important, as stated by the women with a CBD and in previous research. 3 Next to this, novel treatment options for women may become available in the near future. 36 Insight into the impact on mental health can be measured with patient-reported outcome measures (PROMs),37,38 for which Patient-Reported Outcomes Measurement Information System (PROMIS®) is recommended.37,39–41 The obtained insight on mental health can then be used in the communication between patient and HCP, preferably a psychologist, and could support in the (medical) decision making.40,42,43 Also, for sexual functioning the PROMIS measures could be used. The PROMIS® Sexual Function and Satisfaction offers insight into multiple components of sexual functioning 44 and is currently being translated and validated in the Netherlands.
Limitations
Next to adding valuable insights, certain limitations of this study should be considered. One limitation is the potential bias in included women. A convenience sampling method was used, meaning we did not specifically attempt to include women with more severe symptoms or from diverse socioeconomic backgrounds. Regarding severity of symptoms, we included women with a broad range of symptoms. Although we determined data sufficiency was reached, it is possible that outcomes could have been slightly different if only women with severe symptoms had been included. Most women had a higher educational background, which may introduce bias. Notably, despite their higher education level, which is typically associated with better access to health information, many reported a lack of information about the impact of a CBD. Additionally, the participating women with a CBD might be women that feel more empowered to talk about the impact of their bleeding disorder. To minimize this limitation, we offered the option of interviews instead of focus groups for those who might feel less empowered to participate in a group setting. No differences in responses were observed between women in focus groups and those interviewed individually.
Recommendations for future research
Recommendations for future research include the inclusion of women with diverse sexual orientations and cultural backgrounds, as well as attention for the experiences of family members or partners. Additionally, future research should explore the impact of CBD on mental health in more detail. Although this study highlighted the effect of a CBD on women’s mental health, future research should aim to identify specific psychological challenges and the types of support women with CBD sought or needed. These aspects could be assessed using PROMs.
Conclusion
In conclusion, this in-depth qualitative study underscores the need for improved symptom recognition and a better understanding of the impact of a bleeding disorder on the daily and social life, and mental health of women with CBDs. There is a need for accessible informational materials (for patients and HCPs), educating general practitioners and HCPs from general hospitals, and platforms for women with CBDs to share experiences. Additionally, the provision of appropriate, multidisciplinary care, and tools or strategies to gain insight into and address the impact of bleeding disorders is essential.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251362582 – Supplemental material for A qualitative study on the impact of bleeding disorders on the daily life of Dutch women
Supplemental material, sj-docx-1-whe-10.1177_17455057251362582 for A qualitative study on the impact of bleeding disorders on the daily life of Dutch women by Tessa C. M. van Gastel, Lorynn Teela, Manon E. L. Degenaar-Dujardin, Vicky Lehmann, Marjolein Peters, Karin Fijnvandraat and Lotte Haverman in Women's Health
Footnotes
Acknowledgements
We thank all patients who participated in this qualitative study, Joyce van Steenbergen, Eke Hullegie, and Cathy Verbraeken for sharing their expertise, and Nadia van Silfhout for her assistance during focus groups. We also thank Marlène van Beijlevelt, Dr. Michiel Coppens, and the Dutch Hemophilia Patient Association; for everyone with a hereditary bleeding disorder (NVHP) for their help recruiting participants. Additionally, our appreciation goes to Stichting Haemophilia for their financial support.
ORCID iDs
Ethical considerations
This study was approved by the Medical Ethics Testing Committee at Amsterdam UMC, the Netherlands (approval no. W22_164 # 22.213) on May 12, 2022.
Consent to participate
Written informed consent was provided by all patients for participation and the use of their data for this study.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by funding from Stichting Haemophilia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.