
Abstract
Background:
Puerperal sepsis is a severe bacterial infection that occurs in women between the beginning of labor or rupture of the membrane and the 42nd day following birth. In Ethiopia, it is the fourth leading cause of maternal death, accounting for 14.7% of pregnancy-related deaths. The risk factors for puerperal sepsis are not well understood in Ethiopia, particularly in southwestern Ethiopia.
Objectives:
This study aimed to identify risk factors for puerperal sepsis among postpartum women at public hospitals in the Dawro Zone, Southwest Ethiopia.
Design:
A facility-based unmatched case–control study.
Methods:
From February 1 to April 30, 2023, 260 participants (65 cases and 195 controls) were included in the study. The cases were postpartum women who were diagnosed with puerperal sepsis, whereas the controls were postpartum women confirmed to be free from puerperal sepsis. Cases selected consecutively, and controls enrolled via systematic random sampling. Data were collected via an interviewer-administered questionnaire and medical records review. STATA version 17 was used for analysis. The associations between variables were analyzed via a binary logistic regression model. A p value <0.05 was considered statistically significant.
Results:
Rural residence (adjusted odds ratio (AOR): 3.62; 95% confidence interval (CI): 1.40, 9.33), no formal education (AOR: 4.40; 95% CI: 1.25, 15.49) compared with college or above, no antenatal care (ANC; AOR: 14.04; 95% CI: 4.56, 43.20) compared with three or more ANC visits, prolonged rupture of the membrane above 24 h (AOR: 9.51; 95% CI: 2.49, 36.35), home delivery (AOR: 3.06; 95% CI: 1.26, 7.49), ⩾5 vaginal examinations (AOR: 7.44; 95% CI: 2.77, 19.94), and cesarean section (AOR: 2.89; 95% CI: 1.13, 7.42) were significantly associated with the puerperal sepsis.
Conclusions:
Rural residence, lack of formal education, lack of ANC follow-up, prolonged rupture of membrane, home deliveries, frequent vaginal examinations, and cesarean section deliveries increase puerperal sepsis. Targeted intervention requires on modifiable risk factors such as ensuring at least on ANC, promoting institutional delivery, ensuring timely administration of appropriate antibiotics for prolonged rupture of membrane, avoiding unnecessary vaginal examinations and cesarean section.
Plain language summary
Introduction
Puerperal sepsis is defined as a genital tract infection occurring at any time between rupture of the membrane or labor and the 42nd day after childbirth with two or more of the following criteria: pelvic pain, fever (temperature ⩾38.5°C on any occasion), abnormal vaginal discharge, and delay in uterine involution (less than 2 cm/day) during the first 8 days. 1 Recently, the World Health Organization updated the definition of maternal sepsis by including infection during pregnancy and post-abortion period. Maternal sepsis is now defined as a life-threatening condition characterized by organ dysfunction resulting from infection during pregnancy, childbirth, post-abortion, or postpartum period. 2
Puerperal sepsis is a significant cause of maternal morbidity and mortality, particularly in resource-limited countries such as Ethiopia.3,4 A meta-analysis conducted in China including studies from 2010 to 2020 estimated the pooled incidence of puerperal sepsis to be 4.95% with individual study incidence rate ranging from 0.30% to 32.67%. 5 Another systematic review and metanalysis in sub-Saharan Africa reported an overall pooled prevalence of maternal sepsis to be 19.21%. 6 In 2017, an estimated 5.7 million women developed sepsis during pregnancy, delivery or the postpartum period. 7 Puerperal sepsis is rated as the sixth leading cause of disease burden for women of reproductive age (15–44 years), 8 and sepsis is responsible for 11% of global maternal deaths. 9 It also accounts for 15% of all maternal deaths in developing countries. 3
Puerperal sepsis has been linked to a number of risk factors, some of which include prolonged labor, cesarean section delivery, frequent vaginal examination, retained products of conception, unhygienic practice during labor, delivery, postpartum care, prolonged rupture of membranes, instrumental delivery, and weakened or impaired immunity.10 –13 If untreated as early as possible, puerperal sepsis can cause complications such as acute and chronic pelvic inflammatory disease, disseminated intravascular coagulation, prolonged hospital stay, septicemia, infertility, septic shock, and death.14 –17
Reducing maternal mortality remains a major global agenda item under the sustainable development goals (SDGs). The SDG goal 3.1 aims to achieve a maternal mortality ratio (MMR) of less than 70 per 100,000 live births by 2030.18,19 However, despite a significant reduction in global maternal mortality, it remains high in resource-limited countries in sub-Saharan Africa. In 2017, the pooled MMR for the sub-Saharan Africa region was 534 per 100,000 live births. 20 The government of Ethiopia introduced the Maternal Death Surveillance and Response System in May 2013 to increase maternal healthcare during pregnancy, childbirth, and the postpartum period. 21 However, the MMR remains high in Ethiopia despite several initiatives and efforts. According to the 2016 Ethiopia demographic health survey, the country reported a high MMR of 412 per 100,000 live births. 22 Similarly, a recent subnational study reported an MMR of 623 per 100,000 live births. 23
In Ethiopia, a systematic review and meta-analysis estimated the pooled prevalence of puerperal sepsis at 14.8%. 24 A study in Southwest Ethiopia reported a prevalence of 11.8%, 25 whereas another recent study found a prevalence of 20.6%. 26 Moreover, in Ethiopia, puerperal sepsis is the fourth leading cause of maternal death, accounting for 14.7% of pregnancy-related maternal deaths. 4 Factors that increase the risk of puerperal sepsis may vary regionally or sub-regionally due to contextual differences. Risk factors that may increase the incidence of puerperal sepsis are not well understood in Southwest Ethiopia. More context-specific information is needed for targeted prevention interventions. Therefore, to contribute to the national ambition to accelerate maternal mortality reduction, the present study aimed to identify the determinants of puerperal sepsis among postpartum women at public hospitals in the Dawro Zone, southwestern Ethiopia.
Materials and methods
Study setting and period
The study was conducted in the Dawro Zone, Southwest Ethiopian Peoples Region of Ethiopia, from February 1 to April 30, 2023. The Dawro Zone is situated 554 km from Addis Ababa, the capital city of Ethiopia. The zone has 11 districts and 2 town administrations. According to the Ethiopia Central Statistics Agency population projections for Ethiopia: 2007–2037 report, 27 the projected total population of the zone in 2023 is 700,073, of which 344,436 (49.2%) are female. According to the 2022 Zonal Health Department report (unpublished), the potential health coverage of the zone was 87%, with 1 general hospital, 2 primary hospitals, 22 health centers, and 177 health posts. The three hospitals (Tercha General Hospital, Tocha Primary Hospital, and Gessa Primary Hospital) serve over 1.3 million people in the catchment area. The Tercha General Hospital, located in Tercha Town, the capital of the zone, is equipped with 141 beds, including 58 in the maternity ward and 24 in the labor and delivery wards. In 2023, the hospital managed 3154 inpatients, 37,200 outpatients, 10,988 emergency cases, and 1743 deliveries. The Tocha Primary Hospital, with 36 beds (15 in maternity and 9 in labor and delivery), provided services for 557 inpatients, 23,820 outpatients, 5219 emergency cases, and 793 deliveries in 2023. Gessa Primary Hospital, with 28 beds (8 in the maternity ward and 5 in labor and delivery), treated 1552 inpatients, 22,988 outpatients, 7982 emergency cases, and 877 deliveries in 2023.
Study design
A facility-based, unmatched case–control study design was employed among postpartum women attending public hospitals in Southwest Ethiopia. The reporting of this study follows the criteria described in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 28
Study participants and eligibility criteria
All postpartum women who received services in public hospitals in the Dawro Zone composed the source population. All postpartum women who received services during the study period (between February 1 and April 30, 2023) in public hospitals in the zone composed the study population. This study included postpartum women who had puerperal sepsis or who were confirmed to be free from sepsis as study subjects. The study excluded women with obstetric fistulas, serious illnesses, unable to communicate, or mental health problems in both the cases and controls groups. Serious illnesses are conditions that require intensive medical care, like acute renal, liver or respiratory failure, septic shock, diabetic patients with ketosis, terminal diseases (e.g., advanced cancer), or conditions that require mechanical ventilation.
Cases
Postpartum women who came to hospitals during the study period to receive postpartum care and were diagnosed with puerperal sepsis.
Control
Postpartum women who came to the same hospital where cases were seen during the study period to receive postpartum care and were confirmed to be free from puerperal sepsis.
Sample size determination and sampling technique
The sample size for the study was determined via a double population proportion formula via OpenEpi version 3.01 software (Online, available at: http://www.openepi.com). The following assumptions were considered: a 95% confidence level, 80% power, a case-to-control ratio of 1:3, and a 10% contingency for nonresponse. Factors associated with puerperal sepsis in an institution-based, unmatched case–control study conducted in central Ethiopia were taken into account when determining the sample size. 29 The largest sample (n = 260, number of cases = 65, number of controls = 195) was taken as the final sample for the present study, as shown in Table 1.
Sample size determination via the OpenEpi software program.

AOR: adjusted odds ratio.
All the three public hospitals in the Dawro Zone—Tercha General Hospital, Tocha Primary Hospital, and Gessa Primary Hospital—were included in this study. Then, on the basis of the number of cases of puerperal sepsis that occurred in the 3 months of February, March, and April of the previous year in 2022, the required sample was allocated proportionally to each hospital. Finally, cases were selected consecutively (one after the other), and three controls per case were chosen immediately using systematic sampling technique. For cases at Tercha General Hospital and Gessa Primary Hospital, controls were consecutively selected at intervals of five (k = 5), whereas at Tocha Primary Hospital, controls were selected at intervals of three (k = 3), based on the patient load at each hospital (Figure 1).

Schematic representation of the sampling procedure used to select cases and controls among postpartum women in public hospitals in the Dawro Zone, southwestern Ethiopia, 2023.
Data collection procedure and quality assurance
Data were collected via a pretested, interviewer-administered questionnaire and data abstraction format to review medical records. The questionnaire was adopted from previous similar studies and was adapted to the local context.21,29 –31 The questionnaire consisted of three main parts: sociodemographic, obstetric, and comorbid characteristics. The questionnaire was initially developed in English and then translated to Amharic and returned to English to ensure consistency. The interviews were conducted with the study participants prior to their exit from the hospital following outpatient treatment or with hospitalized patients after they stabilized and were about to be discharged to their home. The data collectors used patient card numbers to avoid multiple entries of a single study participant into the study during the first 42 days post-pregnancy. Six diploma midwife nurses who were proficient in Dawrotsuwa and Amharic were employed as data collectors, whereas three midwives with bachelor’s degrees were designated supervisors. Pretesting was conducted at Amaya Primary Hospital with a 5% sample size to make necessary modifications to the questionnaire and data abstraction format prior to the actual data collection. One-day training was given to the data collectors and supervisors about the tools, data collection procedures, ethical issues and objectives of the study. The data collection process was closely supervised on a daily basis to solve problems and ensure data quality.
Variables
The dependent variable was puerperal sepsis (yes, if the patient was diagnosed with puerperal sepsis and coded as “1”; no, if the patient was free from puerperal sepsis and coded as “0”). Independent variables include sociodemographic characteristics (place of residence, maternal age, marital status, maternal educational level, maternal occupation, husband occupation, husband education, monthly income, and living arrangement); obstetric factors (parity, mode of delivery, time of rupture of membrane, duration of labor, status of vaginal examination, type of current pregnancy, type of labor, attendant of delivery, measurement to maintain hygienic practice, status of antenatal care (ANC) visit, referral status, and place of delivery); and comorbid factors (human immunodeficiency virus (HIV) sero-status, hypertension, and diabetic mellitus).
Definitions of terms
Puerperal sepsis is an infection of the genital tract occurring at any time between the onset of rupture of membranes or labor and the 42nd day postpartum, in which two or more of the following are present: pelvic pain, fever (axillary temperature of 38°C or higher on any given occasion), abnormal vaginal discharge (pus), abnormal smell or foul odor discharge, or delay in uterine involution (less than 2 cm/day) during the first 8 days. 1
Prolonged rupture of membrane
Multiple vaginal examinations
A woman has undergone five or more vaginal examinations. 33
Referral status
The study categorized the study participants as “formally referred” or “yes” if women were referred by qualified health personnel from other hospitals or health facilities, such as hospitals, health centers, or private clinics, and “self-referred” or “no” if they came directly from home, bypassing referring facilities. 29
Statistical analysis
Tablet-based Kobo Toolbox Version v2022.4.4 (KoBo Inc., Cambridge, MA) was used to collect the data. The data were subsequently downloaded as an Excel file and exported to STATA Version 17 (StataCorp, College Station, TX, USA) for analysis. Descriptive statistics—means with standard deviations for normally distributed continuous variables, medians with interquartile ranges (IQRs) for noncontinuous variables, and frequencies and percentages for categorical variables—were calculated. To investigate the predictors of puerperal sepsis, a binary logistic regression model was fitted to the dataset. Variables with a p value <0.25 in the bivariable analysis were included in the multivariable analysis to control for potential confounding factors. The Hosmer–Lemeshow goodness-of-fit test was used to test model fitness, and the test result was a p value of 0.3533, indicating good model fitness. Multicollinearity was checked via variance inflation factors (VIFs), and the maximum variance VIF score was 1.42. The adjusted odds ratio with a 95% confidence interval was used to assess the presence and strength of associations. A p value <0.05 was used to declare an independent association in the multivariable analysis.
Results
Sociodemographic characteristics of the study participants
A total of 260 postpartum women participated in the study—65 cases and 195 controls—for a 100% response rate. The median (IQR) age of the participants was 25.0 (22.0–29.0) years, with (24 (20–26) for cases and 26 (22–30)) for controls. The majority, 217 (83.5%), of the study participants were married. Two-thirds (41 (63.1%) of the cases, and 74 (37.9%) of the controls were rural residents. Eight (12.3%) of the women from the cases and 66 (33.8%) of the controls had attended college or above. Nearly half, 30 (46.2%) of the cases and one-third, 66 (33.8) of the controls were housewives. The majority, 206 (79.2%), of the study participants were living with their husbands, whereas the remaining 54 (20.8%) were living without their husbands (Table 2).
Sociodemographic characteristics of determinants of puerperal sepsis among postpartum women at public hospitals in the Dawro Zone, Southwest Ethiopia, 2023 (n = 260).

IQR: interquartile range.
Obstetric characteristics of postpartum women
Nearly half of the cases, 28 (43.1%), and the majority of the controls, 118 (60.5%), delivered their last child vaginally. Nearly half of the cases, 28 (43.1%), and one-fifth, 42 (21.5%) of the controls gave birth via cesarean section. Over half of the cases, 37 (56.9%), and approximately one-fifth of the controls, 41 (21.0%), had delivered by laboring for more than 12 or more hours. Over half, 36 (55.40%) of the cases and approximately one-fourth, 55 (28.20%) of the controls had been referred from other institutions. The detailed obstetric characteristics are presented in Table 3.
Obstetrics characteristics of determinants of puerperal sepsis among postpartum women at public hospitals in the Dawro Zone, southwestern Ethiopia, 2023 (n = 260).

ANC: antenatal care.
Comorbid characteristics of the study participants
Six (9.20%) cases and two (1.20%) controls were positive for HIV. Five (7.7%) patients were known hypertensive patients, whereas two (1%) of the controls were diagnosed with hypertension. Similarly, four patients and one control patient had diabetes (Table 4).
Chronic diseases among postpartum women at public hospitals in the Dawro Zone, southwestern Ethiopia, 2023 (n = 260).
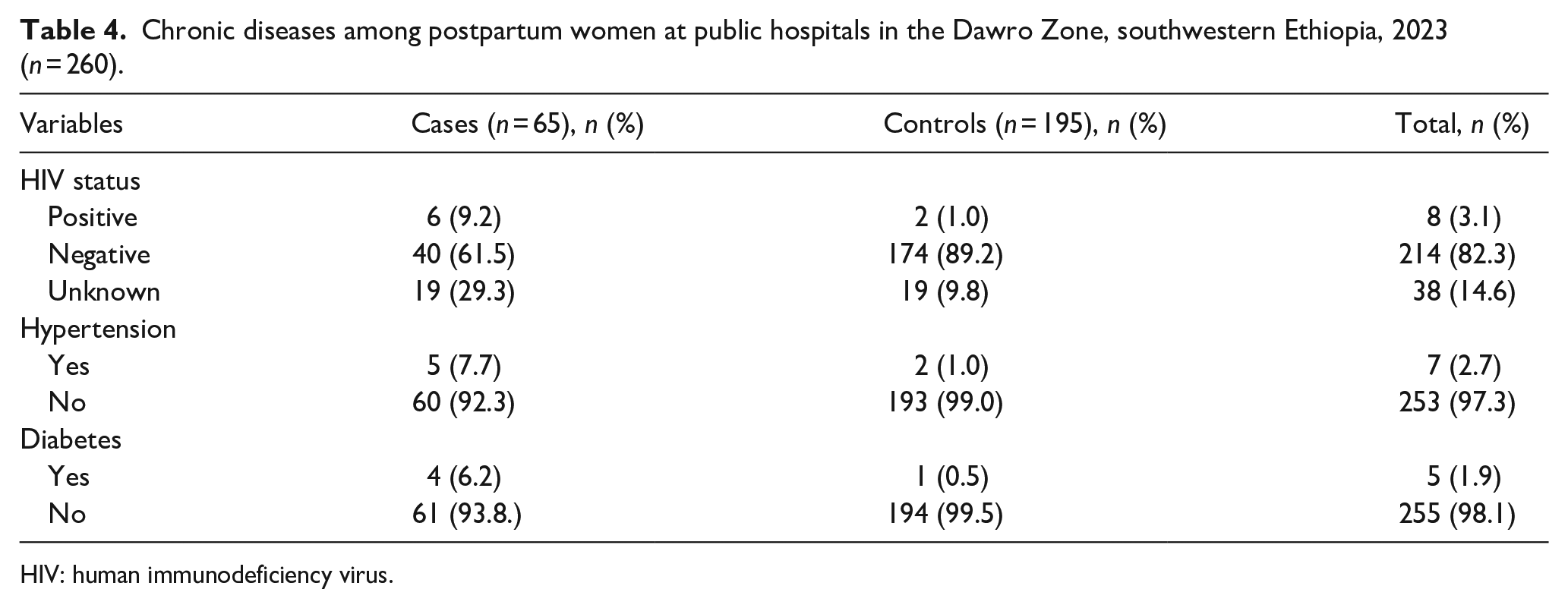
HIV: human immunodeficiency virus.
Factors associated with puerperal sepsis among postpartum women
In the bivariable logistic regression analysis, sociodemographic factors such as living in rural areas and having no formal education or occupation were associated with puerperal sepsis. Obstetric-related factors such as a lack of ANC, prolonged rupture of the membrane, home delivery, multiple vaginal examinations, cesarean section delivery, and referral status were significantly associated. However, after adjustment for possible confounding variables in the multivariable analysis, rural residence, no formal education, prolonged membrane rupture, home delivery, multiple vaginal examinations, and cesarean section delivery were found to be independent predictors of puerperal sepsis.
Compared with urban women, women who live in rural areas are approximately four times more likely to develop puerperal sepsis. Mothers with no formal education had 4.4 times greater odds of having puerperal sepsis than those with a college education or above. The odds of infection increased by 14-fold in women with no ANC follow-up compared with those with three or more ANC visits. Mothers with prolonged rupture of the membrane for more than 24 h were 9.5 times more likely to develop puerperal sepsis. Mothers who delivered at home are more likely to develop puerperal sepsis than are those who delivered at health facilities. Compared with those with fewer than five examinations, women with five or more vaginal examinations were 7.44 times more likely to develop puerperal sepsis. Mothers who gave birth via cesarean section had approximately three times greater odds of developing puerperal sepsis than those who gave birth via spontaneous vaginal delivery (Table 5).
Bivariate and multivariate analyses of determinants of puerperal sepsis among postpartum women at public hospitals in the Dawro Zone, Southwest Ethiopia, 2023 (n = 260).

AOR: adjusted odds ratio; COR: crude odds ratio; CI: confidence interval; ANC: antenatal care.
Discussion
This unmatched case–control study aimed to identify determinants of puerperal sepsis among postpartum women at public hospitals in southwestern Ethiopia. The study identified a number of factors, such as rural residency, lack of formal education, lack of ANC follow-up, prolonged rupture of membranes, home delivery, frequent vaginal examinations, and cesarean section delivery, as risk factors for puerperal sepsis.
This study revealed that women living in rural areas were more likely to develop puerperal sepsis compared to those living in urban areas. This finding was consistent with previous studies in different parts of Ethiopia29,34 –36 and studies from Uganda. 31 This association might be due to limited health service access for ANC follow-up and institutional delivery care in rural areas.37 –39 Moreover, maternal undernourishment 40 and poor sanitation conditions because of a lack of water access could contribute to this high risk of puerperal sepsis in rural areas. 22 The findings of the present study underscore the need for targeted interventions that enhance maternal healthcare services in rural settings.
The mothers who did not attend formal education more likely to have puerperal sepsis than among those who did attend college and above. This finding was consistent with reports in previous studies.29,41,42 The reasons for this association might be poor personal hygiene, low ANC and postnatal care uptake, and poor awareness of early medical care seeking compared with educated mothers. A study conducted in Tanzania revealed that adequate knowledge and self-care practices aimed at preventing puerperal sepsis were associated with better educational status. 43 Thus, mothers without formal education should receive special attention to improve their knowledge and skills in preventing puerperal sepsis.
The odds of developing puerperal sepsis were 14.04 times greater among non-ANC followers than among those who received three or more ANC visits. This evidence was comparable with the findings of studies conducted in Mekelle city public hospitals, Tigray, Ethiopia, 34 the Shoa zone Oromia region, Ethiopia, 29 and Uganda. 44 In contrast, another study revealed that ANC follow-up was negatively associated with postpartum sepsis. 45 The possible reason could be that puerperal sepsis was more common among women who did not receive ANC, which can be attributed to several factors, such as women who missed ANC may lack access to comprehensive fetal and maternal health screening for infections prevention, counseling on hygienic practices, nutrition, and those women without ANC may have home deliveries without proper hygienic conditions that may lead them to develop sepsis.
Our study demonstrated that mothers with prolonged rupture of the membrane more likely developing infection than those with a duration of less than 24 h. This finding was supported by evidence documented elsewhere.24,29,34 The possible explanation could be that when the membranes rupture, the amniotic sac no longer provides a sterile environment for the fetus, which may allow bacteria from the external environment or vagina to travel upwards into the uterus. The longer the rupture remains, the greater the risk of bacteria entering and causing infection, which may be strongly associated with chorioamnionitis. In addition, the defense may be lost, and pathogens can more easily reach the uterus, leading to infections in the amniotic fluid, placenta, and uterine lining.
The odds of developing puerperal sepsis were 3.06 higher for home delivery than for health facility delivery. This study finding was consistent with the evidence documented elsewhere.45,46 The probable reason could be that health facilities are mostly equipped with clean and sterile equipment for delivery and assigned trained health professionals to conduct delivery. However, home delivery is conducted in an unhygienic environment by an untrained person, who may contaminate the vagina, that may lead to infection.
A study found that frequent vaginal examination of five or more increased the risk of puerperal sepsis by more than seven folds compared to their counterpart. This result was consistent with the studies in Uganda, 47 Ethiopia,24,34 –36,48 and South Asia. 49 This could be the risk of inoculating bacteria from outside environment and vagina to the internal sterile part of the reproductive organs.
The odds of developing puerperal sepsis among women who gave birth via a cesarean section were approximately three times greater than among those who gave birth via spontaneous vaginal delivery. This finding was in line with studies conducted in California, 50 Scotteland, 51 Uganda, 47 and Ethiopia.24,29,30,34 –36 The possible reason might be that those women delivered by cesarean sections have the chance to stay in the hospital and have a tendency to acquire wound site infection, poor infection prevention technique utilization, and poor hygiene and sanitation practices. In contrast, a study at the University of Gondar Referral Hospital in Ethiopia reported that compared with spontaneous vaginal delivery, cesarean section delivery reduced the risk of sepsis development by 62%. 13 The discrepancy may be due to differences in the setting, skill of the surgical team, and the postoperative care. In the tertiary specialized referral hospital settings in Ethiopia like Gonder Referral Hospital, cesarean sections are more commonly performed by experienced physicians, which may reduce the risk of complications, including infection, due to better surgical techniques and aseptic protocols. Moreover, postoperative care such as the use of prophylactic antibiotics and proper wound care would have been better in the tertiary specialized referral hospitals compared to general and primary hospitals.
Limitations of the study
The study had a number of limitations: (1) there may be a possible recall bias since patients could forget their prior medical conditions that lead to puerperal sepsis; (2) the study may be susceptible to social desirability bias, as women prefer to report socially acceptable responses; for example, they may report less per vaginal examination because of the sensitivity of the issue. To minimize such biases, the study team used female midwifery data collectors, and interviews were conducted in a private setting. (3) Since this study was conducted in public hospitals, it may not be generalizable to health centers, private clinics and hospitals, or mothers treated at the community level with traditional medicines.
Conclusions
The study identified rural residence, lack of formal education, lack of ANC follow-up, prolonged rupture of the membrane, home delivery, frequent vaginal examinations, and cesarean section delivery as predictors of puerperal sepsis among postpartum women. Therefore, scaling up appropriate health education packages on risk factors for puerperal sepsis during ANC, labor, and postdelivery is highly encouraged. In addition, we recommend timely screening of risks for pregnant women, which can lead lately to cesarean sections and avoid unnecessary vaginal examinations during the intrapartum period. Further qualitative evidence is required to understand the dynamics of identified risk factors from both patient and health worker perspectives.
Footnotes
Acknowledgements
The authors would like to acknowledge Hawassa University, College of Medicine and Health Sciences, School of Graduate Studies, for their technical support. The authors would like to forward their sincere gratitude to the Dawro Zone Health Department, administrators of the included hospitals, for their permission to conduct this study in their health institutions. Finally, they thank all the study participants, data collectors, and supervisors.
Ethical considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) of the College of Medicine and Health Sciences at Hawassa University prior to data collection, with approval reference number IRB/248/15, dated March 16, 2023. An official support letter was written by the School of Public Health at Hawassa University to the Dawro Zone Health Department and participating hospitals.
Consent to participate
Before data collection began, hospital administrators granted permission, and participants provided written informed consent after the objective of the study was clearly described. For illiterate participants who could not provide a written signature, we obtained a fingerprint after reading the information sheet to them. In addition, written consent was obtained from the parents or guardian of postpartum women younger than 18 years old. Data from each patient were collected once the patient had stabilized and received the necessary treatment from the hospital. Each patient was informed that their participation was voluntary and that they had the right not to participate or withdraw at any time without compromising their hospital care services. To ensure the confidentiality of the study participants, the study staff kept all personal and other medical information in compliance with good clinical practice. All the data and information were not shared with the third body, which was not part of the study personnel. All data with the study participants’ names were kept on a computer with passwords.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from corresponding author on reasonable request.