
Abstract
Background:
Sexual and gender-based violence (SGBV) is a human rights and social justice issue that impacts individuals worldwide, particularly university students. The literature demonstrates that culturally and contextually tailored programs to reduce and ultimately prevent SGBV for university students have received little priority in sub-Saharan African countries.
Objectives:
This pilot study assessed the feasibility, acceptability, and safety of the peer-delivered Relationship Tidbits intervention for use with health science students in Ghana.
Design:
We conducted a pilot feasibility test to determine if this approach and content were feasible for this setting and these students.
Methods:
Health science students enrolled at a central university in Ghana were recruited in July 2019 for participation in a peer-delivered primary prevention intervention, Relationship Tidbits. All participants completed pre- and post-test surveys focused on acceptability, safety, gender equality, and rape myth acceptance.
Results:
Health science student participants (n = 137) had a significant history of physical abuse, sexual abuse, and emotional abuse. Overall, this pilot study demonstrated that the Relationship Tidbits intervention is feasible, acceptable, and safe for use with health science students in Ghana during their university education. While this study was not powered to focus on outcomes, there were indications that this short, one-time intervention may result in at least short-term attitudinal changes related to gender equality and rape myth acceptance.
Conclusions:
The findings of this study highlight the importance of implementing comprehensive, culturally appropriate SGBV prevention efforts in Ghanaian university settings.
Keywords
Introduction
Sexual and gender-based violence (SGBV) is a public health problem that reverberates around the globe and consists of any form of violence against an individual based on biological sex, gender identity or expression, or social expectation for men or women. 1 SGBV encompasses several types of violence including sexual, physical, psychological, and socioeconomic. 1 A common form of SGBV experienced by women is intimate partner violence (IPV), which refers to any behavior by an intimate partner or ex-partner that causes physical, sexual, or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviors. 2 Although individuals of all gender identities may experience SGBV, women and girls face a disproportionate risk of SGBV due to the imbalance of power deeply rooted in social and cultural structures. 3
A meta-analysis demonstrated that sub-Saharan Africa has a high prevalence of IPV, when compared to global data. 4 Further analyses of recent data indicate that two out of five women in the region will experience IPV. 5 The prevalence of SGBV in university settings is particularly concerning. A systematic review of female youth enrolled in educational institutions in sub-Saharan Africa found that the overall prevalence of SGBV ranged from 42.3% to 67.7%. 6 School and university settings are an important intervention point because of the impacts of SGBV on physical health, mental health, sexual health, social engagement, and academic outcomes.7 –9 As noted by the World Health Organization, 10 schools are responsible for ensuring the safety of students and have the ability to actively engage their community members in issues related to SGBV.
Ghanaian social norms
According to a 2019 global report on discrimination against women focused on social institutions and gender index (i.e., formal and informal laws, social norms, and practices), Ghana scores as highly discriminatory. 11 Statistics indicate that 24% of Ghanaian women have experienced physical and/or sexual IPV in their lifetime. 12 Meanwhile, IPV is widely socially accepted, with nearly one-third of men across sub-Saharan Africa agreeing to at least one reason to beat their wives. 13 There is also widespread endorsement of rape myths among university students.14,15
These social norms demonstrate why there is a culture of violence on Ghanaian university campuses. 16 These social and cultural factors in Ghana lead to a high prevalence of SGBV on university campuses across the country.17,18 A study on sexual violence in public medical schools in Ghana revealed that 23.5% of females were harassed by their peers and a further 76.5% were harassed by a combination of lecturers, supervisors, or instructors. 19 Another study at a Ghanaian university found that 27.8% of men and 37.1% of women reported being insulted by a partner. 20 In order to address SGBV across the country, in 2005 the government established the Domestic Violence Victims Services Unit (DOVVSU), a division within the police force to prosecute offenders and protect victims. While this is a promising step toward reducing SGBV, this unit currently lacks sufficient resources to effectively investigate, has little reach into university campuses, and has not been able to change the social norms that deter individuals from reporting to the police for resources and support. 20
Data from sub-Saharan Africa 21 and Ghana specifically22,23 find that most individuals who experience IPV seek help from informal sources (e.g., friends, family). However, recent data on formal help-seeking have demonstrated that individuals who experience IPV may also seek formal support from healthcare providers and law enforcement. 24 For this reason, all healthcare providers, including emerging healthcare professionals such as nurses and physicians, may provide informal and/or formal help-seeking support to their family, friends, or patients and therefore need to have an opportunity to learn more about SGBV during their training to help promote prevention, identification, and distribution of resources.
SGBV prevention in sub-Saharan Africa
SGBV prevention and public health approaches focus on three levels of intervention: (1) preventing the occurrence (primary), (2) immediate responses predominantly provided by healthcare providers, social service providers, and law enforcement (secondary), and (3) long-term responses and rehabilitation (tertiary). 25 A review of interventions to reduce SGBV in sub-Saharan Africa by Keith et al. 26 found that the key elements of successful interventions incorporate engaging the community including male partners, participatory learning, utilizing existing platforms, and longer durations with reinforcement. However, the evidence-base for SGBV interventions among university students in sub-Saharan Africa and low- and middle-income countries more broadly is lacking. 27 The majority of interventions introduced in university settings in low- and middle-income countries focus on primary prevention.27 –29 Primary prevention interventions hold great promise when initiated among a university-age population because they have the potential to disrupt knowledge and attitudes that may impact intentions around SGBV. It is therefore important to consider if pre-existing evidence-based interventions like Relationship Remix 30 have components that can be contextually and culturally adapted to new contexts.
Relationship Tidbits prevention program
A promising primary prevention intervention developed and used at the University of Michigan is Relationship Remix, an interactive in-person training delivered to first year students by peers with a focus on healthy relationships and consent using a value-based framework. 30 This primary prevention program was previously adapted to the University of Cape Coast in Ghana using a rigorous process guided by the ADAPT-ITT framework, 31 resulting in a culturally and contextually adapted version, called Relationship Tidbits. The ADAPT-ITT framework is a systematic approach used to adapt evidence-based interventions for new target populations or settings, ensuring cultural and contextual relevance. Specifically, the Relationship Tidbits intervention was created with partners in Ghana using focus groups with faculty/staff and students to better understand the needs for university students in Ghana. The team then agreed to adapt the pre-existing Relationship Remix intervention, and utilized beta testing after each adaptation to ensure the intervention was appropriate for the intended audience before manualizing it and training peer facilitators. 31
The adapted Relationship Tidbits program is a 2-h manualized intervention that uses a combination of interactive activities, including role-play and demonstration, to educate about 10 key concepts (creating a safe and welcoming space, thinking about values, decision-making using values, developing relationship skills, communication, gender equality, consent, making choices about sex, sexual harassment, and resources). Peer facilitators participate in a rigorous training to administer the program in pairs to their peers. 32 Relationship Tidbits has now been adapted university-wide for all incoming students at the University of Cape Coast. However, there has been no evaluation on the effectiveness of the program for specific groups of students, particularly health science students, who will provide primary and secondary prevention to survivors of SGBV.
The literature demonstrates that culturally and contextually tailored programs to reduce and ultimately prevent SGBV for university students have received little priority in sub-Saharan African countries, including Ghana. 33 Implementing a contextually adapted primary prevention program for Ghanaian university students can potentially transform the knowledge, attitudes, and ultimately the behaviors of future leaders in the country, who will be in a position to advocate for more widespread SGBV prevention programs. Furthermore, a primary prevention program for university-age individuals may also decrease current levels of SGBV on campus, as well as improve the mental, physical, and reproductive health of survivors.
Purpose
Thus, the purpose of this study is to pilot the Relationship Tidbits program with health science students at a large university in central Ghana. Specifically, we will address the following aims:
Pilot test the Relationship Tidbits program among residential health science students focusing on feasibility, acceptability, and safety of the intervention.
Compare pre- and post-intervention self-reported attitudes toward SGBV (gender equality, rape myth acceptance).
The study focuses on health science students, who will be future healthcare providers. By doing so, health science students will be better prepared to address SGBV on campus and in their future clinical settings.
Methods
Design
This pilot feasibility study used a pre- and post-test design to explore the feasibility, acceptability, and safety of an adapted intervention for health sciences students in central Ghana. The study was conducted with health science students (nursing, medicine, midwifery, and dentistry) enrolled at one large university who reside in hostels at the affiliated academic teaching hospital in July 2019, prior to the COVID-19 pandemic. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement (see Supplemental Appendix 1). 34
Participants
Recruitment for the Relationship Tidbits program was conducted during July 2019 using snowball sampling through university faculty and class leaders. The class leaders sent messages to the class WhatsApp group inviting students to participate in a study about healthy relationships. They also shared a digital version of the recruitment flyer. In addition, hard copies of flyers were distributed, and messages were sent from resident advisers to health science students at the university, providing details of the dates, times, and locations for the program sessions. The inclusion criteria for participation were: (1) being a health science student at the university, (2) aged 18 years or older, and (3) being able to speak and read English, which is the language of instruction at the university. There were no exclusion criteria.
A total of 144 students expressed interest in the Relationship Tidbits program, and a total of 137 individuals participated in the intervention. No participants left during the intervention. However, those individuals who did not complete the outcomes surveys on gender equality and rape myths (n = 2 in pre-test; n = 1 in post-test) or who had >50% of the survey missing were removed from data analysis. Therefore, a sample of 108 students was included for the attitudes toward SGBV analyses. For the pre-test, there were no individual variables with 5% or more missing values for either outcome scale, and the missing values were found to be missing completely at random using Little’s test. 35 For the post-test, there were no individual variables with 5% or more of missing values for either outcome scale. However, there was some case level missing data with a few participants missing the last few items of each scale.
Procedures
Study procedures did not begin until ethical approval was received from the University of Michigan Health Sciences and Behavioral Sciences institutional review board (HUM00164788) and the participating university ethical review committee. Study procedures were explained to all participants and then written comprehensive consent was obtained by the research facilitators before data collection. To reduce social desirability bias, all survey data were collected anonymously using paper-based self-administered surveys; pre-surveys were completed immediately before the intervention began, and post-surveys once the program was finished. In order to ensure open conversations, all participants were reminded to keep discussions during the intervention confidential.
All Relationship Tidbits program sessions were led by three Ghanaian facilitators from the University of Cape Coast who had previously been trained during the initial adaptation process 32 and co-led by a participating university student who had received 2 days of peer facilitator training. Fidelity of the Relationship Tidbits program was maintained by: (1) using a facilitator manual, (2) co-facilitation by trained facilitators who had previously delivered the intervention to university students, (3) monitoring by research staff, and (4) post-intervention data were only collected from those who participated in the entire program. 36 Due to the sensitive nature of the study topic, all participants were offered a resource list with information about university and community-based healthcare, social service and law enforcement support at the conclusion of the program.
Sessions were delivered in a conference room in one of the health sciences buildings on campus. Refreshments were provided by the study team, but no additional incentives were offered for participation. The program contains one video which requires a computer to project and two worksheets, but no additional resources are needed for delivery.
Variables
Demographic characteristics
Demographic characteristics of the participants were collected on the pre-test only and focused on age, gender, and year in school. In addition, the following personal and institutional characteristics were captured on the pre-test. Personal experiences of SGBV were measured using three items adapted from the World Health Organization 2 questions on SGBV to capture physical, sexual, and psychological abuse. Our adaptation of the WHO questions 2 focused on abuse from the age of 15 years old (as opposed to the standard lifetime or last 12 months). Four items related to consent sought to understand usual processes for giving and receiving consent including the usual provision of consent for sexual activity (verbal and non-verbal) and the usual process for seeking consent (verbal and non-verbal) with values ranging from “1 = All of the time” to “5 = Never.” Three investigator-derived items on institutional response to violence captured student views on institutional response measured on a Likert scale from “1 = Strongly Agree” to “5 = Strongly Disagree” including the: (1) institution has processes to address SGBV on campus; (2) institution takes complaints of sexual harassment seriously, and (3) institution responds to complaints of sexual harassment (see Supplemental Appendix 2).
Feasibility
Feasibility was assessed using the following two indicators: (1) the ability to voluntarily recruit students for participation (e.g., no incentives or requirement for attendance) and retain them for the intervention (measured as a percent of those that participated divided by those that expressed interest) and (2) the time taken to deliver all Relationship Tidbits trainings to the recruited students (measured in days).
Acceptability
Acceptability was measured in the post-test with an investigator-derived acceptability scale (see Supplemental Appendix 3). The scale consists of five items and was measured on a Likert scale from “1 = Strongly Disagree” to “5 = Strongly Agree.” Sample items measured concepts such as the intervention being easy to understand, enjoying the intervention, the intervention was too long, the participant will continue to use the information learned, and the participant will recommend the program to a friend. The internal consistency of the acceptability scale was α = 0.65 in this study, with the item on the length of the survey contributing to the low reliability.
Safety
Safety was measured in the post-test with an investigator-derived five-item scale (see Supplemental Appendix 3). The scale was rated on a 5-point Likert scale ranging from “1 = Strongly Disagree” to “5 = Strongly Agree.” Higher scores indicate greater safety provided by the intervention. Items included concepts such as feeling safe participating, the intervention provided information to keep participants safe, the intervention could improve safety, and feelings of safety at the participating university (see Supplemental Appendix 3). The internal consistency of the safety items was α = 0.83 in this study, indicating good reliability.
Preliminary outcomes
Finally, trends in outcomes were measured including attitudes toward SGBV in the pre- and post-intervention survey to explore the intervention’s potential effect on gender equality and rape myth acceptance.
Gender equality
Gender equality was measured using the Gender Equitable Men (GEM) scale. 37 The GEM scale is a 24-item scale measured on a scale with “1 = Strongly Agree,” “2 = Somewhat Agree,” and “3 = Do Not Agree.” Overall scores range from 24 to 72, with a higher number indicating more gender-equitable norms. The GEM scale has four subscales: (1) Sexual Relationships (e.g., “It is the man who decides what type of sex to have”); (2) Violence (e.g., “There are times when a woman deserves to be beaten”); (3) Reproductive Health and Disease Prevention (e.g., “Women who carry condoms on them are easy”); and (4) Domestic Chores (e.g., “A man should have the final word about decisions in his home”). Estimates of internal consistency for the GEM scale have varied in different countries and contexts ranging from a Cronbach alpha of α = 0.75 to α = 0.88.37,38 In the current study, internal consistency was α = 0.79 in the pre-test and α = 0.72 in the post-test.
Rape myth acceptance
Rape myth acceptance was measured with 21 items from the Modified Illinois Rape Myth Acceptance Scale (Modified IRMA). 39 Individuals responded to the items using a 5-point Likert scale ranging from “1 = Strongly Agree” to “5 = Strongly Disagree.” Overall scores range from 21 to 105, with higher scores indicating a greater rejection of rape myths. The scale is divided in four subscales that organize subtle rape myths that blame the victim or excuse the perpetrator: (1) She asked for it (e.g., “If a girl goes to a room alone with a guy at a party, it is her own fault if she is raped”); (2) It was not really rape (e.g., “If a girl doesn’t physically fight back, you can’t really say it was rape”); (3) He did not mean to (e.g., “If a guy is drunk, he might rape someone unintentionally”); and (4) She lied (e.g., “A lot of times, girls who claim they were raped just have emotional problems”). The modified IRMA scale demonstrated an internal consistency of α = 0.87 as measured by Cronbach alpha. 39 In this study, the modified IRMA internal consistency was α = 0.91 for the pre-test and α = 0.86 for the post-test. A combination of items from the GEM and modified IRMA scales have previously been validated with Ghanaian students. 31
Statistical analyses
The survey data were analyzed using IBM SPSS Statistics (Version 27); significance was set at p < 0.05. Descriptive statistics were assessed first for demographic characteristics, acceptability, and safety. Missing data were examined for the attitudes toward SGBV scales (GEM and modified IRMA). As a result of the missing data analysis, multiple imputation with mean values was deemed appropriate to replace missing data for the remaining sample on the pre- and post-test. 40 As all data were anonymous, individual pre- and post-test scores could not be matched. Therefore, independent t-tests were used to compare the aggregate group pre- and post-test mean scores on gender equality (GEM) and rape myth acceptance (modified IRMA).
Results
Demographic characteristics
In total, 137 health science students participated in the Relationship Tidbits intervention. However, only 108 completed ⩾50% of the post-test. The health science students were predominantly female (64.0%) and had a mean age of 22.85 years (SD = 1.88 years; range 20–30 years). In total, 19% of participants had experienced physical abuse, 10.4% had experienced sexual abuse, and 58.6% had experienced emotional abuse. When asked about verbal consent for sexual activity, 30.0% reported never seeking verbal consent and 30.0% reported never giving verbal consent for sexual activity. Regarding institutional responses to violence, the majority of students were neutral (29%) on their awareness of processes to address SGBV on campus with an average of M = 3.29 (SD = 1.30). A total of 54% were neutral regarding their knowledge about the university taking complaints of sexual harassment seriously, M = 3.00 (SD = 0.99). Finally, 55.5% were neutral on their belief that the university responds fairly to complaints of sexual harassment, M = 3.11 (SD = 0.92). See Table 1 for additional demographic characteristics.
Participant demographics (n = 137).

Feasibility
The pilot study was designed to assess the feasibility, acceptability, and safety of the peer-delivered Relationship Tidbits intervention for health science students. Regarding feasibility, the study team was able to successfully recruit 144 health science students for the intervention program in a span of 2 with no incentives or mandatory requirements provided to the participants. Furthermore, it took four sessions to deliver the intervention to 137 of the 144 students, resulting in 95.1% retention of recruited students participating in the intervention.
Acceptability
The health science student participants also provided high ratings of acceptability, with 95.4% (M = 4.60, SD = 0.65) of participants indicating they agreed or strongly agreed that they would continue using the information gained from the Relationship Tidbits intervention. Additionally, 95.4% (M = 4.61, SD = 0.65) of participants indicated they agreed or strongly agreed that they would recommend the program to a friend. Interestingly, 57.8% of participants either agreed or strongly agreed that the intervention was too long (M = 3.62, SD = 1.08).
Safety
The safety of the intervention also received high ratings with 89% (M = 4.53, SD = 0.74) of participants indicating they agreed or strongly agreed that they felt safe during the intervention. The majority of participants (87.2%; M = 4.28; SD = 0.80) indicated they agreed or strongly agreed that the intervention could improve safety on campus. See Table 2 for additional details about acceptability and safety.
Acceptability and safety of the Relationship Tidbits intervention (n = 109).

SD: standard deviation.
Missing one respondent.
Preliminary outcomes
Finally, a preliminary analysis of pre- and post-test outcomes focused on gender equality (GEM) and rape myth acceptance (modified IRMA) revealed that there were significant short-term changes in this pilot study. The pre–post GEM and IRMA scores are presented in Table 3. Health science students demonstrated significant improvements in endorsement of gender equality as measured by the GEM scale between the pre- (M = 66.07; SD = 4.47) and post-intervention (M = 67.92, SD = 4.16; t(112) = 3.534, p < 0.001). Although not all subscales changed, a significant improvement was noted in the “Sexual Relationship Domain,” the “Reproductive Health and Disease Prevention Domain,” and the “Domestic Chores Domain.”
Pre- and post-intervention modified IRMA and GEM scores.
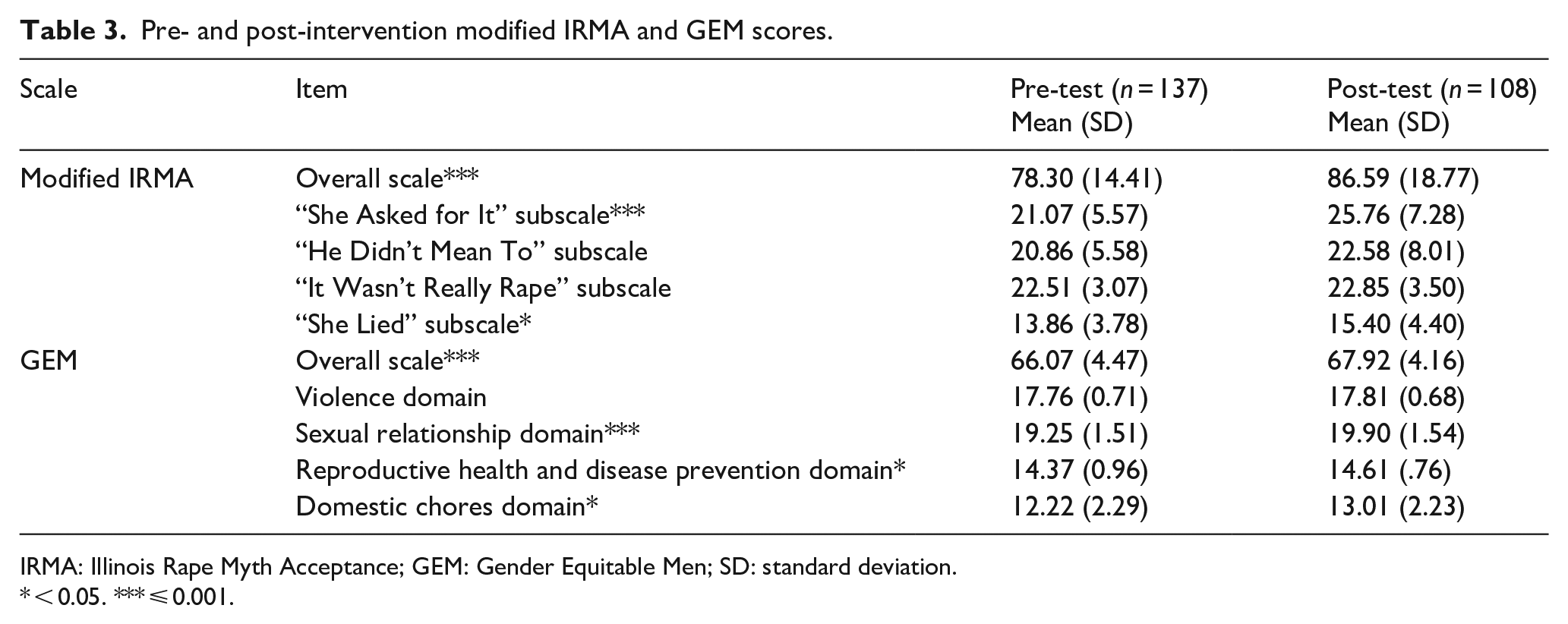
IRMA: Illinois Rape Myth Acceptance; GEM: Gender Equitable Men; SD: standard deviation.
< 0.05. *** ⩽ 0.001.
Health science students also had significantly improved scores (a higher score is associated with less rape myth acceptance) in the modified IRMA with a pre-test M = 78.3 (SD = 14.41) versus the post-test M = 86.59 (SD = 18.77; t(112) = 3.887, p < 0.001). The “She asked for it” and “She lied” subscales also showed a significant improvement among the health science students.
Discussion
This study aimed to conduct a pilot feasibility test of an SGBV primary prevention intervention for health science students that was previously adapted to the Ghanaian context. Our participants reported high rates of emotional abuse, which is in line with other studies that have noted high rates of psychological or emotional violence in Ghana and among university students in sub-Saharan Africa.5,6,41 A study among nine universities in sub-Saharan Africa found that students were experiencing emotional and psychological violence at high rates (64% of a sample of 3512 students). 41 The high prevalence of psychological violence in these studies highlights the vital role of university-based SGBV prevention that is culturally and contextually tailored to the region and context.
One focus of this study was to assess the feasibility, acceptability, and safety of the peer-delivered Relationship Tidbits intervention for health science students. Overall, this pilot study demonstrated that the Relationship Tidbits intervention is feasible, acceptable, and safe for use with health science students in Ghana during their university education. The study found that the components and activities of Relationship Tidbits were implemented satisfactorily in 4 days for 137 health science students who willingly volunteered to participate. This suggests that the program is a practical and effective means of primary prevention for Ghanaian university students. 42
Participants expressed a desire to share the program with their friends and confirmed that they would continue using the information gained from the intervention. This indicates that the intervention is relevant for the students and can be useful in their future, both important aspects related to the acceptability of the intervention. 42 Despite the general appreciation for the intervention, more than half of the participants felt that the intervention was too long. In the future, the program could be modified to reduce its overall length by either decreasing the content or splitting it into smaller parts. Administering the intervention in smaller parts over time could also help promote reinforcement. This is especially important considering that the original intervention from which Relationship Tidbits was adapted only lasted 1.5 h. 30 Participants in the intervention felt safe throughout the program and believed that the program could enhance safety on campus. This outcome is crucial when it comes to interventions related to SGBV. Earlier guidelines for prevention of SGBV on university campuses have emphasized the importance of creating a safe space for students to learn about SGBV prevention efforts. 25
Data also suggest the potential of the Relationship Tidbits intervention in improving attitudes toward SGBV. At baseline, participants demonstrated relatively low levels of gender equality and high levels of rape myth acceptance. The findings from this pilot study point to a shift toward more gender equitable views, and a decreased acceptance of rape myths. Although this study was not powered to focus on outcomes, there were indications that this relatively short, one-time intervention may result in at least short-term attitudinal changes related to gender equality and rape myth acceptance. This attitudinal change is promising as an initial step for SGBV prevention in university settings in Ghana and, potentially, sub-Saharan Africa. Next steps should look at the mid-term and long-term outcomes of this intervention regarding attitudinal change, and if this change is related to a significant change in behavior, and consequently a reduction of SGBV in the university setting. It is worth noting that single-session prevention programs, such as Relationship Tidbits, will only be able to significantly decrease the prevalence of SGBV if they are implemented as part of a comprehensive, multilevel strategy that is tailored to the campus needs. 25
Finally, health science students will become nurses, midwives, physicians, and dentists. These professions often have the first level of contact with individuals who experience SGBV, and increased awareness within these professionals may have an impact on their future practice and response to SGBV. Coupled with the knowledge that overall healthcare providers in sub-Saharan Africa lack knowledge and training to assist patients experiencing SGBV,43,44 this pilot study supports the need to educate healthcare providers before they enter independent clinical care. Once healthcare providers enter independent clinical care, they may lack the time or ability to seek out continuing education and skills training to help them more effectively respond to patients who have experienced SGBV.45,46
Strengths and limitations
The strength of this study includes providing important preliminary evidence about the feasibility, acceptability, and safety of an intervention targeting future healthcare providers who have the potential to experience SGBV as well as be responsible for delivering care to survivors of SGBV. However, there are limitations to this pilot study worth acknowledging. First, it is limited in both geographic and population focus to nursing, midwifery, medical, and dentistry students in central Ghana limiting the generalizability to other regions of Ghana and sub-Saharan Africa, as well as to other health science professions. As this was a pilot feasibility study, we were underpowered to detect significant changes in the outcomes of gender equality and rape myth acceptance. Other limitations are: (1) pre- and post-tests were not matched precluding our ability to determine if different groups of students experienced the program differently, (2) missing data, and (3) a smaller number of participants who completed the post-test.
Conclusion
This pilot feasibility study of a culturally adapted SGBV primary prevention intervention for university students demonstrated feasibility, acceptability, and safety for health science students. Although attitudinal shifts were observed, further research is needed to evaluate long-term behavioral changes. This intervention could be adopted as part of a comprehensive response to SGBV at the university level in Ghana, and possibly other universities in sub-Saharan Africa.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251353328 – Supplemental material for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study
Supplemental material, sj-docx-1-whe-10.1177_17455057251353328 for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study by Abdul-Aziz Seidu, Kwamena Sekyi Dickson, Sarah D. Compton, Ruth Owusu-Antwi, Maria Jose Baeza Robba, Carrie Ann Valadez and Michelle L. Munro-Kramer in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251353328 – Supplemental material for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study
Supplemental material, sj-docx-2-whe-10.1177_17455057251353328 for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study by Abdul-Aziz Seidu, Kwamena Sekyi Dickson, Sarah D. Compton, Ruth Owusu-Antwi, Maria Jose Baeza Robba, Carrie Ann Valadez and Michelle L. Munro-Kramer in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251353328 – Supplemental material for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study
Supplemental material, sj-docx-3-whe-10.1177_17455057251353328 for Expanding a primary prevention program to address sexual and gender-based violence among health sciences students in Ghana: A pilot study by Abdul-Aziz Seidu, Kwamena Sekyi Dickson, Sarah D. Compton, Ruth Owusu-Antwi, Maria Jose Baeza Robba, Carrie Ann Valadez and Michelle L. Munro-Kramer in Women’s Health
Footnotes
Acknowledgements
None.
Authors’ Note
Maria Jose Baeza Robba is also affiliated to School of Nursing Pontificia Universidad Catolica de Chile, Santiago, Chile.
Ethical considerations
Study procedures did not begin until ethical approval was received from the University of Michigan Health Sciences and Behavioral Sciences Institutional Review Board (HUM00164788) and the Kwame Nkrumah University of Science and Technology Ethical Review Committee.
Consent to participate
Study procedures were explained to all participants, and then written comprehensive consent was obtained by the research facilitators before data collection.
Consent for publication
Consent for publication was obtained from all subjects involved.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internal funding was provided by the University of Michigan (PI: Compton).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their sensitive nature.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.