
Abstract
Background:
In France, as women now represent the majority of the medical population, there is a discrepancy in the expected life mode for general practitioners and current society standards in a profession with excess of burnout and suicides. To date, there is only a few data available on the evaluation of quality of life of women general practitioner in France.
Objectives:
To evaluate quality of life among this population, and to identify associated factors.
Design:
Cross-sectional study.
Methods:
Participants were women general practitioners practicing in France. Our questionnaire was based on the World Health Organization – quality of life-BREF (26-item). The questionnaire was distributed through various professional networks. This study was approved by our Institutional Review Board. Both simple and multivariable linear models were developed with sensitivity analysis.
Results:
Upon 984 respondent women (mean age 36.2 ± 6.3), 704 (71.5%) were in private practice, 198 (20.1%) were employed and 82 (8.4%) had a mixed practice. They were mostly in couple (90.4%) with at least one child (73.6%). The number of working days and working hours depended on the practice type (p < 0.01). The average World Health Organization – quality of life was 63.0 ± 12.5, 66.2 ± 15.4 for domain 1 (physical), 62.6 ± 15.2 for domain 2 (psychological), 57.7 ± 19.6 for domain 3 (social) and 65.4 ± 13.4 for domain 4 (environment). No significant differences were observed in the global score or across the four domains according to the type of practice. Variables associated with the World Health Organization – quality of life were age (p < 0.01), daily working hours (p = 0.16), numbers of working days per month (p < 0.01), tobacco use (p = 0.11), presence of a secretary (p = 0.14), frequency of socializing with friends (p < 0.01), leisure time availability (p < 0.01), children (p = 0.04), relationship status (p < 0.01), number of weeks of vacations per year (p = 0.15), area of practice (p = 0.15) and place of residence (p = 0.06). After the multivariable model analysis, being in a couple (p = 0.02), having children (p = 0.03), leisure time availability (p < 0.001) and frequent socialization with friends (p < 0.001) were the remaining variables positively associated with the World Health Organization – quality of life. Advance in age (p = 0.002) and tobacco use (p = 0.04) were negatively associated to the World Health Organization – quality of life scores.
Conclusion:
The weight of private life settings appears more important in quality of life assessment in women general practitioners rather than professional settings.
Introduction
The French Public Health System, built after WWII, was lauded in the past decades for being both one of the most equitable systems for patients and an attractive hub for medical researchers. However, changes in society, despite numerous reforms, make the current French system lesser attractive for medical doctors.
According to the French National Epidemiological Institute (INSEE) in 2019, physicians represent 226,859 French citizens, of whom 45% (102,169) are general practitioners (GPs). Between 2016 and 2019, the amount of physicians increased by 1.44% when paramedics increased by 11%. Thus, between 2012 and 2021, density per 100,000 inhabitants decreases from 325 to 318 physicians. This decrease is especially alarming for GP (154 to 140/100,000 during the same period). 1
In France, 68.2% of women of working age (15–64) worked in metropolitan France, with 71.2% working full-time. These two variables are higher for single women and tend to decrease with the number of children. 2
After decades of male over-representation in medicine, the rate is now reversed. According to the National Healthcare Personnel Repository, the generations who were oldest in 2012 and mostly retired by 2021 are predominantly male (almost three-quarters of doctors aged 60–69 in 2012 are men), while the youngest generations are predominantly female. In 2021, 62% of physicians under 40 were women. Similarly, among the 7900 new physicians in 2021, 58% were women. In 2020, women accounted for 50.4% of GPs in regular practice.
Among GP, 66.1% work in private practice under an agreement with the National Social Health System (CNAM). In parallel to changes in the French society, private practice is declining (15% in the past decade). A GP in private practice earns in average €91.670/year, before ~50%-tax. Moreover, female doctors’ fees are on average 34% lower than their male counterparts. These differences in fees could be explained by less sustained productivity: women’s productivity is 33% lower than that of men. 3 The majority of self-employed doctors are men (57% in 2021), while the majority of salaried doctors are women (58%). 1 In addition, half of female GPs declare that they take part in on-call duty, but they do so in a lower proportion than men. The weekly number of hours devoted to their job is 43% lower than for men (6.6 versus 11.5 h). 4
Burnout occurs more frequently among physicians, with a lower quality of life, compared to American workers of the same age class. 5 In gynecologic surgeons, marked gender differences in quality of life are reported, regarding the impact of workload on the time available for themselves, their family and their friends, leading to a high burnout rate. 6 This lower quality of life among physicians occurs since residency. 7 Despite this new balance in sex distribution and changes in priority with the evolution of the society, quality of life of GP remains poorly reported in women GP.
Numerous quality of life assessment scales have been developed, particularly in the medical field in pathological situations, to monitor the extent or modification of quality of life over time. The most frequently used and validated remain the Short Form – 36 Health Survey, the EQ5D-5L and the World Health Organization – quality of life (WHOQOL)-BREF.
Since quality of life assessment in GP physicians is poorly reported in France, we aimed to evaluate it and identify risk factors associated with poor quality of life.
Methods
Survey
We conducted an observational cross-sectional study in 2022 from January 1 to February 1. This study was based on an anonymous online survey. The questionnaire was distributed through various medical doctor’s unions, alumni associations and via restricted GP groups on social networks. Data were collected on a non-profit server (Framaform – The Framasoft Association) with restraining access to the research team only. The reporting of this study conforms to the STROBE statement (Supplemental Material 1).
Participants
Participants included in this study were all women over 18 with a medical degree, specialized in general practice, practicing in France (metropolitan and overseas territories), regardless of their type of practice, with no missing data on the WHOQOL-BREF questionnaire and who agreed to complete the online questionnaire. Participants currently not working were secondarily excluded from the analysis.
Data collection
The WHOQOL questionnaire in its brief form is a validated and reproducible tool for quality of life assessment for various situations.8 –12 This 26-item questionnaire evaluate four domains (physical, psychological, social and environmental). The sum of the Likert scales is converted into a score out of 100.
Data were collected on professional settings: type of practice (private practice versus employed GP versus mixed practice), daily working hours (dichotomized into “⩽8” versus “>8 h/day”), number of working days per month (dichotomized into “⩽16” versus “>16 days/month”), time devoted to general practice (“<50%” versus “⩾50%”), night shifts (yes versus no), presence of a secretary (“No” versus “Remotely” versus “Local”), number of weeks of vacations per year (“<6” versus “⩾6 weeks”), place of work (rural or semi-rural versus urban), area of practice (“Paris and suburbs” versus “Other areas”) and travel time (“<30” versus “⩾30 min”).
Data were collected also on private settings: age (further categorized into quartiles), the number of children (dichotomized into “none” versus “at least one child”), relationship status (in a couple versus single), tobacco use (“none” versus “occasional or more”), alcohol use (“<3” versus “⩾3 glasses/week”), place of residence (rural versus urban), housing type (flat versus house), leisure time availability (yes versus no) and frequency of socializing with friends (“<1” versus “1–4” versus “>4 times/month”).
Ethics
The study was approved by the Institutional Review Board for Non-Interventional Studies (CERDE, University Hospital of Rouen) under the number: E2024-37.
After information, written consent was taken from the subjects before accessing to the questionnaire.
Statistical analysis
Sample size calculation: Prior to data collection, we estimated that a sample of 470 subjects sample (235/group) would be required to observe a difference in mean of 0.1 between two independent groups, based on an French epidemiological study using WHOQOL in women, 13 with a two-tailed test, a 5% alpha-risk and 95% power. Descriptive data are presented as mean ± standard deviation and number (%) for categorical data. Quantitative variables were compared with the Student t-test or ANOVA depending on the number of variables. In case of significance of the ANOVA, a post-hoc Tukey test was conducted. In case of non-normality distribution, we used a Mann–Whitney U-test (two comparisons) or Kruskal–Wallis test (>2 comparisons), in case of significance of Kruskal–Wallis test, a post hoc Dunn test was conducted with Bonferroni correction. The Shapiro tests assessing the normality and homogeneity of variance was checked with Levene tests. Comparisons between two continuous variables involved simple linear regression. Variables with p < 0.2 on univariate analysis were included in the linear multiple models, with no forced variables. The association between associated factors and the WHOQOL-100 was studied using a multiple linear model with backward stepwise selection for adjusted variables. The same analysis strategy was used to assess the association between potential risk factors and the four domains of the WHOQOL-BREF questionnaire. p value below 0.05 was considered statistically significant. All tests were two-sided. Statistical analysis involved using R v4.3.2 (The R Foundation for Statistical Computing, https://www.r-project.org/foundation/).
Results
Population characteristics
The study sample consisted of 984 GP working women with complete data on the WHOQOL-BREF questionnaire (Supplemental Figure S1). The mean age was 36.2 ± 6.3 years and among the 984 women included, 704 (71.5%) were in private practice, 198 (20.1%) were employed and 82 (8.4%) had a mixed practice. Table 1 describes the characteristics of our study sample for both sociodemographic and medical practice characteristics. Among the 890 (90.4%) respondents reporting being in couple, the average duration of the relationship was 10.5 ± 6.4 years and 427 (48.0%) of them reported being the primary breadwinner in the household. Almost three-quarters, 716 (73.6%) women, reported having a child, and among them, the average number of children was 1.9 ± 0.8. Among the 984 women included, 140 (14.2%) reported having a chronic illness. GP women included in this analysis work an average of 14.6 ± 5.9 days/month with an average of 9.5 ± 1.5 h/day. According to the type of practice, there was a significant difference in the average daily working hours (p < 0.01) as well as in the average number of working days per month (p < 0.01). Pairwise Dunn’s test between groups showed that the difference between “Employed GP” and “Mixed Practice,” as well as between “Employed GP” and “Private Practice,” was significant (pBonferroni = 0.02 and pBonferroni < 0.01, respectively) for daily working hours. For the number of working days per month, a significant difference was observed only between “Employed GP” and “Private Practice” (p < 0.01; Supplemental Table S1).
Characteristics of respondents.

GP: general practitioner.
WHOQOL-BREF questionnaire
Upon the 984 women GPs, the average WHOQOL was 63.0 ± 12.5. Table 2 describes the WHOQOL-BREF score and its different components for the entire population and by type of practice. No differences were found in this score based on the type of practice (p = 0.87), as displayed in Figure 1. Scores for the physical health domain ranged 66.2 ± 15.4, 62.6 ± 15.2 for the psychological health domain, 57.7 ± 19.6 for the social relationship domain and 65.4 ± 13.4 for the environment domain. No difference was found between these four domains and the type of practice (Supplemental Figure S2).
WHOQOL-b and subdomains scores according to type of medical practice.
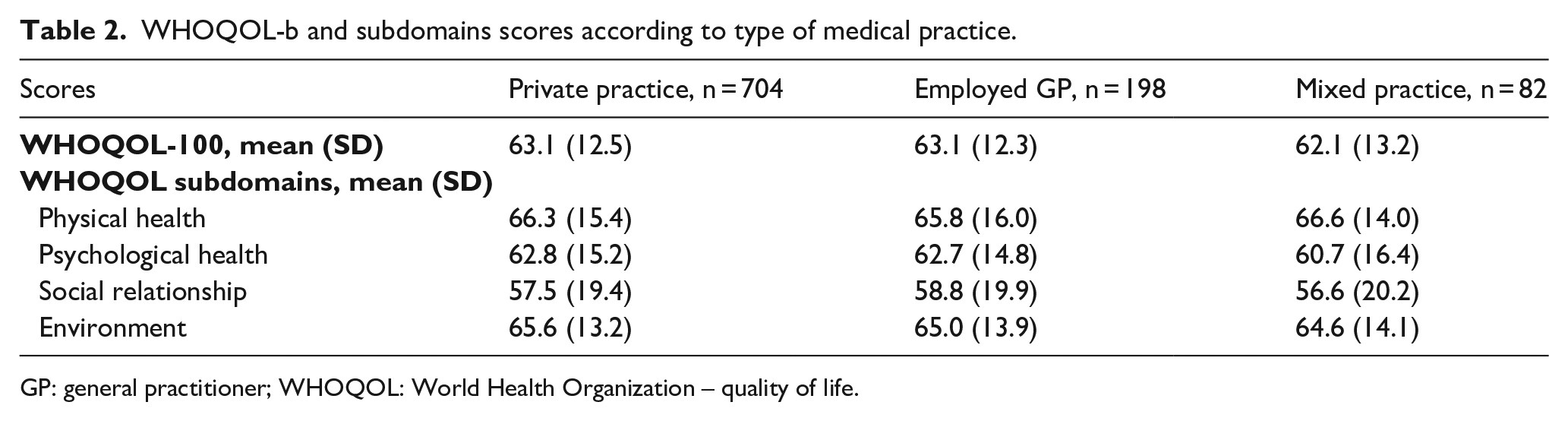
GP: general practitioner; WHOQOL: World Health Organization – quality of life.
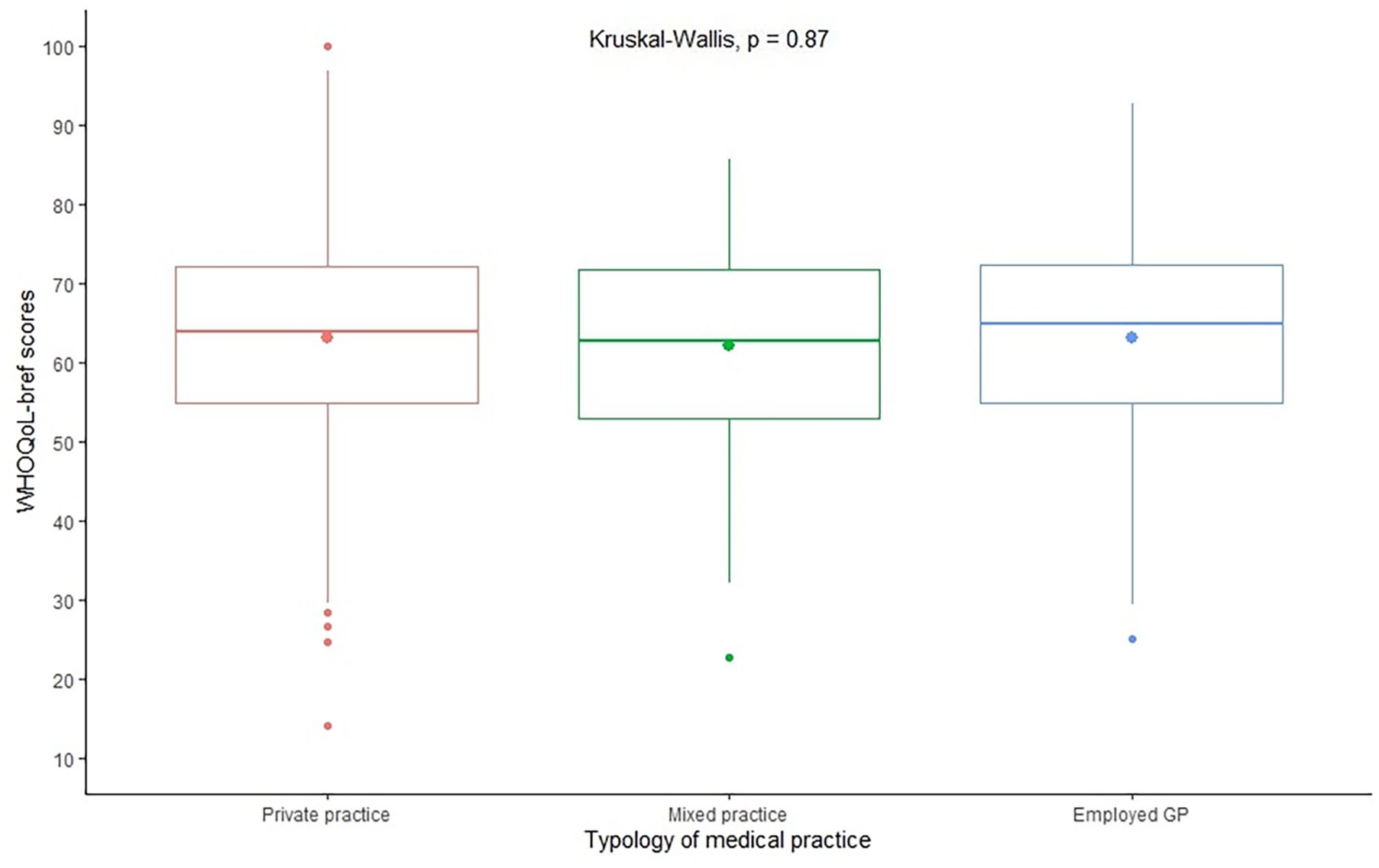
WHOQOL scores according to the type of GP practice. This figure displays mean WHOQOL scores on a 100 scale for the three types of practice and the extent of data. Comparison between groups found no difference between practice type (p = 0.87).
Linear multiple models for the main model
We included in the multivariable regression model the following variables associated with the WHOQOL scores: age (p < 0.01), daily working hours (p = 0.16), numbers of working days per month (p < 0.01), tobacco use (p = 0.11), presence of a secretary (p = 0.14), frequency of socializing with friends (p < 0.01), leisure time availability (p < 0.01), children (p = 0.04), relationship status (p < 0.01), number of weeks of vacations per year (p = 0.15), area of practice (p = 0.15) and place of residence (p = 0.06). Individuals with missing data on the covariates were excluded from this analysis (n = 337). The results of the multiple linear regression after backward stepwise selection are presented in Table 3. In this analysis, we found that being in a couple (p = 0.02), having children (p = 0.03), leisure time availability (p < 0.001) and frequent socialization with friends (p < 0.001) were associated to good quality of life scoring, assessed by the WHOQOL. Advance in age (p = 0.002) and tobacco use (p = 0.04) were negatively associated to quality of life scores. No professional settings for medical practice were found to be associated with quality of life in this analysis.
Multivariate linear regression for the main model (n = 647).

Sensitivity analysis for the four domains of the WHOQOL-BREF questionnaire
As for the main analysis, no significant association was found between covariates related to the mode of practice of general medicine and the four domains of the WHOQOL-BREF questionnaire. Age was negatively associated with the physical health domain (p = 0.01), the psychological domain (p = 0.02) and the environment domain (p < 0.01). Socializing with friends and leisure time availability was positively associated with all the four domains of the WHOQOL-BREF questionnaire (Supplemental Figure S3).
Discussion
In this original work, we collected quality of life data upon 984 French physician women, specialized in GP. Respondents were mostly young, involved a long-time relationship, mainly with children. Although they mostly work <30 days a month, they reported a wide range of working hours. Our main findings were that women with a GP practice appear to have poor quality of life according to the WHOQOL-BREF questionnaire, and only private settings seem to enhance this score after adjustment, in the multivariable analysis. In this study, the mean WHOQOL score was 63.0 ± 12.5. In comparison with the last available extensive national study provided on the French population with the same tool, 13 with results displayed by age class, it is possible to evaluate that our respondents showed poorer quality of life in mean, in their socio-professional and gender categories. Gender difference have not been studied in this survey, as all respondents were women. Age appears as a major factor although we failed to observe a real cumulative effect. In a survey data of 4370 US physicians, women physicians consistently reported significantly worse work–life integration scores when single, after 35, and those working more hours. 14
However, to explain the nonlinear effect of age, we could hypothesize that after a stressful learning curve, GP women reach a plateau of quality of life then affected by cumulative responsibilities. This hypothesis corroborates previous findings highlighting that youngest physician and those having least work control, most work stress, reported the most dissatisfaction. Having children, stress at home, practice type and workload were also identified. However, women physicians are generally satisfied with their careers (84%). 15
In Brazil, among all type of health workers (doctors, nurses, technicians, dentists, etc.) poor quality of life (lowest quartiles) in WHOQOL was observed in 15.4% workers. Associations found were independent of job characteristics and lifestyle. They identified that poor quality of life was associated with imbalanced effort-reward (high effort/low reward) and important commitment at work. 16 When GP physicians lose themselves in their work, the risk of burnout and poor quality of life not only exists but also impacts their global health. Among primary care physicians in Switzerland, more than one-third of respondents reported at least one episode of forgoing care. The most common reason evoked was a heavy workload. Coming to work when sick was associated with female sex, younger age and working full-time. 17 All those results converge to policies which reduce working time to lead to important health benefits. 18
To strengthen these findings, as a mirror, we found that the domain with the lowest scores was the social domain, emphasizing the fact that balance in the social life could be more important than work for this generation. Time dedicated to themselves, especially for socializing with friends, was found as an important factor related to quality of life in our respondents. We could then hypothesize that for young women GP, maintaining a social life is very important. Our respondents mostly dedicated few days of work but with an important efficiency (heavy workload, extended hours). This strategy frees time for other activities. Long working hours are known to increase the risk of injuries and road traffic accidents. Yet, no threshold number of extended hours above which the risks increase is identified. 19 Multiple practice types available in GP allow combining advantages from both private practice and hospital. The risk in private practice is related to extended working hours. According to a recent nationwide survey, 44.8% of French liberal GPs were experiencing burnout (based on the MBI (Maslach Burnout Inventory)). Burnout risk factors in private practice were male gender, working in a suburban area and working over 50 h a week. 20 However, specific burnout and poor quality of life settings are also identified at the hospital, such as the loss of meaning, that the impossibility of dialog with both management and colleagues and daily interactions providing too many conflicts, too much pressure and not enough recognition. 21
The positive effect of having children on quality of life seems easy to understand, if the additional workload provided by them is balanced by an adapted professional workload. Nonetheless, adaptation is needed in private life too. In couples where the wife’s working hours exceed the husband’s, the wife reports lower life satisfaction. 22 Perceived unfairness of the division of household labor could be one possible relevant factor. There is still a need for adaptation of the work environment to women who assume more responsibilities. A US nationwide survey upon physicians women from all specialties returning to work after giving birth, showed the need for schedule flexibility and the need for more support at the institutional level, 23 explaining in part the increase of employed practice as compared to the previous generation. The age of the children is also related to quality of life, such as the presence of support (colleague, spouse and others). Odds of burnout increase in women with young children, especially if home issues are present. 24 In our study, being childless was related to poor quality of life scores. The notion of choice and the burden of a heavy workload and multiple responsibilities may be one explanation. In women, childless by choice in Poland, living in cities, being university-educated and with a good or very good financial standing were identified as protective factors to enhance quality of life. 25
Strengths and limitations
Our study provided a recent insight on the current generation of women working as GP in France. This work with an important sample size (beyond sample size estimation) and a validated tool, provide some evidences to enhance the understanding of quality of life in this population.
However, we suffered from some limitations. The use of a self-administrated questionnaire remains a potential bias however it was only administrated numerically. The cross-sectional design limits the conclusions with the need for following-up answers to limit a potential season effect for instance. As the questionnaire was widely spread, we were concerned about the representativeness of women and a potential selection bias. However, the standardization on age and region of practice, based on national public data on GP did not show difference in standardized rates (data not shown).
Conclusion
In this sample of French women physician in GP, positive factors associated to the WHOQOL-BREF assessment were factors related to social integration: being in a couple, socializing frequently with friends and having children. Age and tobacco use were negatively related to quality of life in this population.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251349613 – Supplemental material for Only private life settings positively affect quality of life of French women general practitioners
Supplemental material, sj-docx-1-whe-10.1177_17455057251349613 for Only private life settings positively affect quality of life of French women general practitioners by Thibaut Sabatier, Julia Blanchemaison, Joël Ladner and Pierre-Emmanuel Cailleaux in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251349613 – Supplemental material for Only private life settings positively affect quality of life of French women general practitioners
Supplemental material, sj-docx-2-whe-10.1177_17455057251349613 for Only private life settings positively affect quality of life of French women general practitioners by Thibaut Sabatier, Julia Blanchemaison, Joël Ladner and Pierre-Emmanuel Cailleaux in Women’s Health
Supplemental Material
sj-pptx-3-whe-10.1177_17455057251349613 – Supplemental material for Only private life settings positively affect quality of life of French women general practitioners
Supplemental material, sj-pptx-3-whe-10.1177_17455057251349613 for Only private life settings positively affect quality of life of French women general practitioners by Thibaut Sabatier, Julia Blanchemaison, Joël Ladner and Pierre-Emmanuel Cailleaux in Women’s Health
Footnotes
Acknowledgements
All authors contributed substantially to the study and approved the final version of the article. The authors thank the Charles-Nicolle Foundation and the INSERM U1073 Laboratory.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board for Non-Interventional Studies (CERDE) under the number E2024-37.
Consent to participate
Written consent was taken from the subjects before accessing to the questionnaire.
Consent for publication
All individual participants received an information about the use of their data for research purposes and publication. According to the IRB for this study, this consent is not mandatory.
Author contributions
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Dataset generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request for scientific purposes.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.