
Abstract
Background:
Overactive bladder and urinary incontinence are strongly associated with falling in older adults. Despite this established link, research on how women experience these coexisting conditions is lacking.
Objective:
This study aimed to better understand how older women with both urgency urinary incontinence and an increased risk of falls perceive their urinary symptoms in relation to fall risk.
Design:
Mixed-methods study using concurrent triangulation design with qualitative interviews and quantitative patient-reported outcome measures.
Methods:
English-speaking women aged 60 and older with urgency or mixed urinary incontinence who screened positive for fall risk were recruited through online advertising. Fall risk was assessed using the Centers for Disease Control and Prevention’s Stopping Elderly Accidents, Deaths, and Injuries “3 Key Questions.” Semistructured interviews explored participants’ perspectives on urinary symptoms, fall risk, and quality of life. Standardized measures included the Falls Efficacy Scale International, PROMIS Physical Function, The International Consultation on Incontinence Modular Questionnaire – Overactive Bladder symptom severity scale, The International Consultation on Incontinence Modular Questionnaire Lower Urinary Tract Symptoms Quality of Life Module, and Functional Comorbidity Index. Thematic analysis of interview transcripts was conducted using constant comparison. Multiple regression models examined associations between fear of falling, symptom severity, physical function, and urinary incontinence-related quality of life.
Results:
Sixty women responded to the online advertising for the study and completed the initial screening questionnaire. Twenty-five were enrolled and interviewed. Mean age was 68 ± 4.7. None were aware of linkages between urinary incontinence and falls. Their concerns about falling were unique to the experience of living with a urinary condition and often interacted with social stigma such as embarrassment from incontinence after a fall. Fear of falling was more strongly associated with urinary incontinence-related quality of life than symptom severity, physical functioning, or comorbid burden after adjusting for age (p < 0.01). Fear of falling and symptom severity were the only factors significantly associated with urinary incontinence-related quality of life in regression models.
Conclusion:
There is a need to better communicate to older women with urinary incontinence the known risk of falling associated with their urinary condition.
Introduction
As a multifactorial geriatric syndrome, the effects of urinary incontinence (UI) reach far beyond embarrassment and impaired quality of life. UI is associated with greater risk of depression, social isolation, loss of independence, institutionalization, and injurious falls.1,2 More than one in three older women live with this stigmatizing condition.3,4 But these estimates are likely imprecise: fewer than half of those affected are believed to report their bladder control problems to health care provider. 5
Urgency UI (UUI) is one of the most common UI types in women 3 (prevention of urinary and fecal incontinence in adults) and defined as a sudden, intense urge to urinate followed by an involuntary loss of urine. It is a characteristic symptom of overactive bladder (OAB) and is strongly associated with falling.6,7 The etiology is complex and is believed to have both environmental and central nervous system contributors.8,9 The urge to urinate frequently on a daily basis can limit physical activity as well. Concern for finding oneself too far from a bathroom can be a powerful motivator for just staying home. 10 For older adults, however, the consequences of reduced physical activity and social isolation are well established: a debilitating spiral of loss of confidence, weakness, physical frailty, fear-of-falling, and falls. 11
Despite the known linkages between UI and fall risk, little is known about the actual lived experiences of women with both co-existing conditions. Qualitative interviews can provide unique personal perceptions of how UI and falls impact daily life, their depth of knowledge on the association between their urinary condition and risk of falling, and the degree to which UI and falls are viewed as separate, unrelated problems or concerns. The objective of this study was to explore perspectives of older women with coexisting UI and increased fall risk and to better understand linkages between concerns about falling, OAB symptoms, and physical functioning. This information could inform more targeted interventions for this patient population and help better elucidate the bidirectional mechanisms that link geriatric syndromes such as UI falls.
Methods
Design
This mixed-methods study used a concurrent triangulation design. 12 The purpose of concurrent triangulation designs is to use both qualitative and quantitative data to more accurately define relationships among variables of interest by obtaining different but complementary data on the same topic. Participants were recruited through targeted online advertising and screened against specific inclusion criteria to identify women with coexisting UUI and high fall risk. The study was conducted over a 6-month period during 2022.
Participants
Inclusion criteria included English-speaking females aged 60 and older with UUI or mixed UI (i.e. both stress and urgency incontinence). UI type was identified using the “3 Incontinence Questions (3IQ)” questionnaire. The 3IQ can identify and classify UUI and stress urinary incontinence (SUI) with reasonable accuracy. 13 Because UUI has been most strongly associated with fall risk, women with 3IQ responses suggestive of stress only UI were excluded. Other inclusion criteria were ambulatory (i.e. able to walk across a small room with or without an assistive device) and an answer of “yes” to one of the questions on the “3 Key Questions” questionnaire. The “3 Key Questions” are part of the Stopping Elderly Accidents, Deaths, and Injuries initiative developed by the Centers for Disease Control and Prevention (CDC) to facilitate fall risk identification and management in primary care. 14 Answering “yes” to any of the following three questions is a screen positive for increased fall risk 15 : (1) Have you fallen in the past year? (2) Do you feel unsteady when standing or walking? and (3) Do you worry about falling?
Exclusion criteria included stress or other cause predominant UI, male (their causes of UI are often different than women); unable to give verbal informed consent; neurologic conditions known to contribute to incontinence (multiple sclerosis, Parkinson’s disease, traumatic brain injury (TBI), dementia, and stroke survivors with limited mobility); current or prior surgically implanted sacral nerve stimulation device or botulinum toxin bladder injections for incontinence; genitourinary cancer undergoing active treatment with chemotherapy or radiation; and chronic kidney disease undergoing dialysis.
Procedures
Potential participants were recruited and initially screened via an online research recruitment platform. The platform helps researchers efficiently find and screen eligible participants through targeted online advertising and automated screening processes. The online advertising was directed to the geographic location surrounding the study site. Those who passed the initial online screening were further screened via a follow-up phone call by a research team member (L.A., C.U.) Participants were informed about the research team and the general focus of the study during this initial encounter. The formal interview was conducted if appropriate scheduled for the near future. All interviews were conducted via teleconferencing platform and took ~1–1.5 h. Verbal consent was recorded and obtained prior to the start of the interview. Completion of the questionnaires occurred following the semistructured interview. Verbal consent, the interviews, and questionnaires were conducted using a semistructured interview guide by team members (C.U., M.P.).
Interview guide
The semistructured interviews consisted of open-ended questions relating to experiences in their daily lives relevant to OAB and UUI; their knowledge of the association between UI and falls; and their attitudes toward possible linkages. Example of the open-ended questions included: What are your thoughts on how concerns about falling might be related to your urinary condition? The audio-recorded interviews were transcribed professionally. All audio recordings and transcripts were stored on in a secured network folder accessible only to the study team.
Measures
Sociodemographic characteristics included age, ethnicity (non-Hispanic Black, non-Hispanic White, Hispanic, other) and body mass index (height in meters divided by weight in kilograms squared). Validated quantitative questionnaires were also used to assess self-reported participant physical functioning (PROMIS Physical Function—Short Form 8b), fear of falling (The Falls Efficacy Scale International (FES-I)), severity of urinary symptoms (The International Consultation on Incontinence Modular Questionnaire (ICIQ) – OAB), UI-related impact on quality of life (The International Consultation on Incontinence Questionnaire Lower Urinary Tract Symptoms Quality of Life Module (ICIQ-LUTSqol)), and comorbid burden (Functional Comorbidity Index (FCI)). See Supplemental Materials for examples of the questionnaires.
PROMIS Physical Function—Short Form 8b includes eight Likert type questions on functioning of upper extremities, lower extremities (walking or mobility), as well as instrumental activities of daily living, such as running errands. 16 Scores range from 8 to 40 with higher scores associated with poorer physical functioning. We used the PROMIS physical function T-score which rescales the raw score into a standardized score with a mean of 50 and a standard deviation (SD) of 10. The physical functioning of a person with a T-score of 40, therefore, is one SD below the mean. Because physical functioning is strongly associated with falls, we also dichotomized the continuous score into lower versus higher function and stratified themes and subthemes by level of functioning.
The FES-I 17 is a patient reported outcome that measures level of concern about falling during daily activities inside and outside the home whether or not she actually does the activity. 18 The 16-item questionnaire has a range of 16–64. Higher scores indicate more concern about falling. Its target population is older adults with or without a history of falling. It has good predictive validity for future falls, muscle weakness, and overall disability. It also has validated thresholds of clinical importance to older adults with a cut-point of ⩾23 identified as a level of concern associated with future adverse outcomes.
ICIQ-OAB is a patient-reported outcome that captures self-perceived degree of urinary frequency, urinary urgency (rushing to the bathroom), and urge incontinence (leakage), as well as symptoms related to nocturia (nighttime urination). 19 The 4-item scale ranges from 0 to 16 with greater values indicating increased symptom severity.
ICIQ-LUTSqol 20 measures the influence of UI problems on the quality of life, limitations in general, physical and mental activities, and changes in interpersonal relations and in everyday life. Scores range from 19 to 76, with greater values indicating an increased impact on quality of life.
The FCI is an index of 18 comorbid diseases. 21 The total number of comorbid conditions present is summed to obtain a total FCI score. It is used to predict general health status and adjust for comorbidity confounding in studies of chronic conditions, with physical function as the outcome of interest. The underlying premise of the measure is that diagnoses associated with physical function would be, at least in part, different from those associated with mortality.
Qualitative analysis
The transcripts from the qualitative data were coded using thematic content analysis techniques. 22 The senior author (M.P.) and another team member (C.U.) independently coded each of the transcripts following a constant comparison approach from grounded theory. After coding five interviews, the coders met to discuss coding consistency and identify any inconsistencies, 23 until all interviews were coded. NVivo 12 Plus (software tool designed for qualitative data analysis) was used to analyze the transcripts and identify themes. Text searches were also employed within the software to identify all relevant quotes for each of the themes and respective subthemes. All members reviewed the findings for member checking and verifying coding quality. The first and senior authors (S.R.F., M.P.) identified exemplar quotes for inclusion. Saturation was achieved when no new themes emerged supporting the adequacy of the sample size for addressing the study’s objectives. 24 The Consolidated Criteria for Reporting Qualitative Research was used to guide the reporting of the qualitative results. 25
Statistical analysis
Means (with SDs) and percentages were calculated using the Statistical Analysis System (SAS) data management software package for the quantitative measures to describe participant demographic and clinical characteristics. Descriptive statistics were also used to plot the frequency of responses to each of the 3 Key Questions fall risk screen by urinary condition type. We then compared the themes identified in the qualitative interviews with statistical analysis of the quantitative data to further examine linkages between UI related quality of life, severity of symptoms, and fear of falling. Four separate regression models were built to prevent overparameterization with this sample size and continuous ICIQ-LUTSqol as the outcome, each model adjusting for participant age. The primary predictors for the separate models included known fall risk factors 26 : comorbid burden, physical functioning, fear-of-falling, and symptom severity (each factor in its own model with age).
Results
Sixty women responded to the online advertising for the study and completed the initial screening questionnaire. The most common reasons for a screen fail were a negative screen on the 3 Key Questions fall risk instrument; the participant lived outside the targeted geographic area; symptoms suggesting stress UI predominance; had a recent surgically implanted sacral nerve stimulation device or botulinum toxin bladder injections; and was less than 60 years old. Five women who passed the initial online screening were subsequently excluded during the first phone conversation.
Twenty-five women ⩾60 years of age with either UUI (56%) or mixed UI (44%) were enrolled and interviewed. Table 1 shows their demographic and clinical characteristics. Mean age was 68 ± 4.7 years. The majority were non-Hispanic white (72%) followed by non-Hispanic Black (16%) and Hispanic (12%). Mean body mass index was 34 ± 8.0. Mean score for the FES-I was 37.48 ± 8.3; all, but one participant scored above the FES-I threshold (i.e. 23) predictive of increased risk of adverse health events. The mean T-score for the PROMIS physical function measure was 41.05 ± 6.7. Participants in the sample had on average, 5.2 ± 2.8 comorbidities.
Demographic and clinical characteristics.
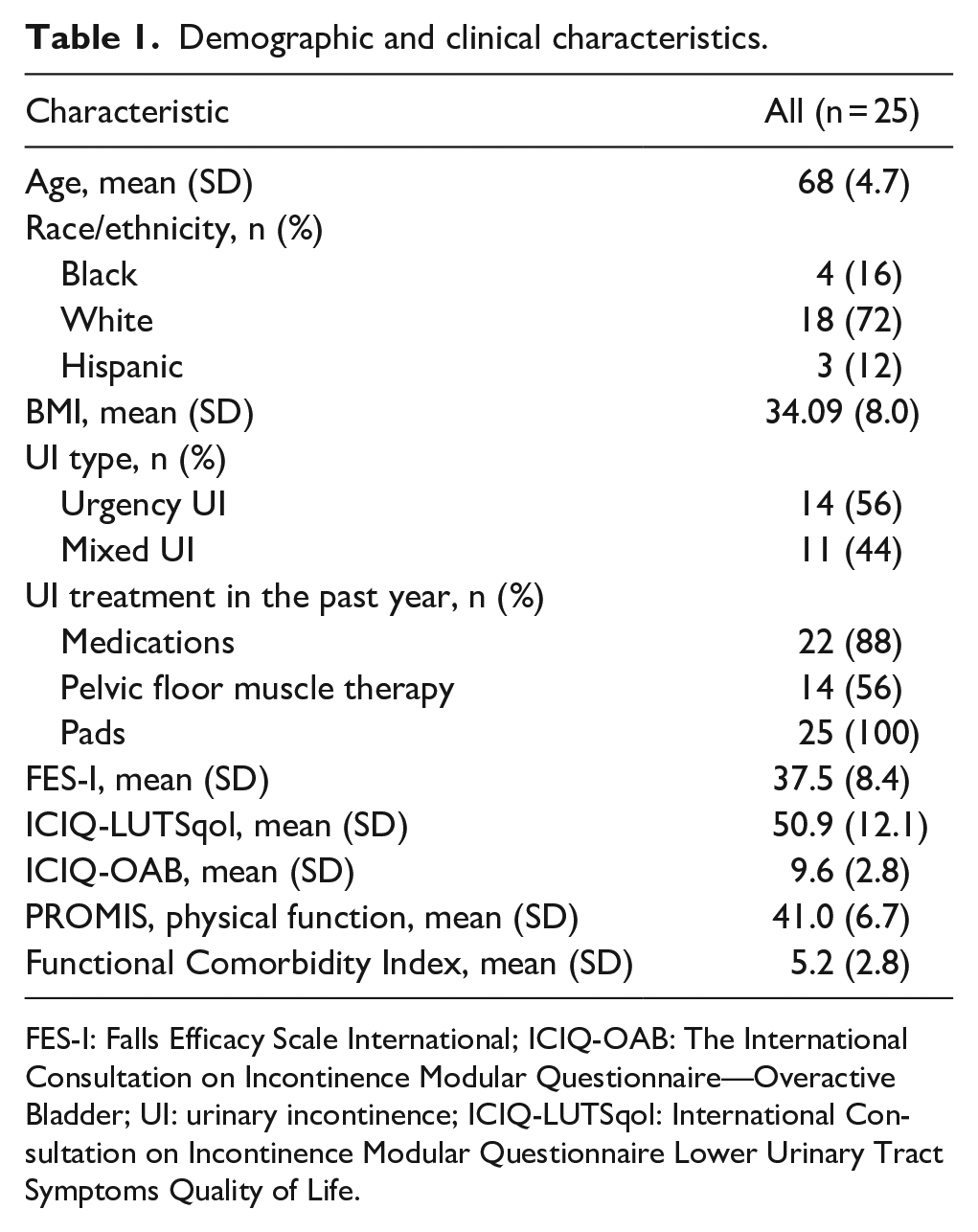
FES-I: Falls Efficacy Scale International; ICIQ-OAB: The International Consultation on Incontinence Modular Questionnaire—Overactive Bladder; UI: urinary incontinence; ICIQ-LUTSqol: International Consultation on Incontinence Modular Questionnaire Lower Urinary Tract Symptoms Quality of Life.
Figure 1 breaks down the frequency of “yes” responses to each of the “3 Key Questions” for those characterized as UUI predominant and mixed UI predominant. More women with UUI reported a past “Fall History” and were “Worried About Falling.” The frequency of the distribution of “Feels unsteady when walking was similar for both conditions.”

Frequency of responses to the 3 Key Questions by UI type.
The thematic content analysis of the recorded interviews revealed three main themes: (1) limited awareness of linkages between UI and falls; (2) fear of falling concerns are unique to the –experience of living with UI; and (3) UI-related behavioral changes secondary to concerns about falling are common. The main themes and the exemplary quotes identified via the thematic analysis are shown in Table 2.
Theme 1: Limited awareness of linkages between UI and falls. None of the women made a direct connection between UI and falls, and none had discussed the issue with a health care provider. They viewed fall risk and UI as each being separate phenomenon that were unrelated. Falls and concerns about falling were most often attributed to things like trip hazards on the way to the bathroom, old age, vision, and motor control problems, decreased strength, and clumsiness. Trip hazards were frequently reported; concern was shared about tripping over pets, slipping on rugs, wet floors, bumping into objects, or just being unaware of their surroundings when rushing to the bathroom.
Theme 2: Fear of falling concerns are unique to the experience of living with UI. Scores on the FES-I highlighted that fear of falling was a significant issue for these women. The qualitative interviews suggested that this fear might be intricately linked to the unique experience of living with UI. Specifically, the embarrassment associated with potential incontinence after falling, especially in public scenarios like rushing to a bathroom, emerged as a predominant concern. This insight underscores the complex interplay between physical health issues and social-psychological factors in shaping individuals’ experiences and fears.
Theme 3: UI-related behavioral changes secondary to concerns about falling are common. Behavioral changes that reflected an underlying concern about falling were common, even though a direct connection between the behavior, UI, and related fall risk may not have been made. These included reported behavioral changes related to likelihood of a fall, such as gait alterations, clearing paths to the bathroom whenever possible, being careful when rushing to the bathroom, or increased awareness of one’s surroundings and locations of bathrooms.
Major themes and subthemes identified in the qualitative analysis.

Quantitative findings and integration
Concerns about falling were more strongly associated with UI-related quality of life than symptom severity, physical functioning, comorbid burden, and age. Fear-of-falling and symptom severity were the only factors associated with UI-related quality of life after adjusting for age. Fear-of-falling, however, had a much smaller p-value, and its model had a larger R2 (Table 3). This indicates that a higher percentage of the variability in UI-related quality of life was accounted for by fear-of-falling as compared to symptom severity. This finding provides some insight into the major themes identified in the qualitative analysis. The strong positive association between fear of falling with quality of life suggests fear of falling is a significant concern, but the qualitative findings suggest that more education is needed regarding raising awareness of behaviors frequently encountered when living with UI that increases fall risk. In addition, the qualitative data indicate that the strong association between fear-of-falling and UI-related quality of life is directly related to the social stigma that accompany living with UI, such as embarrassment from accidents after the fall.
Regression models predicting OAB related quality of life.

All models adjusted for age.
OAB: overactive bladder.
Functional Comorbidity Index.
PROMIS self-report physical functioning.
Falls Efficacy Scale International.
International Consultation on Incontinence Modular Questionnaire – OAB.
Discussion
This study investigated the perspectives of older women with UUI who were also at high risk of falling. Key findings were a lack of awareness of the known associations between their urinary condition and falls in older women; a general disconnect between frequent behaviors that result because of UUI and the increases in fall risk that accompany those behaviors; and concerns about falling that are likely unique to this patient population.
UUI and other LUTS such as frequency and nocturia are highly prevalent among older women. In addition, the association between LUTS and falls is well recognized. 27 Older adults with UUI are significantly more likely to fall and sustain an injury compared to age-matched controls (with estimates of the odds ratio for falls ranging from 1.5 to 2.3)6,28 and have higher health care costs. 29 Participants in the current study viewed fall risk and UI as each being separate phenomenon that were unrelated. Among those who accepted and gained new knowledge about the link between UI and falls, none reported that the issue of fall risk and their urinary condition had ever been discussed with a health care provider.
The mechanisms underlying linkages between LUTS and fall risk has not been fully explained. No clinical trials have been conducted to see if treating LUTS can reduce the risk of falling, despite calls for such work to be undertaken. 30 Behaviors associated with LUTS that are known to increase fall risk were commonly reported by women in this study, however. These included the diverting of cognitive attention and dual-tasking while walking31,32 that can occur in the midst of an urgency episode. Self-imposed activity limitations can also lead to deconditioning and a decline in general health. 33 Side effects of commonly used medications (e.g. blurred vision, balance or motor problems)34,35 have been implicated as well. Our findings are in some conflict with current literature on the association between rushing to the bathroom and falling. Some studies have found no strong temporal associations between getting to the toilet and falling,36,37 but the frequency of the occurrence reported by these women and the many efforts some took to potentially lessen the likelihood of falling during urgency suggest it is likely an important factor worthy of further study.
All the women in this study reported clinically meaningful levels of concern about falling. Fear of falling (i.e. low self-perceived confidence in engaging in activities of daily living without falling) is a serious health condition in older adults that commonly occurs in those identified at high risk for falls. 33 Fear of falling is also highly prevalent in the UUI and OAB patient population.38,39 Associations between fear of falling and quality of life can be independent of fall events and appear to be more important than actual falls on perceived quality of life. 33 Unique to this study was the finding of associations between concerns about falling and the embarrassment of wetting oneself during or after a fall. A fear of falling is known to make people more conscious of their surroundings and in the extreme can lead to activity restrictions and reduced social participation. Both consequences share characteristics with the lived experiences these women reported from dealing with their condition while just going about their daily routine.
Limitations
This study has limitations. Recruitment was accomplished with an online advertising service and so limited to those who had internet access. There is some evidence, however, that when compared with traditional recruitment methods (print, radio, television, and email), benefits include shorter recruitment periods, more diverse representation, and improved participant selection in hard-to-reach demographics and patient populations. 40 In addition, we relied on screening tools to characterize fall risk and the target urinary conditions, but both were intended for use in clinical settings. The 3 Key Questions were developed by the CDC to facilitate fall risk identification in primary care. The 3IQ questionnaire was also developed for use in primary care and is a simple, quick test with acceptable accuracy for classifying urge and stress incontinence among women, with some evidence it is best at classifying stress only incontinence.13,41 For this study, however, we believe self-reports from the interviews corroborated that the participants primary concerns centered around those typically encountered by women who have UUI.
Conclusion
This was the first study to describe the lived experiences of women with co-existing UUI and a positive screen for high risk of falling. Findings suggest more work is needed to communicate potential linkages between specific urinary conditions and related behaviors that may increase the risk of falling in older women. In the clinic, this could include raising the topic with patients whose profile suggests falls may be a concern; developing education materials that help make the connection between behaviors that often occur with UI and how they may impact fall risk; incorporating fall risk into UI treatment options discussions; and when medications are indicated, discussing the fact that the side effects of some drugs may42,43 impact risk of falling more than others.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-1-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-2-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-3-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-4-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-5-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-5-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-6-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-6-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Supplemental Material
sj-docx-7-whe-10.1177_17455057251347079 – Supplemental material for Perspectives of older women with coexisting urinary incontinence and high fall risk
Supplemental material, sj-docx-7-whe-10.1177_17455057251347079 for Perspectives of older women with coexisting urinary incontinence and high fall risk by Steve R. Fisher, Alejandro Villasante-Tezanos, Lindsay M. Allen, Carolyn Utsey, Gokhan Kilic and Monique R. Pappadis in Women’s Health
Footnotes
Acknowledgements
We want to thank the study participants for their generous participation time and insight into these health conditions and Lourdes Munoz, DPT for her assistance with this project.
Ethical considerations
The University of Texas Medical Branch Institutional Review Board approved the study (IRB #20-0118).
Consent to participate
All participants provided verbal informed consent.
Consent for publication
Participants provided consent to publish findings from this research.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this publication were developed with support from grants from the National Institute on Aging (NIA grant numbers NIA R21 AG078153; Fisher); K01AG065492 (Pappadis); and P30AG024832 (Morrow); and the National Institute on Minority Health and Health Disparities (NIMHD contract number L60MD009326L; Pappadis). The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official institutional position or any other federal agency, policy, or decision unless so designated by other official documentation. The contents of this publication do not necessarily represent the policy of the National Institutes of Health, and you should not assume endorsement by the Federal Government.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The quantitative datasets generated during this study are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.