
Abstract
Urinary incontinence is a common and distressing condition, which, although not life-threatening, is known to have a significant effect on quality of life. The incidence of urinary incontinence increases with age and while stress urinary incontinence is more common in younger women, symptoms suggestive of overactive bladder are more common with increasing age. All women complaining of incontinence require simple investigation, and many will benefit from conservative and medical treatments, which may be instituted in primary care. Further investigation in the secondary-care setting should be reserved for those women with refractory or unusual symptoms. The aim of this paper is to review the epidemiology and pathophysiology of common causes of urinary incontinence in younger, premenopausal women, and to review the current algorithms for investigation and management. In addition, treatment paradigms covering conservative, medical and surgical treatment for stress urinary incontinence and overactive bladder will be reviewed.
 Medical Education Online
Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 75% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Evaluate the effects of pregnancy on urinary tract function among women Assess the diagnostic process for women with urinary incontinence Identify the medical management of stress urinary incontinence (SUI) Analyze nonsurgical and surgical treatments of SUI
Financial & competing interests disclosure
CME Author
Author & Credentials
Editor
Urinary incontinence, the complaint of any involuntary leakage of urine [1], is a common and distressing condition, which, although not life-threatening, is known to adversely affect quality of life (QoL) [2]. The incidence of urinary incontinence tends to increase with age, and many younger women may also complain of troublesome urinary symptoms, which necessitate further investigation. While younger, more active women may commonly complain of stress urinary incontinence (SUI), many may also be bothered by symptoms suggestive of overactive bladder syndrome and, consequently, an accurate diagnosis should be made if appropriate management is to be instigated (Box 1). Many women will benefit from investigation both in primary and secondary care, and this should be tailored to the individual patient depending on symptoms and symptom severity. While behavioral modification and conservative measures are important in the initial management of those with refractory or more persistent symptoms, many benefit from both medical and surgical intervention.
The aim of this review is to investigate the epidemiology and pathophysiology of urinary incontinence in younger women, as well as reviewing the current management algorithms on which to base investigation and treatment.
Causes of urinary incontinence in women.
Urodynamic stress incontinence
Detrusor overactivitli:
– Idiopathic
– Neurogenic
Fistulali:
– Vesicovaginal
– Ureterovaginal
– Urethrovaginal
Congenital abnormalitieli:
– Epispadias
– Ectopic ureter
Urethral diverticulum
Temporary: urinary tract infection
Epidemiology
One of the largest epidemiological studies of urinary incontinence has been reported in 27,936 women from Norway, of which 15 out of 116 (54%) were premenopausal [3]. When considering all age groups, 25% of women reported symptoms of urinary incontinence, although, only 7% felt their symptoms were bothersome. The prevalence of incontinence was also found to increase with age, and 50% of women complained of stress, 11% of urge and 36% of mixed incontinence.
Pregnancy & childbirth
Pregnancy is associated with changes in lower urinary tract physiology and, consequently, urinary symptoms are more common. Urine production increases in pregnancy due to increasing cardiac output, and a 25% increase in renal perfusion and glomerular filtration rate. Consequently, many lower urinary tract symptoms may simply represent physiological, rather than pathological, changes.
Urinary frequency affects 60% of women in the first- and mid-trimester and 81% in the last trimester. While nocturia is also a common symptom, it was only felt to be troublesome in 4% of cases. Urgency and urgency incontinence also increase during pregnancy; in multiparous women, urgency incontinence has been demonstrated to have a peak incidence of 19%; however, other studies have reported an urgency incontinence incidence of 10% and urgency of 60%. The incidence of detrusor overactivity (DO) and low compliance in pregnancy has been reported as 24 and 31%, respectively. In addition, stress incontinence is more common in pregnancy, with 28% of women complaining of symptoms, although, only 12% remained symptomatic following delivery [4].
Childbirth is also known to have an effect on lower urinary tract symptoms, and the effect of age and parity has been investigated. The prevalence symptoms among nulliparous women ranged from 8 to 32% and was seen to increase with age. In general, parity was associated with incontinence and the first delivery was found to be the most significant. The relative risk of stress incontinence was 2.7 (95% CI: 2.0–3.5) in the age group 20–34 years for primiparous women and 4.0 (95% CI: 2.5–6.4) for multiparous women. There was a similar association for mixed incontinence, although, not for urge incontinence [5]. The authors concluded that parity was an important risk factor in younger women, although this association was noted to disappear with age.
Mode of delivery has also been investigated in a large population-based cohort study of 5236 primiparous women in Sweden followed-up over 20 years after a single delivery. Overall, the prevalence of stress incontinence, urgency incontinence and mixed incontinence was 15.3, 6.1 and 14.4%, respectively, and was higher in all types of incontinence following vaginal delivery when compared with cesarean section. Moderate-to-severe incontinence was more prevalent after vaginal delivery than after cesarean section (21.3 vs 13.5%; odds ratio [OR]: 1.68; 95% CI: 1.40–2.03). In addition, the prevalence of bothersome urinary incontinence was also greater after vaginal delivery (11.2 vs 16.3%; OR: 1.85; 95% CI: 1.42–2.39) [6].
Stress incontinence
SUI may be a symptom, a sign or a urodynamic diagnosis; urodynamic stress incontinence (USI) is defined as the involuntary leakage of urine during increased abdominal pressure in the absence of a detrusor contraction [1]. Stress incontinence has been shown to be more common in younger, more active women [3].
Pathophysiology
The symptoms of stress incontinence are associated with urethral hypermobility and intrinsic sphincter deficiency. While the former is caused by a weakness in the pelvic floor musculature, pelvic fascia and pubourethral ligaments, the latter is caused by pudendal nerve damage and damage to the intrinsic and extrinsic urethral sphincter.
More recently the ‘integral theory’ has been described by Petros and Ulmsten [7]. This proposes that the distal and midurethra are key for the continence mechanism [8], and maximal urethral closure pressure is controlled at the midurethral point [9].
Overactive bladder
Overactive bladder (OAB) is defined as a symptom complex of urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of a urinary tract infection or other obvious pathology [1].
Pathophysiology
The symptoms of OAB are thought to be due to involuntary contractions of the detrusor muscle during the filling phase. These contractions are termed DO [2] and are mediated by acetylcholine-induced stimulation of the bladder muscarinic receptors [10]. However, the terms OAB and DO are not synonymous; the former is a subjective symptom-based diagnosis, while the latter is an objective urodynamic diagnosis. While the majority of patients with DO complain of OAB symptoms, not all women with OAB have DO, and there are many other causes of frequency and urgency. Approximately 64% of patients with OAB have urodynamically proven DO, while 83% of patients with DO have symptoms suggestive of OAB [11].
The pathophysiology of DO remains unclear, although the association with outflow obstruction has been recognized for some time [12], as well as the observation that relaxation of the urethra is known to precede contraction of the detrusor in a proportion of women with DO [13]. In addition, the myogenic hypothesis has suggested that partial denervation of the detrusor muscle may lead to increased excitability and increased ability of activity to spread between cells, resulting in coordinated myogenic contractions of the whole detrusor [14]. Conversely, the neurogenic hypothesis of DO has proposed that the detrusor cells develop a postjunctional supersensitivity, possibly due to partial denervation [15], with reduced sensitivity to electrical stimulation of its nerve supply but a greater sensitivity to stimulation with acetylcholine [16]. Sensory pathways are also thought to be important and the urothelial afferent hypothesis has described the role of afferent activation in the urothelium and suburothelial myofibroblasts as a cause of DO. Mediators, such as prostanoids [17] and nitric oxide [18], are synthesized locally in the urothelium and may also be released by bladder distension. This cascade of stimulatory and inhibitory mediators are involved in sensory pathways during bladder filling [19], and may be involved in the pathogenesis of DO.
Clinical presentation
Women commonly complain of a multitude of lower urinary tract symptoms, and these may be grouped into storage and voiding symptoms. Storage symptoms include frequency, urgency and nocturia, in addition to stress and urgency incontinence (Box 2). Voiding symptoms are less common in women and include hesitancy, poor stream and incomplete emptying, although, may also be associated with symptoms of incontinence secondary to retention and overflow. Younger women may also present with lower urinary tract symptoms related to sexual intercourse, as well as recurrent urinary tract infection. Some drugs are known to affect lower urinary tract function including diuretics, calcium antagonists, antidepressants and α-adrenergic antagonists and, therefore, a review of medication should be performed in all patients.
Clinical signs
While there are no specific clinical signs in women with urinary incontinence demonstrable urinary leakage may be noted on a cough stress test. A pelvic examination is also important to exclude the presence of urogenital prolapse, uterine fibroids or a pelvic mass, all of which may cause storage symptoms and incontinence. In addition, storage symptoms may also be associated with neurological conditions, and therefore, a basic neurological examination should be performed.
Investigations
While many women with urinary incontinence may be managed initially with conservative measures, all patients should have a basic assessment in order to confirm the diagnosis, as well as excluding any other underlying causes for lower urinary tract dysfunction (Figure 1).
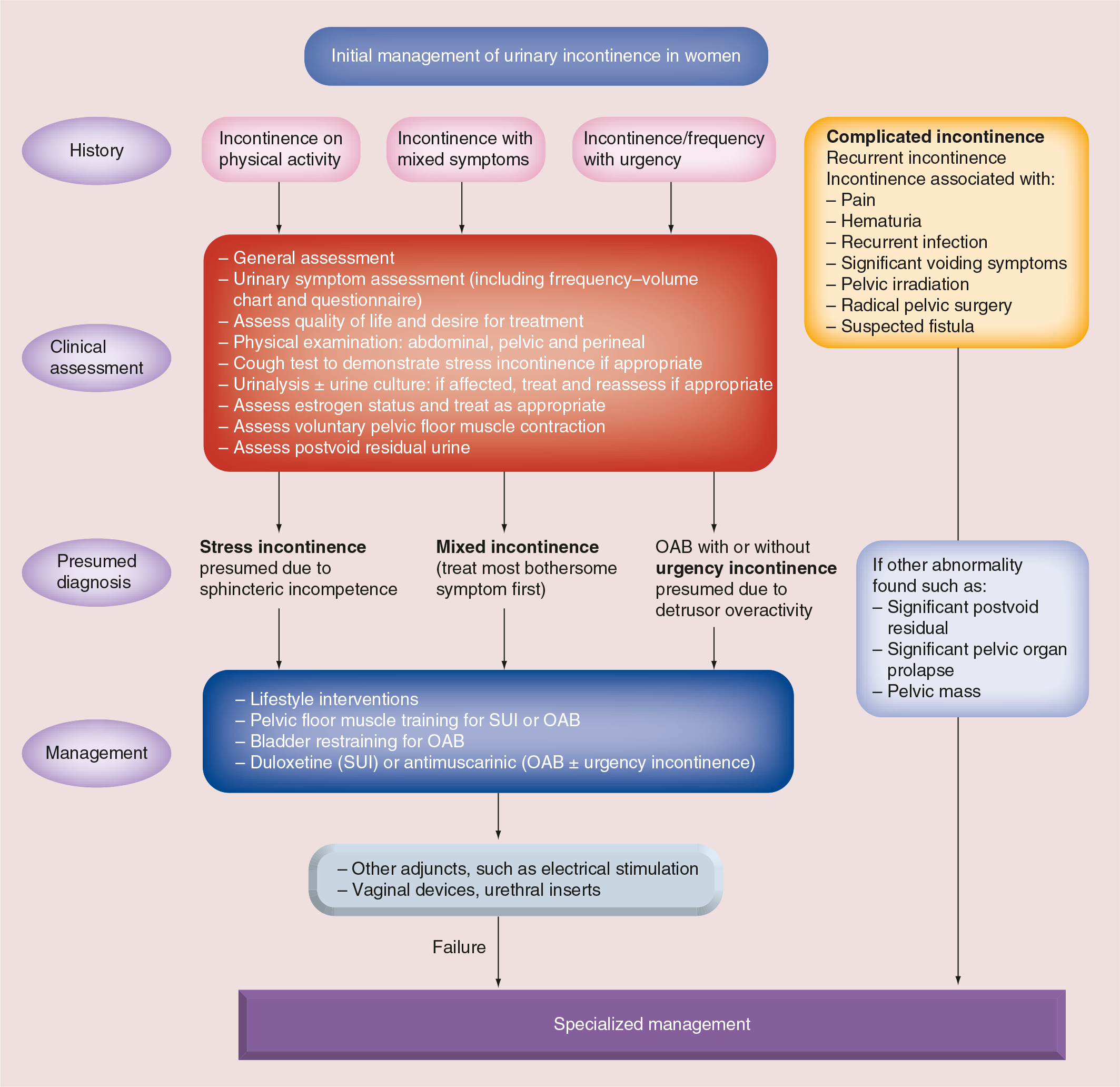
Initial assessment of urinary incontinence (International Consultation on Incontinence Guidelines 2013).
Urine culture
Urinalysis should be performed at the time of initial presentation and, if abnormal, a midstream specimen of urine should be sent for microscopy, culture and sensitivity in order to exclude lower urinary tract infection.
Postmicturition urinary residual
Voiding difficulties may present with symptoms of frequency and urgency, in addition to the symptoms of stress incontinence. Clinical examination is only useful in excluding large residuals, and therefore, a postmicturition ultrasound of the bladder or catheterization, should be performed to exclude a chronic urinary residual.
Lower urinary tract symptoms.
The complaint of involuntary loss of urine on effort or physical exertion, or on sneezing or coughing
The complaint of involuntary loss of urine associated with urgency
The complaint of involuntary loss of urine, which occurs during sleep
The complaint of involuntary loss of urine associated with urgency, and also with effort or physical exertion or on sneezing or coughing
The complaint of continuous involuntary loss of urine
The complaint of involuntary loss of urine with coitus. The symptom may be further divided into that occurring with penetration and that occurring at orgasm
The complaint that micturition occurs more frequently during waking hours than previously deemed normal by the woman
The complaint of interruption of sleep one or more times because of the need to micturate. Each void is preceded and followed by sleep
The compliant of a sudden, compelling desire to pass urine, which is difficult to defer
Urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of urinary tract infection or other obvious pathology
Bladder diary
Patients should be encouraged to complete a bladder diary in order to evaluate their fluid intake, voiding pattern and episodes of incontinence. In addition, to the number of voids and incontinence episodes, the mean volume voided over a 24-h period can also be calculated, as well as the diurnal and nocturnal volumes. An analysis of bladder diaries may be helpful both in making a diagnosis and also in monitoring progress with treatment.
Investigation in secondary care
Although many women complaining of urinary incontinence may be managed effectively in primary care, on the basis of simple investigations alone, those women who complain of unusual or complex symptoms may benefit from further investigation (Figure 2). In addition, those women whose symptoms fail to improve with primary therapy may also benefit from further investigations to exclude other causes of lower urinary tract symptoms. Assessment in secondary care may involve urodynamic investigation and cystourethroscopy.

Specialized assessment of urinary incontinence (International Consultation on Incontinence Guidelines 2013).
While the diagnosis of urinary incontinence in primary care is subjective and based on symptoms alone, further investigation in the secondary-care setting allows a more objective urodynamic-based diagnosis to be made.
Urodynamic investigation
Urodynamics is the term used to describe lower urinary tract investigations that measure the ability of the bladder to store and expel urine. Urodynamic investigations include uroflowmetry, filling cystometry and pressure/flow voiding studies. Further investigation allows a urodynamic diagnosis to be made and, based on this, further management. In younger women, the most common urodynamic diagnoses are USI, DO and mixed incontinence (USI and DO).
Cystourethroscopy
Although cystoscopy is not helpful in diagnosing the cause of urinary incontinence, it may be employed in order to exclude other causes of lower urinary tract symptoms; for example, a bladder tumor or calculus. Furthermore, cystourethroscopy should be considered in all women who complain of symptoms of hematuria, painful bladder syndrome, as well as recurrent or continuous incontinence.
Pad test
A pad test may be used to document or confirm urinary incontinence, although, it is unable to distinguish between the types of incontinence. The test involves wearing a preweighed incontinence pad, which is weighed before and after use. The difference in weight corresponds to the volume of urine lost. Both short- (1 h) and long-term pad tests (24–48 h) have been described, although reliability has been shown to be greater for the longer-term tests [20].
Quality of life
QoL is assessed by the use of questionnaires completed by the patient alone or as part of the consultation and is useful to assess morbidity caused by urinary incontinence, as well as evaluating treatment efficacy.
Generic questionnaires, such as the Short Form-36 [21], are general measures of QoL and are applicable to a wide range of clinical conditions, while disease-specific questionnaires, such as the Kings Health Questionnaire [2], Urogenital Distress Inventory [22] and the Incontinence Impact Questionnaire [23], are designed to focus on lower urinary tract symptoms. More recently, a series of modular questionnaires for use in lower urinary tract dysfunction have been reported and validated by the International Consultation on Incontinence [24].
Conservative management
The majority of women with urinary incontinence benefit from advice regarding simple lifestyle changes, which they can use to help improve their symptoms. Often patients drink too much and, if they complain of urinary symptoms, they should be told to reduce their fluid intake to between 1 and 1.5 1 per day [25], and to avoid tea, coffee and alcohol. In addition, there is also increasing evidence to suggest that weight loss may improve symptoms of urinary incontinence in those who are overweight [26].
Bladder retraining
Bladder retraining remains important in the conservative management of OAB and has been shown to improve symptoms in up to 80% of women, although, may be associated with a high relapse rate in the longer term [27].
A meta-analysis has demonstrated that retraining the bladder is more effective than placebo and medical therapy; however, at present, there is a deficiency in evidence supporting how effective electrical stimulation is, and there is an insufficient number of studies evaluating the effect of pelvic floor exercises and biofeedback in women who have urinary urge incontinence [28]. Consequently, the International Consultation on Incontinence recommend that bladder retraining should be considered as first-line treatment in all women who have OAB [29].
Pelvic floor muscle training
Pelvic floor muscle training (PFMT) remains fundamental in the management of women with SUI with level 1, grade A evidence from five prospective, randomized controlled trials with short-term cure rates between 35 and 80% [30]. Supervised training is generally felt to be more effective than unsupervised training [31], although benefits of biofeedback and electrical stimulation are less clear [32]. Consequently, the International Consultation on Incontinence recommend that PFMT should be considered as first-line treatment in all women with SUI [29]. In addition, there is no evidence to suggest that age is a factor when determining outcome of PFMT [29].
There is also good evidence to support the use of PFMT for the prevention of urinary incontinence in antenatal and postnatal women in a systematic review of 15 studies including 6181 women[33]. Pregnant women without prior urinary incontinence, who were randomized to antenatal PFMT, were less likely than those who had no PFMT to report urinary incontinence in late pregnancy (relative risk [RR]: 0.44; 95% CI: 0.30–0.65) and immediately postpartum (RR: 0.71; 95% CI: 0.52–0.97). In addition, postnatal women who had received PFMT with persistent urinary incontinence 3 months after delivery, were less likely to report urinary incontinence at 12 months (RR: 0.79; 95% CI 0.70–0.90). Consequently, the evidence would suggest that PFMT in women during pregnancy may be useful in the prevention of incontinence.
Urodynamic stress incontinence
All women who complain of symptoms of stress incontinence, and have a urodynamic diagnosis of USI, will benefit initially from conservative measures including lifestyle advice and pelvic floor exercises. While surgical management remains the definitive form of management in many women, some will also benefit from medical therapy.
Medical management
While, historically, several different drugs have been used anecdotally for the management of stress incontinence, duloxetine, a potent and balanced serotonin (5-hydroxytryptamine) and noradrenaline reuptake inhibitor, is the only drug licensed for this indication and works by improving urethral-striated sphincter activity via a centrally mediated pathway [34]. Duloxetine has been shown to be effective in the management of SUI, and has demonstrated a reduction in incontinence episode frequency and a corresponding improvement in QoL [35], although nausea is a common side effect occurring in 25% of women. Duloxetine has been shown to act synergistically with PFMT [36] and may also be useful in those women considering continence surgery [37].
Surgical management
Many women who complain of symptomatic SUI, and are found to have USI following investigation, will require continence surgery. While retropubic suspension procedures, such as colposuspension [38] and the Marshall–Marchetti–Krantz procedure [39], have been shown to be associated with high cure rates and low complication rates. More recently, the description of the integral theory has led to the development of midurethral tape procedures.
Retropubic midurethral tape procedures
The Tension-Free Vaginal Tape is a retropubic midurethral tape that was first described by Ulmsten in 1996 [40], and is now the most commonly performed continence procedure in the UK. Long-term efficacy data are supported by objective success rates of 90% at 17-year follow-up [41] and the procedure has been shown to be comparable with colposuspension in terms of efficacy at short- [42] and long-term follow-up [43].
Transobturator midurethral tape procedures
The transobturator route for the placement of synthetic midurethral tapes was first described in 2001 [44] and the evidence would suggest there is no difference in terms of efficacy between the ‘inside out’ technique (Tension-Free Vaginal Tape Obturator, Ethicon, NJ, USA) and the ‘outside in’ technique (Monarc®, American Medical Systems, Inc., MN, USA) [45]. In addition, long-term follow-up studies suggest that the procedure is safe and durable [46]. A meta-analysis of five randomized trials comparing Tension-Free Vaginal Tape Obturator with Tension-Free Vaginal Tape and six randomized trials comparing transobturator tape with Tension-Free Vaginal Tape [47], suggests that overall cure rates are similar with the retropubic and transobturator tape procedures. However, bladder injuries (OR: 0.12; 95% CI: 0.05–0.33) and voiding difficulties (OR: 0.55; 95% CI: 0.31–0.98) were less common, whereas groin pain (OR: 8.28; 95% CI: 2.7–25.4) and vaginal erosions (OR: 1.96; 95% CI: 0.87–4.39) were more commonly associated with transobturator approach. These findings are also supported by a further meta-analysis comparing midurethral tapes with retropubic suspensions and pubovaginal sling procedures for SUI [48].
Single-incision midurethral tapes
More recently, single-incision mini slings have been developed as a more minimally invasive approach to managing SUI in the outpatient setting. While there is an increasing evidence base to support their use, at present, there is a paucity of long-term efficacy data. A systematic review and meta-analysis has compared single-incision tapes with midurethral tapes in nine randomized controlled trials in 758 women [49]. Overall, the single-incision tapes were associated with significantly lower patient-reported and objective cure rates (RR: 0.83; 95% CI: 0.70–0.99 and RR: 0.85; 95% CI: 0.74–0.97, respectively), although, there was no difference in QoL improvement. Consequently, while the single-incision mini tapes may offer a minimally invasive alternative to standard midurethral tapes, current evidence would suggest that efficacy may be inferior and further long-term studies are required.
Urethral-bulking agents
Urethral-bulking agents are a minimally invasive surgical procedure for the treatment of USI, and may be useful in the elderly, patients with comorbidities and in women with failed previous continence surgery and intrinsic sphincter deficiency. There are several different agents currently available (Macroplastique®, Uroplasty, MN, USA; Bulkamid®, Contura International A/S, Søborg, Denmark) and, while all tend to have lower efficacy than midurethral tape procedures [50], they may be performed under local anaesthesia in the clinic setting and are associated with lower morbidity.
What is the effect of age on surgical outcome?
There have now been a number of surgical trials evaluating the effect of age on surgical outcome for SUI, although many compare cohorts of elderly women rather than elderly and younger women.
The SISTER trial investigated the effect of age on both perioperative and postoperative outcome with both procedures in 659 women [51]. The older group (mean age: 69.7 years) were compared with a younger group (mean age: 49.4 years). There was a slightly longer return-to-normal activities (50 vs 42 days; p = 0.05) in the older-age group, although, there were no differences in the return-to-normal voiding (14 vs 11 days; p = 0.42). In addition, a positive stress test at follow-up was more commonly reported in the older-age group (OR: 3.7; 95% CI: 1.70–7.97; p = 0.001) and were likely to have less subjective improvement in both stress and urge symptoms, and were more likely to require redo surgery (OR: 3.9; 95% CI: 1.30–11.48).
These findings are supported by a further study investigating the safety and efficacy of Tension-Free Vaginal Tape Obturator in a consecutive series of 97 older women aged over 70 years (mean: 75 years) and 256 younger women (mean: 55 years) [52]. Mean follow-up was 30 ± 17 months and postoperative morbidity was similar in both groups, although, there were significantly more recurrent urinary tract infections in the elderly (13.7 vs 6.2%). Postoperative asymptomatic USI was found more commonly in the elderly group (19 vs 3.7%; p < 0.05), although the rates of overt USI was 5% in both. While the incidence of persistent OAB was similar in both elderly and younger women (68 and 62%, respectively),
Consequently, these data suggests that younger women recover quicker following continence surgery and may also have a higher success rate with lower postoperative morbidity.
What is the effect of subsequent pregnancy following continence surgery?
In general, continence surgery should be deferred until completion of childbearing, and there is a paucity of prospective data investigating the outcome of continence surgery following subsequent childbirth and delivery. A small, retrospective study has assessed the effect of pregnancy following colposuspension in four women, and incontinence recurred in three by the third trimester [53]. All were delivered by cesarean section, and while incontinence persisted in two women for 6 months, all were continent by 12 months.
In addition, evidence from case reports [54] and small series [55] would suggest that women following successful retropubic and trans-obturator tape procedures remain continent following delivery in the short term. Furthermore, a retrospective series of 20 pregnancies following either a retropubic or transobturator tape has been reported. Overall, three (15%) patients had recurrent stress incontinence symptoms during pregnancy and there were no tape-related complications. Ten of the 20 patients delivered vaginally while the remainder were delivered by cesarean section. Recurrence of stress incontinence was seen in 20% of cases following vaginal delivery as compared with 12.5% following cesarean section [56].
Overall, the evidence, although only based on small series, would suggest that the outcome of continence surgery following pregnancy and delivery is mixed, and recurrence rates tend to increase.
Detrusor overactivity
Although many patients will benefit from a conservative approach, initially, drug therapy remains integral when managing women with OAB symptoms and a urodynamic diagnosis of DO.
Medical management
There are many antimuscarinic drugs available on the UK market. Each of these have recently been reviewed by the International Consultation on Incontinence, and all have level 1 evidence and a grade A recommendation [57].
Recently, a systematic review and meta-analysis of 83 studies, which included 30,699 patients and six different drugs (fesoterodine, oxybutynin, propiverine, solifenacin, tolterodine and trospium), has demonstrated the overall efficacy of antimuscarinic medication. The results of this work demonstrated that there was a notably higher return to continence, favoring active treatment over placebo; with the pooled RR across the different studies and drugs being 1.3–3.5 (p < 0.01). In addition, antimuscarinic therapy has been demonstrated to be statistically significantly more effective in reducing the incidence of incontinence episodes, micturitions and urgency episodes per day [58].
Furthermore, a subsequent Cochrane review of 61 trials including 11,956 patients, agreed with these findings and there was a significantly greater cure or improvement rate in the antimuscarinic group when compared with placebo (RR: 1.39; 95% CI: 1.28–1.51). In addition, there was also a significant improvement in QoL suggesting that these findings had clinical significance [59]. Overall, the additional benefit of active treatment was approximately 15% more improved or cured, which translates into a number needed-to-treat of seven.
The available evidence would suggest that extended-release oxybutynin [60] and tolterodine [61] have superior efficacy and tolerability when compared with the immediate-release preparations [62]. In addition, solifenacin has been shown to be noninferior to tolterodine extended-release [63], while fesoterodine has been shown to be superior to tolterodine extended-release [64], although, the incidence of adverse effects has been shown to increase with increasing dose.
More recently, β-adrenoceptor agonists have been shown to be effective in the management of OAB, and mirabegron has been recently been launched in the UK [65]. β3-adrenoceptor agonists induce bladder relaxation by the activation of adenyl cyclase with the subsequent formation of cAMP, and have been shown to increase bladder capacity with no change in micturition pressure and residual urine volumes [66]. β3-adrenoceptor agonists may offer an alternative to antimuscarinic therapy, while at the same time offering a better side-effect profile [67]. In addition, the introduction of a new class of drug may offer the possibility of combination therapy, which may minimize adverse events while maximizing efficacy.
Antimuscarinic therapy may act synergistically with conservative therapy. A Cochrane review of 13 trials including 1770 patients has demonstrated that symptomatic improvement is more common among patients who are on antimuscarinic therapy compared with bladder retraining (RR: 0.73; 95% CI: 0.59–0.90). Furthermore, combination therapy correlated with higher levels of improvement than bladder training alone (RR: 0.55; 95% CI: 0.32–0.93). In addition, a larger improvement was observed with an antimuscarinic therapy/bladder retraining combination compared with antimuscarinic therapy alone (RR: 0.81; 95% CI: 0.61–1.06); however, the difference was not statistically significant [68].
Despite this, tolerability, compliance and persistence have limited the usefulness of many antimuscarinic agents regardless of the introduction of newer bladder-specific agents, long-acting drugs and alternative routes of delivery. A recent retrospective analysis of antimuscarinic prescribing in the UK has shown persistence rates at 12 months to range from 14 to 35%, with little difference noted between the different medications [69].
Botulinum toxin
The use of intravesical botulinum toxin type A (onobotulinum toxin) was first described in the management of patients with neurogenic DO [70], although, there is now considerable evidence to support its usage in patients with idiopathic DO as well.
A randomized, double-blind, placebo-controlled trial of onobotulinum toxin 200 IU, has demonstrated a significantly greater improvement in urgency episodes, incontinence episodes and urinary frequency with onobotulinum toxin compared with placebo. The most common side effects were urinary tract infection in 31% of patients and voiding dysfunction necessitating self-cauterization in 16% of cases [71].
These results are supported by a large Phase III randomized, double-blind, placebo-controlled trial of onobotulinum toxin 100 IU in 557 patients with idiopathic OAB. There was a significantly greater decrease in incontinence episodes with onobotulinum toxin compared with placebo (-2.65 vs −0.87; p < 0.001), and incontinence resolved in 22.9 versus 6.5% of patients, respectively. Once again, urinary tract infection was the most commonly reported adverse event, although the rate of urinary retention was found to be reduced to 5.4% with a lower dose of onobotulinum toxin [72].
The efficacy of onabotulinum toxin 100 IU has also been compared with antimuscarinic therapy (solifenacin 5 mg escalating to 10 mg and trospium chloride 60 mg) in a randomized, double-blind, placebo-controlled trial in 249 women. There was no difference between groups in the mean reduction of urgency incontinence episodes between the antimuscarinic arm and the onobotulinum toxin arm (3.4 vs 3.3; p = 0.81), and resolution of incontinence was reported by 13 and 27% of the women, respectively (p = 0.003). While QoL improved in both groups, the antimuscarinic group had a higher rate of dry mouth (46 vs 31%; p = 0.02), but lower rates of self-catheterization at 2 months (0 vs 5%; p = 0.01) and urinary tract infections (13 vs 33%; p <0.001) [73].
Consequently, onobotulinum toxin may be effective in managing women with refractory OAB symptoms, and may be administered either under general anesthetic with a rigid cystoscope or under local anaesthetic with a flexible cystoscope. While botulinum toxin type A (Botox®, Allergan Ltd, Buckinghamshire, UK) is currently licensed in the UK for the treatment of neurogenic DO, it is not currently licensed for the management of idiopathic OAB.
Neuromodulation
Neuromodulation may also be used in women with refractory symptoms and works by altering the somatic afferent inhibition of sensory processing in the spinal cord [74]. Both peripheral and sacral neuromodulation have been described, and both may be use in patients with OAB that is refractory to drug therapy.
Peripheral neuromodulation
The posterior tibial nerve is a mixed motor and sensory nerve containing L4 to S3 fibers and originates from the same area of the spinal cord as the pudendal nerve to the bladder and pelvic floor. Consequently, peripheral neural modulation may have a role in the management of OAB.
Posterior tibial nerve stimulation is performed by the insertion of a needle in the lower leg posterior to the tibia and two finger widths above the medial malleolus. Treatment is performed weekly in the outpatient setting for the first 12 weeks and then monthly maintenance therapy with each session lasting 30 min.
A randomized trial of posterior tibial nerve stimulation versus sham stimulation has demonstrated improvement in 54.5% in the active arm compared with 20.9% in the sham arm [75], and the evidence would also appear to suggest that posterior tibial nerve stimulation offers a similar improvement in efficacy and QoL as tolterodine treatment [76]. A recent systematic review and meta-analysis has reported a subjective success rate of 61.4% (95% CI: 57.5–71.8) and objective success rate of 60.6% (95% CI: 49.2–74.7), and also demonstrated similar efficacy to antimuscarinic therapy [77]. Consequently, posterior tibial nerve stimulation may offer an alternative to drug therapy in those women with persistent symptoms before considering more invasive procedures.
Sacral neuromodulation
Stimulation of the dorsal sacral nerve root using a permanent implantable device in the S3 sacral foramen was first reported in 1997, and has been used in patients with OAB and neurogenic DO [78]. Prior to implantation, temporary percutaneous nerve evaluation is performed to check for a bladder response and, if successful, a permanent implant is then inserted under general anesthesia.
Sacral neuromodulation has been shown to be an effective treatment for OAB in more than 40 studies. While the reported success rates for subjects varied between 60 and 100%, a recent systematic review revealed success rates between 21 and 48% for one-stage implantation with percutaneous nerve evaluation and 75–80% for two-stage implantation [79].
However, the use of sacral neuromodulation is limited by the high cost of the procedure and high reoperation rates; explanation rates of 21% and a surgical revision rates of 39% have recently been reported [80]. The most common reasons for revision were no response, infection and loss of stimulation.
Consequently, while neuromodulation is an invasive and expensive procedure, it does offer a useful alternative to medical and surgical therapy in patients with severe, intractable OAB prior to considering reconstructive surgery, such as an ileal conduit, clam cystoplasty or detrusor myectomy.
Future research
Currently, there is a lack of age-specific data regarding the management of women with urinary incontinence. Since the incidence of incontinence increases with age, many of the reported studies focused on postmenopausal and elderly women. Consequently, future research should be directed toward tailoring therapy for the younger woman and, in particular, assessing the outcome following surgical procedures. In addition, there is also a paucity of data investigating the outcome of continence surgery following subsequent pregnancy and delivery, and hence, an urgent need to report retrospective studies examining mode of delivery and continence outcome. Greater information regarding management and outcome should improve counseling of younger women complaining of urinary incontinence.
Conclusion
Urinary incontinence is a common condition, which is known to have a significant impact on QoL. While the incidence of incontinence tends to rise with increasing age, a significant number of younger women also complain of troublesome symptoms that require further investigation and management. While many women may be managed effectively based on symptoms in primary care, those with refractory symptoms benefit from further investigation in secondary care allowing a urodynamic diagnosis to be made.
All women who complain of urinary symptoms should be treated primarily with lifestyle changes and conservative measures, including bladder retraining and pelvic floor exercises. Those with a diagnosis of USI may find duloxetine useful in addition to pelvic floor muscle training, although, many will benefit from continence surgery. Medical therapy remains integral in the management of women with symptoms of OAB and a urodynamic diagnosis of DO, while botulinum toxin or neuromodulation may be effective in those with refractory symptoms.
Future perspective
With an increasingly aging population, urinary incontinence will continue to have a major impact on the provision of healthcare both in the community and in secondary care. While, historically, many women have regarded urinary symptoms to be common following childbirth and part of the natural aging process, significant advances in the field of urogynecology and urology have altered the perceptions of clinicians and patients.
Primary prevention of urinary incontinence, and patient education, will continue to be important, and there is now good evidence to show that weight loss and lifestyle modifications play a significant role in the management of urinary incontinence.
Antimuscarinic therapy will continue to have a major role in managing the symptoms of OAB and the newer long-acting bladder-specific agents should improve tolerability and compliance. In addition, alternative routes of delivery may help to reduce troublesome antimuscarinic side effects. The introduction of the new β3 agonist, mirabegron, represents the first new class of drug for OAB for over 30 years and offers an alternative to antimuscarinic drugs for those women with lack of efficacy or intolerable adverse effects. Furthermore, another β3 agonist, solabegron, is currently in Phase II clinical trials and may be available in the near future. New drugs with alternative mechanisms of action also remain under investigation, including vitamin D analogs [81], and also drugs, such as neurokinin antagonists [82], which act on the sensory pathways, are thought to be important in the pathophysiology of OAB. Botulinum toxin will continue to have an increasingly important role and is currently licensed for the management of neurogenic DO in the UK, and is soon to be licensed for the management of idiopathic OAB. In addition, neuromodulation will continue to offer an alternative to reconstructive surgery, and both cutaneous [83] and implantable peripheral neuromodulation devices [84] are under investigation as alternatives to sacral neuromodulation.
SUI also remains a significant cause of morbidity, although, medical therapy has not had a major impact in management. Consequently, many women ultimately will benefit from surgery and midurethral tapes will continue to have a significant role in surgical management, despite some concerns regarding long-term complications [85]. Minimally invasive surgery offers considerable benefits in terms of patient experience and morbidity, and single-incision slings remain under development. In addition, the use of autologous stem cells may also prove to be useful as an alternative to midurethral sling procedures and bulking agents.
Executive summary
Urinary incontinence is a common and distressing condition that has a significant impact on quality of life.
The incidence of urinary incontinence increases with age.
Stress incontinence may be a symptom (stress urinary incontinence), a sign demonstrable on examination or a diagnosis following urodynamics (urodynamic stress incontinence).
An overactive bladder is a symptomatic diagnosis, while detrusor overactivity is a urodynamic diagnosis. The terms, although often used interchangeably, are not synonymous.
Basic investigations in primary care include urinalysis to exclude infection and a postvoid residual.
Women with refractory or unusual symptoms should be referred to secondary care for further investigation, including urodynamic investigations.
All women benefit from lifestyle advice and bladder retraining.
Women with stress urinary incontinence should be offered pelvic floor muscle training in the first instance, although many will benefit from continence surgery.
Midurethral tapes (retropubic and transobturator) are the most commonly used procedures and have comparable efficacy.
Drug therapy remains integral in the management of an overactive bladder and, currently, antimuscarinic agents are the most commonly prescribed agents.
Botulinum toxin and neuromodulation may be useful in patients with refractory overactive bladder symptoms and a urodynamic diagnosis of detrusor overactivity.
Footnotes
Urinary incontinence in the young woman: treatment plans and options available
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 75% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider, CME@medscape.net. For technical assistance, contact CME@webmd.net. American Medical Association's Physician's Recognition Award (AMA PRA) credits are accepted in the US as evidence of participation in CME activities. For further information on this award, please refer to http://www.ama-assn.org/ama/pub/category/2922.html. The AMA has determined that physicians not licensed in the US who participate in this CME activity are eligible for