
Abstract
Background:
Violence against women (VAW) is a pervasive public health problem in Canada with detrimental impacts on the mental health of survivors. The COVID-19 pandemic led to an increase in the incidence and severity of VAW, deterioration in population level mental health and well-being, and exacerbated barriers to accessing health and social services. People who were already vulnerable to mental illness or people experiencing marginalization across social factors experienced even greater challenges with their mental health.
Objectives:
We aimed to understand the mental health of VAW survivors accessing services during the pandemic and how experiences differed across diverse life histories and sociodemographic factors.
Design:
We conducted interviews from April to September 2021, with 10 adult women who had accessed at least one VAW service in the Greater Toronto Area since March 11, 2020. These data were collected as part of a community-based study on the processes, experiences, and outcomes of adapting VAW programming during the COVID-19 pandemic. Participants were sampled through staff contacts at VAW organizations to represent a diverse cross-section of sociodemographic factors and types of services accessed.
Methods:
We used narrative thematic analysis to analyze our interview data and identified how life histories and sociodemographic factors intersected with themes about their mental health.
Results:
The research team identified four narrative themes pertaining to survivor mental health: (1) new and exacerbated anxiety, depression, and substance use, (2) feelings of hopelessness and mental exhaustion, (3) shame and low self-esteem, and (4) resiliency. Survivor’s experiences across these themes differed based on personal factors and life histories (e.g. being a newcomer, being a mother, experiences of childhood trauma and abuse, living with a disability, and socioeconomic status).
Conclusion:
During the pandemic, survivors experienced greater mental health needs and at the same time encountered greater challenges in accessing support, which had significant consequences for their mental well-being. Services that support VAW survivors (as essential services) require increased funding and resources to offer effective, accessible, and timely support that improves the lives of survivors. This support must consider survivors’ unique needs based on personal factors and life histories during and beyond public health emergencies.
Background
Violence against women (VAW) is a pervasive public health problem in Canada; 44% of women over the age of 15 have experienced intimate partner violence, the most common form of VAW, in their lifetime 1 and in Ontario, over 90 municipalities have declared intimate partner violence an epidemic. 2 VAW has persistent and detrimental mental health outcomes for survivors,3 –8 including depression, anxiety, post-traumatic stress disorder, substance use, suicide, self-harm, and sleep disorders.8 –12
Across Canada, the COVID-19 pandemic led to both an increase in the incidence and severity of VAW13,14 and a deterioration in population level mental health and well-being. 15 People who were already vulnerable to mental illness or people experiencing marginalization across social factors (e.g. ethnicity, sexuality, gender, disability, or socioeconomic status) faced more significant mental health challenges.7,15 As a result, the pandemic exacerbated the already pervasive mental health concerns faced by VAW survivors. 16 A critical feminist lens is useful for considering how individual and community factors interact with patriarchal systems and power dynamics to explain the relationship of mental health and VAW during public health emergencies. 17 It further allows us to consider the intersecting nature of social support, help-seeking processes, economic independence, cultural norms, and stigma, as described within existing theoretical literature on VAW. 17
VAW organizations offer critical support and services to survivors and respond to both the acute and long-term needs of women experiencing violence, including survivor mental health. Globally, during the pandemic, public health mandates, often made without consideration of the needs of VAW survivors, including lockdowns, quarantine, and social distancing created barriers to both VAW service access18 –23 and delivery.24 –26 For Canadian VAW organizations this often entailed significantly reducing or canceling services due to staffing shortages or an inability to meet pandemic protocols;24 –26 many organizations also switched in-person services to virtual or telephone formats.24,26,27 Canadian VAW organizations that remained open during the pandemic, primarily residential services, had to continually implement infection prevention and control measures for both staff and clients These unprecedented changes placed strain on VAW organizations and their staff, many of whom were already operating at capacity, and were often done in the absence of guidance from the provincial or federal government.24,27,28
In a previous analysis, we demonstrated how changes in work environments due to the COVID-19 pandemic in Canada impacted the mental health of staff working at VAW organizations. 29 We found that staff at VAW organizations faced heightened levels of vicarious trauma and distress, burnout, as well as feelings of hopelessness and despair in meeting client needs. 29 In this analysis, we aimed to understand how the mental health of survivors accessing VAW services during the COVID-19 pandemic and how contextual factors in survivors’ lives influenced survivor experiences.
In Canada, two studies have specifically explored the experiences of women accessing VAW services during the pandemic from the perspectives of survivors. One quantitative study, a survey in Ontario of 49 VAW survivor respondents, found that over half of women reported poorer well-being and reduced access to healthcare and informal supports. 30 The second study qualitatively analyzed interviews with 26 staff from women’s shelters, 8 women (all who identified as Caucasian) accessing shelters, and 10 focus groups with VAW service leaders in Ontario.25,31,32 One analysis from this study found that inconsistency and lack of clarity in pandemic rules and how they were communicated acted as a significant source of stress for survivors, and that quarantine requirements and rules that isolated survivors in shelters posed additional harm to survivor mental health. 25 Another analysis from this study found that mothers living in residential shelters took on sole parenting responsibilities in the context of shelter and pandemic protocols, and isolation requirements increased stress for these mothers as they restricted families to smaller spaces. 31 A third Canadian study interviewed 17 management and frontline staff of VAW organizations across Canada and described the impacts of COVID-19 on intimate partner and sexual violence survivors from the perspective of service providers. 33 This study found that the pandemic made it even more difficult for survivors to seek support than before, both by exacerbating pre-pandemic challenges such as isolation and by introducing new obstacles such as switching to virtual services or travel bans.33,34
These existing studies31,33,34 provide an overview of the challenges survivors faced in accessing services during the pandemic. This article is a dedicated analysis of the mental health of survivors living in Toronto, Canada’s largest city, accessing VAW services. We build upon literature in this field to explore the following research question: How did VAW survivors accessing services in Toronto during the pandemic describe their mental health, and how did survivor experiences differ across diverse life histories and sociodemographic factors? We offer a unique analysis of rich and in-depth qualitative data from a diverse sample of survivors, and a discussion of how survivors experiences differed across types of services accessed, sociodemographics, and life histories.
In 2022, the Canadian federal government committed CAD $601.3 million over 5 years to a National Action Plan (NAP) to End Gender-Based violence and in 2023 released a set five pillars of “opportunities for action” for provinces and territories to consider. While these pillars explicitly state how critical it is for survivors to access well-resourced supports, none of the pillars specifically mention survivor mental health. With an influx in sustained funding and investment into VAW prevention and response, it is crucial to inform the direction and use of these funds with nuanced and contextualized evidence. Doing so can inform how VAW organizations can support survivor mental health emerging from the COVID-19 pandemic and how policymakers in public health consider the mental needs of VAW survivors during subsequent public health emergencies.
Method
The data analyzed in this article were collected as part of a community-based, mixed-methods study on the processes, experiences, and outcomes of adapting VAW programming during the COVID-19 pandemic, in collaboration with 42 VAW organizations across the Greater Toronto Area (the MARCO-VAW Study). 24 We received ethical approval from the Unity Health Toronto Research Ethics Board (REB #20-124) and the Dalhousie University REB (#2022-6275). The reporting of this study conforms to the COnsolidated criteria for REporting Qualitative research (COREQ) statement which can be found in the Supplementary Material. 35
Participants
Survivor participants were recruited through staff at VAW organizations and intentionally represented a diverse cross section of sociodemographic factors and types of services accessed. Survivors were eligible to participate in interviews if they had used at least one service for women experiencing violence or abuse at an organization in the Toronto Region since March 11, 2020, were at least 18 years old, and were able to provide informed consent. Table 1 summarizes the characteristics of the interview sample and Table 2 offers a narrative overview of participant life histories and how they experienced service access during the pandemic. Prior to the interviews, participants provided informed consent via e-mail. The research team conducted safety checks to ensure that survivors were in a physically and mentally safe space to participate throughout the interview process.
Participant demographics.

N: number; M: mean score; IQR: interquartile range (i.e. the 25th and 75th percentile).
Gender diverse includes any participant who reported the following gender identities: (a) fluid, nonbinary, gender queer, or agender, (b) Indigenous or other cultural identity (e.g. two-spirit), (c) transman, or (d) transwoman.
Narrative description of participants.

ODSP: Ontario Disability Support Program.
Data collection
We conducted semi-structured interviews ranging from 1.5 to 3 h in length with adult women (n = 10) who had accessed at least one VAW service in the Greater Toronto Area since March 11, 2020. We aimed to collect rich, high quality interview data, where we were responsive to each participant’s developing narrative and recollections and prioritized participant agency and autonomy, rather than strictly following a predetermined guide.36,37 Interviews were conducted from April to September 2021. The interviews were conducted by ARY, an academic VAW researcher and PS, a community-based VAW researcher, and three peer researchers (women with lived experiences of gender-based violence).
The interview guide is available online 38 and was comprised of five main sections: (1) about you; (2) impact of the pandemic (with specific questions about mental health and well-being); (3) experiences of violence; (4) service access and outcomes; and (5) contextual factors. See Table 3 for a summary of the interview guide. As the interviews were semi-structured, not all questions in the guide were answered in all interviews or in the same order. Further some questions asked in interviews were not on the interview guide. Participant interview responses were narrative in nature and often delved into participants’ life histories to contextualize their experiences during the pandemic. At the end of the interview, participants completed demographic questions. Interviews were conducted with an interpreter when participants were not comfortable speaking in English (n = 3). Following interviews, participants were provided with a list of free VAW mental health resources (developed in collaboration with our VAW partner organizations and our advisory group) that they could contact after the interview and a $40 honorarium. Interviews were conducted and recorded using Zoom (Zoom Video Communications, Inc., San Jose, CA, USA) and transcribed using Trint (Trint Ltd., Toronto, ON, Canada). BS and AY each de-identified and checked the accuracy of all the transcripts compared to the original recordings.
Summary of interview guide.

Data analysis
We used narrative thematic analysis36,39,40 to explore the following research question: How did VAW survivors accessing services in Toronto during the pandemic describe their mental health, and how did survivor experiences differ across diverse life histories and sociodemographic factors? Narrative interview approaches have been found to be empowering for survivors; they give autonomy, space, and time for survivors to discuss and process stigmatized and complex experiences of trauma. 41 Narrative analysis allows researchers to explore not just “what” participants share but to also consider how they tell their stories and to holistically consider participants’ interviews in relation to intersecting social identities. Our participant interviews were rich, complex, and storied and provided crucial context for understanding survivor experiences with VAW service access and delivery. We considered participants transcripts in their entirety in our analysis, instead of just focusing on their answers to specific questions on mental health and well-being. A holistic understanding of participants’ lives and experiences leading up to and during the pandemic, including their experiences accessing VAW services leading up to and during the pandemic, allowed us to conduct a more fulsome analysis of the intersections between mental health, VAW service access, and social circumstances. We applied a critical feminist lens 42 and social justice framework 43 to our analysis, identifying interconnected patterns of disadvantage caused by structural inequities, that systematically marginalize women at the intersection of different social identities. 44
We followed pre-specified stages of narrative thematic analysis.39,40 Four researchers collaborated on data analysis, three of whom were also interviewers with lived experience of violence. First, we thoroughly read and re-read the transcripts multiple times to familiarize ourselves with the data. We then independently coded the same two interview transcripts and met to compare and discuss the initial codes we identified and collaboratively designed an approach for coding the rest of the data. Each analyst was then assigned a subset of the dataset for coding. We met regularly (for ~1.5 h, every 2 weeks) over the course of a 4-month period to discuss and refine our coding process. Finally, each transcript was double-coded, and we continued to meet as a team to discuss adding, combining, removing, and refining codes. All coding was done using Dedoose (SocioCultural Research Consultants, Los Angeles, CA, USA).
For this analysis on survivor mental health, our team analyzed the coded data, specifically looking for how participants described their mental health and then how their mental health intersected with their detailed narratives of accessing VAW services during the pandemic. B.S. and A.R.Y. then thoroughly re-read each participant interview, taking notes on what the contextual components, patterns of disadvantage, sociodemographic factors, and life histories shared throughout their interviews revealed about their mental health. We co-constructed narrative descriptions for participant that were reviewed by the interview and analysis team (see Table 2). Finally, we generated themes based on the most persistent and salient narratives regarding mental health and worked together to interpret the implications and the meaning of the data using participant narrative descriptions. The outcome of this process is visualized in Figure 1.
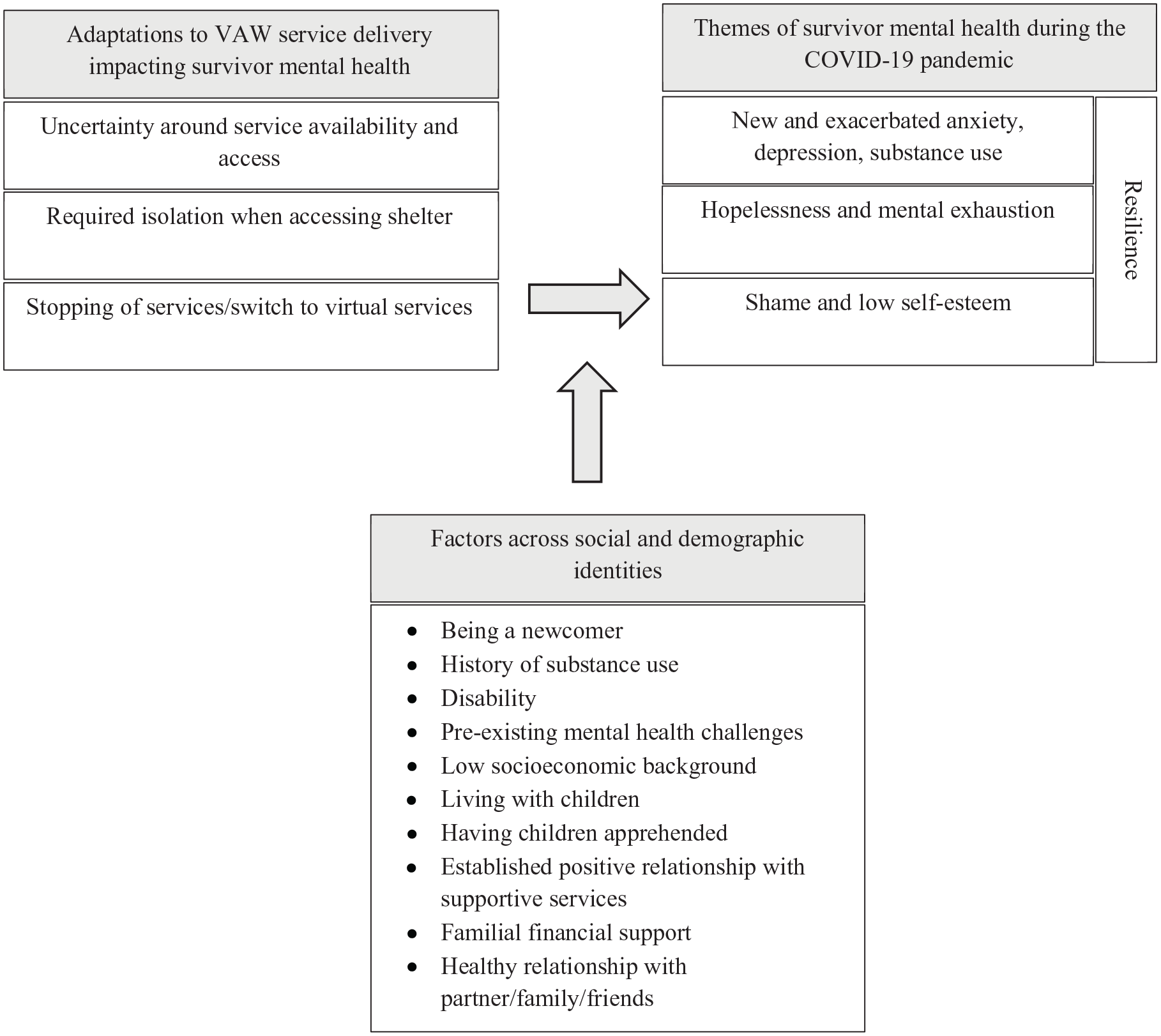
Framework for understanding narratives of mental health as shared by VAW survivors accessing services during the COVID-19 pandemic.
Positionality
The authorship team is comprised of a group of women researchers from different institutions, at different career levels, ranging from students to full professors, as well as community partners from regional VAW networks. We each hold diverse personal identities and social locations across ethno-racial identity, age, caregiver status, and lived experiences of violence. All authors identify as women and are Canadian. We are cognizant that VAW is a stigmatized topic and that research on VAW has the potential to replicate, rather than expose and challenge stigmas. We are also aware and embrace that our presence as researchers and the interactions between the interview team and participants shaped the way the data and our analyzes has been constructed. 45
We, informed by a critical feminist lens, employed narrative methods that intended to empower survivors to take control of their depiction of their lived experiences, which like all lived experiences are filled with the complexities and contradictions of real lives. In listening to, familiarizing ourselves with, and generating themes from participant narratives, we made a specific effort to not describe a uniform survivor experience, prioritize participant agency through a holistic consideration of each interview and its interconnected parts, and diminish, as much as possible, the power imbalance between researchers and participants.46,47
Findings
We identified the following four narrative themes in the data: (1) new and exacerbated anxiety, depression, and substance use, (2) feelings of hopelessness and mental exhaustion, (3) shame and low self-esteem, and (4) resilience. Importantly, while these four themes are used to bring order to the complexity of our data, they are not mutually exclusive, with participants’ stories and experiences often sitting across multiple themes. Figure 1 provides a framework for incorporating the components of the analysis including participant experiences accessing services, their life histories and sociodemographic factors, and narratives around survivor mental health.
New and exacerbated anxiety, depression, and substance use
A recurring narrative across our dataset was that anxiety, depression, and increased substance use was brought on, or exacerbated, during the pandemic. This was true for participants accessing both non-residential services and residential services.
For some participants, anxiety, depression, and substance use was triggered when programs and supports they were accessing regularly stopped or switched to online. The increased isolation and lack of social interaction that came along with no longer being able to rely on services in combination with other pandemic restrictions took a toll on their mental health. We identified that this was particularly salient for women living alone (e.g. C72 and C81), women living with a disability (e.g. C76), and women with a history of substance use or other mental health conditions (e.g. C72, C75, and C76).
C76, a single woman who lived alone, was unemployed, and received disability payments due to health issues, shared her challenges with not being able to access in-person support services during the pandemic. She described how for years she used to access an in-person service two times a week. The benefits of the service itself were helpful, but she detailed how valuable it was for her self-esteem to get out of her house to walk there and have social interaction. When the service switched to virtual, she described suffering physically and mentally.
“but anyway, so when it shut down, it was all virtual, which was really no good for me because the loss of social aspect of everything. Right. [. . .] I really like going there, not only walk there and you see the trees and all that kind of stuff, then you go there, you socialize a bit, you feel good about yourself, like you’ve accomplished something in a day and not just slept all day, you know, but now that’s not an option. And I’m just finding that the reason why I brought that up is because basically that sums up about how I feel about everything right now. I miss all of those type of services [. . .]Those programs make a big difference, physically, mentally, everything.” [C76]
In her interview, C76 noted that she had been accessing VAW related services for over 10 years and that she had a history of problematic substance use that she proudly overcame. However, during the pandemic she described how she “got addicted” again. For C76, accessing VAW services was the only time she left her house during the day, and it was a crucial part of her strategy for staying mentally healthy.
Similarly, C75, described going through “crazy major depression” during the pandemic where she would not eat or move for days. C75 disclosed that she has a history of substance use problems in addition to anxiety and depression. C75, has three young children, but none of them were in her care. During the pandemic, the visitations she was having with her children essentially stopped and she was not able to access the services she previously relied on. These factors combined with persistent isolation, made it a very challenging time for her. However, C75 credited her supportive partner, who lived with her, as life-saving in helping her to get through her lowest times during the pandemic. Social supports stemming from healthy relationships with partners, family members, and friends proved to be essential in preventing serious mental health crises among survivors in our dataset, especially when services they were relying on stopped.
Delays in legal systems for survivors also brought on new and heightened levels of anxiety for survivors. For example, C79, a newcomer to Canada and a mother who recently left her abusive partner, struggled to navigate the justice system, virtually. C79 had support of a community-specific organization as well with financial support from her parents, but the extensive waiting for a decision on ex-partner’s criminal trial was taxing on her mental health.
“Sometimes I cannot sleep because of the criminal record situation it’s going really slow. I didn’t get the results yet so I have to think about it and I can I get stressed a lot about that. [. . .] Actually, it took a really long time to process my husband’s criminal court, so if I didn’t get a result from the criminal court, then I cannot get any result for my custody fighting. So I get some pressure about that. It’s such a long time. [. . .] So just I’m anxious about that.” [C79]
For other participants, anxiety and depression was brought on by forced isolation while living in shelter (e.g. C73, C77, and C78). Infection prevention and control policies for staff and clients contributed to feelings of isolation among survivors. C77, a single mother of a 2.5 years old and a recent newcomer to Canada, with no family or support systems in Canada, found living in shelter to be confining and restrictive and even shared how it led other women at the shelter to run away due to the unbearably isolating conditions.
“For one year in the shelters, we were all the time in the little room. We can’t go out because of Covid in the little room that was our own world. No TV, no entertainment, no going out. [. . .] Everybody was like, nobody was happy there. So many ladies left within two or three days, they just ran away.” [C77]
C77 experienced regular anxiety and panic attacks when she was living in shelter. She received medication from her healthcare provider to help her manage the symptoms, but this medication made her tired and she ended up not being able to take it out of the necessity of being alert to take care of her child.
“. . .then my doctor called me, my nurse practitioner, she asked me to get the tablets, like, for a daily for 15 days or something. So because if I take the tablet Lorazepam after that, I feel sleepy. So how can I take care of my child? So nobody is there to take care of my child. And so, like, I was taking only when I was feeling like oh something will happen to me, then I take tablets, but daily I was not taking so I talked to my doctor that I can’t take tablets because I feel sleepy and I need to wake up at night for three or four times to soothe my baby and to give her milk so I can’t sleep. So she said, okay, you for 15 days you take it. But after that leave it. But I didn’t take those tablets for 15 days.” [C77]
The cessation of programming for children and childcare at the shelter C77 was staying at during the pandemic made it impossible for her to find reprieve and to take her medication. As a result, C77 was isolated alone with her daughter in a room everyday while experiencing anxiety attacks.
We identified that newcomers (like C77) faced unique and additional challenges. Some newcomers did not have any family or social supports to help navigate systems and offer reprieve for childcare. But for C79, who had financial support from her family, living in shelter was temporary and mostly positive, in part because she was able to quicky secure safe and comfortable housing for her child. Further mothers, like C77 (e.g. C73 and C78) also faced unique challenges with isolation in shelter, often needing to stay in the same room with their children with no break and no programming for their children which was detrimental for their mental health.
Feelings of hopelessness and mental exhaustion
Survivors of VAW accessing services during the pandemic consistently reported feelings of hopelessness and mental exhaustion in trying to access support, determine what services were open and had space, and waiting long periods of time to access supportive services. For example, C74, a mother of a young daughter living in an unsafe situation, described how she tirelessly tried to access a VAW shelter during the pandemic as she feared for her own and her daughter’s life. C74, skilled at navigating social and legal systems from years of experience, described being unable to find a shelter that was open and had space for her and her daughter. Despite constantly calling shelters across the Greater Toronto Area to check availability she kept being told that there was no space for her, forcing her to stay in an extremely unsafe living environment for months.
This intensive dedication to searching for support and inability to escape a dangerous home was mentally exhausting and ended up taking most of time. In addition to the challenges faced in accessing shelter during the pandemic, C74 had further challenges in accessing other wrap around services she needed to support her and her daughter. As a result, C74 described needing to stop a career development course for women she was enrolled in to fully dedicate herself to finding and accessing supports to improve the safety of her family, at the expense of her own mental well-being.
“So they were I was put on pause. I’m still in the course. But it meant that we were so busy dealing with these very credible threats and trying to navigate the legal system and legal aid and food that constantly was changing with each wave of [the pandemic] and school. Right. And my daughter’s mental health and accessing resources and calling and calling and calling. [. . .]And then people just not showing up and just all of these things, you just have to go through it, that it was something that. I was not able to continue because just feeding us and keeping us safe was all I could do each day. It was, it’s been the lowest of the low.” [C74]
For C74 trying to access and navigate services and support became their full-time job. A sentiment that was echoed by other participants across the dataset. For example, C75 described the all-consuming process of trying to find safe and suitable housing for over a year and the discrimination she faced when trying to secure housing while accessing the Ontario Disability Support Program (ODSP), a provincial income support program for people living with a disability.
“But I mean, I’ve been doing this for over a year now and I’m just like I mentally and physically exhausted, but I’m determined to move out of here. So I’m going to keep trying until I find something. I mean, determination got me here. So, I mean, [laughs] I figure that there has to be something out there for me, but I just keep getting declined like nobody wants to touch me. It’s almost like I’m toxic.” [C75]
Survivors who were newcomers to Canada (e.g. C78, C79, and C81) also faced barriers to and delays in accessing services which often led to them feeling hopeless in getting the support that they needed. For example, C81, a self-identified undocumented newcomer to Canada, living alone, described experiencing years of violence from her partner. During the pandemic, when the abuse intensified, she ultimately decided to seek support. However, when she reached out for support from a culturally specific organization, she did not hear anything back. When she finally got in touch with the organization, they told her everything was closed because of the holidays and waitlists and that there was “nothing they could do” for her.
After waiting for over a year, C81 reflected: “So I’m still waiting for them or for someone to call me. I have the idea that here in Canada, women are protected and that there is protection for women. But I realize that that’s not the case. That’s not true.” C81 described that not being able to access services combined with losing her ability to visit with friends and family due to pandemic restrictions and her fear of contracting the virus, made her feel like she would never be able to get help or improve her situation.
Newcomers to Canada, like C81, faced exacerbated challenges in navigating service access due to language and cultural barriers, a lack of familiarity with Canadian systems structures, and at times precarious immigration status which precludes them from certain supports. In comparison, survivors who were well connected with services prior to the pandemic, sometimes had a more support accessing and benefiting from continued support, mitigating some of the mental exhaustion stemming from trying to find help. For example, C72 and C73 had longstanding and positive relationships with counsellors who were able to be consistent and reliable sources of support during the pandemic, alleviating some of the exhaustion stemming from navigating systems.
Shame and low self-esteem
We identified feelings of shame and low-self-esteem to be a salient narrative theme across our dataset, especially among mothers and newcomers to Canada.
For survivors living with children (and especially those living in shelter with children), the lack of privacy and space needed to talk to counsellors or support staff due to VAW services being delivered remotely and schools and other forms of childcare being closed impacted their self-worth. For example, C73, a single mother of two daughters with autism, living in one room together in a VAW shelter, without programming for her children, meant that her children were exposed to her processing and dealing with her abuse. She described feeling like a failure and hating herself for how she had to keep her children and herself isolated.
“Same room all the time, like I couldn’t get away from it. So my kids heard everything. I hated myself for that because I didn’t want my kids to hear everything. My kids saw me crying every day. I hated that, but I didn’t have that alone time or I’m couldn’t just put them in day care.” [C73]
Furthermore, C74, living in a basement apartment with her daughter, also felt regret over what her daughter had to overhear when she was discussing her situation with support services and processing her trauma. C74 shared that her daughter’s mental health suffered as a result reinforcing C74’s shame that she was not able to provide a better situation for her daughter.
While virtual service delivery for C73 and C74 exacerbated feelings of shame and low self-esteem, in some cases the switch to virtual service delivery worked to reduce these feelings. For example, for C80, a mother and newcomer to Canada, being able to access services virtually allowed her to share her story more comfortably during a time when she felt vulnerability and shame. This fear was compounded by feelings of cultural shame she harbored about her community finding out about what she experienced. At the time of accessing this support, C80 was really having “a hard time mentally,” but she valued interacting virtually with this organization. By not showing her face, she shared how she was able to provide more crucial details about her experiences to help staff determine what supports would be needed.
“Actually, I thought to telephone service was the most comfortable way to me, because if I want to show my face, it was really uncomfortable and it was just a shame to me. And then if I get a service through a telephone, I can cover my face so I could open one hundred percent of my story if I have to open my face I was really ashamed about what happened to me I couldn’t tell exactly what happened.” [C80]
After months of working with a supportive staff at the organization virtually, C80 eventually needed to go in person to the organization to meet with a staff at the organization who had yet to see her face and found it very comfortable as the staff sharing “she gave me courage to show my face in public.”
“I never show my face to her, but she was really nice and make me comfortable. And then when I met her, it was also very comfortable that she gave me courage to show my face in public.” [C80]
Juxtaposing the experiences of C80 with C73 and C74 sheds light on the importance of contextualized supports for survivors based on survivor life histories. For C73 and C74, changes to service delivery during the pandemic brought on feelings of shame and self-hatred, but for C80 being able to access service virtually (due to adaptations made during the pandemic) helped to mitigate her feelings of shame and embarrassment.
Like C80, feelings of shame and low self-esteem were salient among newcomers, who discussed that they were embarrassed about the abuse they experienced (e.g. C79 and C81). These feelings were further perpetuated when newcomers were mothers and struggling to access support. C78 described feeling like a “loser” because it was taking her a long time to complete her permanent residency application.
Like the thing with the baby, that they have to deal with the baby all the time. I have telling them like it’s very hard for me to work on my immigration case. Like, it’s very hard. I mean, I feel bad because you have it took me like two months for now, like and I feel like I am a loser, you know, like, what the heck. [C78]
C78, like other mothers accessing shelter in the dataset, had her baby with her at all times. Trying to complete a complex task with no childcare, in a new language, and with little support from services would be daunting for anyone, yet C78 felt like she should be doing more or better. This narrative was common among survivors in our dataset, who in the face of extreme adversity, demonstrated resilience and persistence, compassion, and self-reflection, and at the same time were plagued with shame, self-criticism, and self-hatred.
Resilience
A cross-cutting narrative theme we identified across all survivor transcripts in our dataset was resilience. As demonstrated in the above three themes, the pandemic proved to be particularly a challenging time for survivors accessing services. We found that participants showed remarkable perspective and strength when facing significant adversity, persistently navigating complex and at times hard to access social and VAW services, and coping with serious mental health and substance use challenges. In this section, we identify three additional ways that participants showed resilience through committing to support other VAW survivors, modeling positive thinking and a healthy lifestyle for their children, and expressing gratitude for the support they were receiving.
C72 shared how despite having a difficult experience in shelter, she carried out clothing and toy drives for the shelter she stayed at during the pandemic. Furthermore, some participants described taking courses or going back to school to be able to find better jobs and gain financial freedom and support other survivors of violence, while also contending with significant mental health challenges (e.g. C73, C74, C75, and C77). For example, C73 described how she wanted to go back to school to get training to work in a shelter as she found her passion through helping others who went through similar things to her:
“Yeah, I have depression. I have anxiety. But I’m still standing, I am still here, and I just want another person to hear that out and understand to just still be there and still stand up and still be strong. I know those hard days, but just keep going. And that’s my passion. And that’s what I really want to do. Like, I want to actually go back to school to go and work in a shelter because I want to give back as much as I can. But like, I know everything about a shelter. I grew up in a shelter, so why not do it type of thing. Right.” [C73]
C73 also described how she wanted to stay strong for her children to ensure that they did not have to experience the same things she did when she was growing up. This was similar for other women across the dataset who had children. In the previous themes, we identified that having children added complexities in navigating and leaving abusive situations and accessing VAW services during the pandemic, and yet we also identified that children were often the impetus for staying resilient during devastating times. For example, C80 described modeling healthy behavior and positive thinking to support her son who was struggling with his mental health.
“So even if I cannot I sleep well at night, I am exercising hard and then I try to think positively and then I have to do my best. And I told I told my son, also, don’t try too much if you cannot control the situation. So you do your best what you have to do in your situation. And then I ask him to have more exercise and morning and evening twice a day, I told them your physical health can lead to your mental health. So we always try to think positively and healthy.” [C80]
C80, like C74, demonstrated resilience in the face of challenging times to try to provide a stable and supportive environment for their children.
Embedded within survivors’ resilience was the gratitude they exuded when telling their stories. Survivors consistently shared how helpful the services and support they were receiving was and how thankful they were to be receiving support, often a testament to the resilience, compassion, and dedication embedded within the VAW sector. For some participants who were newcomers to Canada, this feeling of gratitude was exemplified when reflecting on the support they might have received in the country they lived in before coming to Canada. For example, C78 shared:
“So I have thought, like, you can always improve. Right? You can always do better. And I think that I have, I’m very, I’m very thankful to be here because sometimes I feel like I don’t deserve it right. Because I have this in my mind, like I’m not Canadian. What I’m doing here, they are helping for free right, like I think that I am in debt with them. So I’m very thankful to be here just to have a room with my baby, to have food in the fridge. Right. So I don’t want to ask for more, you know. I, I just don’t want to ask for more, and so I just feel like I have, I’m OK [laughs].” [C78]
The gratitude C78 felt to be receiving and accessing services in Canada encouraged her to want to improve her circumstances sharing, “I want to try even if I fail.” However, the gratitude she felt bordered on not feeling deserving or worthy of supports, which was a narrative we identified in other survivor interviews and points the independence and autonomy survivors desire but also is reflective of structural and societal norms that undermine and devalue the importance of women’s well-being.
In addition to the examples shared in this theme, resilience was a thread running through all the themes in this analysis and is represented by the persistence, positivity, and reflexivity survivors shared in pursuit of trying to improve their circumstances under, at times, insurmountable obstacles, and while living with significant mental health challenges.
Discussion
We aimed to understand how VAW survivors accessing services during the pandemic described their mental health and how survivor experiences differed across diverse life histories and sociodemographic factors. It has been well established that VAW profoundly affects mental health, leading to an increased risk of depression, anxiety, post-traumatic stress disorder, and suicidal ideation among survivors. 8 We found that the COVID-19 pandemic and the resulting restrictions placed on VAW service access and delivery had the potential to place additional strain on the mental health concerns of survivors. We identified four narrative themes in the data: (1) new and exacerbated anxiety, depression, and substance use, (2) feelings of hopelessness and mental exhaustion, (3) shame and low self-esteem, and (4) resilience. Our study offers a nuanced understanding of the mental health of a group of VAW survivors accessing services in Canada’s largest city during the pandemic and how their experiences differed across diverse life histories and sociodemographic factors.
First, we identified that participants described experiencing new and exacerbated anxiety, depression, and substance use. This finding was consistent with what was found in other Canadian studies on the impact of the pandemic on VAW service delivery.25,30 For many, the social interaction and physical activity associated with attending these services were critical to their mental well-being. The switch to virtual services, while beneficial for some (as we discuss in theme 3), failed to meet the needs of others who relied heavily on face-to-face interactions for social support.
Being a survivor of VAW can be incredibly isolating even during non-pandemic times.48,49 Survivors may withdraw from social networks due to feelings of shame and embarrassment, and restricting or controlling behaviors from abusive partners may prevent women experiencing violence from engaging with their family and friends.48,50 Survivors’ lives then became exceptionally challenging, and when formal supports become less accessible, there are even fewer opportunities to engage with social networks, and there is a lot of fear and uncertainty surrounding health and safety. 51 Similar to what has been found in existing studies, we found that this impact may be even greater for marginalized survivors, including survivors living with disabilities, or survivors living alone, due to structural inequalities that exacerbate the effects of isolation.52,53
We also found that survivors who were living in shelter experienced anxiety and depression. Shelters, in addition to providing a safe living environment, can foster a sense of community among survivors and their families, and staff through offering group programming and activities for survivors and their children, and this certainly would be the case pre-pandemic. However, as shelters are congregate care settings, they had to adopt strict quarantine, social distancing, and lockdown measures as part of federal and provincial mandates during the pandemic. This often led to a reduction in support offerings to clients. 24 As a result, survivors face heightened forms of isolation accessing a service that was intended to provide safety, support, and community which, impacted their mental health. 52
For some survivors, delays in service access and availability were the impetus for experiencing new and increased anxiety. This was particularly salient for newcomers to Canada who did not always have the context for how long legal and immigration processes were supposed to take, faced language barriers, and sometimes were not able to access certain supports due to immigration status. In the context of the COVID-19 pandemic, distress from the uncertainty was an understandable reaction for everyone. However, research on how individuals coped with this level of uncertainty found that women faced the largest burden of uncertainty during the pandemic and had the most challenging time coping with it. 54 For survivors of VAW specifically, and especially survivors who were newcomers, when uncertainty became a pervasive element in every aspect of their lives, it has profound psychological impacts. 54
Second, consistent with other Canadian studies, we found that survivors described feelings of hopelessness and mental exhaustion while accessing and attempting to access services and supports during the pandemic.33,34 The time and effort some survivors needed to spend to get support added new sources of stress in their lives, with some survivors sharing that trying to access services became a full-time job. Research has identified that staff working at VAW organizations in Canada felt hopeless in the face of the closure and delay of social services, especially the justice systems, which created additional barriers for survivors navigating an already overburdened system.29,31 We build on this literature by showing how this feeling of hopelessness was also felt by survivors, who despite persistent efforts were often continuously led to believe that they would not be able to get the basic supports that they needed to be safe. Adding to feelings of hopelessness among survivors, and substantiated by existing research, was discrimination they faced when trying to access supports, including securing housing while being on ODSP 55 or receiving trauma-informed healthcare as newcomer. 56
Third, we found that survivors described experiencing feelings of shame and low self-esteem. Shame is represented by intense feelings of inferiority, worthlessness, and embarrassment and has been shown to predict depressive symptoms.57,58 Furthermore, both shame and depression are associated with self-harm and substance use, 57 which contribute to feelings of insignificance and worthlessness. 58 In non-crisis situations, extensive literature has identified that shame is pervasive among VAW survivors59,60 and in particular immigrant women. 61 We found that VAW service delivery during the pandemic created new pathways for some survivors to feel shame while at the same time unintentionally offering other survivors’ ways to alleviate feelings of shame. For example, survivors living both at home and in shelter often needed to access supports in front of their children or loved ones and lacked private spaces to process their trauma and discuss future planning, causing significant feelings of failure and embarrassment. Furthermore, survivors, especially mothers, faced barriers to completing tasks, work, or improve their situation (through securing housing, nutrition, immigration status, etc.) during the pandemic which impacted their self-worth. At the same time, we also found that adding virtual support helped to mitigate feelings of shame and embarrassment for some new-commers to Canada, highlighting how modes of service delivery are experienced differently across participants with different lived experiences and personal circumstances. This nuance has yet to be fully discussed in existing literature, with studies instead either solely arguing the benefits or drawbacks of virtual services. For example, one Canadian study recommended offering virtual programming for women accessing VAW services when in-person care options are reduced with little discussion of how this could impact survivors feelings of shame and self-esteem. 22
Fourth, we identified that a consistent narrative thread running through survivor interviews and interconnected to the other three themes was resilience. Survivors, in the face of harrowing circumstances, described dedicating their time and resources to supporting other VAW survivors and giving back to the services they accessed, maintaining a positive outlook, and modeling healthy coping strategies for their children. Survivors were persistent and determined in their pursuit to secure sustainable autonomy and independence for their lives, create financial stability for their families, and heal from the trauma they experienced. Extensive literature documents resiliency among VAW survivors and identifies resiliency as a protective factor for mental health and well-being in the face of adverse circumstances.62,63 We found that both resiliency and adverse mental health can be present at the same time for survivors, and all survivors had to demonstrate resiliency as a survival mechanism. Furthermore, we recognize the potential harm that comes along with describing resiliency as something survivors should aspire to have, placing additional pressure on survivors who are by necessity resilient, working tirelessly to protect their own and their family’s lives. A potential consequence of not identifying as resilient is guilt or shame, or feeling undeserving or unworthy of help. Mantler et al. described this phenomenon as obligatory gratitude, when survivors are grateful for services even when their needs are not being met. 31
Strengths and limitations
Our sample was comprised of a small but diverse group of participants in terms of personal factors (i.e. ethnic and racial identities, disability status, having children) and services accessed, who provided rich and in-depth data in narrative form. We analyzed our data using a narrative thematic analysis. This allowed us to capture the complexity in survivors’ stories and conduct a nuanced exploration of the contextual factors that shaped how and why stories were being told. By applying a critical feminist lens and social justice framework to our analysis, we were able to identify interconnected patterns of structural disadvantage that systematically marginalize women at the intersection of different social identities.
A growing body of literature points to the unique help-seeking barriers faced by gender and sexual minorities, including the relationship between help-seeking and mental health.64 –66 We were not able to identify how gender identity and sexual orientation intersected with mental health as this was not present in our data.64 –66 While saturation was not a goal of our study as it was not a component of narrative thematic analysis methodology, 67 most of our participants identified as heterosexual cis-women and our sample may not be representative of the experiences of gender and sexual minorities accessing VAW organizations during the pandemic. Furthermore, our study also only focuses on VAW survivors from Toronto, Canada’s largest and most diverse city. While we provide an in-depth snapshot of Toronto-based perspectives, it is necessary to consider other Canadian regions (including rural and remote areas) and Indigenous communities. 68 It is also important to note that some participant interviews were conducted with a translator as the participant did not speak English. While this meant that we were able to have a more diverse sample by including participants who did not speak English, there is a possibility that the translator may have missed some of the nuance of participant responses.
Conclusions
VAW has clear and detrimental impacts on the mental health of survivors and our findings show that public health emergencies exacerbate these impacts, even for survivors accessing and engaging with supportive services. During the pandemic, survivors experienced greater mental health needs and at the same time encountered greater challenges when accessing support from a chronically under-funded sector, which had significant consequences for their mental well-being.
Implications
Protecting and prioritizing the mental health of VAW survivors should be an essential component of Canada’s NAP to End Gender-Based Violence. It is also imperative for policymakers to consider how public health mandates, intended to protect population health, might inadvertently and uniquely harm VAW organizations and the mental health of VAW survivors. VAW services must be considered essential services throughout future public health emergencies and be resourced accordingly. This requires that wrap around services that survivors commonly access including legal, justice, immigration, health, and housing systems are resourced to offer trauma-informed, timely, and accessible, support that meets the unique needs of VAW survivors during and beyond public health emergencies Consistent and concrete funding that is specifically supportive of VAW survivor mental health is urgently needed. With mental illness and VAW being deemed pandemics, in their own right, the consequences of not doing so could be catastrophic.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251338484 – Supplemental material for The mental health of survivors of violence against women who accessed supportive services during the COVID-19 pandemic: A narrative thematic analysis
Supplemental material, sj-pdf-1-whe-10.1177_17455057251338484 for The mental health of survivors of violence against women who accessed supportive services during the COVID-19 pandemic: A narrative thematic analysis by Bridget Steele, Priya Shastri, Catherine Moses, Elizabeth Tremblay, Monique Arcenal, Patricia O’Campo, Robin Mason, Janice Du Mont, Maria Hujbregts, Amanda Sim and Alexa R. Yakubovich in Women’s Health
Footnotes
Acknowledgements
We thank the participants in the study for their time and their willingness to share their experiences with the research team.
Ethical considerations
The Unity Health Toronto Research Ethics Board (REB #20-124) and the Dalhousie University Research Ethics Board (REB #2022-6275) approved this study.
Consent to participate
Written informed consent was obtained from all individual participants included in the study, prior to study initiation.
Consent for publication
As part of the informed consent process, participants consented to having their anonymized transcripts be analyzed and have the results, including, selected quotes, published in academic journals.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge funding from the Canadian Institutes of Health Research (PCS-183421), the Temerty Foundation and the University of Toronto through the Toronto COVID-19 Action Initiative; the University of Toronto’s Faculty of Medicine Equity, Diversity, and Inclusion fund; and the St. Michael’s Hospital Foundation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Priya Shastri was employed by the Toronto Region Violence Against Women Coordinating Committee (VAWCC) at the time of data collection, and Elizabeth Tremblay is employed by the VAWCC. The VAWCC is funded by the Ontario Ministry of Children, Community and Social Services (MCCSS), which is a primary funder of many VAW organizations in the Greater Toronto Area. Maria Hujbregts was employed by Family Service Toronto, which receives funding from MCCSS. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.