
Abstract
Background:
Gestational weight gain (GWG) impacts both foetal and maternal health outcomes, with excessive GWG in overweight and obese people further increasing the risk of complications for this population. Lifestyle changes including consuming a healthy diet and physical activity are core strategies for management. Since 2020 and the emergence of the COVID-19 pandemic, use of telehealth has increased; however, little is known about the effectiveness of virtually delivered strategies for maintaining healthy gestational weight during pregnancy.
Objectives:
To describe the effect of virtually delivered lifestyle interventions on promoting healthy GWG and reducing maternal and foetal complications associated with excessive GWG, with the view to inform future clinical practice.
Design:
This systematic review followed preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines and targeted quantitative studies assessing virtually delivered lifestyle interventions for maintaining healthy gestational weight for overweight and obese pregnant individuals aged 18 and older.
Data sources and methods:
Six databases (MEDLINE, CINHAL, EMBASE, EMCARE, MIDIRS and APA PsycINFO) were searched using a rigorous search strategy. Data extraction investigated mode of telehealth delivery, intervention type and GWG outcomes. Quality appraisal was conducted using the Critical Appraisal Skills Programme tool and risk of bias was assessed using the Risk of Bias assessment (RoB-2).
Results:
Nine studies met inclusion criteria and within those studies, six different telehealth modalities were identified. Interventions varied and included GWG tracking, step counts, diet and exercise goal setting. Effectiveness of studies was inconsistent, with five studies demonstrating lower GWG.
Conclusion:
Results suggest that lifestyle interventions delivered via telehealth may be effective at reducing excessive GWG. The development of targeted interventions integrated into obstetric guidelines aimed at reducing excessive GWG via telehealth platforms should be considered as a strategy not only for pandemic situations, but to increase antenatal care and service access.
Registration:
PROSPERO International Prospective Register on 26 January 2023 (CRD42023392095).
Introduction
Healthy gestational weight gain (GWG) during pregnancy, irrespective of pre-pregnancy body mass index (BMI), is one aspect of antenatal care known to positively influence maternal, foetal and neonatal outcomes. 1 Healthy GWG refers to GWG within the National Academy of Medicine (NAM) recommended guidelines compared with pre-pregnancy BMI, whilst excessive GWG is defined as exceeding the weight target stratified by pre-pregnancy BMI. 2 Globally, estimates suggest between 30% and 50% of pregnant people gain more gestational weight than recommended within healthy weight guidelines.3 –5 Compared with people of a healthy preconception weight, overweight or obese individuals are at a higher risk of excessive GWG during pregnancy,4,5 with excessive GWG further increasing the risk of complications for this population.6 –8 Given the potential impact on pregnant people and their baby, maternal obesity represents a serious and ongoing challenge to midwifery and antenatal care. 1
Pregnancy complications known to impact overweight and obese people may include maternal and foetal disease, injury or death, either antenatally, during delivery or postpartum.6,7 Maternal complications resulting from excessive GWG can include hypertensive disorders of pregnancy, gestational diabetes mellitus (GDM) and caesarean delivery.4,6 –8 Excessive GWG also increases the risk of foetal/infant complications, including macrosomia, large for gestational age, preterm birth and congenital abnormalities.4,6 –8 The impacts of excessive GWG extend beyond pregnancy and postpartum, having been associated with an increased risk of childhood overweight/obesity. 9
Lifestyle and/or behavioural interventions involving nutrition and physical activity are recommended strategies for promoting healthy GWG in pregnant people and general weight loss within the wider community. 10 Standard antenatal care guidelines provide basic information on lifestyle interventions during pregnancy.11,12 Whilst informative, these guidelines lack specificity around how to implement behavioural changes during pregnancy. 13 Dietary modification interventions have focussed on portion-control of carbohydrate, protein and fat intake, as portion control has been linked to greater weight reduction during pregnancy and an overall decrease in pregnancy complications.14 –16 Exercise-only interventions, including participation in aerobic and muscle-strengthening exercises, have significantly reduced the risk of people exceeding GWG guidelines,13,17 –19 whilst interventions combining dietary modification and physical activity have been found more successful in reducing GWG than diet or exercise alone, reducing the risk of excessive GWG by up to 20%.14,20,21
Traditionally, lifestyle interventions have been delivered to pregnant people through face-to-face antenatal care appointments; however, disadvantaged populations such as low-income earners, people of minorities and/or rural populations may contend with barriers in accessing face-to-face healthcare. 22 People with poor access to antenatal care are more likely to experience GWG outside recommended guidelines regardless of pre-pregnancy BMI. 23 Whilst pregnant people experiencing socioeconomic, cultural or environmental barriers are known to access face-to-face antenatal care less frequently, 22 telehealth has been demonstrated as a useful alternative in delivering antenatal care and advice. 24
Defined as the use of a technology-based virtual platform to deliver aspects of health information, telehealth is one of the fastest growing sectors of healthcare provision. 25 With increased use of mobile phone applications, short messaging services (SMS)/text messages, wearable devices, live audio-visual communication and multimedia and services offered via telehealth have rapidly proliferated.25 –27 Reported successes of telehealth include a reduction in health disparities, improvement in health literacy and elimination of access barriers, particularly in low socioeconomic status populations.26,27 Inclusive of all virtually delivered interventions, telehealth has been found effective in improving obstetric outcomes, with demonstrated equivalence to in-person care. 26 More specifically, telehealth interventions have been associated with improvements in perinatal smoking cessation, breastfeeding, appointment optimisation for high-risk obstetrics and early access to medical abortion services. 26 Whilst the COVID-19 pandemic provided a catalyst for the uptake of telehealth globally, 28 evidence-based use and implementation of telehealth platforms in obstetric and maternal care continues to be informed by ongoing research, including GWG. 26
The complex nature of GWG, pregnancy and post-partum outcomes, particularly in overweight and obese pregnant people, necessitates a comprehensive approach to antenatal care. Through leveraging the innovative strategies of telehealth and lifestyle/behaviour change interventions, healthcare professionals can strive to reduce rates of excess GWG, thereby limiting associated maternal and foetal complications. Despite a number of primary studies having been conducted examining telehealth interventions aimed at managing and preventing excessive GWG, there is currently a lack of evidence-based detail informing the practice of telehealth-delivered lifestyle and behavioural interventions in antenatal care. The purpose of this systematic review was to inform future practice by describing the effect of virtually delivered lifestyle interventions in promoting healthy GWG in pregnant people with a BMI over 25 kg/m2, and the effect of those interventions on reducing maternal and foetal complications associated with excessive GWG.
Methods
Search procedures
This review followed the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines 29 to identify and analyse relevant studies. The protocol was registered with PROSPERO International Prospective Register on 26 January 2023 (CRD42023392095). 30 Search terms were pregnancy, obesity, overweight, BMI, physical activity, diet, behavioural interventions and telehealth and databases were MEDLINE, CINHAL, EMBASE, EMCARE, MIDIRS and APA PsycINFO (see Supplemental Appendix 1, for example, search strategy). The literature search was limited to peer-reviewed articles published between 2001 and January 2023.
Retrieved studies were exported to a shared reference managing system (EndNote). 31 Duplicates were removed, and the remaining studies were exported into a systematic review management tool (Covidence) 32 for title and abstract screening. Two researchers independently completed the screening process, and conflicts were resolved through team consensus. See Table 1 for inclusion and exclusion criteria.
Inclusion criteria and exclusion criteria.

GWG: gestational weight gain; BMI: body mass index.
Data extraction
Information was collected and tabulated with regard to study characteristics, study participants; health professional involvement; intervention type; mode of telehealth delivery and outcomes related to GWG, foetal and maternal complications.
Quality assessment
Two researchers independently evaluated methodological quality using the Critical Appraisal Skills Programme (CASP) randomised controlled trial (RCT) checklist, 33 and three researchers independently completed the Risk of Bias assessment (RoB-2). 34 Discrepancies were resolved via group consensus. Findings were consolidated into a summary table and discrepancies were resolved through consultation with the research team.
Results
Figure 1 presents the PRISMA flowchart outlining study selection process. The initial search identified 2897 articles across the 6 databases. After 1198 duplicates were identified and removed, and an additional 5 articles were marked ineligible by automation tools, 1694 articles underwent title and abstract screening. Following this, 110 articles were deemed eligible and underwent full-text evaluation. Of those, nine articles met the inclusion criteria and were selected for this review.
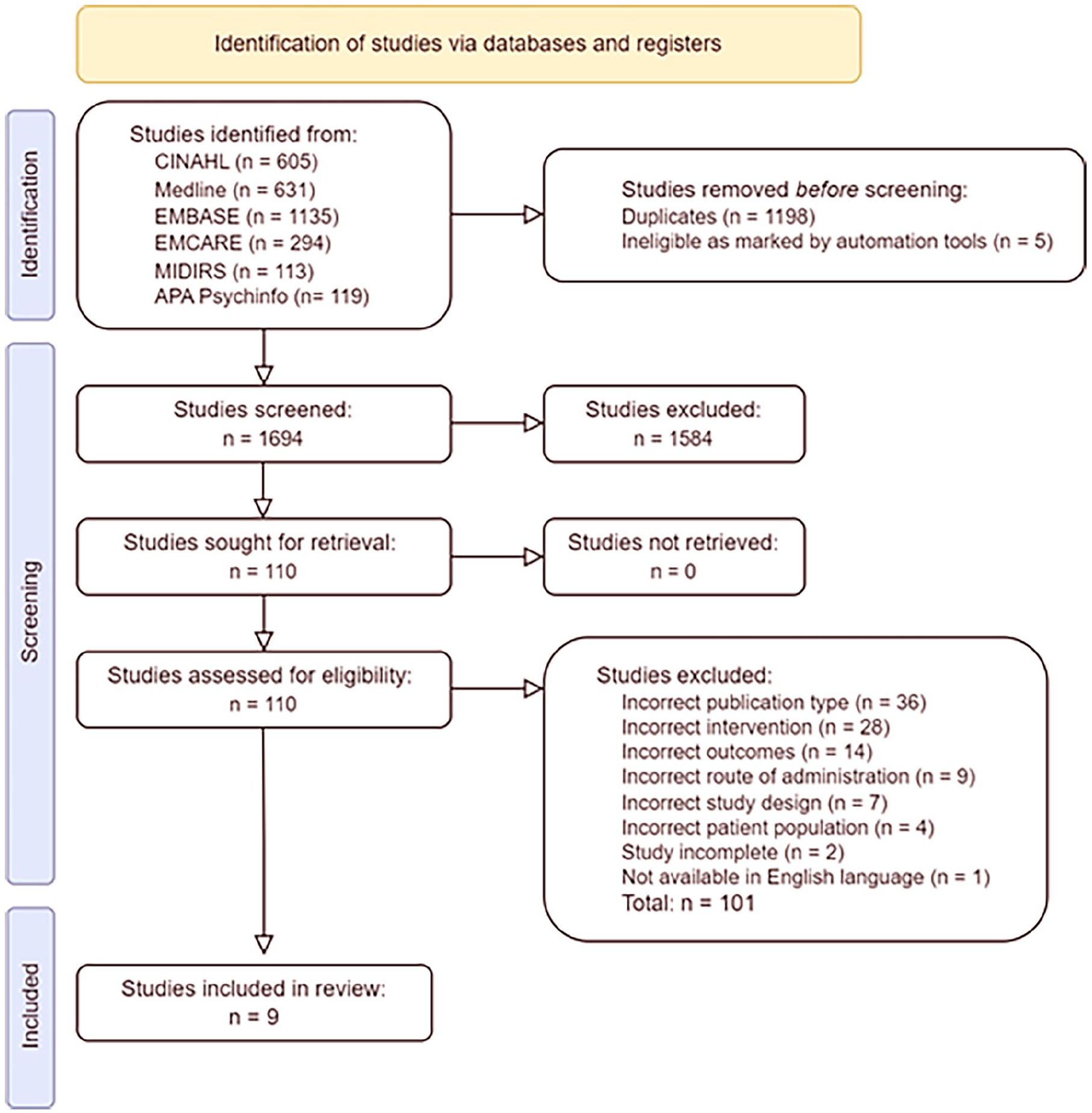
PRISMA flowchart.
Study characteristics
All nine included studies were RCT, published between 2014–2022. Most included studies were conducted in the United States,35 –40 with one in Australia, 41 one in Spain 42 and one in Taiwan 43 (see Table 2). Sample sizes ranged widely, from 35 to 1689, with an accumulated sample size of 2215. Of the nine included articles, two studies (one authored by Olson et al. 39 and one authored by Graham et al. 35 ) were secondary analyses of one primary Olson et al. study. 38 For the purpose of this systematic review, the Olson et al. primary study has been referred to as Olson et al. (a) 38 and the secondary analyses authored by Olson et al. is referred to as Olson et al. (b) 39
Study characteristics.

RCT: randomised controlled trial; T: total number of participants; I: number of intervention participants; C: number of control participants; GWG: gestational weight gain; BMI: body mass index; SMS: short messaging service; SD: standard deviation; CI: confidence interval.
Study participants
All study participants were aged 18 years and over, with mean ages varying from 25.0 to 33.4 years. Participant BMIs ranged from ⩾18.5 to <45 kg/m2. Aligning with inclusion criteria, this systematic review only included data from participants with a BMI ⩾25 kg/m2. Participants were recruited during the first and second trimester, between 10 and 21 gestational weeks.
Health professional involvement
Telehealth interventions were delivered by seven different healthcare providers, including dietitians, physiotherapists, obstetricians, paediatricians, nurses, midwives and health coaches. In seven studies, research team members were involved in intervention delivery 35,37 –42
Modality of telehealth intervention
Six types of telehealth were used to deliver interventions across the nine studies, including SMS, video messaging, phone calls, mobile applications, websites and social media platforms/chatrooms (Table 3). All of the included studies with the exception of the Olson studies used SMS,36,37,40 –43 with five using individually tailored SMS to encourage participant monitoring and motivation throughout the study.36,40 –43 Eight of the nine studies reported using at least two platforms to deliver behavioural intervention(s).35,36,38 –43 The study by Holmes et al. was the exception, using only SMS as the mode of telehealth delivery. 37 As an adjunct to telehealth platforms, four studies used pedometers to promote physical activity goals, 36,40,42,43 with Herring et al. 36 also providing a listener soundtrack to encourage activity.
Mode of telehealth delivery, intervention type and outcomes for each included study.

SMS: short messaging service; DVD: digital versatile disc; GWG: gestational weight gain; ✓: study included the mode of intervention or the type of intervention; q: goals were set and articles discussed both quality and quantity of nutrition intervention; NS: outcome assessed but not significant; ✓*: outcome assessed and statistically significant positive result noted; ✗*: outcome assessed and statistically significant negative result.
All included studies introduced behavioural and/or lifestyle change interventions, including GWG tracking, physical activity/exercise prescription and/or dietary goal setting/monitoring. Four studies utilised all three intervention types,36,40,41 two studies implemented only GWG tracking and exercise interventions,42,43 whilst one study used only nutrition and exercise interventions. 37
Types of intervention
GWG tracking was a common intervention type, with all but one of the studies requiring participants’ track their weight gain throughout pregnancy as a means to increase motivation and encourage programme adherence.36,38,40 –43 All studies included a physical activity target, with six of the seven primary studies specifying either the amount of time spent exercising37,38 and/or a daily step count.36,40,42,43 The study by Willcox et al. 41 allowed individuals to set a non-specified exercise target aimed towards meeting physical activity guideline recommendations, whereas two studies focussed on time spent exercising as the physical activity goal.37,38 One study-based exercise targets on the American College of Obstetrics and Gynaecology (ACOG) Guidelines, 44 recommending 20–30 min of moderate-intensity physical activity per day. 37 Olson et al. (a) 38 researchers based the physical activity goal on participant’s pre-pregnancy activity levels, creating three targets correlating to ‘sedentary’, inadequately active and ‘adequately active’.38,45 Of those studies that included a step count, all participants received pedometers to assist in achieving a step count goal.36,40,42,43 Six studies allowed participants to monitor their physical activity goal progress via telehealth platforms and/or a supplied pedometer.36,38,40 –43
Dietary interventions based on goal setting and/or self-monitoring of participants’ current diet were implemented in all but the Gonzalez-Plaza et al. study.35 –41,43 Within most studies, dietary goals were set by researchers and/or participants as part of the intervention,36 –38,40,41 where Olson et al. (a) 38 used input from both researcher and participants to formulate the dietary goal via a quiz. 39 Four studies incorporating dietary interventions specified the quantity and quality of foods to help achieve a healthy diet, including increasing vegetable intake, replacing sugar-sweetened beverages and increasing the total daily calories by 300 per day during pregnancy.36,37,40,41 Whilst excluding a dietary goal setting component, one study required participants monitor their current diet to increase daily intake awareness. 43 Similarly, three other studies also required participants monitor their dietary intake via the telehealth platform.36,38,40
Outcomes related to GWG, foetal and maternal complications
Given the range of telehealth platforms and variety of behavioural interventions implemented across studies, measures and study outcomes relating to GWG, and foetal/maternal complications, were varied (Table 2).
Eight of the nine studies included control groups,35 –38,40 –43 of which three showed no statistically significant difference in total or excessive GWG between intervention and control groups.37,38,40 Of those studies that included a control group, four received standard antenatal care,36,41–43 two received generic pregnancy-related SMS37,40 and two received access to a website containing standard antenatal health information.37,40
Three studies yielded no statistically significant difference in total or excessive GWG between intervention and control groups.37,38,40 Eight studies included excessive GWG as an outcome measure, where excessive GWG was reported as a percentage of those participants exceeding recommended GWG guidelines in total kilograms, or as a relative risk.35 –39,41 –43 Three of those studies showed statistically significant results;36,39,43 two of which demonstrated the control group was more likely to exceed both total36,43 and weekly36,43 GWG recommendations. The primary Olson et al. (a) study provided two datasets, with one dataset unadjusted and the other adjusted for covariates including BMI, age, parity and other pregnancy variables. 38 Datasets were further stratified by income, including low-income (Medicaid eligible) and not-low-income. 38 When comparing healthy weight versus overweight and obese participants, Olson et al. (b) found that for higher BMI participants, setting two or more behavioural goals was significantly associated with an increased risk of excessive total GWG. 39
All included studies measured total GWG, five of which reported statistically significant results.35,39,41 –43 Of those five studies, two demonstrated that participants in the intervention arm gained less total GWG than the control arm.41,42 The role of weight tracking using telehealth platforms was inconsistent across studies, whereby not-low-income participants who consistently tracked their weight resulted in less total GWG than those who did not. 35 In the adjusted dataset, not-low-income overweight and obese pregnant participants who were consistent trackers and super users (defined by consistent log-ins to the website and GWG tracking), gained less than those not as engaged with the intervention. 35 The study by Chen et al. demonstrated a statistically significant reduction in total GWG (5.44 kg) in the intervention arm only during the third trimester. 43
Four of the nine studies measured maternal and foetal complications, including GDM, pre-eclampsia, macrosomia, pre-term birth, birth weight and caesarean deliveries.36,38,42,43 Olson et al. (a) demonstrated a statistically significant reduction in pregnancy complications in the intervention arm compared to the control, reporting significantly fewer macrosomic babies whose mothers had participated in an intervention. 38 Olson et al. (a) also identified that high-income overweight and obese mothers participating in an intervention had significantly increased rates of repeat caesareans when compared to control participants. 38
Overall, five studies demonstrated statistically significant results in relation to telehealth-delivered behavioural intervention effectiveness in promoting healthy GWG in overweight or obese pregnant participants and/or reducing maternal and foetal complications associated with excessive GWG.36,38,39,41 –43 All five of those studies used a variety of virtual platforms, and utilised GWG tracking, exercise goal setting and goal-specific self-monitoring as behavioural interventions.36,38,39,41 –43 Additionally, all five studies incorporated a reward for progress throughout the study and/or an incentive to participate.36,38,39,41 –43 The most commonly used virtual platform was SMS,36,41 –43 with all five studies using greater than one platform compared to non-statistically significant studies that used only SMS. These results suggest multiple virtual platforms designed to deliver behavioural interventions that include the ability to track GWG, and set and monitor exercise goals, are effective at promoting healthy GWG throughout pregnancy.35 –39,41 –43
Quality appraisal
A comprehensive illustration of results from the CASP and RoB-2 is presented in Supplemental Appendix 2. In summary, completion of the CASP identified all studies included similar groups at the start of the RCT, received similar levels of care during the studies and the intervention effects were reported comprehensively. Due to the nature of telehealth interventions, six articles were unable to include blinding and were limited by their small sample sizes.36,37,40 –43 Assessment of the risk of bias utilising the RoB-2 tool revealed no study as ‘low risk’; however, four of the nine studies were evaluated as ‘some concerns’35,38,39,41 and the remaining were evaluated as ‘high risk’.36,37,40,42,43
Discussion
This systematic review described the effective of telehealth-delivered behavioural interventions designed to reduce GWG in overweight or obese pregnant people and explored the effect of those interventions in reducing maternal and foetal complications associated with excessive GWG. Across the nine studies, a variety of telehealth platforms were used to deliver behavioural interventions, including SMS, video messages, phone calls, phone applications, websites and social media platforms. All platforms used unique features that allowed GWG-tracking and self-monitoring of dietary and physical activity goals. Aligning with previous research exploring the effectiveness of eHealth weight loss interventions for overweight and obese populations, four studies included in this review identified that individualisation of text messages increased intervention adherence.28,40 –43 Findings from this systematic review complement separate research identifying the addition of behavioural components, such as self-monitoring, or the use of technology platforms such as social media, as more effective than standard telehealth programmes. 46 The result suggests that future telehealth interventions would benefit from the inclusion of personalised messaging to promote sustained engagement, alongside the use of population focussed interventions via social media.
Consistent with previous studies exploring the effectiveness of behavioural interventions delivered in-person, most studies included in this review identified significant reductions in total and/or excessive GWG as per NAM guidelines for virtually delivered care, thus demonstrating that telehealth-delivered interventions appear as effective in reducing GWG as those traditionally delivered face-to-face.14,20,35,36,41 –43 Whilst measurements of GWG were standardised using NAM guidelines across the studies included in this review, exercise and diet interventions were informed by separate guidelines specific to the geographical location and year each study was conducted. Similar to previous reviews, findings from this systematic review support the development and implementation of a standardised guideline for exercise, diet and lifestyle interventions during pregnancy.7,13
Excessive GWG is known to be associated with a higher risk of maternal and foetal complications during and after pregnancy.2 –4 Whilst Olson et al. (a) was the only study to find a statistically significant reduction in foetal macrosomia, 38 both Chen et al. and Gonzalez-Plaza et al. found a non-statistically significant correlation between reduced GWG and lower prevalence for multiple maternal and foetal complications,42,43 further supporting results from previous research investigating adverse pregnancy outcomes.8,9,13 Given the lack of statistically significant findings in those studies that included this outcome measure, it is recommended that all future studies examining excessive GWG include the exploration of maternal and foetal complications as an outcome measure.
Virtually delivered healthcare can play an important role in reducing barriers and improving access options for weight management interventions, 47 providing healthcare providers opportunities to bridge social and cultural challenges potentially impacting intervention uptake and adherence. When considering the diverse geographical locations and socioeconomic status of participants across the studies included in this review, telehealth was reported to be well received, with virtual-care platforms offering an accessible delivery method of antenatal care.35 –43 This finding supports the inclusion of telehealth as an intervention delivery option, supporting those who may experience socio-economic and/or environmental disadvantage and have limited access to face-to-face maternity care. 5 Whilst the methods for telehealth-delivered care continue to evolve, virtual-care platforms offer a cost-effective, culturally sensitive and individualised alternative to traditional methods of antenatal care.
Limitations
As identified in the quality appraisal, studies included in this review were limited to nine overall, with small sample sizes affecting reliability, consequently affecting accuracy when considering the effects of virtually delivered lifestyle interventions across a broad population. Additionally, six of the studies 36,37,40 –43 included in this review were unable to blind participants, thus potentially affecting participant behaviour and individual study outcomes. To support reliability, thus improving intervention guideline development, it is recommended that more studies examining the effect of telehealth interventions on GWG are undertaken, with larger sample sizes.
Conclusion
This systematic review evaluated telehealth-delivered behavioural interventions in overweight or obese pregnant people. Results suggest that lifestyle interventions delivered via telehealth may be effective at reducing excessive GWG. This information can be used to develop targeted interventions integrated into obstetric guidelines aimed at reducing excessive GWG via telehealth platforms. However, strategies to address the limitations of cost and inaccessibility of telehealth to the wider community are required before full integration into the healthcare sector.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251336292 – Supplemental material for Virtually delivered lifestyle interventions for overweight and obese pregnant people: A systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057251336292 for Virtually delivered lifestyle interventions for overweight and obese pregnant people: A systematic review by Tahlie Park, Scarlett Brickwood, Kelsey Buss, Vivian Tran, David Parsons, Kerrie Wisely, Katharine Gillett, Heidi Lavis and Susan Heaney in Women’s Health
Footnotes
Acknowledgements
The authors would like to acknowledge Fiona Jones, Teaching Liaison Librarian, The University of Newcastle for her assistance with final search terms and strategy.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kerrie Wisely, Heidi Lavis and Susan Heaney are employed under the Rural Health Multidisciplinary Training Programme funded through the Australian Commonwealth Department of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All included articles are published.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.