
Abstract
Background:
Sixty-three percent of pregnant persons report experiencing lumbopelvic pain (LPP), which can negatively impact quality of life and lead to the development of fear avoidance behaviors. Exercise is a safe, non-pharmacological treatment for reducing and preventing the development of pain, but the volume of exercise required for one to benefit from it is unknown.
Objectives:
Determine whether meeting exercise guidelines during pregnancy associates with LPP, disability, and fear avoidance behaviors.
Design:
Cross-sectional study.
Methods:
Pregnant persons (n = 50, 32.0 ± 4.2 years, 28–32 weeks of gestation) were included. Participants completed questionnaires assessing second-trimester physical activity (PPAQ), current pain, lumbopelvic disability, and fear avoidance and then underwent a physical examination for the presence of LPP. Participants who met exercise guidelines (>150 min moderate intensity physical activity/week, PA, n = 24) were compared with those who were not physically active (<90 min moderate intensity physical activity/week, NPA, n = 26). Nonparametric tests compared groups on outcomes with significance set at p < 0.05. Post hoc odds ratios were calculated for moderate disability status. Spearman’s rho correlations were conducted between physical activity (MET min/week), pain, and disability.
Results:
NPA participants reported more disability due to LPP (p = 0.02), more fear avoidance behaviors (p = 0.03), and more provoked LPP (p = 0.09) than PA participants. NPA participants were also more likely to report LPP disability (OR = 3.89, 95% CI: 1.19–12.68) and fear avoidance behaviors (OR = 4.38, 95% CI: 1.03–18.56). In all participants, more moderate intensity physical activities were associated with less disability (ps < 0.05) and fewer fear avoidance behaviors (p = 0.06). Pain severity did not differ between groups (ps > 0.05).
Conclusion:
Meeting pregnancy exercise guidelines throughout the second trimester associated with less LPP disability, fewer fear avoidance behaviors, and less-provoked pain, but did not associate with pain severity.
Plain language summary
Low back and pelvic pain are common during pregnancy and impact quality of life, physical activity participation, job performance, childcare abilities, and mood. Pain can also lead to the development of avoidance behaviors, when an individual limit their activity to avoid provoking their pain. In the nonpregnant population, those who exercise more experience less back pain, reduced disability, and fewer avoidance behaviors, but more research is needed among the pregnant population. The aim of this study was to determine whether individuals who exercised regularly throughout pregnancy (greater than 150 minutes of moderate intensity exercise per week) reported less low back and pelvic pain, less disability related to back and pelvic pain, and fewer avoidance behaviors due to that pain than non-active pregnant individuals (less than 90 minutes of moderate intensity exercise per week). Participants who regularly exercised throughout pregnancy reported less low back and pelvic girdle disability and fewer avoidance behaviors than the non-active participants. The severity of back and pelvic girdle pain did not differ between groups. These findings support prior work highlighting the benefits of exercise during pregnancy. Maintaining physical activity levels that align with current recommendations (150 min/week) during pregnancy associates with less disability and avoidance behaviors. Healthcare providers should discuss the benefits of being active during pregnancy with their patients.
Introduction
Lumbopelvic pain (LPP) affects ~63% of pregnant persons, particularly during the second and third trimesters.1,2 Nonspecific LPP is a global term comprised of pregnancy-related low back pain (LBP), pelvic girdle pain (PGP), or a combination of both (LBP and PGP).3,4 While LBP relates to pain located inferior to the 12th rib and above the gluteal fold, 5 PGP is specific to the sacroiliac joints between the iliac crest and gluteal fold, with or without pain at the pubic symphysis. 5 PGP prevalence data vary based on how it is classified, but a recent review article found a prevalence between 16% and 25% using objectively verified studies. 6 Each type of pain has different etiologies, diagnostic tests, and prognoses.4,5 Nonspecific LPP in pregnancy has been associated with lower quality of life, less physical activity, poorer job performance, more sick leave, impaired childcare abilities, and the development of fear avoidance behaviors. 7
The fear avoidance model, based on a biopsychosocial approach to pain, refers to the cognitive anticipation of pain because of injury, movement, or activity that leads to changes in behavior.8 –10 Fear avoidance is related to pain catastrophizing and negatively impacts quality of life, work status, physical ability, and activities of daily living during pregnancy.11,12 Higher fear avoidance during pregnancy is predictive of persistent LPP into the postpartum period, which affects up to one-third of pregnant persons with LPP.3,11,12 Olsson et al. 9 found that pregnant persons with LPP in early pregnancy have significantly higher fear avoidance beliefs than those without LPP. Associations among fear avoidance, disability, and pain severity in late pregnancy are not known.
Exercise in nonpregnant persons has been shown to reduce fear avoidance behaviors, improve occupational disability ratings and increase self-efficacy. 13 Greater daily physical activity has been correlated with lower fear avoidance among nonpregnant persons with chronic LBP. 14 Exercise (both aerobic and resistive) can increase the strength of the muscles and tensile strength of the surrounding ligaments, fascia, and tendons in the lumbopelvic region, thereby providing better support and motor control. 15 This type of specific muscle strengthening during pregnancy can reduce the odds of pain in the postpartum period (OR = 0.52; 95% CI: 0.28–0.94). 16 Vleeming et al. 5 hypothesized that PGP results from dysfunctions with form closure and/or force closure of the pelvis. Therefore, performing regular exercise may strengthen this region and protect LPP from developing. Indeed, exercise has been shown to reduce the severity of both LBP and PGP (standardized mean difference: 1.03, 95% CI: −1.58 to −0.48), but not to decrease the odds of developing LPP during pregnancy. 3 Exercise in pregnancy has also been found to improve LPP through stabilization exercise, cardiovascular exercise, aquatics, and yoga/Pilates in some, but not all studies. 17 Thus, current data support exercise in pregnancy as having a therapeutic effect on LPP, but less is known about how much exercise (volume) is needed in pregnancy to see benefits related to LPP disability and fear avoidance.
The American College of Obstetricians and Gynecologists (ACOGs) recommends that pregnant persons perform a total volume of moderate intensity exercise for a minimum of 150 min per week. Unfortunately, only 19% of pregnant persons meet this recommendation.18 –20 This is worse than in the nonpregnant adult population, where 23.4% of adults meet their exercise guidelines (150 min moderate intensity exercise per week plus 2 days of strengthening exercise). 21
This study sought to compare LPP disability and fear avoidance behaviors between pregnant persons who met exercise guidelines (⩾150 min moderate intensity physical activity per week) with those who were not physically active (<90 min moderate intensity physical activity per week). It was hypothesized that physically active pregnant persons would report lower pain intensity, less pain-related disability, and fewer fear avoidance behaviors than nonphysically active pregnant persons.
Methods
This study was conducted between October 2021 and May 2022.
Participants
Participants were recruited in their second trimester (between gestation weeks 20 and 28). Study posters and brochures were posted in the community around the college campus, at community events and on social medial sites including Facebook and Instagram. Interested participants scanned a QR code, which opened a series of screening questions related to inclusion and exclusion criteria (via Qualtrics).
Inclusion and exclusion criteria were implemented to identify participants eligible for a larger parent study focused on exercise and sleep. Participants were included if they: (1) were between 12 and 32 weeks pregnant; (2) were between the ages of 18 and 40 years; (3) understood and comprehended study procedures and measures written and spoken in English; (4) reported either physical inactivity or activity (see below); (5) were willing to complete all study procedures; and (6) obtained medical clearance via the PARmed-X pregnancy screening form from their obstetric health provider. Regarding the inclusion criteria for physical activity: on the screening questionnaire, participants were asked “Do you participate in regular physical activity where your heart beat is elevated and you are breathing hard? Yes or No.” If they responded No, they were considered eligible and moved forward with the screener (i.e., physically inactive). If they responded “Yes,” they were prompted with two follow-up questions: “About how many minutes/day on average do you exercise for? _____” and “How many days per week on average do you exercise? _____.” If they responded with <90 (not physically active) or ⩾150 min (physically active) of moderate intensity exercise per week minute. These thresholds were based on American College of Sports Medicine (ACSM) guidelines for pre-exercise medical clearance stratification (<90 min/week moderate intensity physical activity = not physically active) and the ACOGs recommendations for physical activity in pregnancy (150 min/week moderate intensity physical activity). 22
Participants were excluded if they: (1) had a history (i.e., before pregnancy) of severe LBP or back surgery that would limit exercise participation; (2) had a diagnosed sleep disorder; (3) had any contraindication to participating in moderate intensity exercise, including but not limited to: severe anemia, maternal cardiac dysrhythmia, chronic bronchitis, poorly controlled type 1 or type 2 diabetes mellitus, poorly controlled hypertension, heart disease, or restrictive lung disease; (4) had a non-singleton pregnancy, an orthopedic and/or cardiovascular limitation; (5) had low body weight (BMI < 18 kg/m2) or extreme obesity (BMI > 40 kg/m2) prepregnancy; (6) experienced one or more of the following during this or a prior pregnancy: premature labor, placenta previa, poor fetal growth, premature rupture of membranes, preeclampsia, uterine growth retardation, incompetent cervix, persistent vaginal bleeding, anemia, or gestational diabetes.
Protocol
This cross-sectional study recruited participants between 28 and 32 weeks of gestation. The reporting of this study conforms to the The Strengthening the Reporting of Observational Studies in Epidemiology statement. 23 Interested participants were screened for participation via an online screening questionnaire (Qualtrics). Eligible participants were contacted by phone, told more about the study, and scheduled for an in-person visit at a fitness facility in a large public university. At the in-person visit, participants who met a second eligibility check then underwent informed consent. After consent was obtained, participants completed a series of questionnaires electronically on a tablet (see section “Materials”). Participants then underwent a physical examination by a licensed physical therapist (author TM), which included resting vitals (e.g., blood pressure and heart rate), and a battery of LPP provocation tests. The battery included the following: the Straight Leg Raise Test (SLR), 24 the Bowstring Test, 25 The Slump Test, 25 the Posterior Pelvic Pain Provocation Test (PPPP), 26 the Flexion Abduction External Rotation Test (FABER), 27 a Compression Test, 27 and a Distraction Test. 27 A positive test provokes a participant’s pain whereas a negative test does not. Collectively, these tests have a high validity and reliability for determining the presence of low back (SLR, bowstring, and slump tests) and pelvic girdle (PPPP, FABER, and compression and distraction tests) pain particularly when performed together in a battery of tests in pregnant persons. 27 Data were stored electronically in dual factor–locked cloud-based system and are available upon request. Participants were compensated for their time following completion of the study.
Measures
Participants completed questionnaires during the in-person visit on a tablet via Qualtrics. To account for potential covariates, participant age, parity, gestational age, race, marital status, gestational weight gain, and socioeconomic status (SES) were collected via a demographic questionnaire. Physical activity was assessed using the Pregnancy Physical Activity Questionnaire (PPAQ). The PPAQ is a validated questionnaire designed to assess and measure physical activity in pregnant persons throughout a specified trimester. 28 For our participants, they were asked to respond for how active they were during their second trimester. The questionnaire provides cumulative MET min/week information for all types of physical activity and splits it into domains including occupation, leisure, and exercise (moderate-to-vigorous physical activity). 28 After participants completed the study, they were grouped according to their self-reported moderate-to-vigorous minutes of physical activity per week on the PPAQ (<90 min moderate intensity physical activity/week = not physically active, NPA; ⩾150 min moderate intensity physical activity/week = physically active, PA).
The Oswestry Disability Index 29 was used to determine a patient’s perceived disability and activity limitation due to LBP using a 5-point Likert scale for 10 different activities and is considered the gold standard of low back functional outcome tools. 29 The outcome score was calculated using standardized scoring methods with higher values representing greater disability and the minimal detectible change score (MDC) of 1.7.29 –31 The Numeric Pain Rating Scale (NPRS) is a widely used tool to determine the severity of pain using a 10-point Likert scale. 32 The Pelvic Girdle Questionnaire (PGQ) 33 evaluates quality of life in women who experience PGP using a 4-point Likert scale for 25 different activities and has a MDC score of 14.8. 30 The Fear-Avoidance Beliefs Questionnaire, Physical Activity Subscale (FABQ-PA) was administered to assess body impairment limited by fear avoidance behaviors. It uses a 7-point Likert scale to determine the level of fear avoidance belief and has an MDC of 6.1.30,34
The following diagnostic criteria were used for each questionnaire to compare frequencies in each group: Oswestry Disability Index 29 (>15), PGQ (>20) and FABQ-PA (>15). Additionally, participants with either LBP or PGP were analyzed together as nonspecific LPP (i.e., either ODI > 15 or PGP > 20). Score thresholds were identified from LPP literature on pregnant and postpartum persons.30,35
Statistical analyses
Sample size estimates were based on Sonmezer et al., 36 who examined the effects of Pilates exercise on low back disability and found a mean difference benefit of −6.6 ± 8 in the Pilates group (n = 20). 36 Using the power calculator from clincalc.com on June 2021, with Type 1 Error set at 0.05 and Type 2 error set at 0.8, the estimated sample size needed was N = 48 (n = 24/group). 37 Assuming a 20% attrition rate, 60 participants were enrolled to retain a sample size of 48.
Data were analyzed using the IBM SPSS Statistics for Windows software, version 26.0 (IBM Corp., Armonk, NY, USA). Data were analyzed for descriptive statistics, tests of normality, and checks for assumptions for statistical analyses. Due to non-normality, nonparametric tests were conducted to compare differences in demographic variables and measures of pain, disability, and fear avoidance between NPA and PA groups. Receiver operating characteristic (ROC) analysis was conducted to determine the predictability of nonspecific LPP from the FABQ score. Pearson chi-squares were used to calculate odds ratios for disability incidence and diagnostic pain provocation between groups. Spearman’s rho correlations analyzed the relationship between moderate intensity physical activity MET min/week and pain and disability measures. Participants with missing data (<5% of the responses) were contacted over the phone and email to complete any missing questions from the questionnaires, no data were missing in the final analysis.
Results
A total of 50 participants aged 32.0 ± 4.2 years old (n = 26 NPA, n = 24 PA) completed the study and were included in the final analysis (Figure 1). Two enrolled participants became ineligible during the study (2/52 = 3.8%). No adverse events were reported. There were no statistically significant differences between PA and NPA groups on age, parity, race, education level, SES, employment status, marital status, prepregnancy or pregnancy body mass index (BMI), pregnancy weight gain, or weekly activity in METs (ps > 0.05, Table 1).
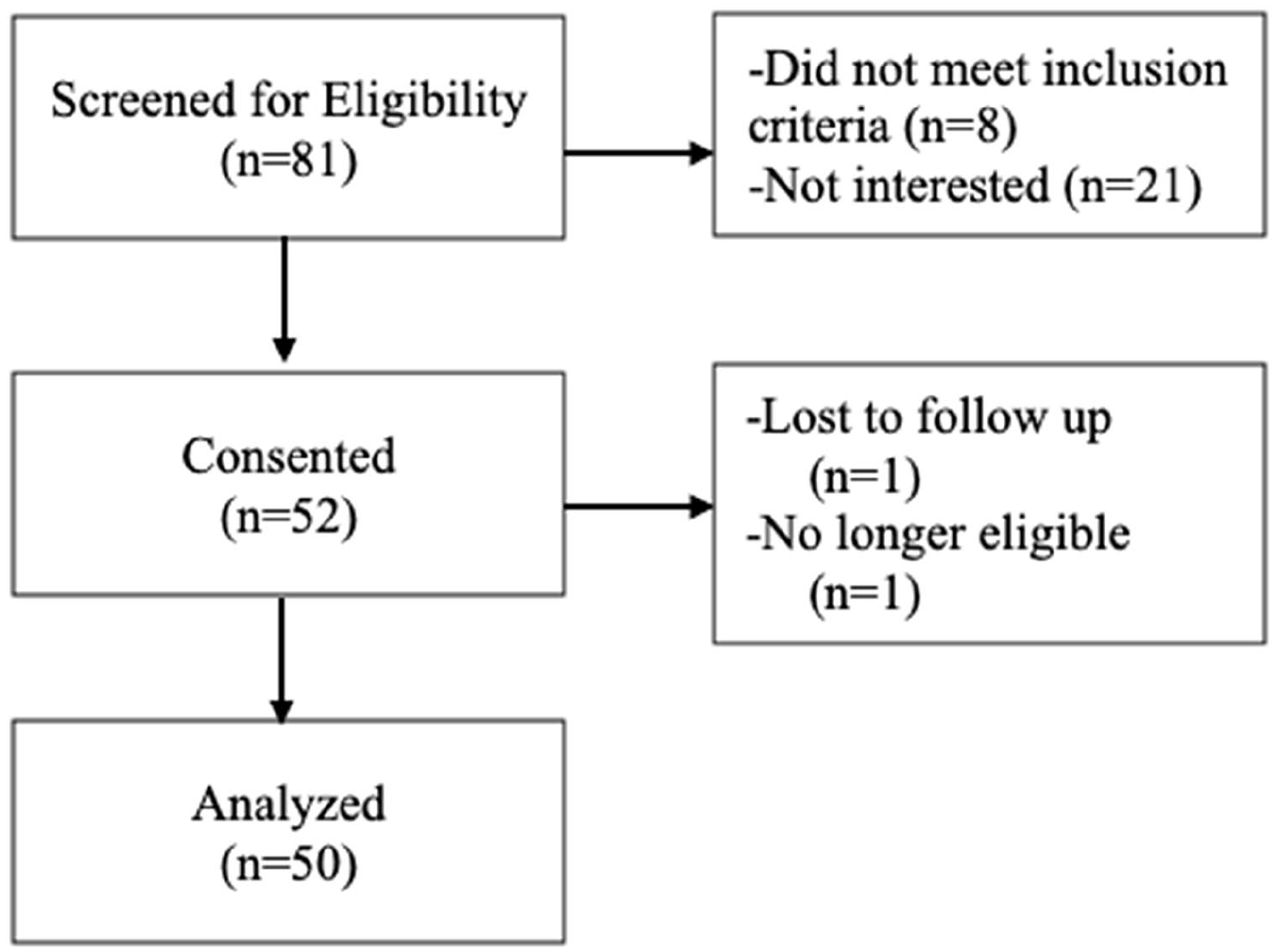
Consort flow.
Participant and group demographics.

n: sample size; NPA: not physically active; PA: physically active; HS: high school; BMI: body mass index; lbs: pounds; PPAQ: Pregnancy Physical Activity Questionnaire; METs: metabolic equivalents.
Participants in the PA group reported less back disability (U = 190.0, Z = −2.4, p = 0.017) (Figure 2(a)), less pelvic girdle disability (U = 209.5, Z = −2.0, p = 0.046) (Figure 2(b)), and less fear avoidance (U = 214.0, Z = −1.9, p = 0.056) (Figure 2(c)) than the NPA group. No differences in pain severity were observed between groups (p > 0.05). Compared with participants in the NPA group, participants in the PA group had lower incidence of being classified with disability for LBP (X2(1, N = 50) = 3.91, p = 0.048), PGP (OR = 5.18, 95% CI: 1.48–18.18, X2(1, N = 50) = 7.07, p = 0.01), nonspecific LPP (OR = 3.89, 95% CI: 1.19–12.69, X2(1, N = 50) = 5.27, p = 0.02), and had lower incidence of fear avoidance (OR = 4.38; 95% CI: 1.03–18.56, X2(1, N = 50) = 5.27, p = 0.02) (Figure 3(a) and (b)).

(a) Disability scores between the NPA and PA groups, (b) Pelvic Girdle Questionnaire scores between the NPA and PA groups, and (c) Fear-Avoidance Beliefs Questionnaire scores between the NPA and PA groups.

(a) Frequency of classified LPP disability between groups and (b) frequency of classified FABQ between groups.
ROC analysis was used to determine whether fear avoidance, measured with the FABQ, predicted nonspecific LPP. Results showed fair predictive ability (AUC = 0.724, 95% CI: 0.583–0.864, p = 0.002) (Figure 4). Furthermore, cutoff scores of 8 OR 14 appear to best balance sensitivity and specificity of the FABQ to accurately classify nonspecific LPP. A cutoff score of 8 on FABQ corresponds to a sensitivity = 65.2%, specificity = 33.3%, Youden’s index = 0.319. A cutoff score of 14 on FABQ corresponds to a sensitivity = 43.5%, specificity = 11.1%, and Youden’s index = 0.324.

Receiver operating curve for FABQ and LPP categorization.
Among all participants, higher moderate intensity physical activity MET min/week in the second trimester associated with lower ratings of back disability (rho(48) = −0.41, p = 0.003), pelvic girdle disability (rho(48) = −0.40, p = 0.004), and less fear avoidance (rho(48) = −0.27, p = 0.06), but not with pain intensity (ps > 0.05). Higher total weekly METs score, calculated from total PPAQ score (including all activity domains) associated with subjective reporting of higher pain severity when feeling “at their best” (rho(46) = 0.30, p = 0.04) and “at their worst” (rho(46) = 0.29, p = 0.047) but not with disability or fear avoidance (ps > 0.05).
When comparing groups on primary reported pain location (assessed via self-report; X2(4), N = 50, p = 0.061; Table 2), more NPA participants (n = 12, 46.2%) reported lower back pain than PA participants (n = 4, 16.6%), but more PA participants reported “other pain” (e.g., hip, upper back, n = 4, 16.7%) than NPA participants (0%). Both groups reported similar frequencies for PGP (NPA: n = 7, 26.9%, PA: n = 7, 29.1%) and for being pain free (NPA: n = 7, 26.9%, PA: n = 8, 33.3%). When comparing groups on positive provoked pain by location (assessed via the physical exam; X2(2) = 4.8, p = 0.09, Table 2), more NPA participants tested positive for PGP only (NPA: n = 9, 34.6%, PA: n = 5, 20.8%), combined LPP (NPA: n = 3, 11.6%, PA: n = 0, 0%), than PA participants. Reported pain location matched pain provocation testing 50.0% of the time with no differences in pain matching between groups.
Participant and group outcome measures.
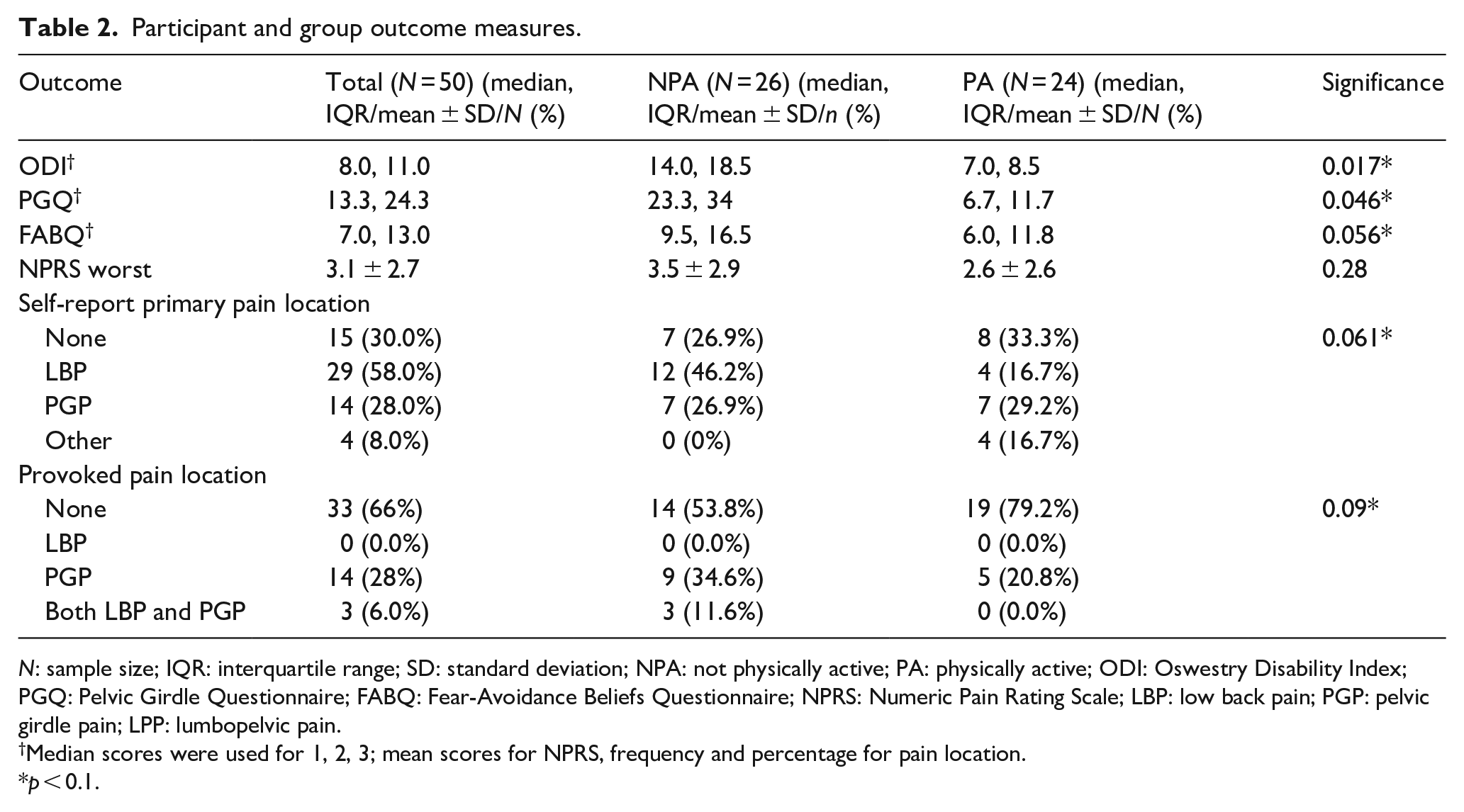
N: sample size; IQR: interquartile range; SD: standard deviation; NPA: not physically active; PA: physically active; ODI: Oswestry Disability Index; PGQ: Pelvic Girdle Questionnaire; FABQ: Fear-Avoidance Beliefs Questionnaire; NPRS: Numeric Pain Rating Scale; LBP: low back pain; PGP: pelvic girdle pain; LPP: lumbopelvic pain.
Median scores were used for 1, 2, 3; mean scores for NPRS, frequency and percentage for pain location.
p < 0.1.
Two potential confounding variables for LPP are BMI and parity. Prepregnancy BMI classification was not related to disability (ps > 0.05). Nulliparous participants had a lower incidence of PGP (OR: 0.16, 95% CI: 0.05–0.54, X2 (1, N = 50) = 9.15, p = 0.002), LBP (OR: 0.26, 95% CI: 0.07–0.94, X2(1, N = 50) = 4.47, p = 0.04), and nonspecific LPP (OR: 0.19, 95% CI; 0.06–0.63, X2(1, N = 50) = 7.78, p = 0.01).
Discussion
To our knowledge, this is the first study to investigate whether meeting exercise recommendations throughout the second trimester of pregnancy associates with less LPP, disability, and fear avoidance. This study also assessed pain subjectively (via questionnaire) and objectively (via a physical exam). Although pain severity did not differ between groups, pregnant persons who met exercise guidelines reported lower low back and pelvic girdle disability ratings and less fear avoidance than those in the non-active group. These findings highlight that maintaining exercise routines that meet current guidelines during pregnancy may be beneficial for reducing pain-related disability and fear avoidance behaviors and support the current ACOG guidelines.
The benefits of exercise for pain have been supported in multiple meta-analyses; however, the quality of evidence is tempered by methodological limitations and variability.3,38 Some randomized controlled trials found improvements in pain severity after an exercise intervention,36,39,40 while other randomized trials did not.41,42 The studies varied significantly in exercise volume, mode, intensity, and duration, which make it difficult to determine how exercise should be prescribed to be beneficial for pain. In this study, we found no difference between groups on pain severity; however, our findings may have been influenced by how we operationalized exercise. We categorized groups based on minutes of moderate intensity exercise. Therefore, we did not consider total daily physical activity, which includes activities such as cleaning, gardening, and childrearing.
Indeed, correlational data from our study found that higher total activity MET min/week, including all domains of daily activity, was associated with higher pain ratings whereas moderate intensity physical activity MET min/week did not associate with pain severity. Pain may be provoked more often from activities of daily living than from planned exercise movements. Fear of injury and pain are common barriers to exercise participation reported by pregnant persons. 43 Thus, better characterizing the relationship between types of physical activity and pain would help improve exercise participation in this population, which in turn could result in less fear avoidance and preserve their quality of life.
To begin to explore how to predict nonspecific LPP, we conducted an ROC analysis using The Fear Avoidance Beliefs Questionnaire with a cutoff score of 15 and found that a lower cutoff score of 8 is useful for properly classifying pregnant persons with nonspecific LPP. Clinicians should utilize the Fear Avoidance Beliefs Questionnaire to support a LPP diagnosis and understand that the standardized cutoff score may be too high to capture LPP avoidance patterns during pregnancy. Interestingly, we observed discrepancies between self-reported pain location and provoked pain during the physical examination in 50% of cases. Thus, although the use of objective pain provocation tests is important, self-reported questionnaires should be continued to be used and future research should further explore the underlying cause of these discrepancies.
Limitations
There were a few limitations in the design and implementation of this study. First, study staff were not completely blinded to participant grouping. The DPT who conducted the physical examination knew that participants reported being either physically active or not on the screening questionnaire as these were inclusion criteria for the study. However, she did not score the PPAQ (a different study staff member scored all questionnaire data). During data analysis, the DPT confirmed PA group classification for data analyses; however, this occurred after the physical examination. Second, this study was a cross-sectional study conducted at the beginning of the third trimester that correlated reported physical activity in the second trimester to pain in current pain outcomes. Pain tends to increase throughout pregnancy, and physical activity participation tends to decrease.1,20 Future studies should evaluate progression over multiple trimesters to observe a more complete relationship between exercise and pain over time. Third, the study was underpowered to statistically analyze each pain classification in isolation; therefore, despite the importance of classifying PGP and LPP separately, they were combined into nonspecific LPP. Additionally, the sample was primarily “pain free” individuals, with only 44% having a positive pain provocation test. Fourth, time of testing may have impacted the sensitivity of the tests because the physical examination was not performed at the time of day when an individual typically experiences the most pain. 44 Fifth, there is the possibility of sampling bias as the population was primarily white, highly educated, married, and of higher SES; therefore, the sample is not representative of the general pregnant population.
Conclusion
Meeting exercise guidelines by exercising a minimum of 150 min/week at moderate intensity throughout the second trimester of pregnancy associated with less reported low back and pelvic girdle disability, fear avoidance, and provoked pain in the third trimester. Total physical activity (which included everyday activities) associated with more reported pain whereas moderate intensity physical activity did not. Healthcare providers should include disability and fear avoidance ratings in evaluations of pregnant persons with any nonspecific LPP and encourage exercise during pregnancy to improve quality of life.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251321019 – Supplemental material for Meeting exercise guidelines during pregnancy associates with less lumbopelvic disability and fear avoidance
Supplemental material, sj-docx-1-whe-10.1177_17455057251321019 for Meeting exercise guidelines during pregnancy associates with less lumbopelvic disability and fear avoidance by Traci A McCarthy, Adrienne H Simonds, Sarah Velez and Andrea M Spaeth in Women’s Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057251321019 – Supplemental material for Meeting exercise guidelines during pregnancy associates with less lumbopelvic disability and fear avoidance
Supplemental material, sj-pdf-2-whe-10.1177_17455057251321019 for Meeting exercise guidelines during pregnancy associates with less lumbopelvic disability and fear avoidance by Traci A McCarthy, Adrienne H Simonds, Sarah Velez and Andrea M Spaeth in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.