
Abstract
Background:
Human immune virus (HIV) remains a major cause of death in children and women worldwide. Women’s desire to have children in the future has significant implications for the transmission of the human immune deficiency virus to sexual partners and newborns. People living with HIV desire to have children, and counseling by their healthcare providers plays a critical role in ensuring planned pregnancies and minimizing mother-to-child transmission. However, in many settings, a large majority of HIV-positive women who desire more children do not discuss reproductive health and childbearing with their healthcare providers. The objective of this study was to assess fertility desire and associated factors among reproductive age women living with a HIV attending antiretroviral therapy (ART) in public hospitals in Eastern Ethiopia.
Design:
Cross-sectional study.
Methods:
A facility-based cross-sectional study was conducted on November 01–30, 2022 among 598 reproductive age women attending ART clinics in public hospitals in Eastern Ethiopia. A systematic random sampling technique was used to select the participants. Data were collected from five female nurses through face-to-face interviews using a structured and pre-tested questionnaire. Data were entered into Epi-Data 3.1 and analyzed using IBM SPSS version 24. Bivariate and multivariable logistic regression analyses were performed. Variables with a p-value <0.25 in bivariate analysis were included in the multivariable logistic regression analysis. Variables associated with desire for fertility were declared at p-value <0.05, with adjusted odds ratio (AOR) and 95% confidence intervals (95% CI).
Results:
This study showed that 42.0% (95% CI: 31.7%–52.28%) of women had a desire for fertility. Women aged (15–24) (AOR = 2.52, 95% CI: 1.58–3.50), married women (AOR = 3.21, 95% CI 1.42–5.11), having no children (AOR = 1.94, 95% CI: 1.51–2.52), and desire to have children (AOR = 2.98, 95% CI: 1.84–4.12) were significantly associated with desire for fertility.
Conclusion:
This study revealed that a significant proportion of women desire fertility despite their positive status. Moreover, being young, married, having no child, and having a partner’s desire to have children were factors associated with the desire for fertility.
Introduction
Globally, an estimated 39.9 million people are living with human immune virus (HIV)/acquired immune deficiency syndrome (AIDS) in 2023. Of these, 38.6 million were adults and 1.4 million were children aged 0–14 years. More than half (53%) of the patients were female. 1 Even though health improvement has occurred with the advent of antiretroviral therapy (ART), resulting in intense reductions in HIV-related morbidity and mortality and improvements in quality of life, the number of new HIV infections has increased as a result of an increase in women’s desire for fertility. 2
People living with HIV like the general population desire to have children. 3 Women’s desire for fertility can put them in danger against preventive strategies for the vertical transmission of HIV/AIDS. Over 90% of HIV infections among young children worldwide are caused by mother-to-child transmission (MTCT). In the absence of appropriate intervention, the transmission of HIV/AIDS ranges from 15% to 45%. This transmission rate can be reduced to <5% with effective interventions during pregnancy, labor, delivery, and breastfeeding. 4
The burden of pregnancy among HIV-positive women is high in sub-Saharan Africa (SSA), where women in the reproductive age group account for 60% of all adult HIV infections. Among 1.4 million HIV-positive pregnant women in low- and middle-income countries, more than 90% were found in SSA. An estimated 430,000 children were newly infected with HIV in the same year, and over 90% of them were through MTCT. 5
Ethiopia has a generalized epidemic with an estimated adult prevalence of 0.9%, ranging from 4.7% in the Gambella region to <0.1% in the Somali region. The prevalence of HIV among women of reproductive age is 1.2%, which is higher than that among men (0.6%) of the same age. 6 The pooled prevalence of MTCT of HIV was 9.93%, and almost 1 in every 10 HIV-exposed infants became HIV-positive. 7
In countries like Ethiopia, the complex relationship between HIV/AIDS and the high fertility rate further threatens preventive strategies toward the vertical spread of HIV. Moreover, low preventing MTCT (PMTCT) coverage and poor integration with maternal services have been documented as the main challenges faced by the Ethiopian government. More than 30,818 (8%) mothers required PMTCT for HIV/AIDS, which could not be addressed in 2018. 8
To achieve the goal of an “HIV-free generation,” the need related to fertility desire of this population group must be prioritized, as many HIV-positive women continue to want to have children despite knowledge of their HIV status. However, Ethiopia seems far-reaching toward achieving the target to eliminate MTCT of HIV by 2025, with the current poor reproductive health outcomes such as a high prevalence of HIV among reproductive age women, a high total fertility rate (4.6%), and poor PMTCT outcomes. 9 In cases where people living with HIV desire to have children, counseling by their healthcare providers plays a critical role in ensuring planned pregnancies and minimizing the prevention of MTCT. However, in many settings, a large majority of HIV-positive women who desire more children have not discussed childbearing with their healthcare providers.10,11
Although different studies have been conducted in Ethiopia, they are old and current data are required for intervention, particularly in the eastern part of Ethiopia. No study has been conducted that points out desire for fertility and its associated factors among reproductive age women living with HIV. Therefore, this study fills this gap. The findings of this study could help to decrease new HIV infections, maternal and child morbidity, and mortality in the general population. The information obtained from this study can also be used for planning intervention programs by government officials and any other concerned bodies to design appropriate prevention and control strategies for MTCT of HIV.
Methods
Study settings
The study was conducted at public hospitals in Eastern Ethiopia. Among public hospitals providing ART services in Eastern Ethiopia, Dilchora, Haramaya, Jijiga, Hiwot Fana, and Chiro Hospital were included in this study. The study was conducted from November 01 to November 30, 2022. A total of 19,221 HIV-positive individuals were on ART follow-up at public hospitals of Eastern Ethiopia, among which 10,007 were women of reproductive age (15–49 years). 9 All stable clients attend the clinic every month. The ART clinics were providing counseling, tracing, ART treatment, and nutritional and medical treatment services.
Study design and study populations
A facility-based cross-sectional study was conducted among reproductive age women living with HIV attending ART clinics at public hospitals in Eastern Ethiopia.
Selected women of reproductive age (15–49 years) living with HIV attending ART clinics at public hospitals in Eastern Ethiopia were the study populations. Pregnant women, women with severe mental illness, women with confirmed inability to conceive, women who have had a hysterectomy, and those with incomplete records on cards were excluded from the study.
Sample size determination and sampling techniques
A sample size (610) was determined by single population proportion formulas, considering p = 63.9%, 12 95% confidence interval (95% CI), 5% of margin of error, design effect 2, and 10% non-response rate. A simple random sampling technique was used to select five hospitals from hospitals providing ART services. A total of 10,007 women of reproductive age living with HIV were enrolled and registered in ART registration at public hospitals of Eastern Ethiopia during the study period among which 4150 reproductive age women in selected five hospitals. Out of this, a total of 610 HIV-positive women aged 15–49 years in the ART clinic were enumerated and sampled from the sampling frame. Proportional allocation of the calculated sample size was applied to those selected hospitals. Participants were selected through a systematic random sampling technique in which (k = 7) (Figure 1).
Schematic presentation of sampling

Schematic presentation of sampling in a study of fertility desire and associated factors among reproductive age women attending ART at public hospitals in Eastern Ethiopia.
Study variables
Dependent variable
Fertility desire (yes/no)
Independent variables
Sociodemographic and individual factors (age, religion, ethnicity, educational status, occupation, marital status, residence, and monthly average family income)
Sexual and reproductive health-related factors (abortion, alive children, child’s biological sex, parity, sexual violence, sexual activity, sexual partner, partner desire, partner HIV status, history of sexually transmitted infection (STI), and discussion on Familiy planing).
HIV clinical status (CD4 count, viral load, ART duration, HIV diagnosis, HIV disclosure, partner HIV status, health status (having Diabetes mellitus, hypertension, chronic heart diseases), and existence of stigma)
Data collection procedures and data collection tools
After obtaining written informed consent, selected participants were asked to respond to an interviewer-administered questionnaire which was prepared in the local languages. The questionnaire assesses sociodemographic and socioeconomic characteristics, fertility desire, sexual and reproductive health characteristics, and clinical characteristics. Questionnaires were adapted from previously conducted similar studies and modified based on the objectives of this study 13 and were pre-tested on 5% of similar participants in hospitals not included in the study. Medical records of HIV-positive women were reviewed simultaneously to confirm the relevant medical history.
Data quality control
To ensure the quality of data the following measures were undertaken. The questionnaire was translated into local languages (such as Amharic, Afan-Oromo, and Af-Sumali languages) and back-translated into English. Pre-testing of the questionnaire was undertaken in 5% of women not included in the sample (at Sabiyan Hospital) before the actual data collection took place and corrections on the instruments were made accordingly. One-day training was given to all data collectors and facilitators. Data collection processes were supervised and collected data were checked for completeness, clarity, and consistency by the investigators as soon as submitted.
Data analysis
Data were cleaned, edited, coded, and entered into Epi-data version 3.1, software, then exported to IBM SPSS software version 24.0 for analysis. Descriptive statistics like frequencies, proportions, and summary statistics were used to describe the study population in relation to relevant variables. Multicollinearity between the independent variables was checked and model fitness was assessed. Binary Logistic regression was used to assess the presence of association between dependent and independent variables, and variables having p-value <0.25 were candidates for multivariable logistic regression. Adjusted odds ratio, p-value <0.05 with 95% CI were used to determine the significance and the level of association between dependent and independent variables.
Operational definition
Viral load
The amount of HIV in a sample of blood. The Viral load was reported as the number of HIV RNA copies per milliliter of blood. In this study, it had three categories. The first category was TND which means the target was not detected or the virus is not at a detectable level. The second and third categories were the detectable level which was <20 copies and ⩾20 copies of HIV RNA copies per milliliter of blood, respectively. 13
Results
Sociodemographic and individual characteristics of the study participants
A total of 598 women living with HIV attending ART participated in the study which gives a response rate of 98%. The mean age of participants was 28.5 years (with SD ± 9.5), and about 267 (44.6%) of respondents were in the age group of 25–34 years. Most, 472 (78.9%), of the respondents were urban residents, 236 (39.5%) of the participants were Oromo, and 239 (41.0%) of the participants were Muslim.
The majority, 508 (95.0%), of the study participants had formal education and 90 (5.0%) of them were lacking formal education. Half, 256 (50.4%), of the participants attended primary school and 186 (36.6%) of them had attended secondary school. Most, 355 (59.4%) and 430 (71.9%), of the participants were housewives and married, respectively (Table 1).
Sociodemographic characteristics of respondents on the study fertility desire and associated factors among reproductive age women living with HIV attending antiretroviral therapy at public hospitals in Eastern Ethiopia, 2022 (n = 598).

HIV: human immune virus.
Adare, Tigre, Hadiya, Walayita.
Sexual and reproductive health characteristics of the respondents
The majority, 468 (78.3%), of respondents were sexually active, among which all of them have had sexual practice in the last six months, of which 35 (7.5%) of them were with more than one sexual partner. Most, 285 (60.9%), of them used condoms, of which 200 (70.2%) used always during sexual intercourse. The main reason mentioned for the use of condoms, 120 (42.1%) reported that for dual protection, 90 (31.6%) to protect a negative partner, 40 (14.0%) fear of re-infection with a new strain of HIV, and 35 (12.3%) advised by health professionals.
About 7.4% (5.7%) and (1.7%) of the respondents have had a history of abortion before and after testing HIV-positive respectively. Moreover, 145 (24.2%) of the respondents have had a history of STI and its treatment. Most, 502 (84.0%), of the participants had information on the prevention of MTCT of HIV.
The majority, 555 (92.8%), of the study participants ever used contraceptives, among which 285 (51.4%) participants used condoms, 161 (29.0%) participants used oral pills, 180 (32.4%) participants used injectable, and 76 (13.7%) of participants used implants.
Similarly, 320 (53.5%) and 390 (65.2%) of the participants were currently using and plan to use in the future, respectively (Table 2).
Sexual and reproductive health characteristics of respondents on the study fertility desire and associated factors among reproductive age women living with HIV attending antiretroviral therapy at public hospitals in Eastern Ethiopia, 2022 (n = 598).

HIV: human immune virus; MTCT: mother-to-child transmission; STI: sexually transmitted infection.
HIV clinical status of the study participants
More than four-fifths (83.3%) of study participants were diagnosed (confirmed HIV+ status) 5 years back, and 354 (59.2%) of them were taking ART for more than 5 years.
About half, 290 (48.5%), of the participants were in a WHO clinical stage I, 290 (48.5%) of clients were their CD4 greater than or equal to 350/mm3 cell, and 139 (23.2%) of them were their viral load had not been detected. After taking ART, 539 (90.1%) of them had got improved health status, and 59 (9.9%) of them had not got improvement. The majority, 560 (93.7%), of the participants disclosed their HIV status to their family members. About 110 (18.4%) of the participants reported that there is still stigma because of HIV-positive status (Table 3).
HIV clinical status of reproductive age women living with HIV attending antiretroviral therapy at public hospitals in Eastern Ethiopia, 2022 (n = 598).

HIV: human immune virus; ART: antiretroviral therapy.
Fertility desire of the study participants
Four-fifths, 489 (81.8%), of the participants had living children; of which 189 (38.7%) of them had three or more children, 176 (36.0%) and 124 (25.3%) of them had two and one children, respectively.
In this study, the fertility desire of reproductive age women living with HIV and on ART was 252 (42.0%) [95% CI: 31.7%–52.28%]. Among participants who had the desire to have children, 63 (25.0%) of them needed to have one child, 112 (44.4%) of them needed to have two children, and 77 (30.5%) of them needed three or more children. The main reasons for the desire to have children in the future were: 109 (43.3%) wanted a child to replace themselves, 80 (31.7%) to achieve a desired number of children, 51 (20.2%) to get an HIV-free baby by using ART/PMTCT, and 12 (4.8%) others for reasons like to strength their marriage and replacing previously died baby. Of participants who had the desire to have children, 110 (43.7%) of them needed to have a child within 12 months, 63 (25.0%) within 12–24 months, and 50 (19.8%) within 24–36 months (Table 4).
Fertility desire of women in the reproductive age living with HIV attending antiretroviral therapy at public hospitals in Eastern Ethiopia, 2022.

HIV: human immune virus.
Factors associated with fertility desire
In bivariate logistic regression analysis: age, marital status, occupation, number of live children, having no child, child’s biological sex, partner HIV status, perceived health status, and partner desire to have children were found significantly associated with fertility desire. In a multivariable logistic regression analysis, only four variables were significantly associated with fertility desire, such as age, marital status, having live children, and partner’s desire to have children.
The odds of having fertility desire among women aged (15–24 years) were 2.52 times more likely to have fertility desire compared to women in the other age groups (adjusted odds ratio (AOR) = 2.52, 95% CI: 1.58–3.50). In this study, married women were 3.21 times more likely to have fertility desire than those women divorced/widowed/separated (AOR = 3.21, 95% CI 1.42–5.11). Women who had no children had almost two times higher odds of having fertility desire compared to women who already had one or more children (AOR = 1.94, 95% CI: 1.51–2.52). Moreover, this study demonstrated that women whose partners had a desire to have children were almost three times more likely to have fertility desire as compared to women who their partners had no desire to have children (AOR = 2.98,: 95% CI: 1.84–4.12) (Table 5).
Factors associated with fertility desire among reproductive age women living with HIV attending antiretroviral therapy at public hospitals in Eastern Ethiopia, 2022.
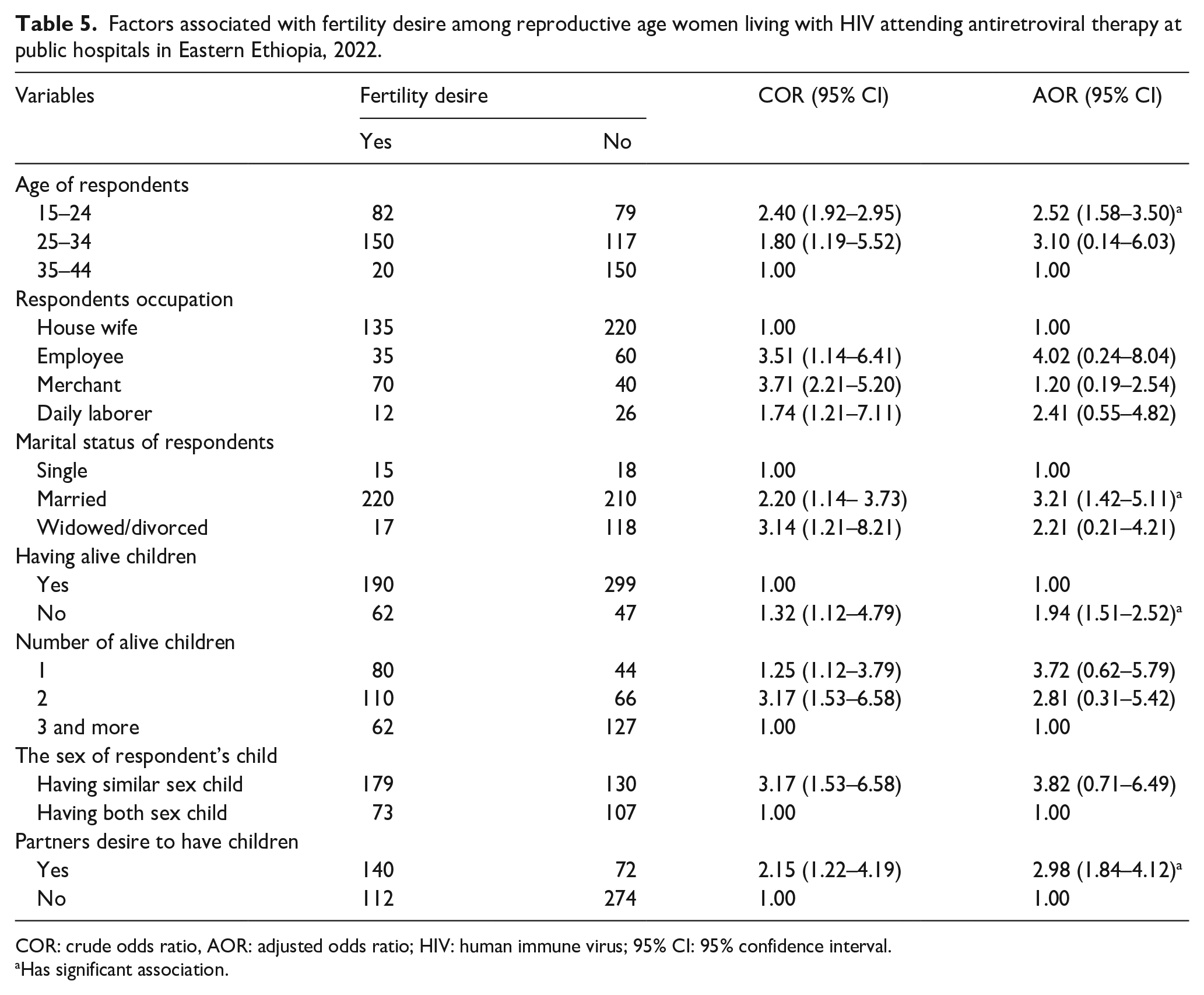
COR: crude odds ratio, AOR: adjusted odds ratio; HIV: human immune virus; 95% CI: 95% confidence interval.
Has significant association.
Discussion
Understanding the desire for fertility among women living with HIV/AIDS plays a significant role in reducing MTCT of HIV with the introduction of ART, which changes the views of childbearing despite having the disease. 14
The findings of this study revealed that the desire for fertility of reproductive age women living with HIV and on ART in the study area was 42% (95% CI: 31.7%–52.28%). This finding was almost comparable with those previous studies conducted in Tigray (45.5%), Addis Ababa (44%), and Adama (46.6%),15 –17 but higher as compared to the studies conducted in Tanzania 36%, 18 Malawi 17%, 19 and in south Wollo 15.7%. 20 This difference might be explained by the difference in sociodemographic characteristics of the populations and cultural differences in having large families. Moreover, the difference might also be due to the level of improvement in health services provision or awareness creation, particularly on PMTCT of HIV, across the study settings. The other possible explanation is a decrease in the level of stigma and discrimination toward people living with HIV in the current time to help them to utilize ART freely, which improves their health. However, this result was lower than studies conducted in the Harari region 52.9% 21 and in the Oromia regions 92.3%. 13 This could also be due to the time difference and better health service providers’ counseling about the risk of having a child on their health and the possibility of MTCT at the current time, which could decrease the level of desire to have a child.
In Ethiopia, studies have demonstrated an association between women’s age and desire for fertility. Young women living with HIV experience significantly more fertility desire than HIV-infected older women.12,15,16 Similarly, this study revealed that the odds of having a desire for fertility among young women (15–24 years) was 2.52 times more likely to have a desire for fertility than among women in the other age groups. This finding was in line with studies conducted in the Wolaita Zone 22 and other parts of Ethiopia.23-27 The possible similarity is that it is quite normal to have a desire for fertility during this period because it is the peak of reproduction. Another explanation could be that women’s ability to conceive decreases over time. However, a study conducted in Uganda indicated that being young was inversely associated with the desire for fertility.28-32 The possible reason for this inconsistency may be the sociocultural or methodological differences between the study participants.
In this study, married women were 3.21 times more likely to have a desire for fertility than divorced/widowed/separated women. This finding was similar to those of studies conducted in the Woreilu and Oromia regions of Ethiopia.29,30 This could be because being married created a sense of security and reliable support for raising children. However, this study’s result is opposite to the finding of a study conducted in Wolaita, Ethiopia, 22 which showed that married women had low desire for fertility. The possible explanations for these differences are not clear, but they are likely the result of using different source populations.
In most African communities, satisfying the desired family size, desire for biological children, maintaining the stability of the union, and sociocultural pressures are important reasons for continuing fertility desire among HIV-positive women.23,24 The findings of this study showed that women who had no children had 1.94 times higher odds of having a desire for fertility compared to women who already had children. Similar findings have been reported in studies conducted in Cape Town, South Africa, and Tanzania.3,18 The findings of this study are also in line with those of studies conducted in Nekemte town, Hossana town, Harari region, Gondar University Hospital, and Addis Ababa.16,21,29 –31 This may be due to the fact that those who do not have children need to replace themselves, and as in our culture, they need someone to take of them when they get old and weak. Another explanation could be that in some Ethiopian communities, a child is a prerequisite for a fulfilled and happy life. Partner desire might be due to children offering social security, maintaining family lineage, and satisfying emotional needs. 21
The results of this study demonstrated that women whose partners had a desire to have children were almost three times more likely to have a desire for fertility than women whose partners had no desire to have children. This is supported by evidence from other studies.16,21,23 This might be due to the presence of discussions about fertility issues among couples, since fertility issues are a concern of both couples or due to only men’s decision-making power (power imbalance) in the household.
Limitations of the study
Men were not included in the study despite their essential role in determining family size. This study is also limited to women who are receiving chronic, long-term care for their HIV infection, despite the desire for fertility differing from women who are not receiving care, which may bias the findings of this study. Moreover, this study lacked a comparison between HIV-positive and HIV-negative women.
Conclusion
The findings of this study showed that a significant proportion of women living with HIV and attending ART at public hospitals in the study area had a desire for fertility. This study revealed that being young, being married, having no child, and partners’ desire to have more children are factors associated with desire for fertility among women living with HIV attending ART in the study area. Therefore, service providers should strongly focus on counseling and prevention of MTCT of the HIV, with more attention paid to young and married women, women with no children, and women whose partners desire to have more children. Further studies including men and qualitative methods are recommended to obtain a deeper understanding of fertility desire among women living with HIV on ART follow-up.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251320481 – Supplemental material for Fertility desire and associated factors among reproductive age women attending antiretroviral therapy at public hospitals in Eastern Ethiopia
Supplemental material, sj-docx-1-whe-10.1177_17455057251320481 for Fertility desire and associated factors among reproductive age women attending antiretroviral therapy at public hospitals in Eastern Ethiopia by Legesse Abera, Betelhem Mengistu, Mickiale Hailu, Mawerdi Adem and Daniel Tadesse in Women’s Health
Footnotes
Acknowledgements
First and foremost, we would like to thank Dire Dawa University’s research affairs directorate for providing us the opportunity to conduct this research. Second, we would like to thank all hospitals administration for providing us with permission and different data to conduct this research. Third, we would like to extend our thanks to all data collectors for their contributions and study participants for their participation in this study.
Declarations
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.