
Abstract
Background:
Adequate gestational weight gain affects birth outcomes and increases the risk of non-communicable diseases later in life. Weight gain in pregnant Ethiopian women with hyperemesis gravidarum has not been investigated comprehensively.
Objective:
To assess the determinants of weight gain in pregnant women with hyperemesis gravida in Dire Dawa Administration, Eastern Ethiopia.
Design:
Unmatched case-control study
Methods:
Pregnant women who visited health facilities for ante-natal care were recruited into this study using random sampling techniques. The World Health Organization Global Physical Activity Questionnaire, FANTA Version III Women’s Dietary Diversity Score Questionnaire, and anthropometric measurements were used for the assessment of physical activities, dietary diversity, and gestational weight gain, respectively. Bivariate and multivariate logistic regression analyses with a 95% confidence interval (CI) and a Hosmer-Lemeshow goodness model were used to identify the determinants of gestational weight gain in the study population. A P value of <0.05 was considered significant.
Results:
A total of 657 pregnant women (219 patients and 438 controls) were included in this study. Among them, 44.3% and 47% of those in the patient and control groups, respectively, gained adequate weight during pregnancy (Std. 0.499: 95% CI: 42–49.8). Gravidity (adjusted odds ratio (aOR): 0.43, 95%CI: 0.22–0.81), planned pregnancy (aOR: 0.28, 95%CI: 0.11–0.69), and pre-pregnancy weight (aOR: 0.16, 95%CI: 0.72–0.74) were determinants of weight gain in the patient group, whereas the secondary level of education (aOR: 0.59, 95%CI: 0.36–0.97) and pre-pregnancy weight (aOR: 0.20, 95%CI: 0.08, 0.50) were determinants of gestational weight gain in the control group.
Conclusion:
The main determinants of gestational weight gain in women with hyperemesis gravidarum are gravidity, planned pregnancy, and pre-pregnancy weight. However, educational status and pre-pregnancy weight are the main determinants of gestational weight gain in women without hyperemesis gravidarum. Strengthening the nutritional life-cycle approach during pregnancy is important for ensuring that mothers maintain a healthy gestational weight.
Plain language summary
This unmatched case-control study was conducted to identify the determinants of weight gain in pregnant women with hyperemesis gravidarum in Eastern Ethiopia. The results of this study could inform the development of strategies for reducing the risk of insufficient gestational weight gain, especially in women with hyperemesis gravidarum.
The main aim of this study was to assess the determinants of weight gain in pregnant women with hyperemesis gravida in Eastern Ethiopia. We hypothesized that weight gain in pregnant women with hyperemesis gravida will be low.
Introduction
Nausea and vomiting are very common early symptoms of pregnancy, with 85% of women experiencing them during the first half of their pregnancy. Notably, between 30% and 35% of these women experience severe symptoms, a condition known as hyperemesis gravidarum. 1 Studies have indicated that hyperemesis gravidarum is the main reason for gestational weight catch-up up to the second trimester and that hyperemesis gravidarum is associated with nutritional deficiency during pregnancy.2,3 Preterm birth and low birth weight are unfavorable perinatal outcomes associated with hyperemesis gravidarum, which is also associated with poor maternal weight gain.4 –6
In pregnant women with hyperemesis gravidarum, inadequate total gestational weight gain and not regaining pre-pregnancy weight by weeks 13–18 are independent risk factors for delivering small-for-gestational-age (SGA) babies. 7 In addition, inadequate gestational weight gain has been suggested as the foundation of intrauterine growth restriction.8,9 A well-balanced diet that consists of satisfactory intake of energy, protein, vitamins, and minerals is necessary during pregnancy to meet the nutritional needs of the mother and the fetus. However, the fruit, vegetable, meat, and dairy intakes of several pregnant women are often insufficient to meet these needs and may lead to micronutrient deficiencies. Moreover, insufficient macronutrient and micronutrient intake is exacerbated by the presence of hyperemesis gravidarum during pregnancy. 10 Notably, poor maternal nutritional status leads to adverse pregnancy outcomes, such as low birth weight. 11
The energy requirements during pregnancy increase by an average of 300 kcal/day compared with pre-pregnancy requirements. However, sufficient energy and food intake during pregnancy is hindered by hyperemesis gravidarum,7,12,13 which is associated with inadequate gestational weight gain. Growing evidence from preconception nutrition trials has demonstrated that weight gain during pregnancy is associated with the size of the baby at birth. In addition, previous studies have shown that pre-pregnancy anemia and low pre-pregnancy weight are associated with an increased risk of low birth weight and SGA births. However, several important aspects of maternal nutrition before and during pregnancy remain unexplored. 14 The existing evidence suggests that women who have a high body mass index (BMI) in early pregnancy, frequently attend antenatal care (ANC) appointments, are employed, have a high income level, and consume diverse food items are likely to have an adequate gestational weight. 15 Insufficient income and easy access to low-fat foods are associated with inadequate gestational weight gain. 16 Notably, a previous study indicated that mother’s age, prepartum BMI, direct and indirect prenatal care, household size, food insecurity, stress, anxiety, stress and pregnancy-specific stress, as well as violence, have a positive and increasing effect on weight gain during pregnancy. 17
Cross-sectional studies conducted in different parts of Ethiopia have revealed that adequate gestational weight gain among pregnant women ranges from 27.9% to 67.2%.15,18,19 To address the issues related to gestational weight gain and nutritional problems in pregnant women, the government of Ethiopia has stressed the need for both nutrition-specific and nutrition-sensitive approaches to alleviating malnutrition and improving the nutritional statuses of women of reproductive age. In addition, the government promotes the incorporation of nutrition goals and actions into a wide range of sectors to prevent malnutrition in women of reproductive age. This strategy involves the adoption of a “life cycle” approach to addressing nutritional issues across life cycles and generations. Notably, noticeable differences in the adoption of national multisector nutrition plans, including a change in the perception of nutritional problems, have been observed among pregnant women in Ethiopia.20,21 However, the determinants of weight gain in pregnant women with hyperemesis gravida have not been well investigated in countries in the horn of Africa, including Ethiopia. Identifying the determinants of gestational weight gain is critical for the implementation of effective clinical interventions. Therefore, the aim of this study was to assess the determinants of weight gain in pregnant women with hyperemesis gravida in Dire Dawa administration, Eastern Ethiopia. The results of the study can facilitate the development of appropriate nutritional counseling focus points, monitoring interventions, and strategies for ensuring that pregnant women maintain an appropriate gestational weight.
Methods
Study design and setting
This was an unmatched case-control study conducted to assess the determinants of weight gain in pregnant women with hyperemesis gravida in Eastern Ethiopia. This study was conducted in government and private healthcare facilities in Dare Diwa, Eastern Ethiopia. There are two government hospitals (Sabian and Dilchora), four private hospitals (Bilal, Iftu, and Delt hospitals), five clinics, and nine government healthcare centers in Dare Diwa. All the healthcare facilities provide a full range of maternal, neonatal, and childcare services. The government healthcare facilities provide exempt services (ANC, postnatal care, immunization, labor and delivery, abortion, prevention of mother-to-child transmissions, and family planning) for the communities to promote the health of women and the communities. 22 The data used in this study were collected between September 10, 2023, and November 15, 2023.
Participants
All pregnant women who visited the Sabian General, Delt, and Iftu hospitals; Melkajebdu and Goro health centers; Ethiopia Family Guidance Association; and Dr. Desalegn Clinic were screened for recruitment into this study. The selection of participants to be included in the patient and control groups was based on the objective of this study. The participants eligible for inclusion into the patient and control groups were identified using the patient history data extracted from the ANC registers of the healthcare facilities and the follow-up charts of patients. The participants (patients and controls) were selected using simple random sampling techniques from the sampling frame, and their antenatal visit schedule data were collected.
The eligibility criteria for inclusion into this study were as follows: provision of consent to participate in the study, aged ⩾18 years old, first-trimester antenatal visit was scheduled at ⩽12 weeks of gestation, and mothers with a singleton pregnancy. Pregnant women who were unable to communicate during data collection and those whose anthropometric measurements indicated that they had deformities were excluded from the study.
The participants included in the patient group were selected from pregnant women with hyperemesis gravidarum who visited Sabian General, Delt, and Iftu hospitals; Melkajebdu and Goro health centers; Ethiopia Family Guidance Association; and Dr. Desalegn Clinics during the study period and were diagnosed with hyperemesis gravida. The participants included in the control group were selected from pregnant women without hyperemesis gravidarum who visited the abovementioned healthcare facilities during the study period.
Variables
The dependent variable analyzed in this study was weight gain in pregnant women, which was categorized as adequate or inadequate based on the 2009 guidelines presented by the Institute of Medicine (IOM). The independent variables analyzed were as follows: sociodemographic variables (age of the mother, type of occupation, employment status, and income), obstetric variables (pre-pregnancy weight, antenatal visit, number of births, presence of vomiting and nausea symptoms, presence of chronic disease, and nutritional status of the mother), dietary factors (dietary diversity practices of the mother), and behavioral factors (regular physical exercise, smoking, chewing khat, and drinking).
Hyperemesis gravidarum was diagnosed in the first 16 weeks of pregnancy if the mother presented with or reported nausea and vomiting, at least one of which was severe enough to impair sufficient food intake and affect activities of daily living. 23
Measurements
Anthropometric measurements
Pre-pregnancy weight was considered to have been measured at the first antenatal visit (before 12 weeks). Weight gain was calculated by subtracting the weight measured in the third trimester (at 37 weeks) from the pre-pregnancy weight measured at the first antenatal visit (before 12 weeks) and then compared with the recommended gestational weight gain proposed by the IOM. Pre-pregnancy BMI was calculated using the mother’s antenatal weight and height and classified according to the 2009 IOM guidelines as follows 24 : underweight, BMI < 18.5 kg/m2; normal weight, BMI of 18.5–24.9 kg/m2; overweight, BMI of 25.0–29.9 kg/m2; and obesity, BMI ⩾ 30 kg/m2. Inadequate weight gain was classified based on the pre-pregnancy BMI categories according to recommendations in the IOM guidelines: 12.5–18.0 kg for women who were classified as underweight, 11.5–16.0 kg for women who were classified as a normal weight, 7.0–11.5 kg for women who were classified as overweight, and 5.0–9.0 kg for women who were classified as obese(24). The height of each participant was measured to the nearest 0.1 cm using a portable stadiometer (Harpenden; CMS Weighing Equipment). During the measurement, each participant was instructed to place her head in the Frankfurt plane, knees straight, and heels, buttocks, and shoulder blades touching the vertical surface of the stadiometer (anthropometer) or wall. Weight was measured to the nearest 0.1 kg (after removal of shoes and heavy clothing) using calibrated electronic scales (Seca, Hamburg, Germany). The calibration of the scale at zero was checked before each use. These measurements were used for the calculation of BMI based on the established cutoff points.25,26
Dietary diversity assessment
The Food And Nutrition Technical Assistance Women’s Dietary Diversity version III (FANTA III) questionnaire was used for the assessment of dietary diversity among the participants.27,28 The total score was calculated by adding the number of food groups consumed by each respondent over a 24-h recall period. 29 Given that the total FANTA Version III scores were normally distributed, the scores were recoded as low and high based on the mean value.
Measurement of physical activities
The Global Physical Activity Questionnaire developed by the World Health Organization was used for the assessment of physical activity in this study. In addition to sedentary behavior, the three domains of the questionnaire (activity at work, travel to and from places, and recreational activities), which comprise 16 questions (P1–P16), were assessed. 30 In this study, we considered vigorous physical activities during pregnancy as activities that lasted for more than 2 h per day and caused a significant increase in breathing rate, such as construction work, baking or making enjera, daily activities that require energy and power, and washing clothes. Moderate-intensity physical activities were defined as activities that lasted for less than 2 h per day and caused a moderate increase in breathing, such as household or office activities. Physical activity data and the type, frequency, duration, and intensity of physical activity during work, transportation, and leisure in a typical week questionnaire were adopted from a previous study. 30 Non-significant variables were excluded from the analysis.
Controlling bias
To minimize selection bias in this study, the participants included in the patient and control groups were selected by carefully reviewing their diagnostic charts based on the eligibility criteria. To minimize measurement bias, each anthropometric measurement was taken three times, and the average value was used for analysis.
Sample size and sampling procedure
The sample size was determined using Epi-Info 7 under the following assumptions: proportion of exposed and non-exposed participants were 74.2% and 61.3%, respectively, 31 95% two-sided confidence interval (CI), power = 90%, and the ratio of exposed to non-exposed participants, 1:2. Based on these assumptions, the total sample size was calculated to be 219 patients and 438 controls. Considering a non-response rate of 5%, the total sample size required was 657 participants.
Based on these results, 30% of the healthcare facilities in Dare Dawa (n = 19) were selected for this study. Of 19 health facilities, seven (three government and four private) were randomly selected (three hospitals, two health centers, and two clinics) to acquire an adequate sample size. Thereafter, proportional sampling was performed, and the total number of participants selected from each facility was based on the average monthly attendance of the patients. A systematic sampling method was used for the selection of patients and controls from each health facility.
Data collection procedure and quality assurance
Data were collected using structured questionnaires and anthropometric data were collected using checklists. Weight measurements taken in the first trimester were extracted from each participant’s chart. In the third trimester (37 weeks and above), the weight of each participant was measured directly to calculate weight gain. Charts were reviewed for the extraction of data on weight measured in the first trimester and pre-pregnancy nutritional status. These data were collected during face-to-face interviews using a pre-tested and validated structured questionnaire from previous studies.3,15,28,30 The pre-test was conducted using 5% of the total sample. The questionnaires included questions on sociodemographic data, obstetric factors, diet, physical activity, and anthropometric measurements (weight and height). Weight and height were measured using standardized techniques and calibrated equipment.
Seven health professionals, who worked in the selected health facilities, collected relevant data from each facility within two months under continuous monitoring by trained supervisors. The data collectors underwent two days of training on interviewing techniques and questionnaire completion. Data clearance, range, and logic checks were conducted regularly to ensure data quality before data entry. Incomplete or inconsistent data were excluded from the analysis. The STROBE checklist for case-control studies was used to develop this manuscript. 32
Statistical analysis
The study data were checked for comprehensiveness and consistency. The cleared data were entered into Epi-data version 3.02 and exported to Social Package for Statistical Software (IBM SPSS) version 23. The main outcome variable, weight gain in mothers with and without hyperemesis gravidarum (patients and controls, respectively), was cross-tabulated using a custom table. Weight gain in the patient and control groups was cross-tabulated with different variables and presented in tables and graphs. Gestational weight gain was dichotomized into adequate and inadequate based on the IOM recommendations. To compare the differences in weight gain between the patient and control groups, the mean differences in bivariate data and proportional differences in categorical variables were analyzed using a chi-square test (X2 test). Dietary diversity practices were categorized into low and high dietary diversity based on the number of the 16 food groups in the FANTA III questionnaire consumed.
Bivariate and multivariate binary logistic regression analyses with 95% CIs were performed. A Hosmer–Lemeshow goodness-of-fit test model was used to identify the determinants of weight gain in the patient and control groups. Statistical significance was set at p < 0.05.
Results
Socio-demographic characteristics of the study population
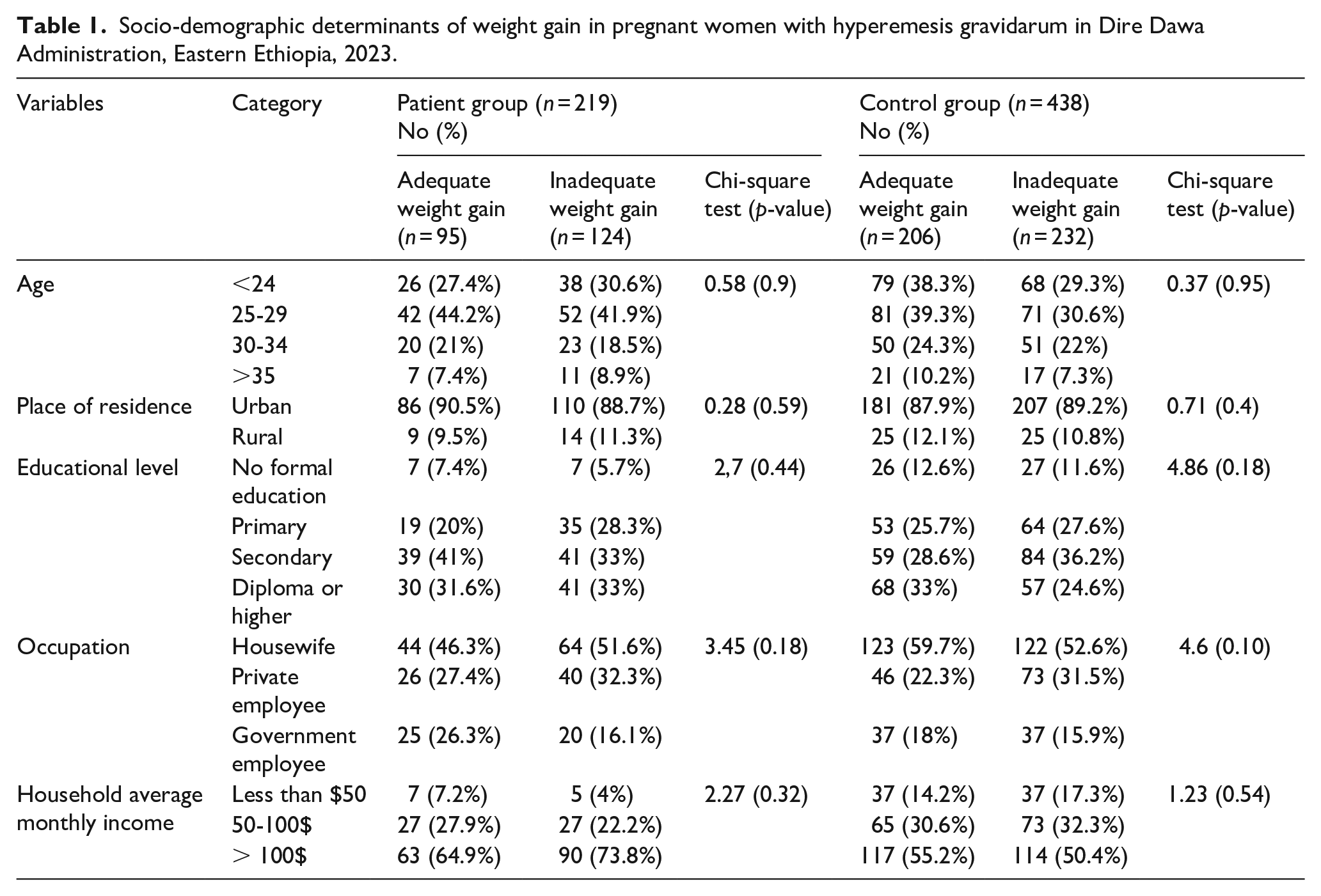
A total of 657 participants (219 patients and 438 controls) were included in this study. Among the participants, 44.2% of those in the patient group and 39.3% of those in the control group gained adequate weight (age range: 25–29 years). Regarding the occupation of the mothers, most of the government employees in both the patient (26.3%) and control (18%) groups gained adequate weight during pregnancy. However, 51.6% and 59.7% of the housewives in the patient and control groups, respectively, gained inadequate weight. Among participants with an average household income ⩾$100, 73.7% and 55.25% of those in the patient and control groups, respectively, gained inadequate weight. However, there was no statistically significant difference in weight gain between the patients and controls stratified according to age group, place of residence, marital status, educational status, mother’s occupation, and monthly average household income. The characteristics of the women in the patient and control groups are presented in Table 1.
Socio-demographic determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa Administration, Eastern Ethiopia, 2023.
Obstetric characteristics
There was a mean difference in weight gain between the participants who had planned pregnancies and who had unplanned pregnancies. In the patient group, 88.7% of the women who planned their pregnancy gained adequate weight (X2 = 5.1; p < 0.05). In the control group, the history of abortion in the last two years was associated with weight gain (X2 = 3.99; p < 0.05). In addition, there was a significant difference in mean weight gain between the women in the control group who had hypertension and those who did not (X2 = 4.45, p < 0.05). Furthermore, there was a significant difference in mean weight gain between women with chronic diseases and those without chronic diseases in the control group (X2 = 4.8; p < 0.05). However, there was a significant proportional difference between the pre-pregnancy weights of women in the patient and control groups (X2 = 5.86, p < 0.05 and X2 = 19.8, p < 0.05; respectively; Table 2).
Obstetric determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa Administration, Eastern Ethiopia, 2023.

Dietary diversity practices
Among the participants, 46.1% and 47.95% of those in the patient and control groups, respectively, showed low dietary diversity, whereas 53.9% and 52.1% of those in the patient and control groups, respectively, showed high dietary diversity. Overall, 47.3% of all the participants showed low dietary diversity, whereas 52.7% showed high dietary diversity (Figure 1).

Dietary diversity practices of all the pregnant women included in this study (patients, n=219; controls, n = 438).
Physical activity practices
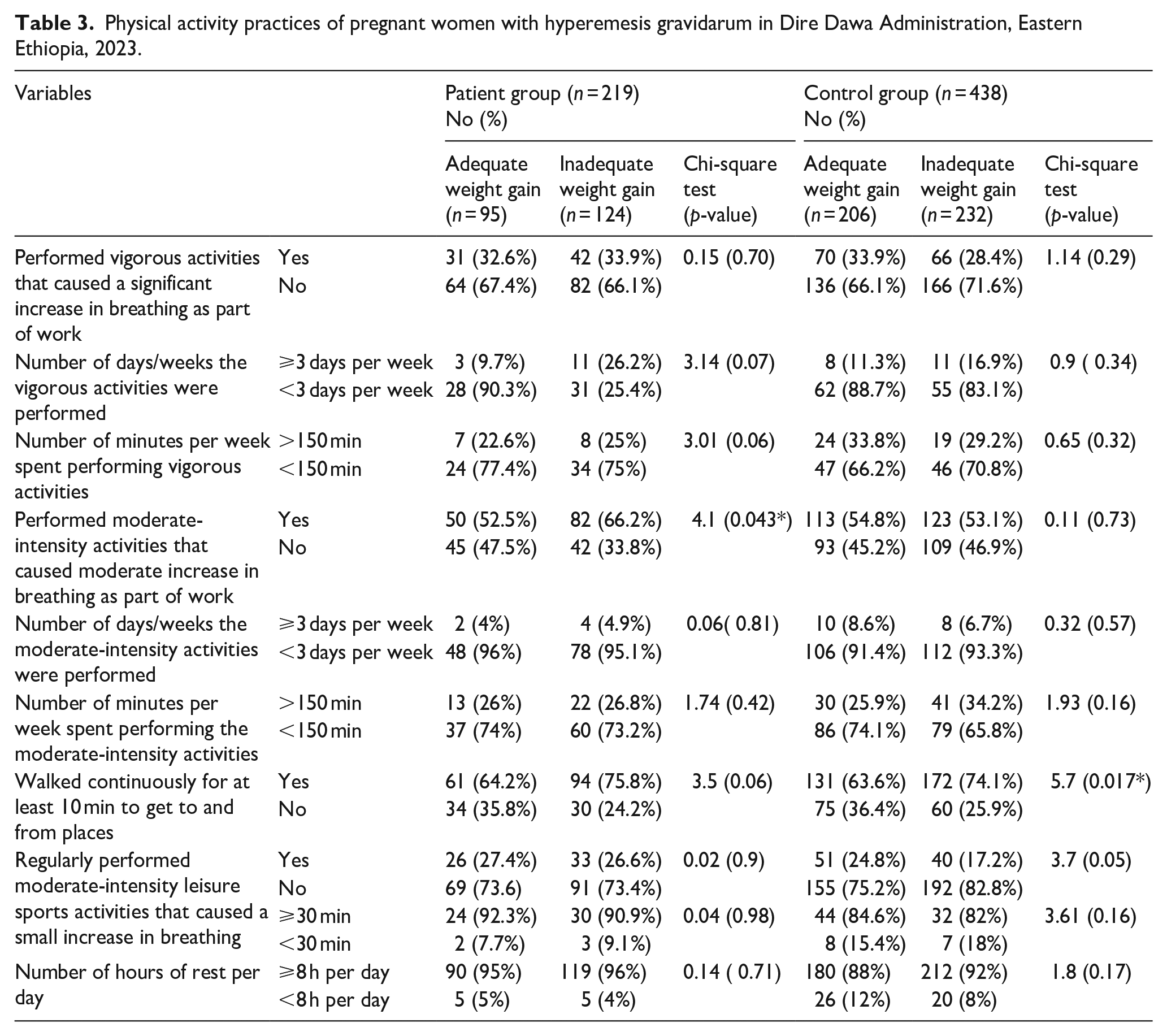
The majority (66%) of the women in the patient group who did not engage in vigorous physical activity gained adequate weight. However, of those in the control group who did not perform vigorous physical activities, 71.2% gained inadequate weight. Performing moderate-intensity physical activity was significantly associated with weight gain (X2 = 4.1, p < 0.05). In the control group, walking continuously for at least 10 min was associated with weight gain (X2 = 5.7, p < 0.05). Taking adequate rest, most of the participants in the patient and control groups had adequate rest for ⩾8 h per day (Table 3).
Physical activity practices of pregnant women with hyperemesis gravidarum in Dire Dawa Administration, Eastern Ethiopia, 2023.
Weight gain among the patients and controls
Analysis of the pre-pregnancy nutritional statuses of the women in the patient group indicated that 8.4% of the undernourished women, 83.2% of those with a normal weight, and 8.4% of the overweight women gained adequate weight, whereas 18.5% of the undernourished women, 77.4% of those with a normal weight, and 4% of the overweight women gained inadequate weight.
In the control group, 11.2% of the undernourished women, 79.1% of those with a normal weight, and 9.7% of the overweight women gained adequate weight, whereas 27.2% of the undernourished women, 68.1% of those with a normal weight, and 4.7% of the overweight women gained inadequate weight. Overall, 44.3% of the women in the patient group and 47% of those in the control group gained adequate weight during pregnancy (Std. 0.499; 95% CI: 42–49.8). In addition, 56.7% of the women in the patient group and 53% of those in the control group did not gain adequate weight (Std. 0.499; 95% CI: 50.2–58). Overall, 46% of the participants gained adequate weight, whereas 54% did not gain adequate weight (Figure 2).

Weight gain among the pregnant women included in this study (patient group, n = 219; control group, n = 438).
Determinants of weight gain among the women in the patient group
Binary logistic regression analysis showed that educational level, gravidity, planned pregnancy, abortion history, infection during pregnancy, presence of anemia during pregnancy, moderate physical exercise during pregnancy, and pre-pregnancy weight had a p value of < 0.25 in the patient group; therefore, these variables were included in the multi-variate logistic regression analysis. The multivariate logistic regression model indicated that multigravidae were 57% less likely to gain adequate weight than primgravidae (adjusted odds ratio (aOR) = 0.43; 95% CI: 0.22–0.81). The women with unplanned pregnancies were 72% less likely to gain adequate weight than those with planned pregnancies (aOR = 0.28; 95% CI: 0.11–0.69). Women who were underweight before pregnancy were 84% less likely to gain adequate weight during pregnancy than those who had a normal prepartum weight (aOR = 0.16, 95% CI: 0.72–0.74; Table 4).
Multivariate logistic regression analysis of the determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa Administration, Eastern Ethiopia, 2024.

Significantly associated with weight gain.
aOR, adjusted odds ratio; cOR, crude odds ratio.
Determinants of weight gain among women in the control group
Binary logistic regression showed that educational level, history of abortion, gestational hypertension, presence of chronic disease, walking for at least 10 min per day, and pre-pregnancy weight had a p value of <0.25; therefore, these variables were included in the multivariate logistic regression analysis. The multivariate logistic regression model showed that in the control group, pregnant women who had a secondary educational level were 41% less likely to gain weight during pregnancy than those with a diploma or higher (aOR = 0.59; 95% CI: 0.36–0.97). In addition, women who were underweight before pregnancy were 80% less likely to gain adequate weight than those who were overweight (aOR = 0.20, 95% CI: 0.08–0.50; Table 5).
Multivariate logistic regression analysis of the determinants of weight gain in pregnant women without hyperemesis gravidarum in Dire Dawa Administration, Eastern Ethiopia, 2024.

Significantly associated with weight gain.
cOR, crude odds ratio; aOR, adjusted odds ratio.
Discussion
Adequate gestational weight gain has a positive effect on pregnancy outcomes. In this study, 44.3% and 47% of the women in the patient and control groups, respectively, gained adequate gestational weight per the IOM recommendations. However, 56.7% of the women in the patient group and 53% of those in the control group did not gain adequate weight during pregnancy. Overall, 45.8% (95% CI: 42%–49.3) of the participants gained adequate weight, whereas 54.2% (95% CI: 50.7%–58%) gained inadequate weight. There were no significant differences in mean weight gain or the proportion of women who gained adequate weight between the case and control groups. This finding is similar to that of a study conducted in Iran, which indicated that 49.6% of the participants showed adequate weight gain during pregnancy. 17 In another study conducted in Malaysia, 47.2% of the pregnant women gained inadequate weight during pregnancy. 8
The proportion of women who gained adequate gestational weight in the present study is lower than that reported in a study conducted in Gondar, Ethiopia, wherein adequate gestational weight gain was observed in 65.12% of the pregnant women (95% CI: 60.08–69.85). 18 In an Egyptian study, adequate weight gain was observed in 81% of underweight pregnant women and 75.5% of women with a normal weight. 33 In Thai study, inadequate gestational weight gain was observed 12.99% of women analyzed. 34 The differences in these findings may be attributed to differences in population characteristics, study settings, dietary habits, lifestyle habits, access to healthcare facilities, healthcare follow-up systems, study design, and nutritional counseling. Notably, the proportion of women who gained adequate gestational weight in the present study is higher than that reported in a study conducted in Harare, Zimbabwe, wherein 69.3% and 28% of the women evaluated gained inadequate and adequate gestational weight, respectively. 15 In a study conducted in Addis Ababa, Ethiopia, 67.2% of the women gained inadequate weight (95% CI: 62.2–72.0%), whereas 27.9% gained adequate weight (95% CI: 23.4%–32.8%). 19 In Niger, low gestational weight gain was observed in 62.9% of pregnant women. 35 In a study conducted in Nigeria, 16.9% of women evaluated showed optimal gestational weight gain, whereas 26.9% gained insufficient gestational weight. 36 Another study conducted Iran revealed that 50% of the women gained inadequate weight during pregnancy. 37 The differences in the findings of these studies may be due to a lack of appropriate counseling in early pregnancy regarding the benefits of adequate gestational weight, economic disparities, and differences in access to healthcare between these populations. In addition, differences in sample size and study design may be possible reasons for these discrepancies in findings.
In the present study, a multigravida status (aOR = 0.43, 95% CI: 0.22–0.81) was identified as a determinant of weight gain. This finding is in line with that of a study conducted in Gondar, Ethiopia, which indicated that primigravidae have an increased risk for long-term weight gain because they gain the most weight during pregnancy, and that women with a high parity (4þ) have an elevated risk of long-term weight gain because they gain more gestational weight, irrespective of the amount of weight they gained during their previous pregnancies. 18
The present study revealed that being underweight before pregnancy (aOR = 0.16, 95% CI: 0.72–0.74) was a determinant of adequate weight gain. This finding is similar to that of a study conducted in Harare, Zimbabwe, which showed that adequate gestational weight gain is associated with a BMI of ⩾25 kg/m2 in early pregnancy (aOR = 3.2, 95% CI: 1.6–6.3). 15 In a study conducted in Addis Ababa, Ethiopia, being underweight was associated with weight gain (aOR = 3.30, 95% CI: 1.32–8.24). 19 Other studies have shown that pre-pregnancy weight (p < 0.001) (37) and pre-pregnancy BMI (aOR = 17.95, 95% CI: 8.13–36.95). 8 are significantly associated with gestational weight gain. The results of the present study indicated that planned pregnancy (aOR: 0.28, 95% CI: 0.11–0.69) was the main determinant of weight gain in the patient group. Notably, most previous similar studies did not indicate whether these variables are determinants of gestational weight gain. However, given that unplanned pregnancy is influenced by multiple factors, such as social support, economic readiness, and care, the results of the present study may be applicable to developing countries only.
In the control group, pregnant women who had a secondary school educational level were 41% less likely to gain adequate weight during pregnancy than those with a diploma or higher (aOR: 0.59, 95% CI: 0.36–0.97). Previous studies have indicated that a mother’s educational status is a determinant of adequate gestational weight gain.34,35,38 These findings may be related to the fact that as educated women are more likely to have paid work than uneducated women, women with a higher educational level are more likely to have the financial means to meet their nutritional needs during pregnancy. 39
The findings of this study indicated that in the control group, mothers who were underweight were 80% less likely to gain adequate weight than the overweight mothers (aOR: 0.20, 95% CI: 0.08–0.50). Studies conducted in different parts of Ethiopia have indicated that women who were underweight before pregnancy gained gestational weight below the IOM recommendations.18,19 Notably, findings from different continents indicate that pre-pregnancy nutritional status is the main determinant of adequate weight gain during pregnancy.17,36,37 In the present study, being underweight before pregnancy was an independent risk factor for inadequate gestational weight gain in both the patient and control groups. However, the difference between the gestational weight gain observed in the patient and control groups was not statistically significant. The main implication of this finding is that in both women with and without hyperemesis gravidarum, being underweight before pregnancy increases the risk of inadequate gestational weight gain, which in turn increases the risk of maternal complications and poor pregnancy outcomes. These findings can be used as the focus of interventions for promoting adequate weight gain and can be served as a baseline for further research.
Strengths and limitations
This study is valuable in that it is the first case-control study conducted to assess the determinants of weight gain in pregnant women with hyperemesis gravidarum in Ethiopia. In addition, the sample size of both the patient and control groups is adequate. Furthermore, sampling bias was minimized in this study by selecting more than 30% of the healthcare facilities in Dare Diwa. Moreover, a control group was included to ensure the internal validity of the study.
The main limitation of this study is that gestational weight gain was classified based on the IOM gestational weight gain recommendations, which were established for developed countries and may not be applicable to developing countries such as Ethiopia. In addition, the possibility of measurement errors by the data collectors cannot be completely ruled out. Furthermore, the medical interventions administered to the participants were not assessed, and some of their pre-pregnancy weights were self-reported. Moreover, the lack of comparability of our findings with those of other studies of the same design is a notable limitation of this study.
Conclusion
This study demonstrated that gravidity, planned pregnancy, and pre-pregnancy weight are the main determinants of gestational weight gain in pregnant women with hyperemesis gravidarum, whereas the educational status of the mother and pre-pregnancy weight are determinants of weight gain in pregnant women without hyperemesis gravidarum. These findings indicate that advocacy for nutritional behavioral changes and strengthening the nutritional life-cycle approach in pregnant women are important for ensuring adequate weight gain during pregnancy.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251318193 – Supplemental material for Determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa administration, Eastern Ethiopia: An unmatched case-control study
Supplemental material, sj-docx-1-whe-10.1177_17455057251318193 for Determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa administration, Eastern Ethiopia: An unmatched case-control study by Tariku Derese Asfaw, Yibekal Manaye and Mahder Girma in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251318193 – Supplemental material for Determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa administration, Eastern Ethiopia: An unmatched case-control study
Supplemental material, sj-docx-2-whe-10.1177_17455057251318193 for Determinants of weight gain in pregnant women with hyperemesis gravidarum in Dire Dawa administration, Eastern Ethiopia: An unmatched case-control study by Tariku Derese Asfaw, Yibekal Manaye and Mahder Girma in Women’s Health
Footnotes
Acknowledgements
We thank Dire Dawa University for monitoring the credibility and authentication of the research paper and the Dire Dawa Regional Health Department for their optimistic cooperation during the data collation procedure and ethical authorization process. We would like to thank Editage (www.editage.com) for English language editing. We also thank all the data collectors and study participants.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.