
Abstract
Postpartum fatigue (PPF) is a common issue affecting mothers, characterized by reduced capacity for physical and mental activity in the weeks to months following delivery. While often attributed to the demands of infant care, severe or atypical PPF can signal an underlying medical condition, such as multiple sclerosis (MS). In this narrative review, guidance is provided to clinicians on recognizing signs of severe or atypical PPF, differentiating it from MS-associated fatigue. Patients’ qualitative descriptions of fatigue, its intensity, and specific triggers can be particularly informative, as MS fatigue is severe, recurrent, often refractory to rest, and/or exacerbated by high temperatures. By identifying such cases early, healthcare providers can support timely diagnosis and intervention, ultimately improving outcomes for women who may be at risk for MS.
Introduction
Postpartum fatigue (PPF) affects up to 64% of mothers, making it the most common problem women experience after childbirth 1 —even if its significance in women’s lives may be ignored. 2 PPF is defined as reduced capacity for physical and mental activity in the weeks to months following delivery. Experientially, it entails a persistent lack of energy, a feeling of being overwhelmed, and difficulty concentrating not easily relieved by rest or sleep. 3 Though PPF most directly results from disrupted sleep due to night-waking infants and/or night-time feeding, 4 it is also correlated with postpartum stress, anxiety, and breastfeeding problems.5 –8 PPF is a normal response to the lifestyle change of caring for a new baby and usually improves within a few weeks or months as the body adjusts to post-birth changes and as the infant establishes a regular feeding pattern.
Occasionally, however, fatigue in the postpartum period can also indicate a chronic, underlying health condition—like multiple sclerosis (MS). Certainly, not all PPF is MS—in medical jargon, MS is the zebra and PPF the horse. However, PPF may present with some stripes, and recognizing these could support early recognition of conditions like MS with life-altering implications. Furthermore, the postpartum period provides a critical opportunity for surveillance because for some women it serves as the sole time that they will receive consistent follow-up healthcare. Therefore, a detailed history of the patient’s health prior to delivery is crucial when PPF is more severe or atypical to avoid must-not-miss diagnoses such as MS. The goal of this narrative review is to provide guidance for clinicians caring for women in the postpartum period in how to recognize signs that PPF is more severe or atypical and reflective of an underlying condition. This includes features of the patient’s presentation as well as from a detailed history of health prior to delivery.
Methods
For this narrative review, a search was performed of English language, peer-reviewed publications on pubmed.gov. The first phase focused on qualitative studies of PPF, then on MS fatigue. Studies were selected based on their relevance to PPF, including factors contributing to fatigue, its prevalence, and potential long-term implications. The reference lists for each article were reviewed for additional relevant articles. The search was expanded to include diverse perspectives on maternal health, sleep patterns, and psychological stress. Then, studies addressing fatigue in MS were reviewed, given the overlapping symptoms and potential insights into the management of fatigue in postpartum women. An emphasis was placed on signs and symptoms present in the MS prodrome and on those that would distinguish MS-related fatigue from PPF.
Discussion
MS is an autoimmune, demyelinating disease of the central nervous system, most commonly diagnosed in women ages 20–40, that is, in their peak reproductive years. 9 Fatigue is the most common symptom of MS, reported by at least 75% of people with MS (PwMS) at some point in the disease course 10 and has a major impact on quality of life: 55% PwMS identify it as one of their worst symptoms. 11 Fatigue can be experienced far before onset of clear demyelinating symptoms and is considered part of the MS “prodrome.” “Vague,” less specific prodromal MS symptoms and signs are recognized as occurring up to 5 years prior to a first clearly recognized clinical attack.12 –17 These can include migraine, pain, sleep disturbance, bowel or bladder issues, anemia, and other complaints, and lead to increased use of healthcare services, 13 including up to 49% increased use of prescription medications 14 and up to 50% increased utilization of mental health services (visits to psychiatrists 13 ) in the 5 years preceding MS “onset.” With relevance to pregnancy, the MS prodrome may influence a woman’s subsequent childbearing. In the 5 years prior to MS symptom onset, women with MS have been reported to have a lower likelihood of becoming pregnant and a higher likelihood of using oral contraceptives than controls. 14 These findings suggest a behavioral shift occurring whereby women consciously or subconsciously forego or delay pregnancy when experiencing prodromal MS symptoms. Fatigue in particular is a very common prodromal symptom: one study of nearly 17,000 PwMS found that 28.9% were labeled with chronic fatigue syndrome or generalized malaise or fatigue prior to MS diagnosis 18 ; similarly, another study showed that fatigue predated other MS symptoms in a third of patients. 19 Thus, fatigue can herald MS, sometimes even by years.
In the setting of pregnancy, MS inflammatory activity increases in the first 3 months postpartum, 20 where up to half of untreated women can develop new demyelinating injury on MRI with or without associated clinical relapses.21,22 Therefore, occasionally severe, unexplainable fatigue following childbirth could indicate early MS disease activity. PPF can in turn inherently worsen a mother’s quality of life, as PPF is associated with increased anxiety, 7 reduced sense of competency and esteem in parenting abilities, 23 and completely weaning before infants are 6 months old. 24 PPF is also strongly correlated with postpartum depression, 25 which is associated with weaker mother–infant bonding. 26
This review has limitations, primarily due to the paucity of literature on PPF. Furthermore, the lack of standardized measures for assessing PPF also hinders comparisons with the well-documented metrics used in MS fatigue studies. Additionally, the absence of patient-reported experiences of PPF in existing studies restricts insights into its day-to-day impact, making it harder to draw specific distinctions from the more persistent nature of MS fatigue. Despite these constraints, we have endeavored to prepare clinicians to distinguish PPF from MS fatigue by describing the severity of MS fatigue.
To support early distinction of fatigue associated with MS from PPF, patients’ qualitative reports can be informative. MS fatigue is described as excessive whole-body tiredness that often is not relieved by sleep or explained by anything else; PwMS can wake up after a full night of sleep just as exhausted as before they went to bed. MS fatigue is further depicted as an “ever-present, ongoing experience” that can feel like “being hit by a tidal wave” 27 or “wearing a giant sandbag.” 28 Thus, the intensity of MS fatigue is greater than that of “typical” PPF, which can most often be alleviated quite well with rest or sleep. Additionally, MS fatigue is worsened by high temperatures,19,29 another factor that can distinguish it from usual PPF (Table 1). While thyroid disease, rheumatoid arthritis, systemic lupus erythematosus, 30 fibromyalgia, 31 depression, 32 malignancy, 33 and even viral infections 34 can similarly cause severe, unrelenting fatigue, a careful history of MS predictors and remote, episodic neurological symptoms can help distinguish these from MS.
Signs and symptoms that could indicate MS in a patient with postpartum fatigue.
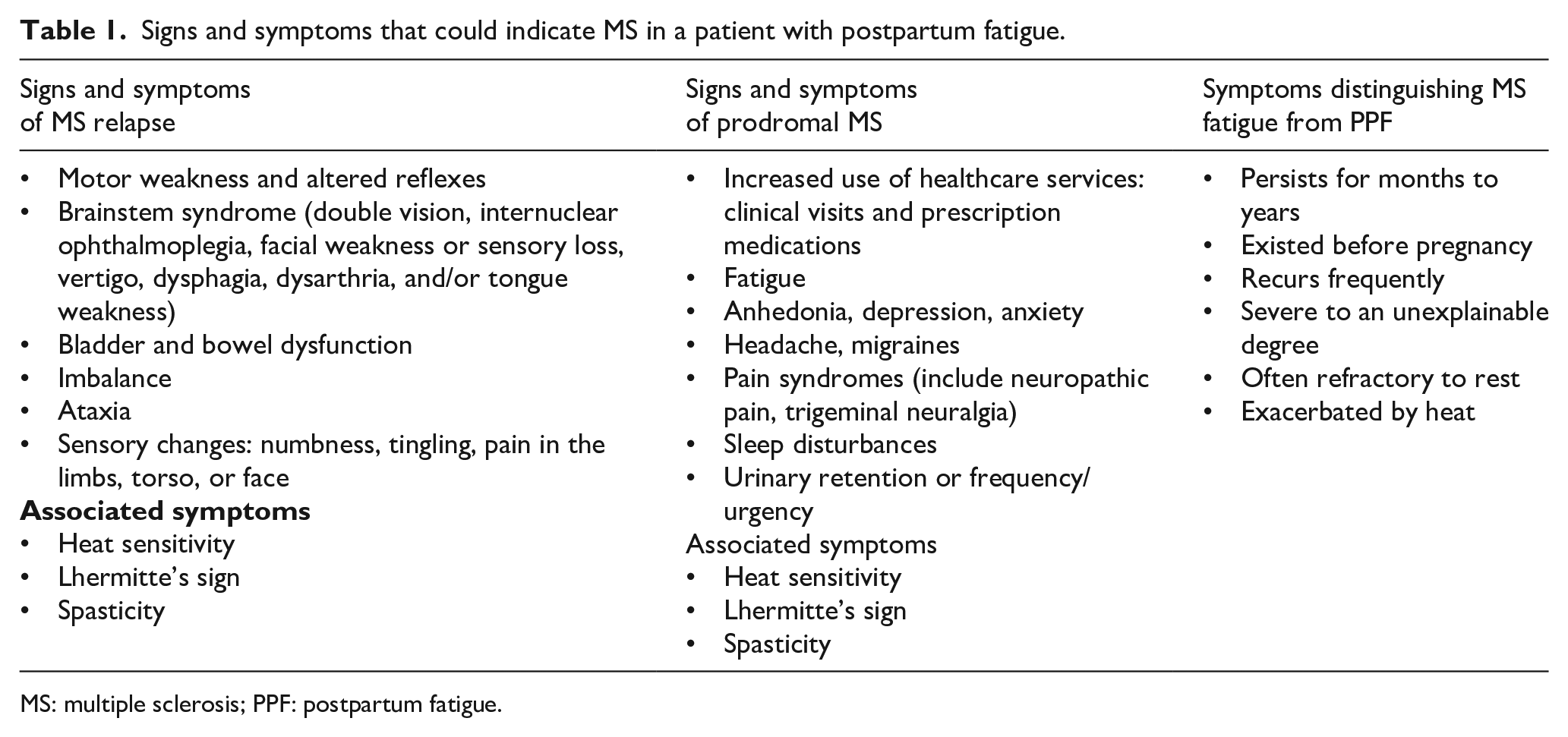
MS: multiple sclerosis; PPF: postpartum fatigue.
Conclusion
The dramatic improvements in MS outcomes observed in recent decades can be attributed to earlier recognition of MS symptoms and diagnosis, as well as earlier initiation of more effective disease modifying therapies to prevent ongoing disease activity, slow disease progression, reduce symptom severity and impact, and improve quality of life. Given that MS most often presents in women during their childbearing years, for many women, the postpartum period may represent not only a particular period of vulnerability, but also a period where more consistent healthcare coverage is provided. Fatigue is extremely common in MS and is the prodromal symptom that can be most easily disregarded in new mothers. To aid busy clinicians who are managing myriad postpartum health concerns, qualitative assessments of fatigue intensity and a comprehensive exploration of signs of prodromal MS or histories of episodic neurological symptoms is encouraged when patients present with PPF that is severe, recurrent, often refractory to rest, or exacerbated by high temperatures (Figure 1). Ultimately, such inquiries could help uncover the occasional zebras for whom further disability can be prevented.

Graphic aid to distinguish PPF from multiple sclerosis-related fatigue. PPF that is severe, recurrent, often refractory to rest, or exacerbated by high temperatures in the setting of an increased use of healthcare services and other systemic and neurological symptoms warrants a multiple sclerosis workup.