
Abstract
Multiple sclerosis (MS) is a chronic autoimmune condition causing damage to the protective covering of nerves in the central nervous system. Pediatric multiple sclerosis is a rare form of the disease that affects 3–5% of individuals with multiple sclerosis. Pediatric Onset Multiple Sclerosis (POMS) has a rather different clinical profile from the more prevalent adult multiple sclerosis. Alongside the classic symptoms of multiple sclerosis, children tend to present with various atypical symptoms that can impact motor milestones, speech development, and cognitive functions. This review aims to explore the pathogenesis, clinical features, diagnosis and progression of Pediatric Onset Multiple Sclerosis into adulthood, address the challenges accompanying this transition and identify strategies and therapies to overcome them. Pediatric multiple sclerosis patients transitioning into adulthood face many challenges, such as difficulty in school and social life, and dealing with uncertainties especially due to changes in healthcare providers from pediatric to adult settings. These challenges can be overcome by an emphasis on a well-structured transition plan, early planning, personalized care, proper counselling of the patient as well as the family and caretakers, a multidisciplinary approach with good communication and coordination between all healthcare personnel a robust support network with a gradual transition rather than an abrupt one. Proper care during the transition period is crucial to enhance patient adherence and deepen the understanding of the disease for both patients and their families. This will empower them to seek timely assistance when needed, reduce loss to follow-up, and ultimately improve overall quality of life.
Keywords
Introduction: bridging the gap
Pediatric onset Multiple sclerosis (POMS), also known as early-onset multiple sclerosis or juvenile-onset multiple sclerosis is generally defined as multiple sclerosis with an onset before the age of 16 years. Of people diagnosed with multiple sclerosis, < 1% are under the age of 10 years and 3–10% are under 16 years of age. 1 As per epidemiology meta-analysis data pediatric multiple sclerosis incidence ranges from 0.05 to 2.85 per 100,000 individuals annually and the overall prevalence ranges from 0.69 to 26.92 per 100,000 individuals. 2 Pediatric onset Multiple sclerosis differs from adult-onset multiple sclerosis as the interval to next relapse is longer in pediatric patients as compared to adult patients and 50% risk of reaching EDSS 3 and 6 takes longer than in adult patients though happens at a relatively younger age. 3 Better neuroplasticity in children prevents the development of irreversible physical disability in Pediatric onset Multiple sclerosis. 4
Multiple sclerosis is a chronic illness that starts in childhood and continues till adulthood. So, a patient needs to shift from his pediatric healthcare provider to an adult setting and this is where transition happens and needs to be taken care of. Appropriate transition can educate youth regarding the importance of adherence and its benefits for improved clinical outcomes. 5 A year-long study on seventeen pediatric multiple sclerosis patients regarding their transition to adult healthcare services revealed that they did not receive any medical care during this transition period. 6
It should always be kept in mind that health care transition is a slow process and is not a single-time event. Cessation of pediatric care in the absence of adult health care transition leads to a gap in continued health services and can be of dreadful consequence which otherwise would have been prevented by merely enrolling, guiding, and proper training to transition to adult health care services. This review article frames the outline required for a smooth transition as well as its adherence by the youth so that their lifelong well-being can be maintained.
Epidemiology: understanding the landscape
MS is widely recognized as the most common demyelinating disease, particularly in high-income countries, where its burden is most pronounced. The global median prevalence of MS has risen over recent years, reaching a rate of 35.9 per 100,000 individuals in 2020. 7 However, the prevalence of MS varies significantly across the different regions of the world, with the highest rates observed in North America, where it affects approximately 140 per 100,000 people, and in Europe, with a prevalence of 108 per 100,000. 8
In the United States alone, nearly 1 million individuals have been diagnosed with MS, as reported in a 2019 prevalence study funded by the National MS Society. This figure represents more than double the estimates from previous studies. On a global scale, MS organizations estimate that approximately 2.8 million people are affected by the condition, highlighting the significant global burden posed by MS. 9
An analysis of the prevalence of MS across different racial and ethnic groups reveals significant disparities. White individuals exhibited the highest prevalence, with 374.8 cases per 100,000. Following them, Black individuals had a prevalence rate of 298.4 per 100,000. In contrast, Hispanic individuals showed the lowest prevalence among the groups analyzed, at 161.2 per 100,000. These differences highlight significant health disparities that may inform targeted prevention and intervention strategies for multiple sclerosis across diverse populations. 10
The majority of individuals with MS receive their diagnosis between the ages of 20 and 40; however, approximately three to five percent of MS cases are diagnosed in children. 11 In recent years, the recognition and diagnosis of pediatric-onset MS has grown considerably in recent years, reflecting an increased awareness of the disease in younger populations. Currently, over 30,000 cases of MS have been identified in individuals under the age of 18 across 47 different countries. This marks a significant rise in reported cases compared to previous years. For instance, in 2013, only around 7000 cases of pediatric-onset MS were documented by 34 countries, highlighting a notable expansion in both diagnostic efforts and data collection in this age group. 7
Pathogenesis: unraveling the complexity
MS is a complex chronic inflammatory heterogeneous disease that affects the central nervous system (CNS) that leads to extensive demyelination in the white matter with axonal, neuronal and astroglia injury. 12 The exact etiology of MS remains unclear, but it is generally understood to be a multifactorial condition influenced by genetic predispositions and environmental factors that contribute to the abnormal immune response.
While no specific genes are definitively linked to MS susceptibility, the HLA region on chromosome 6 is a key associated locus. Other genes, such as those related to interleukin-1β and apolipoprotein E, are linked to disease progression but require further validation. 13
Environmental factors, such as infectious diseases and vitamin D deficiency, play a significant role in MS pathogenesis. Pathogens like human herpesvirus 6 (HHV-6) and Chlamydia pneumoniae may trigger autoimmune responses, but no single infectious agent has been confirmed as a root cause, suggesting a multifactorial process. 13 Similary, Vitamin D deficiency is critical, with higher MS prevalence in regions with lower UVB exposure. Low vitamin D levels, combined with reduced dietary intake and limited outdoor activity, have been associated with an increased risk of MS, particularly in individuals with genetic variants that lead to lower vitamin D levels. 14
In MS, the inflammation in both the gray and white matter are essentially the origin of the damage. T cells become abnormally reactive, targeting self-antigens in the CNS, which leads to both cellular and humoral immune responses that harm myelin, oligodendrocytes, and neurons. 14 This autoimmune process begins when antigen-presenting cells (APCs) present antigens bound to major histocompatibility complex (MHC) molecules. T cells recognize these antigens using their T cell receptors (TCR) and co-receptors like CD4 or CD8, while also interacting with co-stimulatory signals from the APCs. Helper T cells are critical in MS (especially Th1 and Th17) because they activate and mature other immune cells, such as B cells, cytotoxic T cells (CTLs), macrophages, and neutrophils. After migrating into the CNS, T cells must undergo reactivation by APCs, such as macrophages or microglia, in order to sustain their damaging activities. 15
Figure 1 illustrates Intercellular adhesion molecule-1 (ICAM-1) – Vascular cell adhesion molecule-1 (VCAM-1) – Central nervous system (CNS) – Blood–brain barrier (BBB) – Tumor necrosis factor-alpha (TNF-α) – Interleukin-1 (IL-1) – Integrin very late antigen-4 (VLA-4) – Stromal cell-derived factor-1 (SDF-1) – Lymphocyte function-associated antigen-1 (LFA-1) – Interferon-gamma (IFN-γ) – TNF-beta (TNF-β).
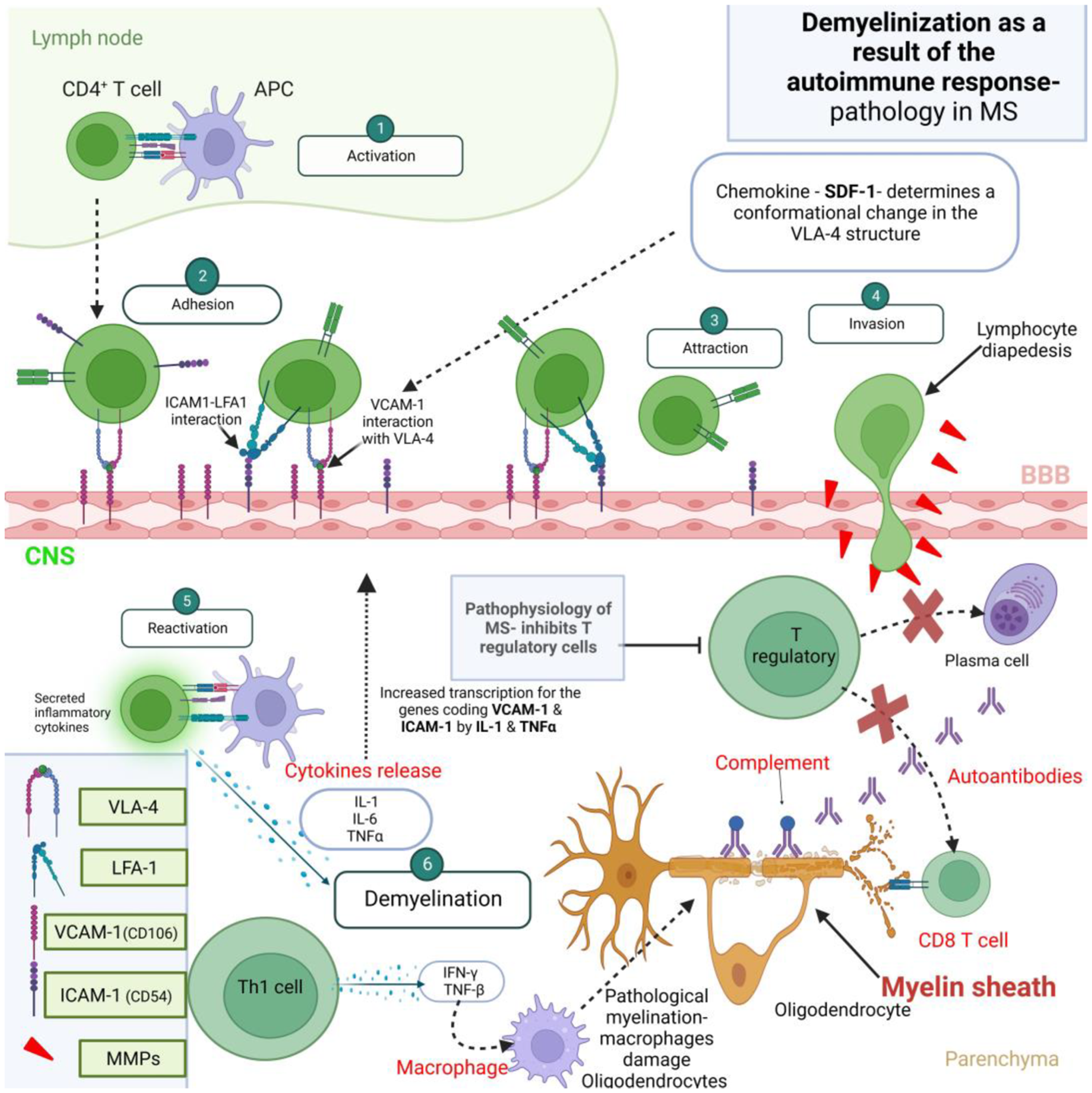
Demyelinization as a result of the autoimmune response – Pathology in MS. 16
Clinical features: a comprehensive profile
MS in children often presents with distinct symptoms compared to adults. While the classic triad of optic neuritis, transverse myelitis, and brainstem demyelination may occur, children frequently experience more subtle or atypical manifestations. 3 MS can impact motor milestones, speech development, and cognitive function, and children may exhibit irritability, mood swings, or difficulty concentrating. Academic performance may be affected due to fatigue, mental challenges, or visual impairments. Muscle stiffness and tightness can interfere with daily activities and mobility, and numbness, tingling, or pain can be experienced in different body parts. It is essential to address these mental health challenges early to support the overall quality of life for pediatric patients.17,18 A child's developmental stage significantly influences how they perceive and express MS symptoms. Younger children may have difficulty articulating their experiences, relying on parents or caregivers to report changes. As children mature, they become more capable of self-advocacy and understanding the implications of their condition. Adolescents and young adults may face unique challenges related to identity formation, body image, and independence. 19 MS can have a profound impact on the cognitive and emotional well-being of children. Fatigue, attention deficits, and memory difficulties can affect academic performance and social interactions. Additionally, the diagnosis of a chronic illness can lead to anxiety, depression, and feelings of isolation. It is essential to address these mental health challenges early to support the overall quality of life for pediatric patients.20,21
Patient education is crucial for understanding MS, its symptoms, and available treatment options. Providing age-appropriate information can empower patients to make informed decisions about their care. Support services can play a vital role in helping patients and families cope with the challenges of MS. 22 These may include peer support groups, counseling, and respite care. Disease-modifying therapies (DMTs) can help slow the progression of MS and reduce the frequency of relapses. However, the choice of DMT should be carefully considered based on individual factors, including age, disease severity, and potential side effects. 23 Rehabilitation is essential for managing the physical and functional challenges of MS. Therapies such as physical therapy, occupational therapy, and speech therapy can help improve mobility, daily living skills, and communication. 24 Complementary and alternative therapies may also be beneficial for managing MS symptoms and improving quality of life. These may include yoga, meditation, massage, or acupuncture. 25 By addressing the unique challenges faced by children with MS and providing comprehensive care, a smooth transition to adult care can be facilitated, ensuring ongoing support and optimal outcomes.
Diagnosis: evolution of diagnostic practices
Pediatric diagnostic criteria: current standards and challenges
MS is defined as neurological symptoms disseminated in time (DIT) and space (DIS). The International Paediatric Multiple Sclerosis Study Group (IPMSSG) first developed diagnostic criteria for multiple sclerosis in 2007. These criteria were later revised and updated in 2012, following updates to the McDonald criteria.
17
To diagnose MS, at least one clinical episode with symptoms lasting ≥24 h must be present.
17
According to this criteria, POMS is defined by the occurrence of any of the following26,27:
≥2 CIS (Clinically Isolated Syndrome, which refers to refers to optic neuritis, brain stem syndrome, spinal cord syndrome, or an isolated cerebral hemisphere syndrome separated by more than 30 days, with involvement of more than one area of CNS.
28
One CIS associated with MRI findings that are consistent with dissemination in space (DIS), and a follow-up MRI with at least 1 new lesion consistent with dissemination in time (DIT) A single episode of Acute Disseminated Encephalomyelitis (ADEM) followed by one CIS occurring more than three months after symptom onset, with new brain MRI lesions indicative of dissemination in space (DIS). CIS accompanied by MRI findings consistent with dissemination in time and space, if the patient is ≥12 years of age.
Diagnosing multiple sclerosis in pediatric patients presents unique challenges that directly impact their care and transition to adult services. The International Pediatric Multiple Sclerosis Study Group (IPMSSG) allows a diagnosis of MS to be established after the first clinical episode, provided other conditions mimicking MS are excluded through rigorous evaluation. This includes comprehensive clinical, radiological, and laboratory assessments to ensure that MRI findings satisfy the criteria for dissemination in space (DIS) and dissemination in time (DIT). 29
Conditions such as neuromyelitis optica spectrum disorder (NMOSD) and acute disseminated encephalomyelitis (ADEM) frequently mimic MS in children, complicating diagnosis. These conditions share overlapping clinical and MRI features, making differentiation critical to avoid misdiagnosis. 29 Moreover, non-inflammatory conditions like metabolic disorders and leukodystrophies can resemble MS, further underscoring the need for an accurate and thorough diagnostic process. 29
Key MRI features of pediatric MS include ovoid, periventricular lesions in the juxtacortical white matter, corpus callosum, pons, cerebellum, and spinal cord. However, distinguishing features of mimickers, such as bilateral and symmetrical lesions or extensive gray matter involvement, must also be carefully considered. 17 Progressive MS types are rare in children, with relapsing-remitting MS being the most common, making clinical history critical.3,27,30 Additional tests, like cerebrospinal fluid analysis, though not routinely required, may aid diagnosis in challenging cases. 17
Transitioning to adult diagnostic protocols: adjustments needed as patients age
The McDonald criteria are used to diagnose MS in adults. It was initially proposed in 2010 and has undergone numerous revisions, with the latest one being in 2017. The 2010 McDonald criteria has been proven to be highly sensitive and specific, with a high positive predictive value, in children ≥11 years of age without features suggestive of ADEM.17,28 It has a positive predictive value of 55% in children <11 years of age, thus, it should not be used in that population. The revised criteria given in 2017 are more accurate and sensitive for MS diagnosis in the paediatric population than the 2010 one, but again, it has shown limited improvement in children <12 years. 17 When compared with adults, children with MS tend to show more T2 lesions, and the number of lesions increases rapidly in the first few years of the disease. 26 It is also worth noting that the pattern of lesions on MRI that are typically found in adult-onset MS are not always found in children. 30
This flowchart in Figure 2 illustrates the diagnostic and transitional approach from pediatric-onset MS to adult care. It begins with pediatric MS diagnosis using IPMSSG criteria, followed by pediatric MS management, and then a transition phase into adulthood. The final stages include adjustment of diagnostic methods in adults and long-term adult MS care using McDonald criteria.
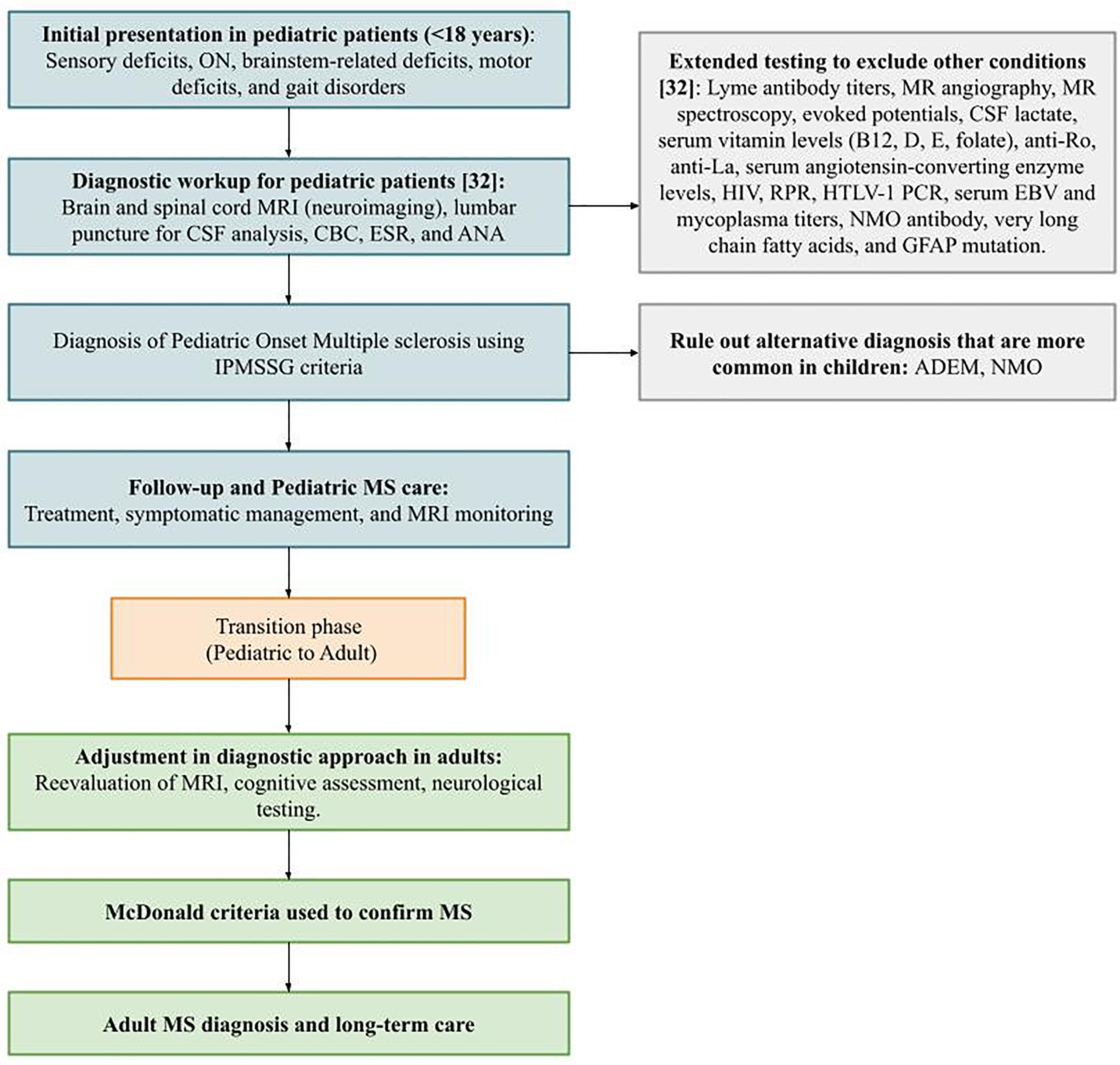
Flowchart: diagnostic and transitional flowchart for pediatric to adult MS care. 31
Use of advanced imaging techniques: role of MRI and biomarkers in diagnosis
Neuroimaging, particularly MRI of the brain and spine with and without Gadolinium, plays a pivotal role in diagnosing MS, especially in adults. Both the IPMSSG and the McDonald diagnostic criteria include MRI findings for diagnosis, as supported by the European collaborative research network MAGNIMS. 32 However, studies indicate that MRI spine is less useful in pediatric populations, with only 10% of pediatric patients meeting the DIT and DIS criteria based on spinal imaging.17,26 Brain MRI aids not only in diagnosis and prognosis but also provides vital information for differential diagnosis. Pediatric MS patients tend to have fewer T2 bright foci and larger lesions compared to adults.17,26 In addition to neuroimaging, CSF biomarkers can also support the diagnosis of MS. One of the most important among these is the presence of Oligoclonal bands (OCBs), which is a marker of ongoing neuroinflammation. It is especially effective in diagnosing MS in the 12–27-year-old age group since its presence is less frequent in the younger population. 17 However, it must be noted that the presence of OCBs in the CSF is a nonspecific finding, and their mere presence does not exclude other potential diagnoses. Other CSF markers that are frequently used in the diagnostic workup include IgG index, cell count, protein, and glucose content. Besides these, some serum tests can also be used to exclude the differentials, some of these are non-specific, like ESR, CRP, and CBC, and more specific ones include NMO antibodies (AQP-4-IgG antibodies, in cases of optic neuritis).26,33
Symptomatic management: tailoring treatment approaches
Transitioning from pediatric to adult care represents a crucial phase where careful management and collaboration between providers, patients and caregivers are essential. Some of the limitations that are commonly faced include changes in care structures, patient independence, and adjusting to adult therapeutic regimens.
Disease-modifying therapies (DMTs) for pediatric multiple sclerosis:
To target recurrence and slow disease progression, DMTs have been engineered. MS in children is very difficult to treat due to the lack of approved therapies for the condition. Most of the currently existing DMTs were based on adulthood structures, though some of them have shown promise in the pediatric environment. However, there is a shortage of proper research studies that include younger patients. First-line treatment with conventional interferon-beta and glatiramer acetate is commonly used. However, these agents were mainly licensed as adult drugs. These injectable agents have proven to cut relapses quite significantly in pediatric MS cases, but more is required to be known about the long-term outcome. 34 Newer DMTs such as Fingolimod is the first DMT formally approved for pediatric MS by the FDA, showing significant relapse reduction. Other therapies, including natalizumab, rituximab, and ocrelizumab, are used off-label, with early studies indicating safety and efficacy profiles similar to those seen in adults, especially in children aged 12 and older. 35 Early initiation of immunomodulatory treatment strongly enhances long-term prognosis. As a result, there is an increasing tendency to treat more children and young persons newly diagnosed with MS with DMTs that have initially received approval for adults. However, pediatric clinical trials are considerably challenging, and most of such decisions are mainly based on observational data and extrapolated from adult studies. The security in the long term, especially of immune suppression and infections, calls for close monitoring.36–38
Symptomatic management: addressing fatigue, spasticity, and cognitive symptoms:
Symptom management is essential to improve quality of life and reduce disability in children and adolescents with MS. Fatigue is one of the most disabling symptoms, often managed with lifestyle interventions (e.g., structured rest and physical activity). Pharmacologic treatments, such as amantadine and modafinil, are occasionally prescribed, though with mixed results. Baclofen and tizanidine are used to manage spasticity, but pediatric patients must be monitored closely for adverse effects. Physical and occupational therapy are also integral to prevent contractures and improve mobility which are often combined with adult-appropriate dosing of medications. 39 Cognitive impairments of the child with MS may involve neuropsychological evaluations and interventions since such children could survive to adulthood at the expense of the child's scholastic experience and quality of life. Accommodations in school like individualized education plans may help counter the educational limitations. 37
Transitioning to adult ms care: adapting treatment approaches:
Some paediatric patients continue with their existing DMTs during adulthood, while others switch to therapies better suited for adult MS, such as ocrelizumab or natalizumab.
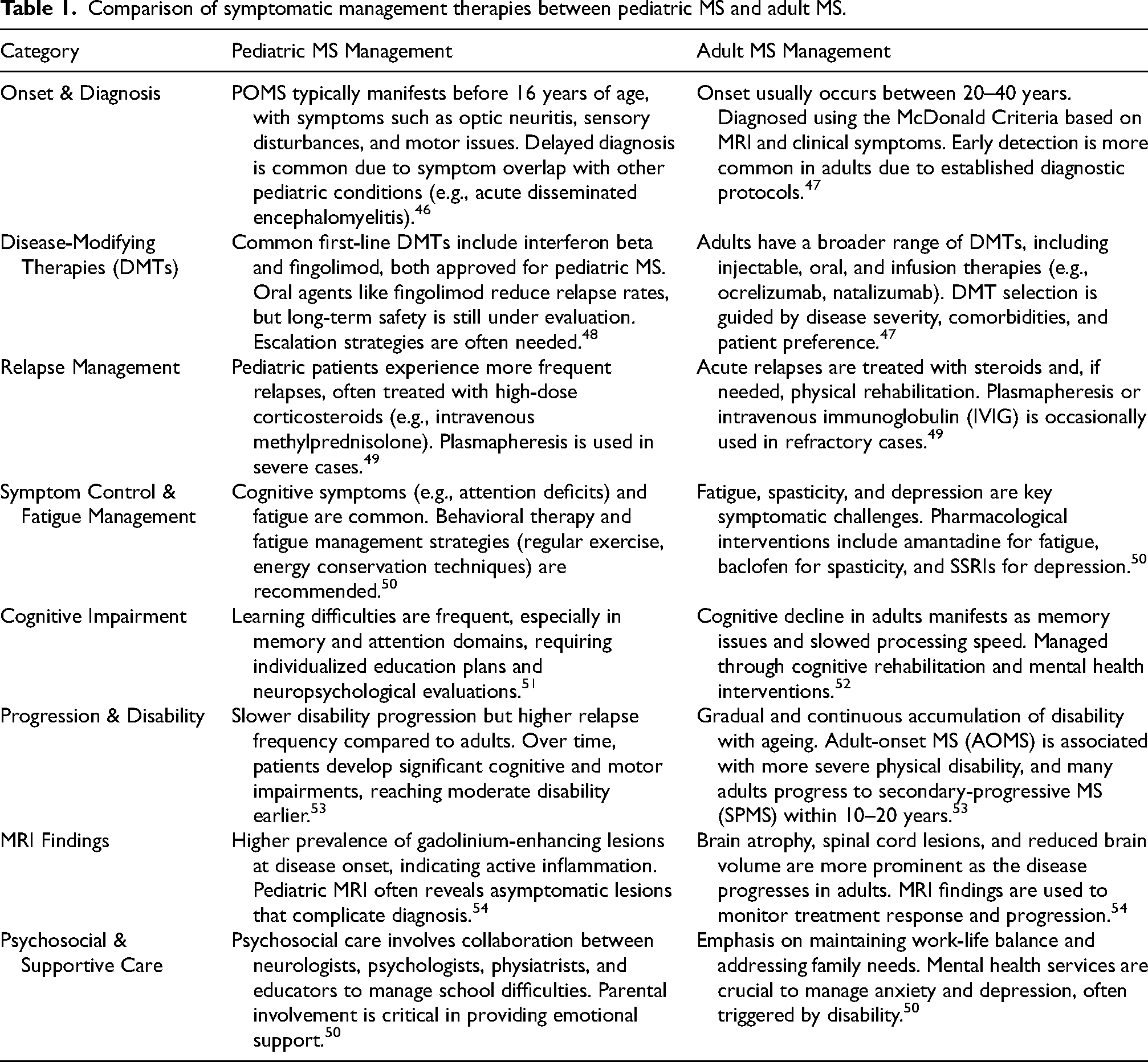
Treatment changes depend on disease activity, response, and tolerance. 40 In adulthood, new stressors like employment, independent living, and higher education arise, necessitating adjustments in fatigue and mental health management. Collaborative care involving neurologists, mental health providers, and vocational counselors can be helpful. 41 A structured transition plan, often facilitated by joint pediatric-adult MS clinics, can smooth this process. Empowering patients to engage in self-management is essential to achieving long-term adherence to therapy and monitoring regimens. 42 The transition of care from pediatric to adult MS involves adapting treatment approaches to account for ongoing central nervous system development in children, alongside ensuring long-term safety, efficacy, and compliance as patients mature into adulthood. 38 Lulu et al. highlights the importance of maintaining adherence to therapies during the transition from pediatric to adult MS care to reduce relapse rates. Wong et al. emphasizes the benefits of collaborative transition strategies, like joint pediatric-adult clinics, in minimizing care gaps and improving outcomes during this critical phase. 43 Effective sleep hygiene and appropriate pharmacological management are critical components in the care of pediatric MS patients, especially during the transition to adulthood, as they help manage symptoms like fatigue and improve overall quality of life. Integrating these strategies with long-term therapy adherence ensures smoother transitions and better disease control during this crucial phase. 44 The transition requires fostering patient autonomy and continuous care planning, with early preparation and emotional support being vital to reduce anxiety and depression risks. Key considerations include changes in disease course, necessitating modifications in treatment regimens with stronger DMTs like Ocrelizumab, and the importance of regular monitoring through MRI scans. Psychosocial challenges, such as identity formation and heightened mental health risks, must also be addressed, alongside the evolving family dynamics as young adults take on more self-management responsibility. Successful transitions rely on collaborative care models, educational support, and the use of digital tools for symptom management. Essential success factors include early planning, personalized care approaches, empowerment through education, and robust support networks (Figure 3 and Table 1). 45
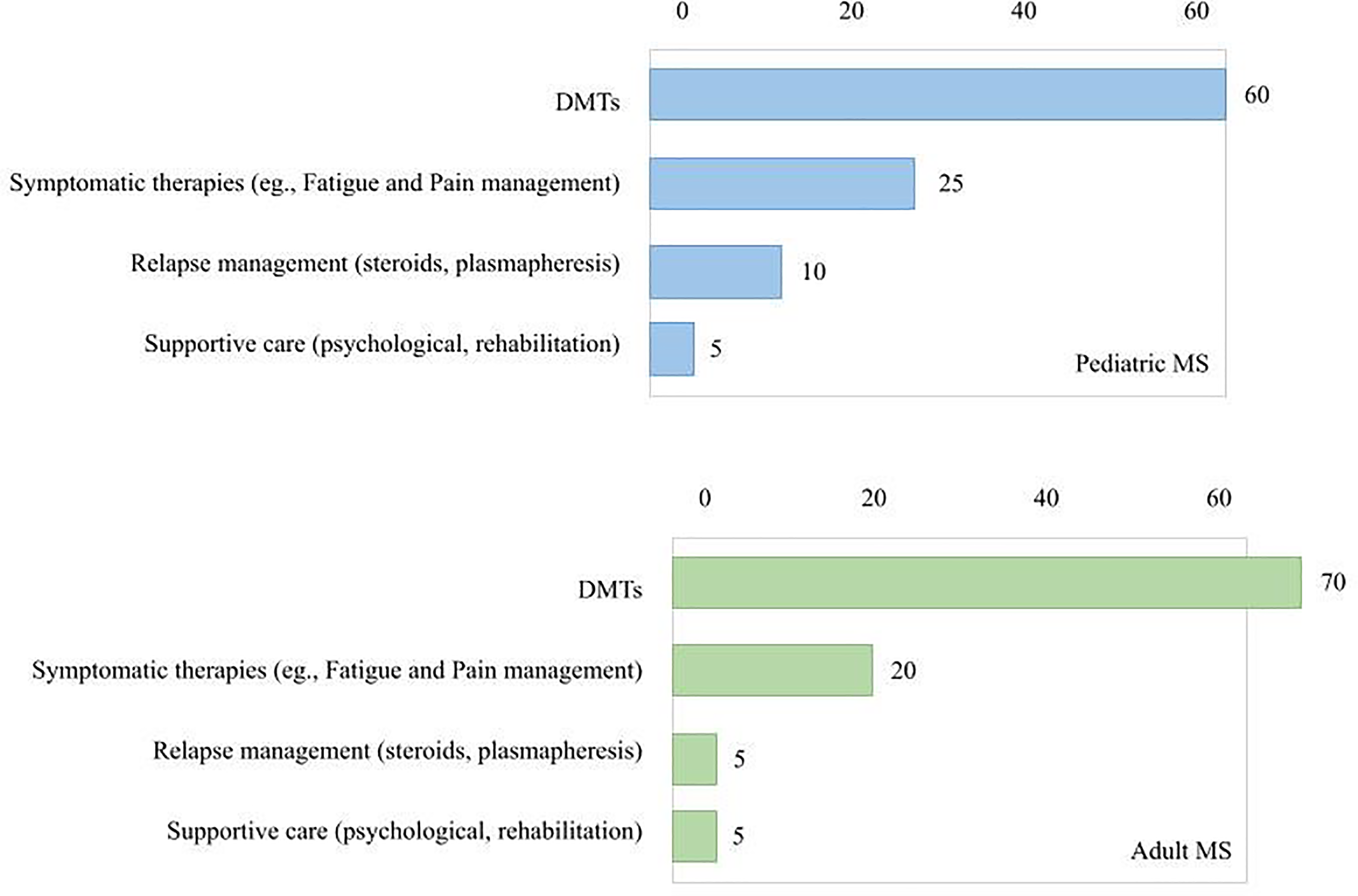
The line bar chart in Figure 3 compares the therapeutic focus in symptomatic care between Pediatric and Adult MS patients. In pediatric MS, there is a relatively higher emphasis on symptomatic therapies and relapse management, while adult MS management is dominated by DMTs, with symptomatic care and relapse management receiving comparatively lower focus. Supportive care interventions, such as psychological and rehabilitation services, remain minimal in both groups.37–39,44
Comparison of symptomatic management therapies between pediatric MS and adult MS.
Navigating the transition: challenges and best practices
Patients transitioning from pediatric to adult MS admit to finding it challenging during the treatment process, experiencing difficulties in school and social life, dealing with uncertainty and intense stress, inability to access sufficient information, and ineffective communication with healthcare providers. 55 As MS is a chronic condition that necessitates long-term care through a cohesive team approach between health care providers, family members and caretakers, the need for clearly defined roles for each team member and a personalized care plan focused on the unique needs of the patient and their family is of great importance 56 However, coordinating care among multiple providers can present challenges 57 that need to be addressed for smoother transition of care into adulthood.
Importance of multidisciplinary collaboration
Effective communication and co-management among healthcare providers can lead to improved patient care, better outcomes, reduced costs, greater efficiency, fewer emergency visits, and higher satisfaction. 57 This is particularly crucial for children needing specialty care, where collaboration between primary care pediatricians and subspecialists is essential. Proper management involves contributions from neurologists, psychiatrists, physiatrists and physiotherapists. Additionally, transitioning to adult healthcare requires ongoing support from these specialities, as patients often face psychosocial challenges like disease disclosure, employment issues, sleep disturbances, dietary changes, exercise, and peer pressure related to drug addiction. 58
Patient and family engagement
The child as well as family should be appropriately and properly guided for therapeutics and follow-up. Untrained patients can result in a loss to follow-up and trouble with relapse and other complications. Family members should ensure a proper understanding of the patient regarding his illness and help make them understand the importance of seeking timely medical care. This transition might be especially worrisome for parents whose children are stable with a particular healthcare service. However, with proper counselling and education, their fear can be overcome. It has been established that family or parental involvement has been shown to result in a smooth transition. As shown by a UK-based study ParTNerSTEP– – Parents in Transition– – a Nurse- led Support and Transfer Program, results are better when they involved parents of patients by using three modalities of educating parents: by informing websites, online teaching, and meeting with both pediatric and adult providers. 59
Creating structured transition plans
During the transition, a detailed history of the patient, of all his/ her relapses, maintenance drugs, and management regarding treatment should be transferred to the concerned new healthcare team. How the patient relapses were managed and what were the previous adverse effects of the concerned medications, if any, should all be informed to the adult treating health care team. Allow a visit by the patient to the future provider or, if possible, a combined visit. Joint clinic visits can also be managed by a patient, pediatric, and adult care provider. 60
The treatment plan should be updated in subsequent visits until the patient is ready for implementation in early adulthood. It is important to document the steps to be conducted to meet the identified needs, as well as identifying appropriate adult care resources. Tools we can implement in our practice are the “Transition Youth Registry” to track the progress of each patient in the transition process, and a “Longitudinal Readiness Checklist” to assess the adolescent's ability for independence and self-management. 61
Transition of care should also be part of the curriculum in residency programs. There is lack of training in transition of care at many levels including undergraduate/graduate medical education.57,62 This issue must be addressed to improve patient care in children with chronic illnesses.
Innovative approaches: future directions in care
It is essential for children with a diagnosis of multiple sclerosis to have a well-structured transition into adult healthcare. It is essential to ensure continuity without a lapse in treatment especially when it comes to chronic diseases like MS wherein the transitioning youth represent a vulnerable population that may carry forward their unhealthy habits further into their adulthood. Adherence to treatment and maintenance is a critical point for a successful transition from pediatric care.
It has been found that young patients with a higher degree of disability and affected cognitive functioning are the ones who face more challenges during the transition with considerations for quality of life and further education and employment opportunities.43,63 Therefore there is a potential need for individualizing methods and programs based on their degree of disability and needs. This approach is imperative to ensure a more successful transition for long term benefit. With the advent of new therapeutic modalities, it is a point of interest to further investigate which will lead to improved adherence patterns in the pediatric populations as this will also carry forward into adult care. Adherence and self management attributes in the pediatric MS often offer frequent insight into particular needs of the patients and hence are crucial in formulating an individualized treatment plan with a higher level of adherence during the transition. 43
In the recent spread of COVID- 19 pandemic, the majority of the health services have had to adapt alternate methods of healthcare delivery and effectively limit outpatient care. Therefore, telerehabilitation came into play, which is an integrated system for guiding remote rehabilitation in order to improve accessibility and continuity of care. Multiple models have been implemented over the globe along with multiple studies who have examined their success as well.64,65 These models have been particularly useful in low resource populations as well with limited access to healthcare bodies.66,67 Often in a low resource setting, telemedicine can be utilized effectively by the health providers to achieve an individualized treatment plan. 68 It has contributed towards balance and increasing the levels of physical activities in patients of multiple sclerosis – both pediatric and adult populations.
In terms of recent advances, research into the use of recreational marijuana is on the rise and is often found to be a frequent topic of discussion for teenage MS cases. Nearly 50% of a cohort of teenagers of MS who used marijuana recreationally reported it to be beneficial in reducing stress and insomnia. Despite its positive outcomes associated with recreational use, there is a lack of studies in the long term and short-term risks pertaining to its usage. 69
Conclusion
POMS is a chronic illness that occurs in children under the age of <16 years and progresses to adulthood with overall prevalence ranging from 0.69 to 26.92 per 100,000 individuals. The classic triad of MS includes optic neuritis, transverse myelitis, and brainstem demyelination while children frequently experience more subtle or atypical manifestations with longer relapse intervals. The major impact is on motor milestones, speech development, cognitive function, visual function which hinders daily activities. For the diagnosis of adult and pediatric MS cases we use McDonald diagnostic criteria along with MRI of the brain and CSF biomarkers, the latter being more reliable in pediatric MS. Multidisciplinary approach is necessary in treatment along with disease modifying therapies targeting recurrence and to slow the disease progression. Symptomatic treatment, occupational therapy, physical therapy, neuropsychological evaluation and interventions aids in improving the quality of life and reducing the disability in children. Multidisciplinary approach in treatment also raises many challenges including ineffective communication between healthcare providers of different fields, no proper information and guidance to patient and family members. These deficiencies can lead to loss in follow-up of patients, lack of social functioning, etc. These challenges resolve with proper documentation, educating family members, guiding and explaining to the patient themselves about their treatment plans, and the need for regular follow-ups. Telemedicine is alternate method of healthcare delivery system which could be accessible to patient for continuity in treatment.
The transition between pediatric and adult healthcare is not a single time event, but rather a process. It needs effective plans and encouragement in the healthcare system to prioritize structured transition programs for MS patients like making individual treatment plans, using pamphlets, focused groups for educating patients and family members, and providing joint health care and rehabilitation centers. In this review article we have discussed the challenges and have encouraged the health care system to improve for smooth transition between pediatric care to adult care.
Footnotes
Abbreviations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.