
Abstract
Background:
Heart failure (HF) is increasing in the United States, and awareness is needed for prevention. Hypertension is the leading cause of HF, and adherence to antihypertensive medication is critical for reducing HF risk. Self-efficacy positively influences health-promoting behaviors.
Objectives:
Assess HF awareness, test associations with antihypertensive medication adherence, and self-efficacy for managing chronic conditions.
Design:
We conducted a cross-sectional, observational survey research study.
Methods:
We leveraged data from participants enrolled in the American Heart Association’s Research Goes Red™ registry, an online platform powered by Verily. Three surveys ascertained HF awareness, blood pressure management, and self-efficacy. Chi-squared and Wilcoxon rank sum determined associations between survey domains and participant characteristics.
Results:
Two thousand three hundred twenty women took the HF awareness survey, 678 the blood pressure management survey, and 755 the self-efficacy survey (response rates: 12%, 78%, and 76%, respectively). Participants were predominantly non-Hispanic White (78%), with a median age of 51 (interquartile range (IQR): 39, 62). Median HF awareness score was 4/5 (IQR: 4, 5). Participants with high HF awareness versus low were more likely to be older (p < 0.001), non-Hispanic White (p < 0.001), and less likely to smoke (p < 0.001) or have depression (p = 0.004). Nearly 90% of hypertensive participants reported medication adherence, which was not associated with HF awareness or self-efficacy. Participants with greater self-efficacy versus less were more likely to have higher HF awareness (p = 0.01), be older (p = 0.01), and less likely to have depression (p < 0.001).
Conclusion:
Women’s awareness of HF and adherence to antihypertensive medication in this cohort was high. Depression and younger age may be important factors affecting women’s HF awareness and confidence in managing chronic disease medication plans.
Plain language summary
The following study investigated heart failure (HF) awareness, antihypertensive medication adherence, and self-efficacy among women from the American Heart Association’s Research Goes Red for Women Registry. We found high levels of HF awareness and medication adherence among these women. However, younger age and depression were associated with lower HF awareness and self-efficacy. These findings emphasize the importance of targeting education and support interventions, especially for younger women and those dealing with depression, to improve HF prevention strategies and medication management.
Introduction
Improvements in cardiovascular disease (CVD) mortality have stalled in recent years, in part driven by an increasing burden of both heart failure (HF) and hypertension among an aging population in the United States.1,2 HF is the leading cause of hospitalization in the United States, and the lifetime risk of developing HF for both women and men beyond age 40 is 20%. 3 There is an urgent need for effective preventive strategies to alleviate the adverse clinical, public health, and societal consequences of HF. 4 The effectiveness of preventive interventions is grounded in awareness of the disease under consideration. However, it is suggested that the awareness of HF is suboptimal as a World Heart Federation survey found that less than half of Americans surveyed were able to correctly identify the definition of HF, and only one-third correctly identified hypertension as a leading risk factor for HF. 5 Hypertension is the leading risk factor for HF and affects nearly half of U.S. adults. 6 Among U.S. adults 65 and older, hypertension affects a greater proportion of women than men and non-Hispanic Black women experience the greatest burden of hypertension compared to other racial and ethnic groups. 1 Successful management of hypertension requires adherence to a healthy lifestyle and medication plan to control blood pressure levels, which is crucial to reduce subsequent HF and mortality.7,8 Self-efficacy, an individual’s belief in their ability to execute necessary behaviors, has also been associated with greater adherence to antihypertensive medication and blood pressure control.9 –11 While there had been notable progress in blood pressure control from 2000 to 2014, recent data suggest a decline in the attainment of controlled hypertension. 8 In 2017, less than a quarter of U.S. adults with hypertension had their condition under control. 12 This regression in hypertension management poses a significant setback in efforts to combat HF.
The 2020 Surgeon General report emphasizes the importance of raising awareness of the health risks of uncontrolled hypertension, 13 a goal grounded on the premise that greater awareness of the health risks of hypertension would lead to greater blood pressure management. For HF, a major health consequence of uncontrolled hypertension, this hypothesis remains to be tested. Women’s awareness of HF is increasingly important as women often manage family health care needs and are more often family caregivers.14,15 Thus, a better understanding of HF among women could translate to benefits for the family unit and for society. Our study aims to assess HF awareness among women and test the hypothesis that HF awareness is associated with greater adherence to antihypertensive medication among women with hypertension. In doing so, we also sought to explore the role of self-efficacy in managing one’s chronic conditions in these associations, a domain known to influence adherence to health-promoting behaviors and disease prevention.11,16
Methods
Study platform and population
This study aims to evaluate women’s awareness of HF and investigate its relationship with adherence to hypertension medications, while also examining how self-confidence in managing chronic illnesses influences these behaviors. We conducted a cross-sectional, observational research study leveraging electronic survey distribution. Our study population is derived from the American Heart Association’s Research Goes Red™ (RGR) digital research platform, a collaboration between the American Heart Association’s signature women’s initiative Go Red for Women (Go Red), and Verily’s Project Baseline. Project Baseline is a collaborative initiative aimed at making medical research more accessible and engaging by distributing health surveys, materials, and recruitment opportunities online to individuals ⩾18 years old in the United States. The RGR registry was launched specifically to identify and address gaps in women’s health research. Recruitment and engagement with RGR have been previously reported. 17 In brief, 18,849 women ⩾18 years in the United States consented to join the RGR registry to engage with health surveys and research studies. Prior to enrollment, participants are ensured that all of their data is deidentified and encrypted. Electronic surveys for the present study were launched on the homepage of all RGR participants on July 6, 2022. Ten recruitment emails and newsletters were sent to all RGR participants between July 2022 and June 2023 to invite them to participate. Participants were not compensated for completing the present surveys.
Ethics statement
This study was conducted in compliance with ethical principles for medical research involving human subjects, adhering to the Declaration of Helsinki. Ethical approval for the study was obtained from the Verily Institutional Review Board (protocol approval number: 101143). All participants provided digital informed consent through Verily’s Project Baseline platform as part of the Baseline Community Study. Participation in the study was voluntary, and participants had the option to withdraw at any time without penalty or loss of benefits. Data collection and analysis were conducted with strict adherence to privacy and confidentiality guidelines. Finally, the reporting of this study conforms to STROBE guidelines for cohort studies. 18
Survey instruments
The “Heart Health: Insights and Understandings” survey consisted of three segmented surveys (Figure 1). The first survey, the HF awareness survey, ascertained participants’ demographic information, feelings about various CVDs, and knowledge of HF. Questions were derived from (1) the American Heart Association’s triennial women’s health survey, 19 and (2) the World Heart Federation’s HF awareness survey. 5 Only women who completed the HF awareness survey were invited to participate in the subsequent surveys if eligible. The second survey, the National Institute of Health-Patient Reported Outcomes Measurement Information System (PROMIS) Self-Efficacy for Managing Chronic Conditions—Managing Medication and Treatment survey, 20 which we will refer to as the self-efficacy survey, was available to participants who self-reported diabetes and/or hypertension. The self-efficacy survey consisted of four questions used to assess a participant’s confidence in their capacity to manage their medication plan. The third survey, the 2020 Centers for Disease Control and Prevention’s National Health and Nutrition Examination Survey (NHANES) Blood Pressure Questionnaire, 21 which we will refer to as the blood pressure control survey, was distributed only to participants who self-reported hypertension. The blood pressure control survey consisted of four questions regarding participants’ experiences with prescription medication for their condition. All survey instruments can be found in the Supplemental Material.

Survey flow diagram and response rates.
Statistical analysis
Deidentified data was encrypted and transferred to a secure workspace for analysis on the American Heart Association’s Precision Medicine Platform (precision.heart.org). Participants who identified as Hispanic were categorized as Hispanic regardless of their race. Participants who identified as non-Hispanic were further categorized by their identified race (e.g., non-Hispanic Black).
HF awareness scores were calculated for each respondent based on the total number of correct responses to five multiple-choice questions about HF, with a score of 0 indicating the lowest level of awareness and a score of 5 indicating the highest level of awareness. Self-efficacy survey responses were scored using the HealthMeasures Scoring Service. 22 In brief, raw summed scores were rescaled into standardized T-scores, with T-scores equal to or greater than 50 indicating greater levels of self-efficacy and T-scores under 50 indicating lower levels of self-efficacy. Chi-squared, Wilcoxon rank sum, and logistic regression tests were performed to determine whether survey domains (e.g., low versus high HF awareness, low versus high self-efficacy, taking prescribed antihypertensive medication versus not taking prescribed antihypertensive medication) were associated with categorical variables or continuous not-normal or normal distributed variables, respectively. Post-hoc pairwise comparison tests and multivariable regression models were employed where appropriate to further assess the robustness of statistically significant results. Multiplicity was not accounted for due to the exploratory nature of our analyses. We considered a p-value less than 0.05 to be statistically significant. Power analyses were conducted to determine the necessary sample size for outcomes of interest, aiming to detect small to medium effect sizes (Cohen’s d of 0.2 and 0.5) with a significance level of 0.05 and power of 0.80.
Results
Baseline characteristics
As of July 1, 2023, a total of 2320 women from all 50 states and Washington, DC completed the HF awareness survey, equating to a 12% response rate from the RGR community. Power analyses indicated that the study was adequately powered to detect meaningful associations related to HF awareness, self-efficacy, and adherence to hypertension medication. The mean age of participants was 48 (standard deviation (SD): 14) and participants with hypertension and/or diabetes comprised 43% of the cohort. Most participants were non-Hispanic White (Table 1). Participant characteristics by racial and/or ethnic group are reported among non-Hispanic White, non-Hispanic Black, and Hispanic respondents only because they each accounted for >5% of participants (Table 2).
Participant characteristics by survey. Values are N (%) or median (IQR).

HF: heart failure; VTE: venous thromboembolism; PE: pulmonary embolism; IQR: interquartile range.
Participant characteristics by HF awareness score. Values are N (%) or median (IQR). Data includes women who completed the HF awareness survey (N = 2320).
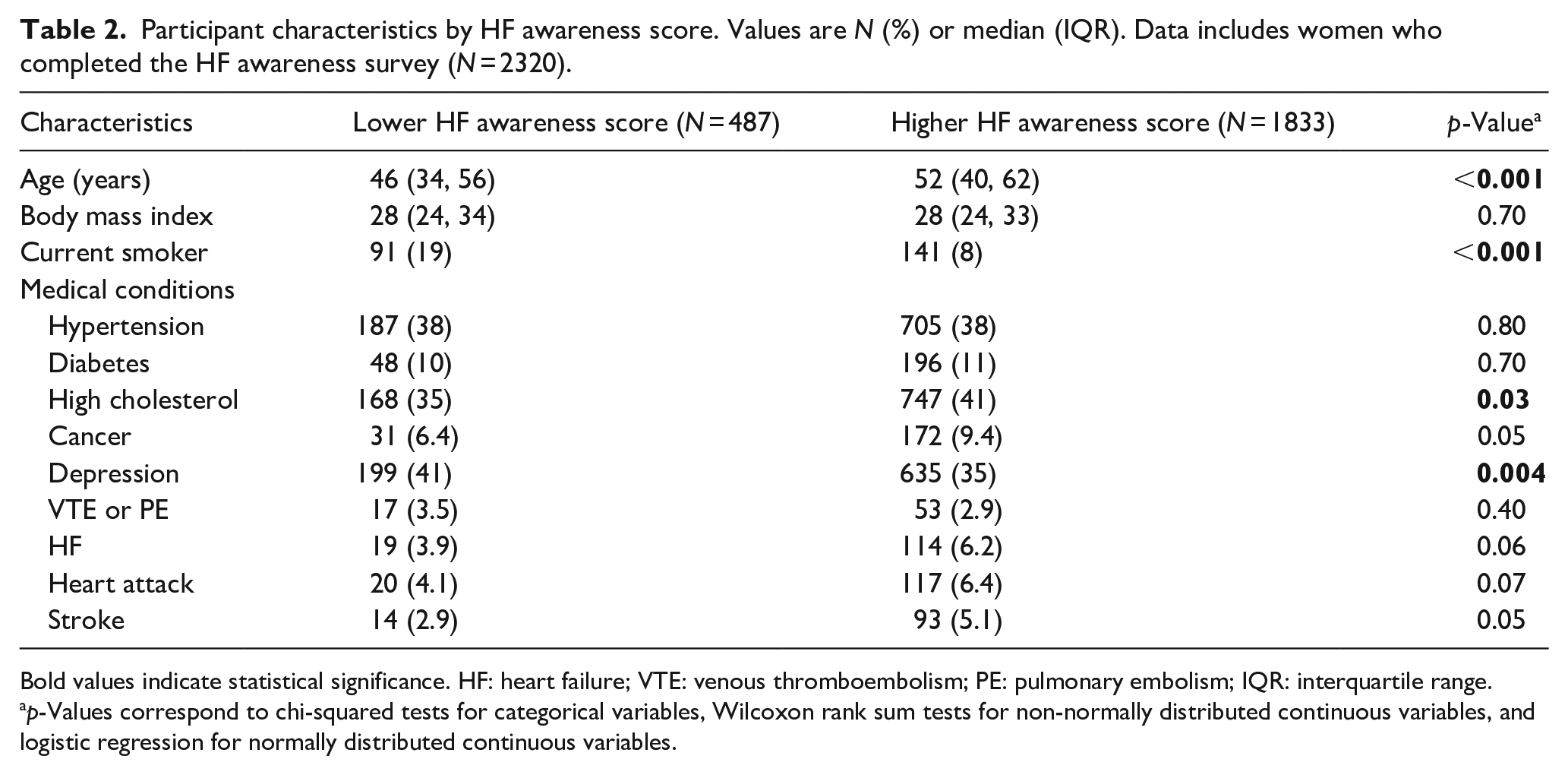
Bold values indicate statistical significance. HF: heart failure; VTE: venous thromboembolism; PE: pulmonary embolism; IQR: interquartile range.
p-Values correspond to chi-squared tests for categorical variables, Wilcoxon rank sum tests for non-normally distributed continuous variables, and logistic regression for normally distributed continuous variables.
HF awareness
Most participants (79%) reported feeling informed or very well informed about HF. The median HF awareness score was 4 (interquartile range: 4, 5) out of 5. We defined low HF awareness as a score less than 4 and high HF awareness as a score of 4 or greater due to the negative-skewed distribution of the scores (Figure 2). Of the five questions on HF, participants were most likely to correctly answer that individuals of all ages can develop HF and least likely to identify the correct definition of HF, with no variation by chronic disease status (Figure 3). In univariate analyses, participants with low HF awareness were younger (p < 0.001) and more likely to report smoking (p < 0.001), depression (p = 0.004), and high cholesterol (p = 0.03) than participants with high HF awareness (Table 2). In multivariate analysis, only age and smoking status remained significantly associated with HF awareness (p < 0.001). Additionally, non-Hispanic White participants showed greater HF awareness compared to non-Hispanic Black (p = 0.02) and Hispanic participants (p < 0.001) (Table 3). However, there was no significant difference in HF awareness between Hispanic and non-Hispanic Black participants (p = 0.30).

Distribution of HF awareness scores.

Participant responses to five questions regarding HF by chronic disease status. Correct answers are designated with asterisk.
Participant characteristics by race/ethnicity. Non-Hispanic Black, non-Hispanic White, and Hispanic groups were chosen for racial analysis as they were the only racial/ethnic groups to comprise >5% of the total sample. Values are N (%) or median (IQR).

Bold values indicate statistical significance. VTE: venous thromboembolism; PE: pulmonary embolism; HF: heart failure; IQR: interquartile range.
p-Values correspond to chi-squared tests for categorical variables, Wilcoxon rank sum tests for non-normally distributed continuous variables, and logistic regression for normally distributed continuous variables.
Self-efficacy
Of the 999 women eligible to participate in the self-efficacy survey, 755 women completed the survey (76% response rate). Participants who completed the survey were older and had a slightly higher body mass index (BMI) compared to those who did not, although the differences were not statistically significant. The mean self-efficacy score was 49 (SD: 8). Participants with low self-efficacy versus high self-efficacy (score below versus above 50) were younger (p = 0.01) and more likely to have depression (p < 0.001) (Table 4). Participants with low self-efficacy were also more likely to have low HF awareness scores compared to those with high self-efficacy (p = 0.01). Lastly, among non-Hispanic White participants, 55% had a self-efficacy score above the sample mean, while only 46% of non-Hispanic Black participants scored above the sample mean (Table 3); however, this difference was not statistically significant.
Participant characteristics by self-efficacy for managing chronic sonditions score. Values are N (%) or median (IQR). Data includes women who completed the self-efficacy for managing chronic conditions survey (N = 755).

Bold values indicate statistical significance. HF: heart failure; VTE: venous thromboembolism; PE: pulmonary embolism; IQR: interquartile range.
p-Values correspond to chi-squared tests for categorical variables, Wilcoxon rank sum tests for non-normally distributed continuous variables, and logistic regression for normally distributed continuous variables.
Blood pressure management
Of the 869 women eligible to participate in the blood pressure control survey, 678 completed the survey (78% response rate). Among eligible participants, those who completed the survey were older and had a slightly higher BMI than those who did not, though the differences were not statistically significant. Of the 678 participants with hypertension, 9% reported that they were never prescribed medication for their condition. Of the 618 participants prescribed antihypertensive medication, 89% reported currently taking their medication. Those currently taking their medication were older (p = 0.01), more likely to have high cholesterol (p < 0.001), and more likely to have HF (p = 0.01) than those not taking their medication (Table 5). Notably, taking one’s prescribed antihypertensive medication was not associated with HF awareness score (p = 0.90) or self-efficacy (p = 0.06).
Participant characteristics by antihypertensive medication adherence. Values are N (%) or median (IQR). Data includes women who reported being prescribed antihypertensive medication on the blood pressure control survey (N = 618).

One participant excluded as they did not answer whether they took their prescribed medication. Bold values indicate statistical significance. HF: heart failure; VTE: venous thromboembolism; PE: pulmonary embolism; IQR: interquartile range.
p-Values correspond to chi-squared tests for categorical variables, Wilcoxon rank sum tests for non-normally distributed continuous variables, and logistic regression for normally distributed continuous variables.
Discussion
Between July 6, 2022, and July 1, 2023, a total of 2320 women responded to the HF awareness survey through the American Heart Association’s RGR digital research platform. Response rates for the subsequent self-efficacy and blood pressure control surveys offered to participants with hypertension and/or diabetes were high. Participants were predominantly middle-to-older age and non-Hispanic White. Most participants reported feeling well informed about HF, and awareness of risk factors for and facts about HF was high. Greater HF awareness, self-efficacy, and adherence to one’s antihypertensive medication were associated with older age, while lower HF awareness and self-efficacy were associated with depression. Notably, non-Hispanic White women had higher HF awareness scores than non-Hispanic Black and Hispanic women. Further, a higher HF awareness score was associated with greater self-efficacy for managing one’s chronic condition medication plan.
The present study is the first to examine awareness of HF specifically among women in the United States. Awareness of HF is essential as most cases are preventable, and delays in seeking medical care after symptom onset increase the risk of adverse outcomes.23 –25 We found HF awareness to be high among our participants compared to data obtained by the World Heart Federation. 5 The present results indicate that middle-to-older age, non-Hispanic White women are highly aware of HF. However, Hispanic, non-Hispanic Black, and young women may benefit from increased education on and awareness of HF. Our findings build upon previous research in this data registry, which found that non-Hispanic Black women were more likely to be unaware that adverse pregnancy outcomes are associated with long-term CVD risk. 26 These collective findings underscore an opportunity for public health and healthcare professionals to bolster cardiovascular health education tailored specifically for non-Hispanic Black, Hispanic, and young women.
Moreover, we noted a greater proportion of non-Hispanic White participants exhibited higher self-efficacy scores for managing their chronic condition than non-Hispanic Black participants (55% versus 46%, respectively). While the variation was not statistically significant, likely due to a small sample size of non-Hispanic Black participants, these results highlight a potential opportunity to improve chronic disease outcomes among non-Hispanic Black women. At present, Black individuals in the United States have higher rates of hypertension and diabetes than White individuals and have been found to be less likely to adhere to their antihypertensive medication than White individuals, regardless of sex.1,27,28 The reasons for this are complex and deeply rooted in disparities in social determinants of health that affect every facet of clinical care. Interventions to increase medication adherence among Black individuals by addressing the social determinants of health at the root of this issue may alleviate a proportion of such disparities. Greater self-efficacy has been associated with better self-management of chronic diseases and adherence to antihypertensive medication.9,10 As such, our results suggest that improving non-Hispanic Black women’s confidence in managing their chronic condition treatment plan may also improve chronic disease outcomes among this population.
Regarding the essential role of blood pressure medication for HF prevention among hypertensive individuals, 29 we found a notably high prevalence of adherence to one’s antihypertensive medication (90%) among our predominantly middle-to-older aged, non-Hispanic White cohort. However, it must be noted that patients tend to overestimate their adherence to medication when self-reporting, as done in the present study. 30 Nationally, antihypertensive medication adherence is estimated to be much lower (~69%), with lower adherence reported among women compared to men. 31 Thus, digital research registries may benefit from employing more sophisticated and/or accurate instruments to assess medication use and obtain more precise results in the future.
Strikingly, the prevalence of depression among our survey participants was over 20% higher than the general population of women in the United States (36% versus 12%). 32 Depression is widely recognized as a risk factor for CVD and is associated with adverse outcomes among patients with HF.33,34 Women with depression were less likely to be aware of HF and its definition, risk factors, and symptoms than women without depression. Further, women with chronic diseases and depression reported feeling less confident in their ability to manage their treatment plans. We also found significantly higher rates of depression in non-Hispanic White women than in non-Hispanic Black and Hispanic women. The present findings are hypothesis-generating as depression may mediate a part of the relationships between diabetes, hypertension, and HF risk. Further research is needed to clearly define the role that depression plays in self-efficacy and awareness of HF.
The present findings hold significant potential for improving the quality of care and preventing chronic conditions among women. Firstly, our data underscores the importance of screening protocols for depression among women and calls for further research to delineate why depression may be a key risk factor for chronic disease development and progression. Further, the sociodemographic composition of our participants highlights the need for targeted outreach efforts to engage young and non-White women in future iterations of digital surveys to ensure greater diversity and representation in health research. Lastly, our findings emphasize a need for strategies that incorporate social workers and pharmacists to address self-efficacy-related barriers affecting adherence to antihypertensive medications among population subgroups at greatest need. Addressing these facets of healthcare delivery may lead to more comprehensive and equitable prevention and care of chronic conditions across diverse patient populations.
Our study has several important strengths. First, we leveraged previously validated survey tools and questions to conduct our research. Additionally, research has shown that survey participants are more likely to disclose personal behaviors and beliefs in online surveys than in paper surveys. 35 Lastly, using a digital platform to conduct our research allowed us to engage women across the United States, irrespective of place and time.
Our study does have limitations to be noted. First, our survey participants represent a group of primarily non-Hispanic White, middle-to-older age women, and replication of our study in different populations is essential as conducting our research solely online introduced selection bias. All RGR participants volunteer to engage in cardiovascular research studies; thus, women who are interested in and aware of CVDs are likely over-represented. Further, self-report bias is present when conducting survey research. Lastly, using a digital platform to conduct this research may also affect the validity of our findings, as participants could have consulted other online sources to respond accurately to questions regarding HF. In summary, further research and additional surveys are required to fully assess HF awareness among women.
Conclusion
Overall, this cohort of women was aware of HF and had high rates of antihypertensive medication adherence. However, depression and younger age appear to be important factors affecting women’s awareness of HF and confidence in managing their chronic disease medication plans.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241306807 – Supplemental material for Awareness of heart failure, blood pressure management and self-efficacy: The Research Goes Red for Women Registry
Supplemental material, sj-docx-1-whe-10.1177_17455057241306807 for Awareness of heart failure, blood pressure management and self-efficacy: The Research Goes Red for Women Registry by Katherine M Conners, Maryam Hashemian, Claire Kinzy, Jennifer L Hall, Christine Herr, Reeti Sharma, Pratheek Mallya, Juan Zhao, Nasrien E Ibrahim, Joseph J Shearer, Haoyun Hong and Véronique L Roger in Women’s Health
Footnotes
Acknowledgements
We thank all members of the American Heart Association (AHA) Research Goes Red™ registry (RGR) Scientific Advisory Group for volunteering their time and expertise to this initiative.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.