
Abstract
Introduction:
Intimate partner sexual violence (IPSV) is sexual violence against women by a current or former sexual partner. Sexual violence among pregnant women is higher in low-income countries, particularly in sub-Saharan Africa (SSA), which has numerous negative impacts for both the mother and the growing fetus. There is no recent and distinct information on the magnitude and factors associated with IPSV among pregnant women in SSA.
Objective:
This study aimed to assess the prevalence of IPSV and its determinants among pregnant women in SSA.
Design:
A cross-sectional study design using demographic health survey data from 2015 to 2022 in 20 sub-Saharan African countries was used.
Methods:
The analysis was conducted using a weighted sample of 10,775 women who were pregnant during the survey period (2015–2022). A multilevel logistic regression model was used to identify the determinants of IPSV among pregnant women. The adjusted odds ratio at 95% confidence interval (95% CI) was computed to assess the strength and significance of the association between explanatory and outcome variables. Factors with a p-value of <0.05 are declared statistically significant.
Result:
In this study, the pooled prevalence of IPSV among pregnant women in SSA was 11.06% (95% CI: 10.48–11.67). Respondents currently working, male-headed households, presence of justified beating, respondent mother’s history of abuse, respondent having no media access, respondent having self-reported sexually transmitted diseases (STIs), partner alcohol use, and residing in East Africa had increased odds of IPSV during pregnancy. On the other hand, nulliparous respondents, respondents involved in healthcare decision-making, households with a high wealth index, and residents of West Africa had decreased odds of IPSV among pregnant women.
Conclusion:
This study revealed that a significant proportion (11%) of pregnant women experienced intimate partner sexual violence during pregnancy in SSA. Hence, the government, policymakers, and other relevant authorities should give special attention to women’s at-risk of sexual violence, including women who live in households with justified beatings, women with STIs, working women’s, women with drunken partners, and non-autonomous women’s. Prioritization of the east African region, increasing media access, and promoting a healthy lifestyle in the community shall be done to reduce the burden of the problem.
Introduction
Intimate partner sexual violence (IPSV) is any form of sexual violence that occurs within a current or former intimate partner by forcing or attempting to force a partner to take part in a sex act, sexual touching, or non-physical sexual event (e.g., sexting) when the partner does not or cannot consent. 1 Sexual violence also includes pressuring one for sex or attempting to persuade one for sex when they do not want to. The pressure or continuous persuasion could contribute to mental health problems such as anxiety. 2
IPSV is a common public health problem and a human rights violation against women, including pregnant women, 3 which almost one in three women has experienced during their lifetime.4,5 Globally, high-income countries such as Japan have the lowest prevalence of intimate partner violence during pregnancy, whereas low-income countries, especially those in the sub-Saharan Africa (SSA) such as Ethiopia and Uganda, have the highest rate.6 –8 Almost two out of every three women in Africa have suffered severe abuse at the hands of an intimate partner at some point in their lives. 9 One-third of adolescent girls report their first sexual experience as being forced.10,11
Since victims of violence are reluctant to disclose their experiences because of numerous obstacles, it is frequently thought of as the tip of the iceberg or a silent epidemic. 12 Fear of humiliation and stigma, financial difficulties, ignorance of legal frameworks, fear of retaliation, fear of divorce, considering inadequate implementation of laws, and a mindset that views violence as a normal part of life are some of the obstacles.13 –15 As a result, underreporting occurs, and correctly assessing the prevalence of violence against women becomes difficult.12,16 Approximately one-third of women are thought to have been victims of violence at least once since they were 15 years old. 17 The majority of the issue, according to the evidence, is found in developing nations with low socioeconomic positions and inadequate access to education, particularly in sub-Saharan African countries.18,19 Compared to other locations, SSA is continuously exposed to violence. 20 The region’s intricate social, political, and economic barriers frequently expose women to abuse, which makes managing and preventing sexual violence more challenging.21,22
Pregnant women who experienced IPSV faced a plethora of negative consequences, including miscarriages, antepartum hemorrhages, preeclampsia, gestational diabetes, sexually transmitted diseases (STIs), unsafe sexual practices, mental health disorders such as eating disorders and sleep disorders, stigma, family breakups, depression, substance abuse, anxiety, posttraumatic stress disorder, suicide, and perinatal problems including perinatal mortality, intrauterine growth restriction, low birth weight, preterm delivery, cesarean delivery, and vertical transmission of HIV.23 –26 Nonetheless, because pregnant women are more vulnerable, the aforementioned consequences are more noticeable. 27
Various factors were associated with IPSV in earlier research. In light of this, factors such as women’s decision-making ability, age, spouse education, women’s education, and alcohol consumption by partners, 28 place of residence, women’s education, wealth index, unemployment, exposure to violence in childhood, weak criminal sanction against perpetuators, and male personality disorder.24,29 –31 Sexual violence against women can begin or worsen as a result of lost sexual relationships, erroneous beliefs about pregnancy, and unusual feelings the spouse experiences related to the pregnancy. 32
The United Nations Sustainable Development Goal 5 (SDG-5), which calls for the abolition of all forms of violence against women and girls, promotes gender equality and women’s empowerment. 33 In addition to being a basic human right, gender equality is also a precondition for a world that is affluent, peaceful, and sustainable. Though there has been some progress in recent years, gender equality is not expected to be achieved by 2030 across the world. The incidence of IPSV is still too high in SSA, despite worldwide attempts to reduce it. 34 For responsible bodies to address the problem and meet SDG-5 by 2030, timely information is crucial.
Pregnant women who are at risk should receive special care to guard against the risks of violence against herself and her developing fetus. Even though there is a review on sexual violence against pregnant women around the globe, there is a paucity of up-to-date information on sexual violence against pregnant women in SSA in particular. In order to provide adequate information on IPSV against pregnant women in the high-risk SSA region, current multi-country data is thus required. This information will enable concerned parties and relevant authorities to address the issue in a way that takes into account each country’s unique socio-demographic and cultural background. Therefore, this study aimed to assess the prevalence of IPSV and its associated factors among pregnant women in SSA using the most recent Demographic and Health Survey (DHS) data.
Methods
Study design, setting, and period
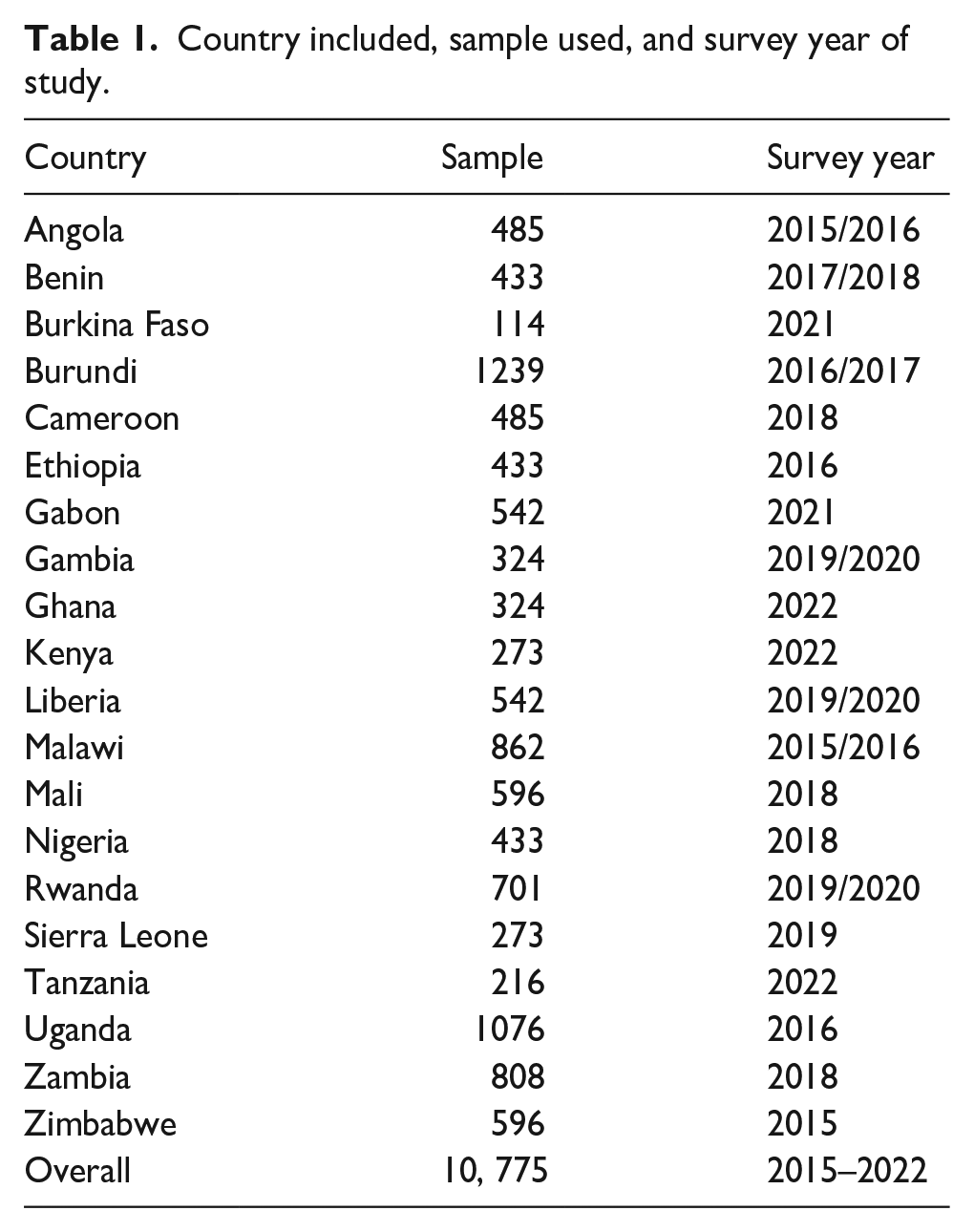
This is a multi-country cross-sectional study using the most recent DHS data of 20 sub-Saharan African countries. The source populations were pregnant women from 20 sub-Saharan African countries who had DHS data between 2015 and 2022. The countries included in this study were Angola, Burkina Faso, Benin, Burundi, Cameron, Ethiopia, Gabon, Ghana, Gambia, Guiana, Kenya, Liberia, Mali, Malawi, Rwanda, Serra Leon, Tanzania, Uganda, Zambia, and Zimbabwe.
Data source and sampling procedure
DHS was a nationwide survey conducted in low- and middle-income countries using standardized, pretested, and validated. The DHS employ a two-stage, stratified cluster sampling technique. The initial stage involved the random selection of all-encompassing clusters, or enumeration areas, from the sampling frame obtained from the last publicly available national survey. In the second phase, systematic sampling was used to interview a subset of the target population’s households, covering all the households listed in each cluster. A weighted sample of 10,775 pregnant women prior to the survey who responded to sexual violence questioners was included in the study. For women having more than one history of self-reported sexual violence by their immediate partner, the most recent abuse history was used. Pregnant women’s who had a missing value for outcome were excluded from the study. We have followed the STROBE guidelines when preparing our manuscript (Supplemental Table 1).
Source and study population
All reproductive-age women who faced sexual violence during their pregnancy were the source population, and those women who gave responses to questions asking sexual violence during the survey were the study population.
Study variable
Outcome variable
The outcome variable was sexual violence among pregnant women by intimate partners. The outcome measures the exposure to sexual violence among pregnant women 5 years prior to the DHS. It was classified as yes = 1 for “women who experienced sexual violence” and no = 0 for “women who had no exposure to sexual violence.” The outcome variables were determined by asking pregnant women in DHS data using the following questionnaires’: (a) being physically forced to have sexual intercourse with him when she did not want to; (b) being physically forced to perform any other sexual acts she did not want to; and (c) being forced to perform sexual acts she did not want to.
Independent variables
Individual-level variables
Individual-level factors were reviewed from previous literature, and these include respondent and their partner education level, respondent work status, household head sex, beating justified in the household, respondents mother had experienced intimate partner violence, media exposure, presence of self-reported STI in respondent, respondent age at first sex, respondent partner polygamy, respondent partner alcohol use, the number of under-five children in the household, parity of respondent, respondent involvement in healthcare decision-making, and household wealth index.
Community-level variables
Community-level media exposure, community-level women’s illiteracy, and community-level poverty were aggregated from individual women’s characteristics of media exposure, education, and wealth index, respectively. Since the aggregate values for all generated variables have no meaning at the individual level, they were categorized into groups based on median values. Median values were used to categorize as high and low because all aggregated variables were not normally distributed. Similar procedures were applied to all aggregate variables.
Regarding the analysis of aggregation, first the individual-level variables were re-categorized and cross-tabulated with the cluster variables using Stata version 17 (Texas, USA). Then, the proportions of media exposure, no education, and poor wealth index categories for each variable proportion were computed using Microsoft Excel 2010. Then, the proportion of each variable result was imported into Stata and combined with the original Stata using a one-to-many variable combination. Finally, we categorized the proportion of each variable as high or low based on the mean proportion.
Operational definition
Statistical analysis
After being extracted from the EDHS portal, Stata version 14 (Texas, USA) was used to enter, code, clean, record, and analyze the data. In DHS, data variables are nested by clusters, and those within the same cluster show more similarities than those with separate clusters. Thus, using the traditional logistic regression model violates the assumptions of independent observation and equal variance across clusters. Therefore, a more sophisticated model is required to account for cluster characteristics. A multilevel, multivariable logistic regression model was employed in the study to identify the variables associated with intimate sexual violence among pregnant women. In the analysis, four models were fitted. The first (null) model, which contains only the outcome variables, assesses the degree of intra-cluster variation in IPSV. The second model contains individual-level variables; the third model contains only community-level variables; and the fourth model contains both individual-level and community-level variables. The following is the equation for the multilevel mixed effect model.

where πij is the likelihood of experiencing sexual violence from an intimate partner, (1 − πij) is the likelihood of not being sexually abused by intimate partner, βo is log odds of the intercept, β1, . . . βn are effect sizes of individual and community-level factors, and x1ij. . . xnij are independent variables of individuals and communities. The quantities uoj and eij are random errors at cluster levels and individual levels, respectively.
Both the fixed and random parts of the mixed effect were assessed. The random effect was assessed using the following parameters: intra-class correlation coefficient (ICC), median odds ratio, and proportional change in variation (PCV). The concept and ways to determine these parameters were stated elsewhere. The fixed effect was assessed by using the adjusted odds ratio (AOR) at a 95% confidence interval (95% CI). The significance of the association between explanatory variables and outcomes was declared when the p-value was less than the level of significance (0.05). So, multilevel is a nested model, and log likelihood and deviance were used for model comparison. The multi-collinearity between explanatory variables was controlled by using the software itself (the nature of Stata omitting variables with multi-collinearity) and multivariable.
Ethical consideration
The DHS data from 20 sub-Saharan African countries was gathered in compliance with national and international ethical standards. Ethical clearance was provided by the Institutional Review Board of ICF International and the United States Centers for Disease Control and Prevention. At the time of data collection for the DHS, all study participants were asked for informed oral consent, and data were collected anonymously. Data collectors explained the purpose of the study and that participation in the study was voluntary. Privacy and confidentiality were ensured by following the ethical requirements of the research. The study involved minimal risk for study participants. More details regarding DHS data and ethical standards are available online at http://www.dhsprogram.com.
Results
In this study, 20 sub-Saharan African countries were included. To come up with existing evidence, we included countries that had recent standard DHS data from 2015 to 2022 (Table 1).
Country included, sample used, and survey year of study.
Prevalence of IPSV among pregnant women in SSA
The pooled prevalence of IPSV among pregnant women in SSA was 11.06% (95% CI: 10.48–11.67). The lowest prevalence was observed in Burkina Faso 2.0% (95% CI: 1.68–2.67), and the highest prevalence was observed in Burundi 23.13% (95% CI: 22.57–23.73) (Figure 1).

The prevalence of IPSV among pregnant women in SSA.
Socio-demographic characteristics of study participants
A total weighted sample of 10,775 pregnant women who responded to sexual violence questioners in the survey was included in the study. The prevalence of sexual violence by intimate partners was 11.06% (95% CI: 10.48%–11.67%). Nearly three-fourths (73.3%) of pregnant mothers were aged 20–34. More than two-thirds (68.03%) of mothers were not working. The majority (83.3%) of households were headed by men. Nearly one-third (30%) of partners (husbands) had no formal education. Nearly half (47.5%) of households were categorized in the poor wealth quintile. Nearly one-fourth (24.54%) of women’s had a history of justified violence by their immediate partner. More than half (59.67%) of mothers were involved in decision-making regarding healthcare. More than two-thirds (63.98%) of participants had more than 5 years of cohabitation. More than two-thirds (67.87%) of participants reside in rural areas. More than one-third of participants (36.72%) had access to the media. Nearly one-fourth (24.65%) of respondent mothers had a history of beating their husbands (Table 2).
Socio-demographic factors of IPSV among pregnant women in SSA.

STI: sexually transmitted disease.
Random effect model fit statics
The null model was run to determine whether the data supported assessing randomness at the community level. The ICC value in the null model indicates 18.3% of intimate sexual violence was due to the difference between clusters. In the null model, the odds of intimate sexual violence were 2.26 times variable between high and low clusters (heterogeneous among clusters). Regarding the final model PCV, about 71.75% of the variability in intimate sexual violence was attributed to both individual and community-level factors. Model IV was selected as the best-fitting model since it had the lowest deviance (Table 3).
Random effects and model fit statics of IPSV among pregnant women in SSA.
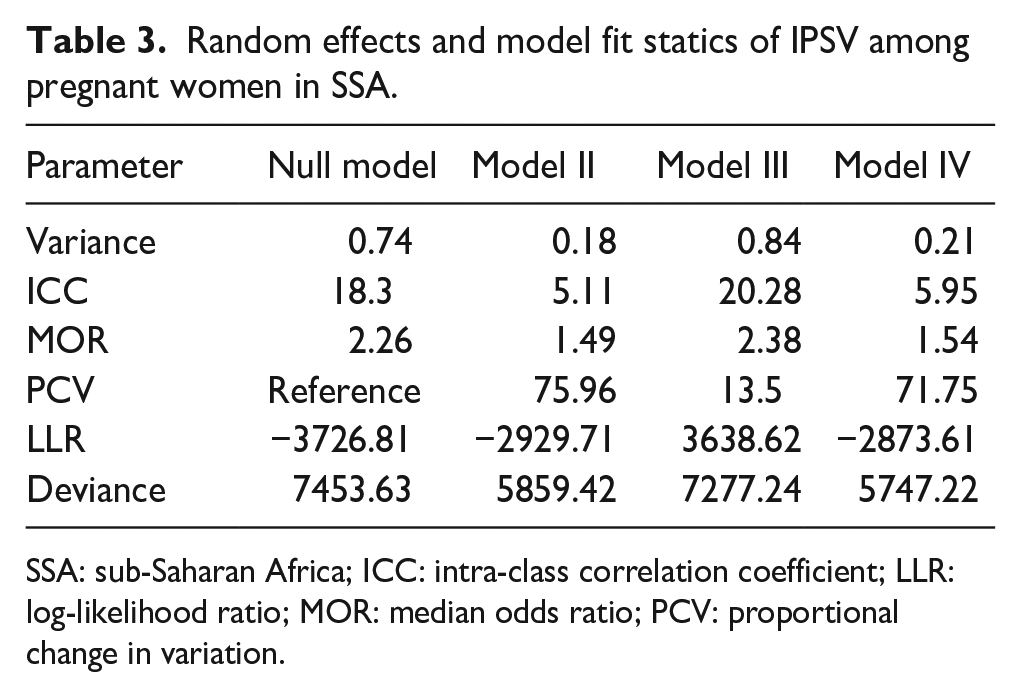
SSA: sub-Saharan Africa; ICC: intra-class correlation coefficient; LLR: log-likelihood ratio; MOR: median odds ratio; PCV: proportional change in variation.
Factors associated with intimate sexual violence among pregnant mothers
In the final multilevel multi-variable regression analysis, respondent working status, sex of household head, beating justified in the household, wealth index, media exposure, respondent involvement in decision-making, partner alcohol use, respondent history of self-reported STI, respondent mother abused ever, parity of respondent, and region were significantly associated with IPSV among pregnant women’s.
Compared to not-working respondents, currently working respondents had 34% increased odds of intimate sexual violence (AOR = 1.34; 95% CI: 1.13–1.58). Being in a male-headed household increases the odds of intimate sexual violence by 28% (AOR = 1.28; 95% CI: 1.04–1.58). Respondents with a history of justified beating increased the likelihood of IPSV by 83% (AOR = 1.83; 95% CI: 1.58–2.13). Having no access to media increases the likelihood of IPSV by 33% (AOR = 1.33; 95% CI: 1.13–1.56). Having self-reported STIs by respondents increases the odds of IPSV by 1.92 (AOR = 1.92; 95% CI: 1.62–2.27). Respondent partner drinking alcohol increases the likelihood of IPSV by twice (AOR = 2.33; 95% CI: 2.02–2.42) as compared to non-alcoholic partner. Compared to respondents involved in healthcare decision-making, respondents having no involvement in healthcare decision-making in households increase the odds of IPSV by 54% (AOR = 1.54; 95% CI: 1.13–1.56). Being in the Easter part of SSA increases the odds of IPSV (AOR = 1.93; 95% CI: 1.54–2.42) as compared to central SSA. Respondent mothers with a history of abuse by their husband increase the odds of IPSV by 34% (AOR = 1.66; 95% CI: 1.43–1.92) as compared to their counterparts. On the other hand, as compared to poorer households being in the richer wealth index, 31% (AOR = 0.69; 95% CI: 0.56–0.85) decreased of IPSV. Similarly, being in the Western part of SSA decreases the likelihood of IPSV by 28% (AOR = 0.72; 95% CI: 0.55–0.93) as compared to central SSA. Compared to grand-parous women’s, uniparous women’s had 32% lower odds (AOR = 0.68; 95% CI: 0.53–0.89) of IPSV (Table 4).
Factors associated with intimate sexual violence among pregnant women in SSA.

SSA: sub-Saharan Africa; AOR: adjusted odds ratio; STI: sexually transmitted disease.
Statistically significant-value < 0.05.
Discussion
Violence against women, committed by intimate partners, is an important public health and human rights issue. 7 Despite sexual violence legislation in Africa, a significant number of pregnant women in SSA faced sexual violence. 35 This study also discloses that 11.06% (95% CI: 10.48–11.67) pregnant women in SSA had sexual violence during their pregnancy by their intimate partner. Thus, responsible bodies and stakeholders shall work together to lower and eliminate the problem in SSA.
Although the study was not limited to pregnant women, another study conducted in SSA revealed a similar finding (11.5%). 36 This indicates that Africa is still under the burden of IPSV and that responsible authorities should enforce strong rules and regulations against any forms of sexual violence against vulnerable pregnant women.
However, this study finding is higher than the study done in Europe, which was 8.3%–21.1%. 37 In addition, the finding of this study is lower than the study done in Brazil, which was 39.1%, Iran, which was 11% 38 and one global study, which was 32%.39,40 The possible explanation for the discrepancy might be due to differences in socio-cultural practice, law enforcement, and individual and community attitudes toward intimate partner violence.
This study found respondents who had witnessed their father beat their mother were more likely to be subjected to IPSV as compared to non-abused mothers. This is in line with the studies in Kenya and Bangladesh.41,42 This could be because women who observe their fathers abusing their moms may, consciously or unconsciously, accept such violence as a normal and necessary part of marriage, developing attitudes and behaviors that make them more vulnerable to abuse in the future.43,44 Furthermore, violence is a learned behavior that may be adapted. 45
According to this study, respondents having self-reported STIs increases the likelihood of IPSV by twice as much as women’s having no self-reported STIs. A woman who has self-reported STIs, including HIV, in the past 12 months is more likely to have experienced IPSV than their counterparts. This is supported by studies done in South Africa and Uganda.46 –48 This may happen because the victim lacks the self-esteem to deny the need for a spouse, as well as the motivation and authority to bargain with her partner for safe sex. 49 In addition, women who had a history of self-reported STIs might also have experienced forced sex, fallen out of treatment, and missed opportunities. 50 Furthermore, women may be pushed into having unwanted and forced sex, most frequently out of fear of painful mating. As a result, it is advisable to screen women with STI for sexual violence to identify further factors behind the attack against these vulnerable women’s.
The odds of sexual violence were higher among respondents whose partners drank alcohol than among respondents whose partners did not use alcohol. This is supported by studies done in Canadian and African countries.51,52 This is because alcohol has a neurotoxic effect that causes interpersonal communication to break down and can result in violence. For a man, having a pregnant partner can be a challenging and stressful period of his life, so in order to cope with the stress, he may turn to alcohol, which can increase their risk of engaging in sexual violence. 53 It is obvious that a person who believes someone has used alcohol may react more violently; therefore, some husbands purposefully “hide” behind alcohol to engage in antisocial activities such as sexual assault.54,55 Furthermore, alcohol use leads to a higher occurrence, severity, and frequency of sexual violence. 56 Therefore, it is essential to advise partners to lower or limit alcohol use to lead a healthy and happier life and to reduce unwanted violence in the household.
Nulliparous respondents had reduced odds of IPSV as compared to multiparous women. This is supported by the study done in Uganda. 57 This is because multiparous women are more prone to having mood swings and other pregnancy-related problems that could lower their libido. 58 Older married women also had more time to develop a history of sexual assault 29 that might increase the episode of sexual violence.
Respondents in the wealthier quintile were less likely to experience IPSV as compared to respondents in the poor household wealth quintile. This is supported by studies done in Brazil, a WHO multi-country study, and low- and middle-income countries studies.59 –61 This is because economically independent women’s are shielded from gender inequity and sexual assault 62 ; on the contrary, women from poorer wealth index households experience more sexual violence. 63 Furthermore, women who are financially independent of their partner find it easier to leave an abusive marriage and are less likely to condone violence. 64 Hence, it is essential to improve households’ incomes to reduce the burden of violence against women and other unwanted social behaviors in SSA.
Respondents from households where beating is considered justified are more likely to experience IPSV compared to those from households where it is not. This is supported by studies done in Ghana, Rwanda, and Uganda.65 –67 This is because societies in low-resource countries had a widespread practice of justifiable beatings against women, which included paying for brides and instructing women to be obedient and submissive. This is closely related to social standards that give husbands the authority to abuse their wives and women who prioritize maintaining the family image over their health issues. Sexual violence is typically not seen as a violation in communities with such unfavorable cultural views, which deprives women of their self-confidence and leaves them open to other sorts of abuse at the hands of males.68,69 These factors collectively deprive women of the ability to make sexual decisions and grant men complete autonomy. 70 Thus, it is appropriate to denounce detrimental customs that lower the quality of life for women.
Working respondents were more likely to experience IPSV as compared to their counterparts. This is supported by studies done in Rwanda, Mexico, and America.71 –73 This may be because women who work because of financial hardship or a regular job work longer hours, experience stress at work that reduces time spent with their spouse, and may not tell their colleagues about violent episodes that they experienced, which in turn causes their partner to feel forced and unwanted to have sex with them. 71 The notion of relative resources and social exchange also explains this: women who are more economically empowered may threaten men’s position and so be more vulnerable to violence. However, compared to working mothers, other research found that jobless women were more likely to experience domestic violence from their spouse. 74 The theory of marital dependency may also provide further insight into this. It postulates that women who have less financial means may be more reliant on their male partner and less able to end or modify relationships, which increases the likelihood of violence. 75
Compared to their counterparts, respondents who participated in household healthcare decision-making were less likely to experience sexual violence. This is supported by a study done in the Philippines. 76 This may be because mothers who are capable of making decisions about the healthcare of their families on their own may also be free to choose and discuss with their partner how they want to have a sexual relationship and that they would such as open communication and understanding. 77 Thus, encouraging women’s autonomy is essential to lessening the prevalence of violence against women in general.
Residing in a male-headed household increases the odds of IPSV as compared to female-headed households. This is supported by a study done in Ethiopia. 8 This is due to the fact that male-headed households had autonomy and control over the entire household activity, including commuting violence. 78 Although female-headed households are less likely to experience sexual violence since they have authority and autonomy to decide what they want in all dimensions of their lives, there might be physical and other violence related to disagreement and other social factors in the community. 65
Respondents in east African countries were more likely to experience sexual violence against them than in central Africa, whereas being in West Africa reduced the likelihood of intimate partner sexual assault. This is supported by studies done in East Africa.77,79 According to a study, the highest proportion of violence in Africa was observed in Uganda and Ethiopia.62,80 In comparison to other sub-regions of Africa, East African women faced a comparatively higher rate of sexual violence. 81 Furthermore, there are conflicts, political unrest, gender-based violence, climate change, and migration in eastern Africa that expose women to violence. 82
Respondents who were not exposed to the media were more likely to experience IPSV as compared to respondents who had media exposure. 83 This is supported by a study done in Ethiopia. 84 One possible explanation is that media coverage contributes to raising awareness of women’s mental and physical health in order to encourage good lifestyle choices, dispel taboos, and stop harmful conduct, such as sexual abuse.85,86 It stops violence against women by making spouses responsible and knowledgeable about the law. It is also a crucial tool for enhancing women’s self-determination, empowerment, and accessibility to healthcare.87,88
Strength and limitation
This study’s strength was based on 20 countries with different social, cultural, and economic levels. Thus, the study has the potential to assist programmers and policymakers in developing effective national interventions because it is based on data from a countrywide survey. Due to the cross-sectional nature of the study design, the results of this study could not infer a causal relationship between outcome and independent variables. Furthermore, because DHS is a cross-sectional survey and depends on respondents’ self-reports, recall bias may be present. Second, information bias may also have an impact on women’s decisions to disclose their sexual violence, since disclosure of violence is highly influenced by the interviewer. In addition, we have not used power analysis for sample size calculation.
Conclusion
The study found that among pregnant women in SSA, factors at the individual and community levels were significantly associated with IPSV. The main factors that determined IPSV in our study were respondent work status, household head sex, having history of beating, respondent mother history of abuse by husband, access to media, self-reported STI, partner alcohol use, parity, respondent involvement in healthcare decision-making, wealth index, and region. Policymakers, the government, health planners, and implementers must therefore understand the burden of the problem, create awareness in the media, empower women, promote healthy lifestyles, and women’s with justified beatings in the east African region and non-autonomous women’s need special attention.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241305268 – Supplemental material for Prevalence and determinants of intimate partner sexual violence among pregnant women in sub-Saharan Africa: Evidence from the most recent DHS data 2015–2022
Supplemental material, sj-docx-1-whe-10.1177_17455057241305268 for Prevalence and determinants of intimate partner sexual violence among pregnant women in sub-Saharan Africa: Evidence from the most recent DHS data 2015–2022 by Berhan Tekeba, Tadesse Tarik Tamir, Gebreeysus Abera Zeleke and Alebachew Ferede Zegeye in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241305268 – Supplemental material for Prevalence and determinants of intimate partner sexual violence among pregnant women in sub-Saharan Africa: Evidence from the most recent DHS data 2015–2022
Supplemental material, sj-docx-2-whe-10.1177_17455057241305268 for Prevalence and determinants of intimate partner sexual violence among pregnant women in sub-Saharan Africa: Evidence from the most recent DHS data 2015–2022 by Berhan Tekeba, Tadesse Tarik Tamir, Gebreeysus Abera Zeleke and Alebachew Ferede Zegeye in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.