
Abstract
Background:
Pubic hair removal (PHR) is common among women in the United States, and understanding current practices is important for public health efforts. The most recent national study focusing on U.S. women’s PHR habits and their correlates was conducted over a decade ago.
Objectives:
The current study aims to provide an updated understanding of PHR practices among U.S. women, examining prevalence, methods, frequency, and motivations. We also examine characteristics of women who choose to remove their pubic hair.
Design:
A cross-sectional, nationally representative survey administered in Spring 2023 via Ipsos KnowledgePanel.
Methods:
Women (N = 522, ages 18–85 years) responded to items inquiring about their demographic characteristics, sexual behaviors, and social media use, as well as methods, prevalence, and motivations associated with PHR. We examine various demographic and behavioral correlates of lifetime and recent PHR among women.
Results:
Findings reveal that the majority of U.S. women have removed their pubic hair at some point in their lifetime, and almost half have done so within the past month. Frequency and preferred styles of PHR varied among women, indicating a wide range of individual preferences. Among top motivating factors for PHR were perceived cleanliness, comfort, and wanting to look good in a bikini. Race, age, and history of sexual activity were all statistically significant predictors of lifetime and recent PHR.
Conclusions:
Findings from the current study may assist skincare professionals in better addressing patient/client PHR needs and concerns while promoting health. Studies should continue examining trends in PHR over time, its relation to societal perceptions of beauty, and its implications for health and well-being.
Plain language summary
Pubic hair removal (PHR) is a common practice among women in the United States, and it’s important for public health experts to understand current habits. Since the last national study on this topic was conducted a decade ago, the goal of this research was to update our knowledge of how and why U.S. women remove their pubic hair, along with examining which personal characteristics are related to a higher likelihood of women’s PHR. We surveyed 522 women aged 18 to 85 across the U.S. in Spring 2023 using Ipsos KnowledgePanel. We asked about their backgrounds, sexual behaviors, social media use, and their methods, frequency, and reasons for PHR. Our findings show that a majority of U.S. women have removed their pubic hair at some point, and nearly half have done so within the past month. Frequency and preferred styles vary, reflecting individual preferences. Most common reasons for PHR included feeling cleaner, more comfortable, and wanting to look good in swimsuit. We found that race, age, and sexual history significantly influenced women’s likelihood of PHR in their lifetime and in the past month. Understanding these practices can help skincare professionals better meet the needs of their patients and clients, promoting women’s overall health. Moving forward, it is important for studies to continue monitoring PHR trends among women, exploring its connection to evolving societal beauty norms and examining its impacts on health and well-being.
Introduction
Pubic hair removal (PHR) is a common practice among women in the United States. 1 Although people of all ages and gender identities engage in PHR, research consistently shows that the practice is most prevalent among young women,1 –9 with most U.S. women typically beginning PHR in adolescence.10,11 PHR has been positively associated with sexual attractiveness and desirability,4,12 perceived cleanliness and hygiene, 13 and more positive genital self-image 5 among women.
Understanding women’s PHR practices is important from a health perspective as research has linked women’s overall skin health to their general health and well-being,14 –16 and PHR is associated with various potential skin health risks including skin irritation, cuts, rash, wax burns, hyperpigmentation, and infections such as folliculitis.14,17 –19 Recent studies have demonstrated that women who frequently remove all of their pubic hair are also at increased risk of contracting urinary tract infections and sexually transmitted infections (STIs).20,21 In addition, awareness of PHR norms among women can help elucidate broader issues related to body image and societal pressures, factors which may also potentially influence women’s decision-making and impact their mental and emotional well-being.22 –24 However, the last national study focusing on U.S. women’s PHR habits and their correlates was conducted in 2013 (i.e., over a decade ago). 2 In that study, Rowen et al. found razors and scissors to be the primary methods used by women to remove their pubic hair; a very small percentage of the sample engaged in alternative methods such as laser hair removal, waxing, electrolysis, or using hair removal creams. 2 The study also uncovered various factors associated with PHR, including age, race, education level, and number of lifetime sexual partners. 2
While some of these findings may translate to the present day, there is reason to believe women’s PHR has undergone substantial transformations over the past decade. While successful laser hair removal was once limited to individuals with contrasting hair and skin tones, recent breakthroughs have allowed for this treatment to be safe and widely accessible across a wider spectrum of women. 25 During COVID-19 restrictions in 2020, those whose preferred PHR methods became unavailable (e.g., laser hair removal, salon waxing, sugaring) had to adapt to an at-home method such as shaving with a razor. 8 It is possible that some women became used to a new norm, and eventually embraced it as a lasting part of their ongoing PHR practices. There has also been a considerable increase in women’s body positivity movements, challenging traditional beauty standards and embracing diverse bodies and natural features, including body hair.26 –28 Conversely, the rise in popularity of social media platforms and influencers promoting beauty standards that are heavily edited, filtered, and unrealistically attainable may influence women to remove their pubic hair more frequently and/or extensively in an attempt to achieve an “ideal” body.29 –32
Understanding the full range of women’s PHR practices may enable skin health experts (e.g., dermatologists) to offer appropriate guidance, support, and health education tailored to individual patients’ routines and skin needs, and provide comprehensive and relevant care. 33 Furthermore, estheticians (i.e., skincare professionals who specialize in PHR, including methods such as waxing, sugaring, or laser) occupy a unique position of trust and rapport with their clients and have become trusted providers of both beauty expertise and valuable health information, 34 making estheticians a potentially valuable resource for delivering accurate and updated information, reinforcing healthy habits, and encouraging preventive health behaviors.
Objectives
The present study builds upon findings of earlier nationally representative research 2 to offer an updated understanding of PHR practices among U.S. women. We assess the prevalence, methods, frequency, and motivations regarding PHR in a cross-sectional study with a nationally representative sample of U.S. women. We also assess characteristics of women who remove their pubic hair and sociodemographic and behavioral predictors of PHR.
Methods
This manuscript was prepared in accordance with STROBE guidelines for cross-sectional studies. 35
Study population
In Spring 2023, a probability-based Internet panel survey (Ipsos KnowledgePanel) including a nationally representative sample of U.S. adult panelists aged ⩾18 years was conducted to assess prevalence of and methods and motivations for PHR. Address-based probability sampling was used to improve population coverage and targeting, particularly for hard-to-reach individuals (e.g., young adults, minority subgroups). More details regarding recruitment and methodology are reported elsewhere.36,37 The KnowledgePanel includes adults in the United States general (non-institutionalized) population. Once household members are recruited for the panel, they can be invited to complete specific survey projects. Once assigned to a study sample, they are notified by email and/or SMS that a self-administered survey is available to complete, and they provide written informed consent to participate. Findings from the current study include only women (N = 522) and are derived from a total of 1017 adults who were surveyed over 2 weeks.
Measures
Demographics
Demographic data were collected on participant age, race, socioeconomic status (SES), sexual identity, marital status, education, geographic region, sexual activity status, and social media use. Categories used to measure race and geographic region were assessed based on the U.S. Census.38,39 To assess sexual identity, participants were able to choose from a list of options, including gay or lesbian, straight, bisexual, or something else. This variable was dichotomized into two categories: heterosexual (straight) and LGBQ+ (all others). Participants were also provided a list of options to choose from regarding marital status: (1) now married, (2) widowed, (3) divorced, (4) separated, and (5) never married; 40 the variable was then recoded into three categories: currently married, previously married (widowed, divorced, or separated), and never married. Age and SES were measured continuously in analyses. Please see Supplemental Material for all measures included in the study.
Sexual activity status
Sexual activity status was determined based on participants’ responses to the question “Over the past month (30 days), how often have you engaged in sexual activity with another person that involved stimulating one or both of your genital or anal areas by hands, mouth, or penis/vagina?” with varying frequency options. If participants selected anything other than “I have not engaged in any sexual activity over the past month,” they were coded as sexually active. Specific information about participants’ sexual activity was also obtained (see Table 1).
Sociodemographic characteristics (N = 522, unless otherwise noted).

For variables with missing data, percentages are reported out of the full sample size (N = 522). See Supplemental Material for exact wording of survey items. PHR: pubic hair removal; SD: standard deviation.
Social media use frequency
Social media use frequency was measured with one item from the Pew Research Center’s 2023 Survey, which read, “On average, how often do you use social media sites, such as Facebook, Instagram, Twitter, Snapchat, or TikTok?.” 41 Response options included: (1) almost constantly, (2) several times a day, (3) about once a day, (4) several times a week, (5) less often, and (6) never. The variable was dichotomized so that individuals who reported using social media sites at least once a day were coded as frequent users and those who used them less frequently were coded as non-frequent users.
Motivations
Participants who reported lifetime PHR were asked to rate their agreement, on a 4-point Likert scale, with a list of 20 team-created motivating factors for PHR with the stem, “Please rate your agreement with the following items: I remove my pubic hair because. . .” (example item: “It is a form of my self-expression”). See Table 2 for all items and frequencies.
Methods for and frequency of pubic hair removal among women who have ever removed pubic hair (N = 323, unless otherwise noted).

PHR: pubic hair removal.
Ipsos limited the responses for recent PHR to only the items selected in lifetime PHR for each participant. Therefore, percentages listed for only recent (past 30-day) PHR are out of the number of women who have EVER used that PHR method.
For the motivations items, the numbers presented indicate the percentage of women who answered “somewhat agree” or “strongly agree” to each item.
PHR (lifetime and past 30 days)
We assessed differences in characteristics of women who: (1) had ever engaged in PHR practices compared with those who had never engaged in PHR practices (lifetime PHR), and (2) had engaged in PHR over the past month compared with those who had not done so over the past month (recent PHR). The N for lifetime PHR was determined by participants’ responses to the items with the stem, “Which of the following methods have you ever (in your lifetime) used to either fully or partially remove your pubic hair?” Women were presented a list of five PHR methods (e.g., “hair removal creams/gels”) and those who selected “yes” to any method were coded as having engaged in lifetime PHR while all others were coded as never having engaged in lifetime PHR. To determine the N for recent PHR, participants were then asked, “Which of the following methods have you used in the last month (30 days) to either fully or partially remove your pubic hair?” and, similarly, women who selected “yes” to any method for this question were coded as having engaged in recent PHR while all others were coded as never having engaged in recent PHR. Importantly, Ipsos limited the responses for Recent PHR to only the items selected in Lifetime PHR (e.g., participants who reported only having shaved with a razor in their lifetime only received a question asking about their razor use in the past 30-days, while all other methods were immediately coded as “no”).
Statistical analysis
All analyses were conducted in IBM SPSS Statistics Version 28; Ipsos created statistical weights and all analyses use the weighted data. Missing data (ranging from 0% to 13.2% across predictor variables) was excluded listwise. 42 Analyses were conducted in three steps: (1) Descriptive statistics and frequency counts regarding women’s PHR prevalence, methods, and motivations were obtained; (2) various correlates of PHR (race/ethnicity, age, SES, sexual identity, marital status, education level, geographic region, sexual activity status, and social media use frequency) were examined between women who engaged in PHR (timeframes: (1) lifetime, and (2) within the past month [recent]); and (3) all variables were added to two multivariable logistic regression models to assess which factors contribute to the greatest odds of PHR among women (outcomes: (1) lifetime PHR, and (2) recent PHR). A sensitivity analysis in G*Power determined that our study was adequately powered to detect medium-sized effects.43,44
Results
Sample descriptives and PHR practices
All sociodemographic characteristics of participants are displayed in Table 1. A total of 323 women (62.0% of total sample) reported that they had ever removed their pubic hair (lifetime PHR) and 260 (49.8% of total sample) reported PHR in the last 30 days (recent PHR). As shown in Table 2, the most commonly reported PHR method was shaving with a razor or trimming with scissors, with 90.5% of women (n = 305) who had engaged in PHR reporting use of this method in their lifetime. Frequency of PHR ranged widely, with only 12 out of the 323 women who reported lifetime PHR (3.9%) acknowledging daily PHR, while larger percentages of women preferred to remove their pubic hair weekly (n = 69; 21.4%), monthly (n = 79; 24.6%), or every few months (n = 75; 23.3%). As shown in Figure 1, there was also a vast range of preferred pubic hair styles, with some of the most prevalent including trimmed (n = 82; 25.4%), partially removed but not fully bare (n = 77; 23.8%), and hair-free/bare (n = 75; 23.3%). The top three most highly endorsed PHR motivations were: feeling cleaner (83.2%), being more comfortable (82.6%), and believing they’d look better in a swimsuit (72.3%).

Participants’ preferred pubic hair styles (N = 323).
Bivariate test results
Table 3 displays all chi-square and ANOVA test results. In terms of both lifetime and recent PHR, women reporting sexual activity in the last 30 days (lifetime PHR χ2 = 46.85, p < 0.001; recent PHR χ2 = 61.96, p < 0.001) were statistically significantly more likely to have removed their pubic hair, compared with those reporting no recent sexual activity. There were also differences in PHR at both timepoints by age and education, with younger women having statistically significantly higher odds of engaging in PHR than older women (lifetime PHR t(520) = 6.556, p < 0.001; recent PHR t(520) = 7.171, p < 0.001) and women with higher education levels generally more likely to have engaged in PHR than those with less education (lifetime PHR F(3, 517) = 4.829, p = 0.003; recent PHR F(3, 517) = 3.256, p = 0.02). For lifetime PHR, LGBQ+ women displayed higher likelihood compared to heterosexual women (χ2 = 5.49, p = 0.02). Women who were previously married had lower odds of lifetime PHR compared with women who were currently or never married (χ2 = 6.71, p = 0.04). For recent PHR, frequent social media users were more likely to report PHR compared with infrequent users (χ2 = 4.16, p = 0.04), and those with higher SES were more likely to report PHR compared with those reporting lower SES (t(520) = −2.650, p = 0.008). There were no statistically significant differences in lifetime PHR by race, geographic region, or social media use, and no differences in recent PHR by race, sexual identity, marital status, or geographic region.
Differences between pubic hair removers and non-removers.

SES and age were measured continuously. Women who reported using social media sites at least once a day were coded as frequent users and those who used them less frequently were coded as non-frequent users. SAS: sexual activity status; SES: socioeconomic status; PHR: pubic hair removal; SD: standard deviation.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Multivariable regression results
To assess the strongest predictors of lifetime PHR, all variables were entered into one logistic regression model. The overall model was statistically significant (χ2 (15, N = 419) = 83.406, p < 0.001), with a Nagelkerke R2 value of 0.246. As displayed in Table 4, race, age, and sexual activity were all independent statistically significant predictors of lifetime PHR, controlling for other variables. Compared with White participants, Hispanic participants had lower odds of reporting lifetime PHR (odds ratio (OR) = 0.295, 95% confidence interval (CI) [0.156, 0.556]). Compared with younger participants, older women had lower odds of reporting lifetime PHR (OR = 0.960, 95% CI [0.943, 0.976]). Participants reporting recent sexual activity had greater odds of lifetime PHR (OR = 2.332, 95% CI [1.416, 3.840]).
Predictors of pubic hair removal.
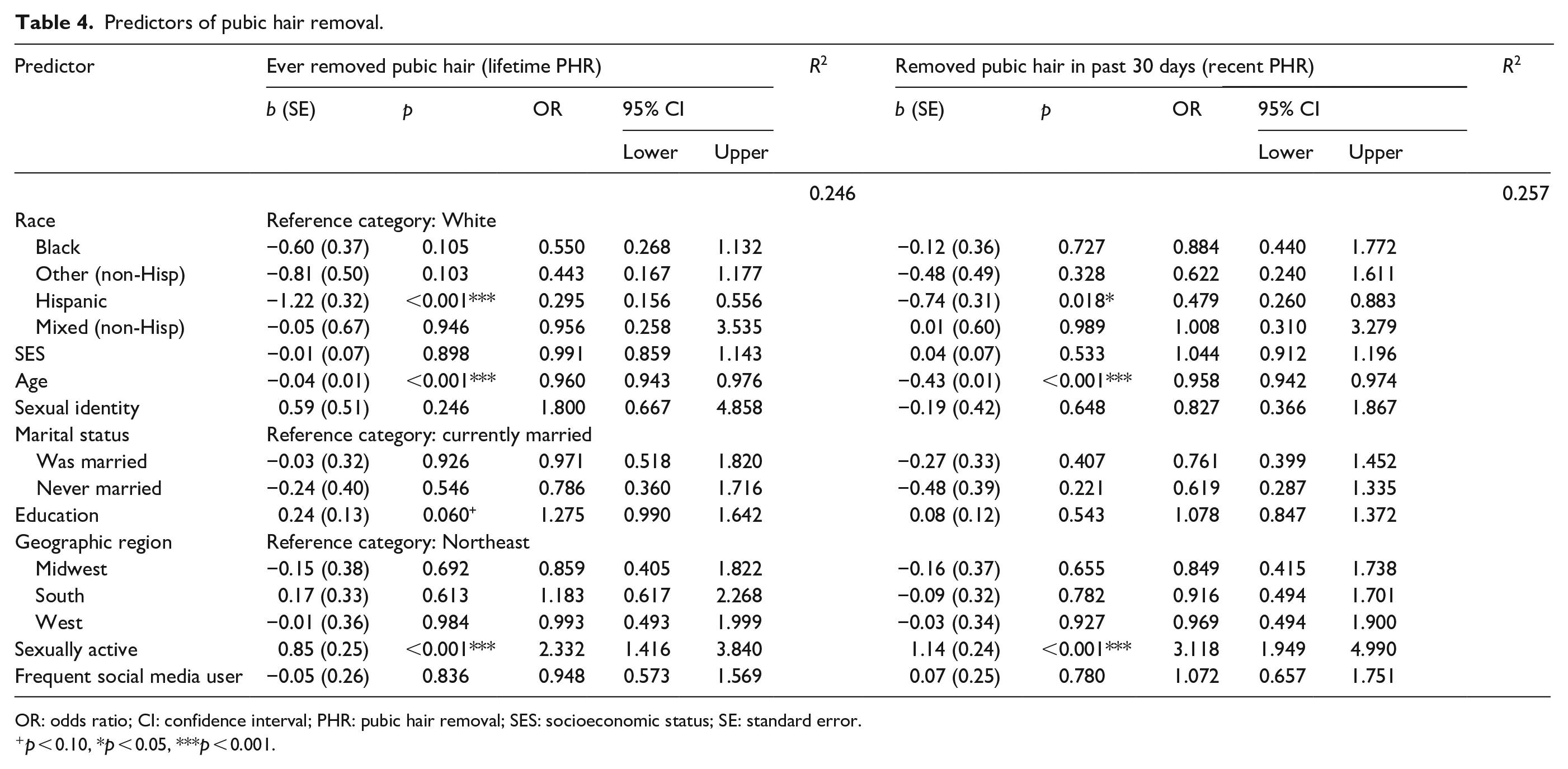
OR: odds ratio; CI: confidence interval; PHR: pubic hair removal; SES: socioeconomic status; SE: standard error.
p < 0.10, *p < 0.05, ***p < 0.001.
All variables were entered into a second logistic regression model to assess these variables’ predictive power of PHR within the past 30 days relative to one another. The overall model was statistically significant (χ2 (15, N = 419) = 90.908, p < 0.001), with a Nagelkerke R2 value of 0.257. The same three statistically significant predictors of lifetime PHR were also statistically significant predictors of recent PHR. Compared with White participants, Hispanic participants had lower odds of recent PHR (OR = 0.479, 95% CI [0.260, 0.883]). Compared with younger women, older women had lower odds of recent PHR (OR = 0.958, 95% CI [0.942, 0.974]). Participants reporting recent sexual activity had greater odds of recent PHR (OR = 3.118, 95% CI [1.949, 4.990]).
Discussion
The current study examined PHR practices in a nationally representative sample of women. In comparing the findings of our study with those of Rowen et al. 2 from a decade ago, several notable similarities and differences emerge. In both studies, the majority of participants reported a lifetime history of PHR, demonstrating that PHR has remained prevalent among women over the past decade, although a greater percentage of women (83.8%) reported lifetime PHR in 2016 2 compared to 62% in the current study, indicating a potential shift over time. The bimodal frequency distribution found by Rowen et al., 2 with monthly PHR having the highest frequency, was found in our study as well, indicating a stable pattern of PHR practices among women. Women’s chosen PHR methods have slightly evolved, with shaving/trimming with scissors being the most common methods in both studies but showing a greater prevalence in the current study. Feeling comfortable and looking better in a swimsuit also gained prominence in the current study compared to other studies. However, across studies and time, hygiene has been a leading motivator for women’s PHR.2,6,45
Women with higher education levels and higher SES had greater likelihood of engaging in PHR practices at various timepoints in our study, aligning with existing literature highlighting the influence of socioeconomic and educational factors on hair removal practices and body image ideals.46,47 Lifetime PHR also appeared to differ by marital status, with women who had previously been married displaying lower odds of PHR than both currently married individuals and those who had never married. Notably, our “previously married group” contained women who were divorced, separated, and widowed, suggesting that women who have endured these adverse, emotionally taxing experiences may prioritize self-care and hair removal differently.
Findings revealed an association between sexual activity and PHR: sexually active women were more inclined to engage in PHR than non-sexually active women. This is consistent with previous research1,6,48 suggesting that intimate relationships may play a role in shaping PHR decisions. Younger age was also predictive of higher lifetime and recent PHR in regression analyses, which aligns with a substantial body of literature supporting the relationship between age and hair removal.3,5,22,46
Multivariable logistic regression findings suggest that Hispanic women are less likely to remove their pubic hair compared to White women, both recently and in their lifetime. This highlights the importance of further investigating cultural factors and their influence on women’s PHR among different ethnic groups. A holistic understanding of the nuances in differing cultural beliefs, practices, or standards regarding PHR can offer valuable insights for researchers interested in developing or tailoring targeted interventions.
Providers should be aware of PHR’s prevalence and correlates among women and be prepared to discuss related health concerns, such as skin irritations and infections, in appointments with patients. Estheticians who specialize in PHR may utilize findings on preferred PHR methods and styles to tailor their services to meet client preferences and provide proper aftercare advice to clients. As LGBQ+ women reported higher likelihood of lifetime PHR (though this association did not remain statistically significant in the logistic regression models), it is essential to ensure inclusivity and sensitivity in these settings, providing tailored services for diverse clients. Awareness of generational differences in PHR practices can ensure tailored services and advice for different age groups.
Perhaps unsurprisingly, given the ubiquity of social media and its influence on modern beauty ideals, 49 frequent social media users had greater odds of recent PHR than infrequent users (though this association did not remain statistically significant in regression models). Social media may play a role in disseminating PHR trends and beauty standards, impacting women’s choices regarding PHR. More specifically, social media platforms hold tremendous potential as means for delivering information aimed at promoting healthy PHR habits among women.50,51 Skincare experts can leverage these platforms to engage with clients, patients, and the wider online community, fostering positive PHR practices. 52 TikTok and Instagram allow for providers and estheticians to create short, visually appealing educational videos and “live” Q+As to demonstrate proper PHR techniques, offer personalized recommendations, and emphasize the importance of maintaining skin health in general. 53
Limitations and future directions
The study relies on self-report data, which may be subject to biases and recall issues.54,55 Our cross-sectional design limits our ability to establish causal relationships or temporal associations. The sample, while nationally representative, may not be generalizable to certain priority populations, such as the unhoused, those who are incarcerated, and non-English speakers.
The PHR motivation item “I remove my pubic hair because people I follow on social media do it” showed very low agreement rates (under 10% of women in our sample). However, we want to be cautious not to make broader claims about social media’s effects on PHR practices from the responses to this one item, especially given that social media users were found to have higher odds of PHR in our study. The wording of the item prevents us from capturing content from influencers that participants did not “follow” on social media, and its vagueness may have left participants wondering whether the question was referring to seeing the actual act of PHR being done in a post, versus hairless bikini lines where PHR was implied.
Our sample of women was based on Ipsos’s standard measure of gender, which relies on binary categorization rather than acknowledging the diverse spectrum of gender identities. Future research should implement more inclusive measurement of gender to ensure a comprehensive understanding of PHR practices among individuals whose identities may not align with traditional binary constructs, as well as between cisgender and transgender women. Also, our demographic range was broad, including women aged 18–85 years. It is possible that different results for social media-related questions may emerge when examining a narrower, more homogenous age group such as young adult women or even college students more specifically, who are both more active on social media and potentially more susceptible to digital influence during their transitional life stage.56 –58
There is promising opportunity for collaborations between skincare professionals (e.g., dermatologists and estheticians) and behavioral scientists to conduct rich research and lead innovative public health interventions that not only address existing skin concerns but also promote long-term skin-related health among women. Researchers may investigate potential health implications associated with various PHR methods and practices, which could help guide skincare professionals to provide evidence-based advice to clients regarding preventive measures and treatment strategies, ultimately leading to more informed choices and improved patient/client satisfaction. For instance, research has produced mixed findings regarding PHR as a risk factor for STIs;9,59,60 however, evidence suggests that estheticians notice symptoms of potential STIs (e.g., herpes, genital warts) during waxing sessions and are even sometimes asked for advice by clients, despite most salons having no official protocols for handling this occurrence. 34 Recent research provides recommendations from a dermatological perspective regarding safer PHR practices, considering waxing and chemical depilation can produce allergic reactions or chemical burns.61,62 Although laser hair removal is generally considered safe, it can result in burns or changes to skin pigmentation if not performed correctly. 63 These findings can serve as a guide to ensure estheticians follow safety protocols and provide proper aftercare advice to minimize women’s health risks. Lastly, understanding women’s PHR motivations may facilitate more empathetic and customized approaches to skincare services. By fostering a culture of informed decision-making, these initiatives can empower women to make choices that align with their personal preferences and comfort levels while minimizing health-related risks.
Conclusion
The current study provides valuable insights and updated data on the prevalence, methods, and frequency of PHR among women in the United States. Findings may assist healthcare providers and estheticians in addressing their clients’ PHR concerns while promoting women’s health. Further research can continue to enhance our understanding of the factors influencing PHR practices and their implications for women’s health and psychological well-being.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241296982 – Supplemental material for Pubic hair removal practices among women: Findings from a U.S. nationally representative survey
Supplemental material, sj-docx-1-whe-10.1177_17455057241296982 for Pubic hair removal practices among women: Findings from a U.S. nationally representative survey by Hannah Javidi, Margaret L Walsh-Buhi, Rebecca F Houghton, Debby Herbenick and Eric R Walsh-Buhi in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.