
Abstract
Background:
Mental health problems among expectant and nursing mothers also affect their infants, partners, and families. While physical activity is a potential method for preventing postpartum depression (PPD), it is difficult for postpartum women to find the time for physical exercise. A recent study reported that improving communication between expectant couples can be used as a preventive intervention for PPD, and a systematic review and meta-analysis recently reported decreased facial emotional expressivity in individuals with different non-psychotic disorders. Therefore, we focused on facial muscle training and its potential as prevention for PPD.
Objective:
We evaluated the effectiveness of online facial muscle training with resonance vocalization using real-time video conferencing programs on the PPD of postpartum women at 2–3 months.
Design:
We recruited 20 postpartum women and used a single-arm, prospective, pre-post design.
Methods:
All subjects participated in 30 min of online facial muscle training with resonance vocalization once a week for 4 weeks. The first and final sessions were performed using a real-time remote chat application, and the second and third sessions were performed on demand. Scores on the Edinburgh Postnatal Depression Scale (EPDS) as an indicator of PPD were used as the primary outcome. Secondary outcomes included the appearance ratio of a happy facial expression, analyzed using FaceReader™; mood, which was measured using a visual analog scale; and stress level, which was measured using a smartwatch.
Results:
The training had a significant effect on EPDS, appearance ratio of a happy facial expression, and mood; however, it did not affect physical stress.
Conclusions:
In the future, intervention studies with a higher evidence level, such as a crossover randomized controlled trial, are required.
Plain language summary
The mental health problems of expectant and nursing mothers also affect their infants, partners, and families. However, it is difficult for postpartum women to find the time for physical exercise. So, we evaluated the effectiveness of online facial muscle training with resonance vocalization using real-time video conferencing programs. 20 subjects of postpartum women at two to three months participated in 30 minutes a time, once a week for four weeks. As the result, this training had a significant effect on the subjective mental health, happy facial expression and mood.
Keywords
Introduction
According to a scientific overview released by the World Health Organization, 1 the global prevalence of anxiety and depression increased significantly by 25% in the first year of the COVID-19 pandemic. Young people, women, and people with pre-existing mental disorders were the most affected. Moreover, many countries reported major disruptions in life-saving services for mental health, such as suicide prevention. As mental health problems among expectant and nursing mothers affect not only themselves but also their infants, partners, and families, support is urgently needed.
In Japan, a survey of about 3,500 pregnant women revealed that the social isolation of expectant women and a reduction of social support during the COVID-19 pandemic significantly increased postpartum depression (PPD). 2 In addition, despite a low infection rate and a mildly imposed lockdown, studies reported negative impacts of COVID-19 on postpartum women in Japan, such as weakening the bonds between mothers and babies, 3 loss of social support, 3 and loss of maternal autonomy in delivery and breastfeeding. 4 At least 13% of women who delivered and raised a baby during the COVID-19 pandemic had postpartum depressive symptoms above the cutoff (Edinburgh Postnatal Depression Scale (EPDS) ⩾13). 4 While a range of physical, genetic, and socioeconomic (e.g., quality of life or social support) factors put postpartum women at risk of mental health problems, a recent review, which included 122 studies, found that mothers with PPD suffer prolonged depression/depressive symptoms, have difficulties in their relationship with their partners, and have suicidal ideation. 2
Influence of PPD on infants
Infants can be affected by PPD in various ways, such as poor health and slow motor, cognitive, and language development. Furthermore, mother-to-infant bonding is often negatively affected, which has long-term consequences. 5 Previous studies have reported that children of mothers who experienced high stress during pregnancy were more likely to have cognitive and behavioral problems and were at higher risk for later mental health problems.6 –10 Prenatal anxiety and depression are also associated with changes in brain structure and function in infants and children.11 –14 Furthermore, infants of depressed and anxious mothers may have higher arousal and less attentiveness 15 and increased vulnerability to cognitive and emotional problems throughout their lifespan.16,17
These findings suggest that postpartum women need to perform self-care and undergo treatment, such as face-to-face or online therapy, as part of their daily lives to prevent mental illness.
Physical activity for preventing PPD
Physical activity (PA) is a potential method for preventing PPD. Findings from meta-analyses, reviews, and recent randomized trials have demonstrated encouraging results for the use of PA in the treatment and prevention of depression in the general population.18,19 PA has been demonstrated to improve the mood of people with mild to moderate depression as much as antidepressant medication, cognitive behavioral therapy, or social support. 20 For healthy pregnancies without contraindications, the current guidelines of the American Congress of Obstetricians and Gynecologists recommend that pregnant women perform 150 min of moderate to intense aerobic activity per week. 21 Furthermore, a meta-analysis reported that exercise is effective for PPD. 22 Interventions include aerobic exercise, stretching, yoga, coaching-based exercise, 22 and walking.22,23 However, PA interventions can be challenging. For instance, inactive people are more sensitive to criticism of their body weight and fitness, more readily embarrassed, and may derive less affective pleasure and reinforcement from exercise, 24 all of which may result in exercise avoidance, particularly when already in a state of mental stress. 25
In Japan, a recent study reported the development of a mental health program for expectant couples that focused on providing information for the prevention and early detection of PPD and examined its effectiveness. 26 Improving communication between expectant couples is a preventive intervention for PPD.27,28 Facial expressions are one means of communication, and a systematic review and meta-analysis recently reported decreased facial emotional expressivity in individuals with different non-psychotic disorders. 29 It has also been suggested that the spontaneous eye blink rate connects the missing link between aerobic fitness and cognition. 30 Subsequently, instead of PA, we focused on facial muscle movement.
Relationship between mental health and facial muscles
Facial muscles are innervated by the facial nerves; however, they are also innervated by the ventral vagus nerve and regulate the bronchi and the heart. These connections help orient people toward human connections and engagement in social interactions, providing more flexible and adaptive responses to environmental challenges, including social interactions. 31 Noser et al. reported that each psychosocial resource mediates the association between mental health and younger appearance. 32 The use of the zygomaticus major to study affect originated with pioneering research by Schwartz. In a series of directed imagery experiments, Schwartz and his colleagues found that unpleasant imagery elicited greater activity in the corrugator supercilii than pleasant imagery, whereas pleasant imagery elicited greater activity in the zygomaticus major.
A recent study suggested that functional electrical stimulation of the facial muscles involved in “genuine smiles,” rather than inhibiting corrugator muscle activity, may improve symptoms in individuals with major depressive disorder. 33 In addition, we previously performed voluntary facial muscle exercises with community-dwelling older women 34 and patients with Parkinson’s disease 35 and reported improvements in mental health and mood.
Recently, internet-based exercises have also been recognized as a suitable method to maintain fitness levels by performing safe, simple, and easy-to-implement exercises at home. 36 Particularly, medical services using real-time video conferencing programs have recently emerged as a means of supervising patient movements and preventing injuries during exercise sessions via the Internet. 37 This method of instruction has demonstrated a better effect than internet-based exercises with only one-way communication 38 and is also linked to patient motivation as patients can receive immediate feedback. 39 Hence, this study aimed to examine whether facial muscle training using real-time video conferencing programs (e.g., Zoom) can prevent PPD.
Methods
Study design and participants
In this pilot interventional study, we focused on the effects of a facial muscle training intervention program on PPD. We recruited 20 participants (2–3 months postpartum women) from a company that supports postpartum women (Baby Calendar, Inc., Tokyo, Japan) via their mailing list.
Inclusion and exclusion criteria
The inclusion criteria were as follows: Japanese postpartum women at 2–3 months who could participate in light- to moderate-intensity exercises and were not restricted from strenuous activities by their attending physician. The exclusion criterion was unsuitability to participate because of a severe disorder such as heart disease or neurological disease.
Research procedures
This study was conducted online from August 2022 to September 2022. All subjects participated in 30-min facial muscle training once a week for 4 weeks (same day of the week, same time). The facial muscle training program consisted of posture/breathing, vocalization, and facial muscle exercises (Table 1). An instructor with international qualifications in facial muscle training provided careful and accurate information. We compared pre- and post-intervention scores for each session (stress levels and visual analog scale (VAS)) and the first- and fourth-week scores (EPDS and FaceReader™).
Procedure for facial muscle training with resonance vocalization.

The first and final sessions were performed using a real-time remote chat application (Zoom Ltd., San Jose, CA, USA), and the second and third sessions were performed on demand.
Measurements
Subjective evaluation
Mental health
The primary outcome was PPD evaluated by the EPDS, 40 which was measured pre- and post-intervention for 1 month. The EPDS is a self-report questionnaire that focuses on the cognitive symptoms of PPD. It excludes somatic items that may generate false positives both during pregnancy and after childbirth. The EPDS consists of 10 items, each with a score of between 0 and 3 points, with a potential scale score of 0–30. The reliability and validity of the Japanese version have been verified. 41 The cutoff score for suspected PPD in the Japanese population is ⩾9.
Mood
VAS 42 was originally used to evaluate pain using a 100-mm line drawn on a blank sheet of paper; the left end is “no pain at all,” and the right end is “the worst pain imaginable.” It is now also widely used for evaluating mood, and McCormack et al. reported its reliability and validity. We asked, “What is the score for your current mood?” immediately pre- and post-training. The left end was “feeling bad,” and the right end was “feeling good.” The mood state was scored between 0 and 100 points and this was all written in Japanese.
Objective evaluation
Facial expression (happiness)
Secondary outcomes included facial expression, which was analyzed using FaceReader (Noldus, Wageningen, Netherlands) (Figure 1), 43 to assess the appearance ratio of a happy facial expression pre- and post-intervention for 1 month. FaceReader is a comprehensive professional software for face coding, which was developed and validated based on psycho-emotional theories, especially Ekman’s research and Facial Action Coding System (FACS). This software allows the coding of emotions and neutral expressions such as happiness, sadness, anger, disgust, fear, surprise, and contempt. A study of Japanese subjects reported that happy and neutral facial expressions were consistent with VAS results. In the present study, participants were asked to smile pre- and post-intervention, and photographs were taken. At that time, to control their emotions, we asked participants to “imagine your baby and smile,” and we then analyzed the smile using FaceReader and calculated the happiness value (%).

Analysis by FaceReader™.
Stress level
We used vivosmart®4 smartwatches (Garmin, Olathe, KS, USA) 44 to estimate heart rate. Stress levels were calculated by evaluating autonomic activities based on changes in heart rate or the interval between pulses. The reliability of the estimated heart rate calculated using a smartwatch was confirmed. The vivosmart4 was selected because it is noninvasive, lightweight (16.4 g), and small (15 × 10.5 × 197 mm); thus, it is not considered burdensome for postpartum women.
Statistical analysis
The sample size was calculated using G*Power3.1.9.2 with effect size = 0.67, 45 α error = 0.05, statistical power = 0.8, and assuming a dropout rate of approximately 20%. The effect size was decided based on a meta-analysis of strength training on improving depression. All results were run on SPSS 29.0.1.0 software (IBM, New York, NY, USA), and p-values below 0.05 were considered significant. Comparisons between pre- and post-intervention were performed using the paired t-test for EPDS and Wilcoxon signed-rank test for facial expression, stress level, and mood.
Results
We enrolled 20 women at 2–3 months postpartum, and there were no dropouts. The baseline characteristics are illustrated in Table 2.
Participant characteristics.

SD: standard deviation.
After 4 weeks, the EPDS scores significantly decreased from 5.5 ± 3.1 to 3.1 ± 2.2 (Table 3).
Changes in EPDS.

EPDS: Edinburgh Postnatal Depression Scale; SD: standard deviation.
p < 0.01.
After each facial muscle training session, there was a significant increase in VAS scores (Table 4).
Changes in mood.

IQR: interquartile range.
p < 0.01.
A repeated measurement one-way ANOVA revealed no significant difference in the mean score of mood among the four times it was evaluated pre-intervention (p = 0.431).
After 4 weeks, the appearance ratio of a happy facial expression significantly increased from 87.3 (mean %) to 91.8 (mean %) in FaceReader (Table 5).
Changes in appearance ratio of a happy facial expression.
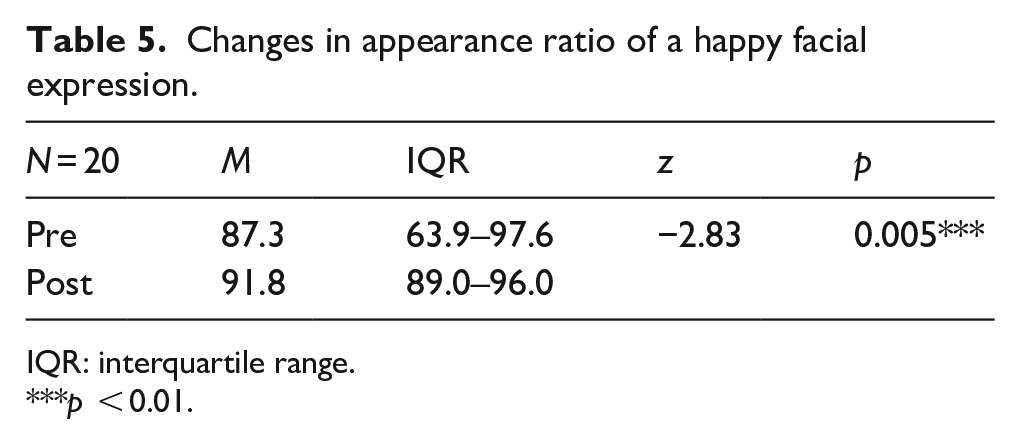
IQR: interquartile range.
p < 0.01.
After 4 weeks, there were no significant differences in stress levels (Table 6).
Changes in stress levels.

IQR: interquartile range.
Discussion
Subjective evaluation of facial muscle training on mental health
The average EPDS score of Japanese postpartum women was 4.5 ± 4.0 (calculated from Tokumitsu et al., 2020). 46 There was a significant decrease after the intervention, suggesting that the facial muscle training program was effective as a preventive intervention for PPD. However, EPDS scores can decrease during the period of physical and mental recovery after childbirth. Therefore, the decrease in scores in this study needs to be examined to determine if higher-quality interventions can achieve a greater reduction.
The mood score significantly increased after each training session; thus, the training improved subjective mood and elicited positive emotions. These findings support those of previous studies conducted on older women 34 and patients with Parkinson’s disease. 35 Our findings suggest that facial muscle training improves subjective mental health and is effective as a preventive intervention for postpartum women.
Objective evaluation of facial muscle training on mental health
With facial expression analysis, the appearance ratio of a happy facial expression was significantly increased after the intervention. This finding supports the results of a previous study 32 in which the degree of mental health improved, and positive emotions were recalled. Thus, it is necessary to examine the relationship with autonomic nerve activity as an objective evaluation of the physical effects of training.
In this study, we demonstrated the effects of facial muscle training on the stress levels obtained using a smartwatch. No significant changes were observed in stress levels after the intervention. In addition, the EPDS questionnaire, appearance ratio of a happy expression, and VAS revealed that the participants’ mental health levels increased. In addition, there was no significant difference compared to mood scores before training. These findings suggest that the training was not stressful for postpartum women.
The algorithm used to analyze stress levels by the vivosmart4 smartwatch is unknown. 47 According to a pilot study examining stress status using smartwatch stress levels in postpartum women, the vivosmart4 smartwatch used in this study calculated the root mean square of the successive differences (RMSSD) between consecutive adjacent RR interval (the time interval between the previous RR wave and the R wave) intervals in heart rate variability. 48 RMSSD is an index calculated from a time domain analysis, and autonomic nerve activity includes calculation methods such as frequency domain analysis and time domain analysis. Nonlinear heart rate variability measurement and linear analyses, such as time-domain and frequency-domain analyses, have been used to assess autonomic nerve activity. 49 In the future, it is necessary to examine the characteristics of autonomic nerve activity to measure the effect of facial muscle training.
No participants dropped out of the facial muscle training, and all were able to practice the entire protocol. Thus, our findings suggest that facial muscle training may help induce moderate pleasant feelings in inactive people.
Limitations of the present study
This study used a single-arm design as an exploratory preliminary study. However, there were several limitations. First, given the single-arm study design, it is unclear whether the improvement in mental health was because of facial muscle training or the passage of time after childbirth. Second, it is unclear whether the facial muscle training program was carried out accurately because it was conducted online and on-demand for the second and third sessions. Third, it is unclear whether the training was carried out accurately, as studies examining in-person and on-demand implementation rates have reported that on-demand is lower. Fourth, there may have been selection bias for postpartum women who had a high motivation and interest in their mental health.
Conclusion
The results of the 4-week real-time online and on-demand facial muscle training program for postpartum women demonstrated that this training program can be used to improve the mental health of postpartum women. In particular, the mood and appearance ratio of a happy facial expression improved. In the future, intervention studies with a higher evidence level, such as a crossover randomized controlled trial (RCT), could be used to alleviate these limitations. We intend to implement an RCT, evaluate reliability and validity, and move toward clinical application.