
Abstract
Background:
Low birth weight (LBW) has been established as a major determinant of neonatal mortality and morbidity. However, there is no evidence of the effectiveness of different types of physical exercise (PE) at different intensities during pregnancy to prevent LBW.
Objectives:
To compare the effectiveness of different types of PE at different levels of intensity in pregnant women to prevent LBW.
Design:
A systematic review and network meta-analysis was performed according to the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols for Network Meta-Analysis extension statement.
Data Sources and Methods:
We searched the PubMed, Cochrane Central Register of Controlled Trials, Scopus, and Web of Science databases from inception to November 2023. We included randomized controlled trials (RCTs). A random effects method was used to calculate the pooled mean difference (MD). The effect of each intervention was calculated using a network meta-analysis with a frequentist perspective.
Results:
Forty-three RCTs were included in the systematic review, and 38 RCTs were included in the network meta-analysis. In the general population, although no significant results, the MDs for light-moderate strength, moderate-vigorous strength, and moderate-vigorous Pilates exercises were favorable for preventing LBW. Furthermore, moderate-vigorous strength exercise was effective to prevent LBW, reporting significant MD compared to control groups in the healthy population (310.00, 95% confidence interval: 78.40, 541.60; I2 = 81.3%).
Conclusion:
Strength exercises at a moderate-vigorous intensity could be a potential strategy for the prevention of LBW in the healthy population. However, our findings should be interpreted with caution because the overall risk of bias was between “some concerns” and “high,” and the overall certainty of the evidence was low.
Registration:
PROSPERO CRD42023401770.
Introduction
Birth weight (BW) is a crucial neonatal health indicator. 1 Adequate BW (2,500–4,000 g) 2 reduces the likelihood of long-term chronic diseases 3 and birth-related complications. The World Health Organization defines low BW (LBW) as a BW less than 2,500 g. 4 LBW has been established as a major determinant of neonatal mortality and morbidity. 5 Approximately 15%–20% of children worldwide are born with LBW, which is a major global health problem. 4 In addition, LBW has been associated with hypertension, cardiovascular diseases, and type 2 diabetes mellitus in adulthood.6,7 Crucial aspects associated with LBW include pregnancy-related factors, sociodemographic characteristics, and lifestyle behaviors.2,8,9
Maintaining unhealthy lifestyle habits during pregnancy can lead to health risks and pregnancy complications. 10 In this sense, regular and tailored physical exercise (PE) during pregnancy provides a wide range of benefits for both mothers and infants, although there may be controversy depending on the type of PE. These benefits include promoting maternal physical and mental well-being, 11 preventing loss of muscular and cardiovascular fitness, 12 reducing the incidence of preterm delivery, gestational pathologies, and excessive maternal weight gain, and preventing the onset of LBW in newborns,13,14 among others. To obtain the benefits of PE, it is important that each woman’s training regimen be planned and tailored specifically to her needs. 11
Pregnant women without prior contraindications are recommended to perform at least 150 min of aerobic, strength, and stretching PE per week, at moderate intensity (and also vigorous if they already exercised at this intensity before pregnancy), from three to seven times per week to acquire greater benefits.13,14 Several recent studies and guidelines have indicated that pregnant women, except those at risk, can engage in PE during pregnancy without increasing the risk of miscarriage, neonatal death, preterm birth, or LBW.13–15
Previous systematic reviews16–20 have examined the impact of PE on various neonatal outcomes, and, in addition, a previous meta-analysis 16 of 14 randomized controlled trials (RCTs) demonstrated the effectiveness of prenatal PE on BW adequacy. However, there is currently no evidence synthesis on the effectiveness of different types of PE and their intensity levels during pregnancy in reducing the likelihood of LBW. By considering type and intensity together, exercise recommendations can be tailored to the specific needs and preferences of women during pregnancy. The American College of Sports Medicine advocates the principles of individualized exercise prescription (i.e., specificity, overload, progression, and variation) and analysis of both type and intensity helps to apply these principles effectively (i.e., selecting exercises that target specific health outcomes and adjusting intensity levels to provide appropriate challenges while avoiding overtraining or injury).21,22 Therefore, the aim of this systematic review and meta-analysis is to compare the effectiveness of exercise types and intensities during pregnancy in preventing LBW.
Methods
Registration
This systematic review with NMA (PROSPERO registration number: CRD42023401770) was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols statement extension for network meta-analysis (PRISMA-NMA) guidelines 23 (Supplemental Methods) and the Cochrane Collaboration Handbook. 24
Search strategy
Two researchers (VD-G and AS-L) independently conducted a systematic search of the PubMed, Cochrane Central Register of Controlled Trials, Scopus, and Web of Science databases from their inception to November 1, 2023. The search strategy included relevant terms related to (i) “pregnancy,” (ii) “exercise,” (iii) “birth weight,” and (iv) “randomized controlled trial.” The full search strategy is detailed in the Supplemental Methods. The reference lists of the included studies and previous systematic reviews were checked to identify additional relevant RCTs.
Selection criteria
The inclusion criteria were as follows: (i) type of studies: RCTs with two or more comparison groups; (ii) participants: pregnant, over 18 years of age, apparently healthy (including all body mass index (BMI) categories) or with frequent cardiometabolic disorders that occur during pregnancy, such as hypertensive disorders or gestational diabetes mellitus (GDM); (iii) type of intervention: studies reporting any type of structured PE intervention (e.g., strength, aerobic, combined [aerobic and strength], interval training, Pilates), and its intensity; and (iv) type of outcome measure: BW as a continuous variable. Exclusion criteria were studies that analyzed participants with a chronic disease prior to pregnancy and that combined PE with a pharmacological or other health intervention (e.g., diet) and the results could not be extracted separately.
The values for each intensity level.

Unified intensity levels according to the classification developed by the American College Sports Medicine.21,22
HR: heart ratio; %HRmax: percent of maximal HR; %HRR: percent of HR reserve; VO2R: oxygen uptake reserve; %VO2max: percent of maximal oxygen uptake.
Data extraction
Data extraction was performed independently by two investigators (VD-G and AS-L). The following data were collected from each study that met the above criteria: (i) author, year and country; (ii) population characteristics (total sample size, mean age, and type of population); (iii) intervention characteristics (frequency, intensity, type of PE, time, duration and sample size of intervention, and control groups); (iv) BW as neonatal outcome; and (v) maternal outcomes (length of gestation, BMI, and gestational weight gain).
Categorization of interventions
The classification of the PE interventions and intensity levels followed the American College Sports Medicine21,22 statements and were detailed in Supplemental Methods and Supplemental Table 1.
Risk of bias assessment
Two investigators (VD-G and AS-L) independently assessed the risk of bias of the included RCTs using the Cochrane Collaboration tool for assessing the risk of bias. 24 Risk of bias was evaluated according to five domains: selection bias, performance bias, detection bias, attrition bias, and reporting bias. Overall bias was classified as “low risk of bias” if the manuscript was classified as “low risk” in all domains, “some concern” if there was at least one domain with the rating “some concern,” and “high risk of bias” if there was at least one domain with a “high risk.” Disagreements were handled by consensus or by a third reviewer (BB-P).
Grading the quality of evidence
The Grading of Recommendations, Assessment, Development, and Evaluation tool was used to assess the quality of evidence and provide recommendations. 25 Each outcome received a score of high, moderate, low, or very low evidence, depending on study design, risk of bias, inconsistency, indirect evidence, imprecision, and publication bias.
Statistical analysis/meta-analysis
The included RCTs were qualitatively summarized in an ad hoc table describing the types of direct and indirect comparisons of the different types of PE and their intensity levels. All analyses were performed according to the type of population, that is, total pregnant (GDM, healthy, overweight, or obesity) or healthy pregnant population (without GDM, overweight, or obesity). Our NMA was conducted in accordance with the PRISMA-NMA statement 23 under a frequentist perspective by following these steps:
First, a network geometry graph was used to depict the trials in the NMA for the total population. In this graph, the size of the nodes represents the number of participants in RCTs that received the intervention identified in the node, and the thickness of the solid line connecting the nodes represents the number of participants in RCTs that directly compared two interventions. 26 In addition, this graph was performed including only healthy pregnant women.
Second, consistency was assessed by testing whether intervention effects estimated from direct comparisons were consistent with those estimated using indirect comparison methods. For this purpose, we used the Wald test, and local inconsistency was assessed using the lateral splitting method.
Third, a comparative assessment of the intervention effect was performed using a standard pairwise meta-analysis for comparisons between PE interventions and non-PE control groups or other PE interventions. The DerSimonian‒Laird random effects method was used to calculate a pooled mean difference (MD) and corresponding 95% confidence intervals (CIs). 27 In addition, these analyses were performed including only healthy pregnant women (without risk factors/comorbidity). Statistical heterogeneity was assessed by calculating the I2 statistic, which ranges from 0% to 100%. According to the I2 values, heterogeneity was classified as not important (0%–30%), moderate (30%–50%), substantial (50%–75%), or considerable (75%–100%). 24 The corresponding p values were also considered. Finally, the τ2 statistic was calculated to determine the magnitude and clinical relevance of heterogeneity. A τ2 estimate of 0.04 can be interpreted as low, 0.14 as moderate, and 0.40 as a substantial degree of clinical relevance of heterogeneity. 28 We created both forest plots and a league table to depict these results.
Fourth, the effect of each intervention was calculated using NMA with a frequentist perspective. 29 The frequentist perspective draws a conclusion based on the level of statistical significance and the acceptance or rejection of a hypothesis. In addition, these analyses were performed including only healthy pregnant women.
Fifth, sensitivity and meta-regression analyses were used to assess transitivity, and we verified that all study participants included in the NMA had, on average, a similar baseline effect distribution. Sensitivity analyses (systematic reanalysis by removing studies one at a time) were conducted to assess the robustness of the summary estimates. Furthermore, consistent with previous evidence supporting a minimum of 8 weeks for exercise effectiveness, 12 complementary analyses were carried out only with RCTs that applied 8 weeks or more of PE intervention (also excluding those that did not report duration). Meta-regression analyses were performed to determine whether mean maternal age, length of gestation, BMI, gestational weight gain, duration and frequency of intervention, as continuous variables, modified the effect of PE interventions and their intensities on BW.
Sixth, once the effect size estimates of the effectiveness of the PE interventions and their intensity levels were calculated, the interventions were classified and graphically presented using rankograms. 30 In addition, the surface under the cumulative ranking curve (SUCRA) was calculated for each intervention. The best intervention would have a SUCRA value close to 1, and the worst intervention would have a value close to 0. 26 Finally, these analyses were performed including only healthy pregnant women.
Seventh, publication bias was assessed by visual inspection of funnel plots and Egger’s test (significant when p < 0.10). 31 All analyses were performed in Stata SE software, version 15 (Stata, College Station, TX, USA).
Results
Study characteristics
A total of 43 studies were included32–74 in the systematic review, and 38 studies32–35,37–62,64–67,71–74 were included in the NMA (Figure 1). All included studies were RCTs published between 1997 and 2022 in Spain,34,36,37,40,41,53,55–61,68–70,74 Brazil,49,50,54,63 USA,38,51,52,64 Norway,45,48,66 Australia,46,67 China,32,71 New Zealand,35,44 Argentina, 62 Croatia, 33 Iran, 47 Netherlands, 43 Poland, 72 Portugal, 39 Sweden, 73 Switzerland, 42 and Turkey. 65
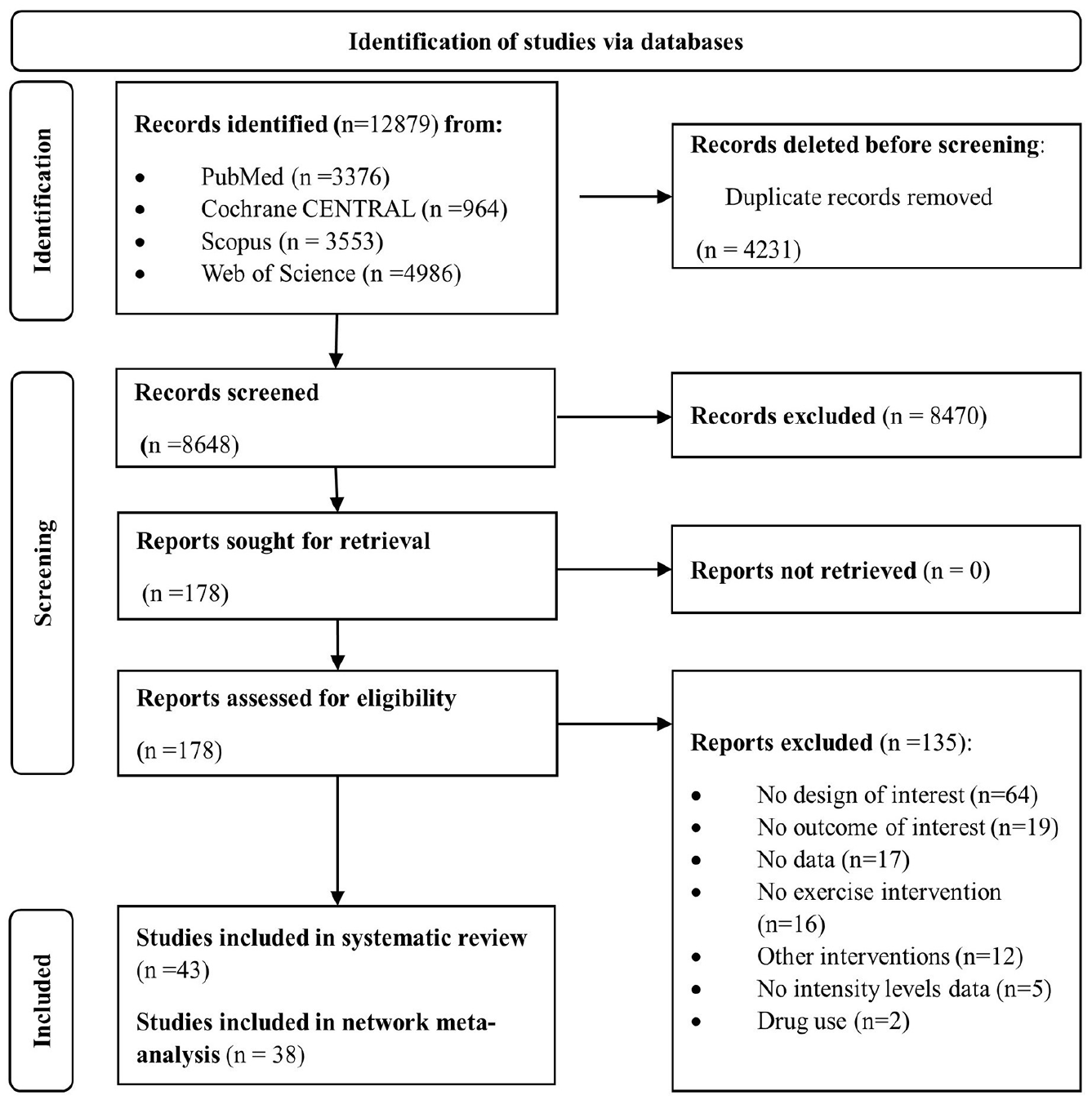
Flowchart of the study selection.
Participants and interventions
The total sample size of the included studies was 9,240 pregnant women (mean age range: 24.0–34.5 years, mean BMI range: 21.5–32.2 kg/m2). The heathy pregnant population had a mean age range of 24.0–34.5 years and a mean BMI range of 21.5–27.0 kg/m2. The groups that received the intervention—a total of 4,395 pregnant women, of whom 3,618 were healthy—performed different types of structured and repetitive exercise (e.g., aquatic activities, exercise bike, dance) at different intensity levels, frequencies, times, and durations. Only six RCTs performed home-based exercise interventions, both supervised 46 and unsupervised,34,35,44,64,67 and the rest applied supervised center-based exercise interventions. In addition, only four studies applied aquatic exercise interventions37,55,62,63 and the remaining RCTs applied weight-bearing exercises. Regarding the types of PE and their intensity levels the RCTs comprised light aerobic exercise (A-Lig),41,56 light-moderate aerobic exercise (A-LigMod),33,39,55,57,62 moderate aerobic exercise (A-Mod),35,38,52–54,64 moderate-vigorous aerobic exercise (A-ModVig),44,45,49,51,74 light combined exercise (Comb-Lig),40,58,60 light-moderate combined exercise (Comb-LigMod),34,43,47 combined moderate-vigorous exercise (Comb-ModVig),42,48,50,66,69 light-moderate strength exercise (S-LigMod), 59 moderate strength exercise (S-Mod), 61 moderate-vigorous strength exercise (S-ModVig),71,73 moderate-vigorous interval training (IT-ModVig),32,46,67 and moderate-vigorous Pilates (P-ModVig).65,72 Regarding the characteristics of the intervention, the duration of exercise ranged from 2 to 30 weeks, the frequency ranged from two to five times per week, and the duration ranged from 15 to 60 min. The main characteristics of the included studies are shown in Supplemental Table S1.
Risk of bias and certainty of evidence
Of the 43 studies, 46.5% had some concerns about risk of bias, 32.5% had a high risk of bias, and 20.9% had a low risk of bias. Regarding the domains, 72.0% had “some concerns” about the selection of reported results. In turn, a low risk of bias was reported in most RCTs when assessing missing data or outcome measures (Supplemental Figures S1 and S2). Furthermore, the PE interventions included in this NMA were rated with moderate (8.3%), low (50%) or very low (41.6%) certainty of evidence (Supplemental Table S2).
Comparative effect of different types and intensity levels of PE on LBW
Considering the total pregnant population (i.e., GDM, healthy, overweight or obesity),32–35,37–62,64–67,71–74 Figure 2 shows the network geometry plot of the comparisons evaluating the effect of different PE interventions and intensity levels on LBW. Supplemental Table S3 shows the MD estimates from the direct studies (upper diagonal) separately from the indirect MD estimates (lower diagonal) in the total pregnant women. Both in the pairwise analyses (upper diagonal) and in the frequentist NMA, although no significant results were shown, the MD estimates for A-LigMod (22.04, 95% CI: −60.06, 104.14), Comb-LigMod (12.95, 95% CI: −109.88, 135.78), S-LigMod (34.00, 95% CI: −106.97, 174.97), S-ModVig (130.88, 95% CI: −30.37, 292.14) and P-ModVig (58.41, 95% CI: −104.44, 221.25) were in favor of PE interventions to prevent LBW compared to the control groups.

Network of available comparisons between different types of physical exercise and intensity levels on low birth weight in the total pregnant women (GDM, healthy, overweight, or obesity).
Considering only the healthy population (i.e., without GDM, overweight or obesity),33,34,37–42,44,51–53,55–60,62,65,66,72–74 Figure 3 shows the network geometry plot of the comparisons evaluating the effect of different PE interventions and intensity levels on LBW. Supplemental Table S4 shows the MD estimates from the direct studies (upper diagonal) separately from the indirect MD estimates (lower diagonal). In both the pairwise analysis (upper diagonal) (310.00, 95% CI: 100.49, 519.51) and the frequentist NMA (310.00, 95% CI: 78.40, 541.60), significant MDs were shown for the S-ModVig intervention to prevent LBW compared to the control groups. Furthermore, S-ModVig significantly increased BW compared to the other PE interventions, except for P-ModVig.

Network of available comparisons between different types of physical exercise and intensity levels on low birth weight only in healthy pregnant women (without GDM, overweight, or obesity).
Probabilities
In the total population included, the S-ModVig exercise had the highest SUCRA (91.4%) and the highest probability of being the best intervention (59.6%). In addition, P-ModVig exercise, with a SUCRA value of 73.3%, and S-LigMod exercise, with a SUCRA of 66.4%, are also likely to be among the best interventions (Supplemental Table S5 and Supplemental Figure S3). When the analyses were performed in the healthy population, S-ModVig exercise also had the highest SUCRA (98.7%) and the highest probability of being the best intervention (93.5%) (Supplemental Table S6). Similarly, when analyses were conducted in those studies reporting an intervention duration ⩾8 weeks, S-ModVig had the highest SUCRA (99%) and the highest probability of being the best intervention (93.3%) (Supplemental Table S7).
A-Lig (I2 = 0.0%, τ2 = 0.0), A-Mod (I2 = 26.7%, τ2 = 5.9), A-ModVig (I2 = 0.0%, τ2 = 0.0), Comb-Lig (I2 = 0.0%, τ2 = 0.0), and P-ModVig (I2 = 0.0%, τ2 = 0.0) exercises versus control exercises showed nonsignificant heterogeneity. A-LigMod (I2 = 33.0%, τ2 = 2.2) and Comb-LigMod (I2 = 33.0%, τ2 = 3.9) exercises showed moderate heterogeneity. The Comb-ModVig (I2 = 51.5%, τ2 = 5.2) and IT-ModVig (I2 = 70.5%, τ2 = 1.8) exercises showed substantial heterogeneity, and the S-ModVig exercises showed considerable heterogeneity (I2 = 81.3%, τ2 = 4.3) (Supplemental Table S8).
Sensitivity analysis, meta-regression models, and publication bias
The pooled MD estimate was not significantly changed (either in magnitude or direction) when individual study data were removed from the leave-one-out sensitivity analysis. After excluding RCTs that did not report or had less than 8 weeks of PE duration,39,45,49,52,60,64,67,71 Supplemental Table S9 shows the MD estimates from the direct studies (upper diagonal) separated from the indirect MD estimates (lower diagonal) of those studies with intervention durations ⩾8 weeks. In both the pairwise analysis (upper diagonal) (310.00, 95% CI: 100.49, 519.51) and the frequentist NMA (310.00, 95% CI: 72.32, 547.68), significant MDs were shown for the S-ModVig intervention to prevent LBW compared to the control groups. In turn, the results in the NMA showed that the S-ModVig provided significant MDs for preventing LBW compared to all other exercises except the P-ModVig. Supplemental Figure S4 shows the network geometry plot of comparisons assessing the effect of different PE interventions and intensity levels on LBW in studies reporting a duration of interventions ⩾8 weeks. Furthermore, random-effects meta-regression models showed that length of gestation and PE duration could influence the pooled MD estimate for the effect of A-LigMod exercise versus the control group on LBW (p = 0.041 and p = 0.035, respectively), and maternal age could influence the pooled MD estimate for the effect of IT-ModVig exercise versus the control group on LBW (p = 0.014) (Supplemental Table S10). Finally, no publication bias was shown in the included comparisons (Supplemental Figure S5).
Discussion
This NMA evaluates the effectiveness of different types of PE during pregnancy and their intensity levels in preventing of LBW. When we performed the analyses in healthy pregnant women, S-ModVig exercise was effective to prevent LBW, as it increased the weight of the newborns, maintaining the values within an adequate weight. Moreover, our results showed that S-LigMod, S-ModVig, and P-ModVig exercises were most likely to be the best interventions for preventing LBW in the general population. These findings should be interpreted with caution due to the overall risk of bias within some concerns to high and the overall low certainty of evidence.
The evidence on the effects of PE during pregnancy is controversial. The physiological changes in the mother during exercise and the effects on the newborn depend on the type, frequency, intensity, and duration of exercise. 75 Some studies suggest that exercising during pregnancy may pose risks to the infant, such as malnutrition or impaired fetal growth, due to competition for energy substrates.76,77 However, several reviews including RCTs in different populations (i.e., GDM, healthy, overweight, or obese) supported that PE was safe on BW, newborn body composition3,17–20,78,79 or on factors associated with LBW, such as preterm delivery or small for gestational age.80–83 Our study confirms these findings suggesting that the types of PE analyzed and their different intensities do not pose a risk for BW, since an adequate range (i.e., >2,500 and <4,000 g) was reported in all intervention groups. In this sense, the choice of PE routine in the clinical setting should consider the needs, characteristics, and preferences of each woman.
Strength exercises during pregnancy are within current guideline recommendations13,14; however, aerobic exercises are more frequently recommended,84,85 possibly due to the lack of available evidence on the effect of strength exercises in pregnant women. The mechanisms by which strength exercises tend to increase BW could be explained by a greater reduction in the percentage of fat mass and an increase in muscle mass compared to other types of PE. 86 Maternal lean mass has shown a correlation and predictive ability with BW.87,88 In this sense, fluid retention may be relevant since body water (i.e., the main component of lean tissue) is closely related to plasma volume, which in turn correlates with BW. 87
Additionally, higher intensity (light to moderate or moderate to vigorous) may favor some maternal physiological mechanisms, such as improved oxidative capacity and increased postexercise oxygen consumption. These mechanisms lead to a decrease in the percentage of body fat 89 and an increase in the percentage of maternal lean mass, benefiting the increase in maternal body water. In turn, moderate-intensity exercise can improve the functional capacity of the placenta, increasing the supply of nutrients and favoring fetal growth.52,90 Our results support strength exercises in healthy pregnant women at a moderate-vigorous intensity to prevent LBW. However, only two RCTs have reported these results,71,73 therefore, more studies are needed to determine the effectiveness and safety of strength exercises in pregnant women and BW as neonatal outcome.85,91
This NMA has some limitations that should be acknowledged. First, the nature of RCTs comparing PE interventions makes it difficult to avoid methodological biases that may have affected the estimates, including blinding or possible participation in PE routines of pregnant women in the control groups. Second, different scales were used to measure the intensity of PE. Third, due to the paucity of studies in some intervention groups, our results should be interpreted with caution. Fourth, it was not possible to analyze the effectiveness of the types of PE and their intensities together with other characteristics of the intervention, such as frequency, duration, or modality applied (weight-bearing versus aquatic), because further stratification would lead to a limited number of studies in additional subgroups to analyze. Fifth, some types of PE, such as Tai Chi or Yoga, were not included because their studies did not report data on intensities. A previous meta-analysis showed that Yoga may be an effective complementary strategy to improve neonatal birth outcomes 92 ; however, our NMA focused on a comprehensive analysis of PE (type plus intensity), and these types of exercises could not be considered. Finally, although the studies were conducted in different types of populations (e.g., different BMI categories) and continents (i.e., Asia, Europe, North America, Oceania, and South America), the generalizability of our findings is limited due to insufficient data on covariates relevant to the study associations (e.g., diet quality and exercise characteristics such as method of delivery or setting),93,94 the overall risk of bias within some concerns to high, and the overall low certainty of evidence.
Conclusions
To our knowledge, this is the first NMA to compare the effectiveness of PE interventions and their intensity levels during pregnancy on newborn BW. S-ModVig could be understood as a first-line approach for the prevention of LBW in the healthy population. These findings may have important clinical implications for antenatal care and maternal health, suggesting that strength training at moderate to vigorous intensities could be included in antenatal exercise recommendations, always considering individual characteristics and pregnancy status. Furthermore, our study suggests that the different types and intensities of PE analyzed were safe for BW; therefore, the choice of exercise routine in the clinical setting must be precise and individualized, considering the needs, characteristics and preferences of each woman, as well as her potential risks of LBW. However, our findings should be interpreted with caution because the overall risk of bias was between “some concerns” and “high,” and the overall certainty of the evidence was low. High-quality RCTs are needed to strengthen our conclusions and establish solid recommendations.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241276253 – Supplemental material for Comparative effect of different types of physical exercise and intensity levels on low birth weight: A systematic review and network meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057241276253 for Comparative effect of different types of physical exercise and intensity levels on low birth weight: A systematic review and network meta-analysis by Valentina Díaz-Goñi, Iván Cavero-Redondo, Bruno Bizzozero-Peroni, Eva Rodríguez-Gutiérrez, Carlos Pascual-Morena, Irene Sequí-Domínguez, Maribel Lucerón Lucas-Torres, Sergio Núñez de Arenas-Arroyo and Alicia Saz-Lara in Women's Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.