
Abstract
Background:
Women’s knowledge of the nutritional guidelines during pregnancy can affect the health and nutritional status of both mother and child. Having good nutritional information related to maternal dietary intake and healthy lifestyles is therefore of great importance. However, there is limited published research that demonstrates pregnant women’s knowledge of the nutritional guidelines during pregnancy in Lebanon.
Objective:
To assess the knowledge on food sources and energy recommendations as well as food safety practices and diet–health relationship among women during pregnancy in Lebanon.
Design:
A cross-sectional study.
Methods:
The study was conducted at prenatal care clinics in Lebanon, and all pregnant women present, regardless of nationality, were invited to complete the self-administered nutrition knowledge questionnaire. The study assessed five different nutrition knowledge domains (food sources of nutrients, dietary behaviors, food safety knowledge, micronutrients for fetal development, and energy requirements and weight gain) and the demographic characteristics of pregnant women who completed a multidimensional online survey based on validated and existing measures.
Results:
Four-hundred and ten responses were obtained. Approximately half of respondents (47%) held a university degree, for 42% of women this was their first pregnancy, and 71% had a planned pregnancy. Among the different nutrition knowledge domains, the highest levels of knowledge were for the behaviors that can minimize the effect of nausea/vomiting, heartburn, and constipation during pregnancy (63.9%) and the lowest levels of knowledge was for the importance of iodine and omega-3 fatty acids in pregnancy (28.4%). Most of females knew about food safety practices during pregnancy (72.9%) but less than half were knowledgeable about listeriosis contamination (45.9%), and the types of fish that are the safest to select during pregnancy (47.8%).
Conclusion:
Despite the fact that pregnant women had an adequate level of knowledge in different nutrition-related areas, there was inadequate level of awareness related to critical nutrients and behaviors that can have adverse effects on mother and/or baby. Therefore, there is a need to focus on specific maternal nutrition aspects such as iron-rich foods, listeriosis food contamination, and nutrients that aid in fetal brain and retina development.
Plain Language Summary
Women who adopt healthy dietary patterns during pregnancy are more likely to prevent adverse birth outcomes. Pregnant women from the Middle East have limited knowledge of the dietary guidelines for healthy eating during pregnancy. Yet there are no studies on nutritional knowledge of pregnant women residing in the Middle East. This study aimed to investigate the nutrition knowledge of pregnant women in Lebanon, which includes food sources of nutrients, diet–health relationships, food safety, and energy requirements during pregnancy. The highest levels of nutrition knowledge were for the behaviors that can reduce the effect of nausea and vomiting, heartburn, and constipation during pregnancy and the lowest levels of knowledge were for the importance of iodine and omega-3 fatty acids in pregnancy. The level of awareness related to critical nutrients and behaviors that can have adverse effects on mother and/or baby is inadequate. Lebanese women need to obtain their information from reliable sources such as their healthcare providers. Collaboration between healthcare providers and dietitians is essential to ensure that pregnant women receive comprehensive and accurate nutritional advice throughout their pregnancy journey.
Introduction
Proper maternal nutrition can prevent adverse birth outcomes, 1 which include miscarriage, birth defect, preterm delivery, low birth weight, and macrosomia. 2 It is widely known that healthy dietary patterns during pregnancy are associated with higher birth weight, whereas “unhealthy” dietary patterns are associated with a higher risk of shorter length of gestation and thus a lower birth weight, 3 whereas maternal diets high in sugar and fat with a higher rate of cardiovascular disease, diabetes, and metabolic syndrome later in life. 4
Despite the fact that a diet adequate in macro- and micronutrients during pregnancy is important for the health status of the mother and child, many pregnant women find it difficult to design a proper diet. 5 Moreover, the diet quality of pregnant women is reported to be poorer in those who are less educated, younger, overweight or obese before pregnancy which highlights the need for an improvement in their diet quality. 6 It is also reported that the diet of pregnant women lacks the recommended energy and carbohydrate and essential micronutrients (iron, calcium, magnesium, folic acid, and vitamin D) intakes, which are essential for the normal development of the fetus. 7 The knowledge of the dietary guidelines for healthy eating during pregnancy is also limited among pregnant women.8,9 However, pregnant women perceive their diets to be healthy, even though they do not meet the dietary recommendations. 10
Many of the existing studies conducted in the Middle East have examined the knowledge and practices of pregnant women regarding a single nutrient (most commonly folic acid) supplementation required during pregnancy.11,12 Other studies investigated the nutritional beliefs of pregnant women, 13 their knowledge in safety issues amid the COVID-19 pandemic, 14 and their micronutrient deficiencies and inadequacies. 15 There have also been studies in the Middle East which investigated the knowledge and awareness of pregnant women about the effect of obesity on maternal and fetal health,16,17 but there are no studies on nutritional knowledge of pregnant women residing in the Middle East. Therefore, the purpose of this study was to investigate the nutrition knowledge of pregnant women in Lebanon, which includes food sources of nutrients, diet–health relationship, food safety, and energy requirements during pregnancy.
Methods
Materials and methods
Study population
This cross-sectional study encompassed pregnant women seeking prenatal care in Lebanon, irrespective of nationality, encompassing Lebanese citizens, Syrian refugees, and Palestinian refugees. The survey was designed for online self-completion, ensuring participant anonymity. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental material).
Questionnaire
The questionnaire employed in this study was developed by researchers, drawing upon previous literature18 –22 and pertinent nutritional aspects of pregnancy. A pilot study involving 30 individuals was conducted to assess questionnaire reliability, leading to necessary modifications for context suitability. Reliability was assessed using alpha-Cronbach’s coefficients.
The questionnaire used to assess pregnant women’s nutrition knowledge was based on an existing survey that explored Australian women’s level of nutrition knowledge during pregnancy. 23 The questionnaire was then reviewed by public health nutritionist, practising dietitian, nutrition instructor, and epidemiologist to ensure the questionnaire reflects the national guidelines for a healthy pregnancy and consisted of multiple sections:
Food Sources of Nutrients: This section evaluated knowledge regarding sources of essential nutrients such as foods rich in vitamin A, iron, iodine, and omega-3 fatty acids.
Dietary Behaviors: It assessed awareness of dietary behaviors to alleviate common pregnancy symptoms such as nausea, vomiting, heartburn, and constipation. An example of a question in this domain is “Do the following behaviours help in minimizing the effect of heartburn during pregnancy?”
Food Safety Knowledge: This section covered topics such as food storage, refrigerator temperature, listeria contamination, and personal hygiene such as a. “It is safe to use same cutting board for raw chicken and raw vegetables if wiped off between uses.” b. “Raw meat and chicken should be stored on open shelves above cooked food in the refrigerator.”
Micronutrients for Fetal Development: It assessed knowledge regarding micronutrients crucial for fetal brain and retina development by asking the following two questions: a. “Which nutrient can help with a baby’s eyes, brain and nerves development during pregnancy?” b. “Which nutrient is particularly important for the healthy development of an unborn baby’s brain?”
Energy Requirements and Weight Gain: This section evaluated knowledge of energy requirements and weight gain recommendations during pregnancy, including changes across trimesters and the necessity of increased food quantity. Examples of questions in this domain include: a. “Do you think women’s energy requirements (calories/day) change during pregnancy?” b. “Which behaviors help in preventing too much weight gain during pregnancy?”
The questionnaire comprised 36 multiple-choice questions with one correct response. The answer options to the questions included “true, false, don’t know”; “yes, no, not sure”; or a choice of different food options and “not sure.” The correct responses were scored as 1, whereas the incorrect, not sure, and don’t know responses were scored as 0, resulting in a total score of 36 for the five domains. The total points that can be scored on each domain are found in Table 2.
Demographic information was obtained through the self-administered questionnaire and included age, stage of pregnancy, planned pregnancy, marital status, prior pregnancies, education, household income, nationality, and seen by dietitian.
Recruitment took place between October 2020 and April 2021. All pregnant women, who were waiting in the antenatal clinic waiting rooms, were invited to complete the survey independently. Women were told verbally about the purpose of the survey and were aware that their participation was voluntary. Women, who agreed to participate, were provided a hard copy to complete the survey at the time or given the link to complete the survey online at a later time. The hard copies of the surveys were then collected by researchers and entered online.
Statistical analysis
Data analysis was conducted using the Statistical Package for the Social Sciences software (IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA)). Descriptive and inferential statistics were applied to describe and analyze the data. The study was examining the nutrition knowledge of pregnant women on five different domains and how the demographic variables relate to the knowledge score. One-way analysis of variance (ANOVA) and independent t-tests (p < 0.05) were utilized to assess variations in mean total nutrition knowledge scores across demographic categories of women living in Lebanon. Five linear regression models were employed to examine the effects of independent variables on knowledge (model 1), diet–health relationship (model 2), food safety (model 3), knowledge of micronutrients (model 4), and caloric needs and weight gain recommendations. Only factors significantly associated with nutrition knowledge (p < 0.05) in one-way ANOVA and independent t-tests were included in the regression analysis.
To ensure adequate statistical power, a minimum sample size of 377 respondents was determined through statistical calculations. This calculation considered a total population of 20,000, a margin of error of 5%, and a confidence level of 95%.
Ethical approval
Written informed consent was obtained from all participants. This study adhered to the guidelines and regulations outlined in the Declaration of Helsinki, and it received approval from the Institutional Review Board of the Lebanese International University (LIUIRB-200706-JR1).
Furthermore, ethical approval was granted by the Institutional Review Board of the researcher’s university, the Lebanese International University. Participation was voluntary, and informed consent was obtained from all participants.
Results
Demographic characteristics
The demographic characteristics of the respondents are shown in Table 1. This study encompassed n = 410 pregnant women. Around 40% of respondents were in their second trimester. Approximately half of respondents (47%) held a university degree and 42% of them were in their first pregnancy. Finally, more than half of them (56.9%) had not seen a dietitian and the majority of them (71%) had a planned pregnancy.
Demographic characteristics of the study participants.

Nutrition knowledge
Table 2 provides a summary of the mean score obtained by respondents after assessing their nutrition knowledge. The greatest levels of knowledge were for the domains “diet–health relationship” (63.9%) and “energy requirement and recommended weight gain during pregnancy” (67.1%). Approximately half of the respondents had an average level of knowledge for “food safety practices in pregnancy” (56.7%) and “food sources of nutrients” (54.3%), and the lowest levels of knowledge were for the section “significance of essential nutrients in pregnancy” (28.4%).
Percentage of participants who gave correct answers to nutrition knowledge questions.

Food sources of nutrients
The majority of women were able to recognize food sources rich in omega-3 fatty acids (81.6%), iodine (70.3%), and dietary fiber (69.3%). Approximately, half of the respondents did not recognize that fat has the highest calories compared to sugar and alcohol (51.4%). The majority of women (63.3%) did not identify liver as a high source of vitamin A. When questioned to classify food sources high in iron, only 20.8% of the pregnant women correctly classified red meat, among a list including spinach and eggs.
Diet–health relationship
In this section, the respondents’ understanding of behaviors that can reduce the effect of nausea and vomiting, heartburn, and constipation during pregnancy was assessed. Most of the respondents knew that “eating less fatty and spicy foods” (68.4%), “avoiding large snacks every few hours” (79.7%), and “eating smaller meals more often” (89.6%) would aid in reducing the effect of nausea and vomiting during pregnancy. On the other hand, less than half of the respondents (42.3%) correctly identified that consuming sweet biscuits in the morning can assist in dealing with nausea/vomiting pregnancy discomfort.
Most respondents correctly identified that consuming “small frequent meals and nutritious snacks” (77.1%) and “less fatty and spiced foods” (80.7%) would aid in reducing the effect of heartburn during pregnancy. However, only half of the respondents (53.6%) were knowledgeable that “remaining away from lying down shortly after eating” would help in managing heartburn and only 20% of them properly recognized that consuming less sugar would aid in dealing with heartburn discomfort.
A large proportion of participants was knowledgeable of the possibility of resolving constipation during pregnancy by “eating more legumes” (63.3%), by “exercising regularly” (81.9%), and by “eating more fruits and vegetables” (86.2%). On the other hand, only 24.9% of the participants correctly recognized that consuming fewer spicy and salty foods would not help in solving constipation discomfort.
Significance of essential nutrients in pregnancy
In this section, the respondents’ knowledge of the role of nutrients in the body and the possibility of nutrient deficiency were assessed. Only 25.8% identified iodine as the nutrient essential for healthy growth of a fetus’s brain and 30.9% identified omega-3 as the nutrient that can aid with the development of a baby’s eyes, brain, and nerves during pregnancy.
Food safety practice in pregnancy
Women’s awareness of food safety issues was assessed in this section. The majority of participants were knowledgeable that washing hands before food preparation reduces the chances of food poisoning (72.9%), that it is unsafe to utilize the same surface for cutting uncooked meat and vegetables (81.2%), that uncooked meat and chicken should not be kept on open shelves above cooked food (60.6%), and that the temperature of the refrigerator should remain between 0°C and 4°C (61.1%). However, only 50% of the participants were knowledgeable that refrigerated foods should remain below 4°C (50%) and that listeriosis is an illness spread by contaminated food (45.9%). A small proportion of respondents (27.8%) were aware that it is harmless to consume cooked refrigerated food without reheating it. When respondents were given a list of foods to select that is appropriate for pregnant women to consume, 63% answered correctly and about approximately (47.8%) correctly identified the safest choice of fish to select.
Caloric needs and weight gain recommendations during pregnancy
This section explored respondents’ knowledge of caloric needs and weight gain recommendations during pregnancy. Most respondents correctly identified that consuming “less saturated fat” (75.4%), “more fruits and vegetables” (74.6%), and not “eating less dietary fiber” (61.1%) would aid in avoiding excessive weight gain during pregnancy. However, most respondents were not aware that participating in at least 30 min of exercise every day would help inhibit excessive weight gain during pregnancy (73.2%). Most of the respondents clearly classified that women’s caloric needs (calories/day) differ during pregnancy (78.3%), that the energy requirements vary based on the trimester of pregnancy (76.1%), and that it is not needed “to eat for two” during pregnancy (77.5%).
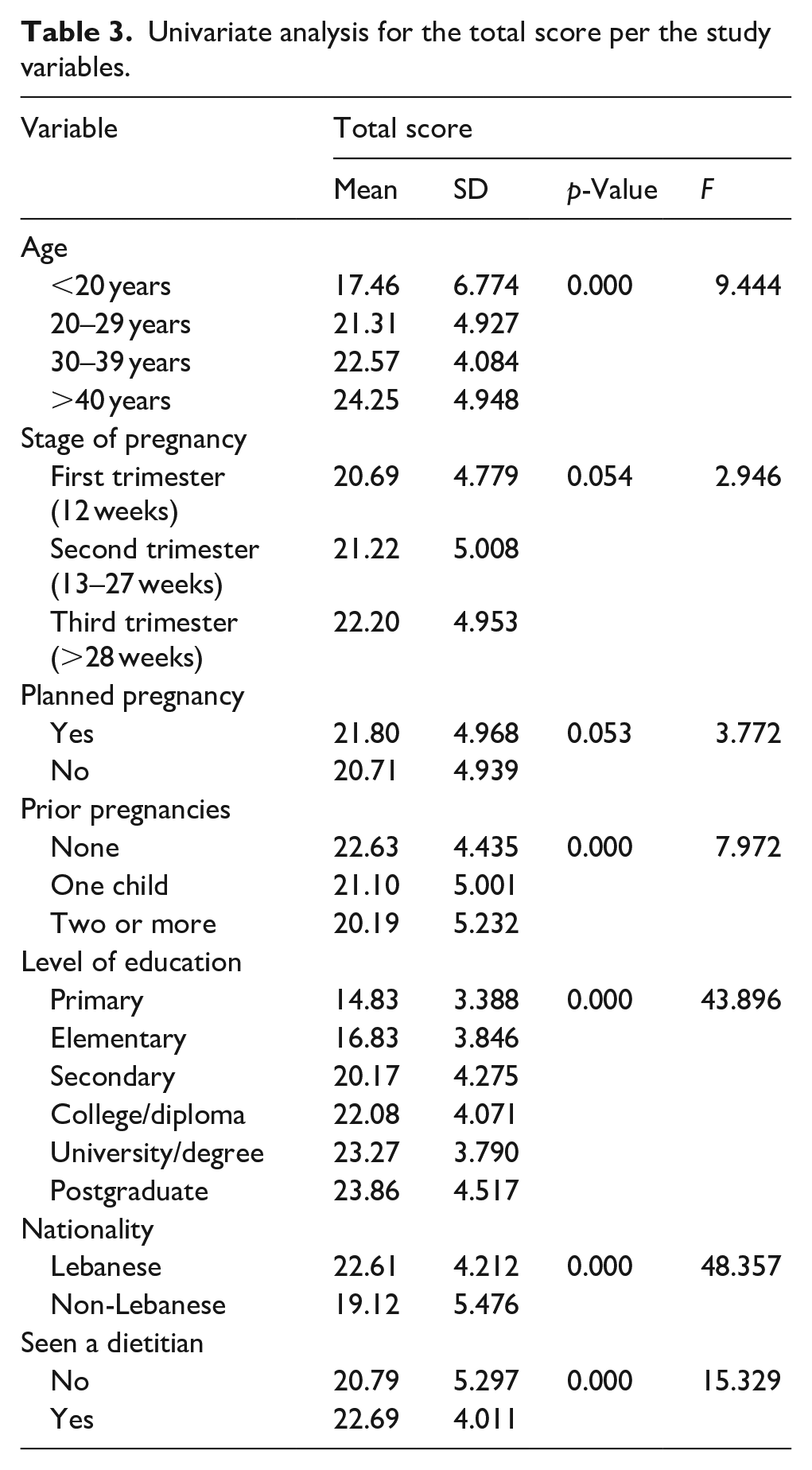
Table 3 displays the univariate analysis for the total score per the study variables. The mean of the total score was 21.47 out of the possible 36. There was a strong, positive correlation between total score and age, with the highest score achieved by older women. Women who scored highest in the overall score had a higher level of education. There was a strong, negative correlation between total score and prior pregnancies, with a lower score achieved by women who had two or more pregnancies compared to women with no previous pregnancies. There was a significant difference between total score and nationalities with a higher score achieved by Lebanese women compared to non-Lebanese women. Moreover, women who had seen a dietitian had a significantly higher total score than women who had not.
Univariate analysis for the total score per the study variables.
Multiple regression analysis of factors influencing nutrition knowledge in pregnancy
Table 4 displays the results of the multiple regression analysis. The independent variables that exhibited significant associations with higher nutrition knowledge scores were education and nationality. Individuals with the highest level of education and those of Lebanese nationality demonstrated a positive correlation with enhanced nutrition knowledge. However, no statistically significant differences were noted for the remaining independent variables, including age, prior pregnancies, household income, and whether respondents had consulted with a dietitian.
Linear regression results with nutrition knowledge score as dependent variable.
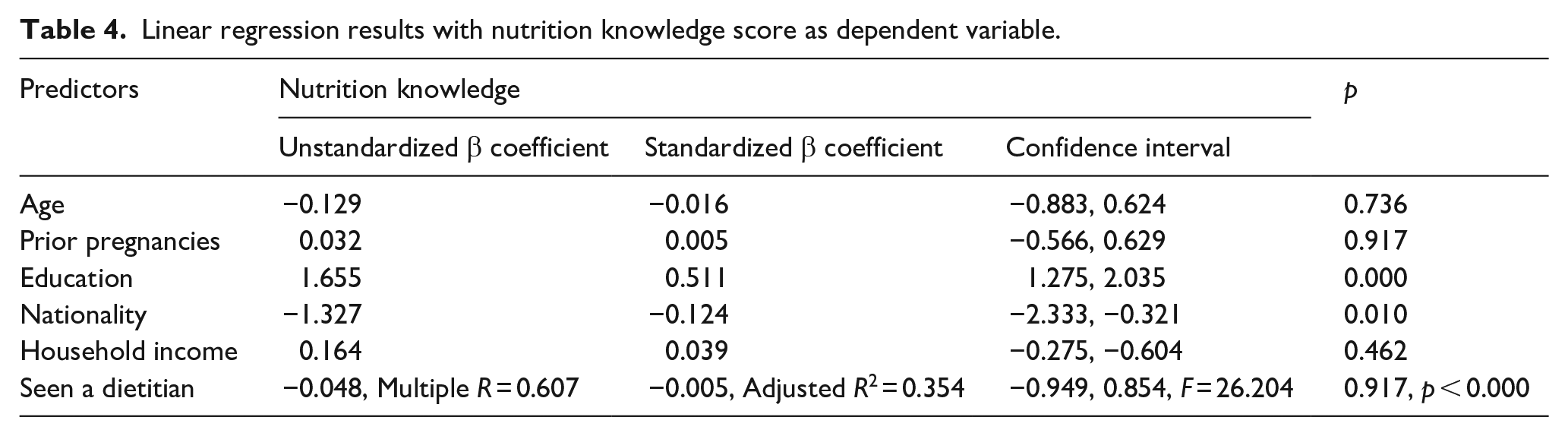
The overall model explained a noteworthy 35% of the variance in respondents’ nutrition knowledge scores, as indicated by the adjusted R2 value. This suggests that education and nationality, among the considered factors, play a substantial role in influencing the level of nutrition knowledge among respondents during pregnancy.
Discussion
This study explored five areas related to the nutrition knowledge of pregnant women in Lebanon, namely food sources of nutrients, diet–health relationships, essential nutrients in pregnancy, food safety practices, and energy and gestational weight gain (GWG) recommendations. The food sources of nutrients area were able to identify whether women are able to identify food items rich in iron, omega-3, iodine, vitamin A that are important for the growth and development of the fetus. Diet–health relationships domain explored women’s knowledge of behaviors that help manage common pregnancy-related symptoms (nausea, vomiting, heartburn, and constipation) that affect over 50% of women and often dietary and lifestyle changes are sufficient in managing those symptoms. 24 The essential nutrients domain was assessing the importance of key nutrients (iodine and omega-3 fatty acids) in pregnancy and what fetal organs they are particularly essential for. The food safety practices domain was exploring women’s knowledge of avoiding certain foods that are high risk for transmitting food-borne infections and safe preparing and handling of foods since pregnant women are more susceptible to foodborne illnesses. The last domain was evaluating pregnant women’s knowledge of energy requirements and weight gain recommendations to identify what pregnant women actually know since energy and weight gain recommendations exist but little is known of women’s knowledge of these recommendations.
Most of the women in this study were capable of recognizing the food sources rich in omega-3 fatty acids, iodine, and fiber, but they were mistakenly choosing spinach as a high-iron source compared to red meat. The results of this study also showed a shortage of knowledge among pregnant women regarding the importance of key nutrients for fetal development. Finally, most of the women were knowledgeable about the energy requirements and the recommendations to prevent excessive weight gain during pregnancy, especially those who were counseled by a dietitian.
Similar to the findings of our study other cross-sectional studies conducted in Australia, Prague, and Pilsen also showed limited nutrition knowledge of pregnant women in some areas of nutrition.8,25 A possible explanation could be that pregnant women receive limited nutrition advice, especially from clinicians according to a mixed methods study design in Australia 26 and they are also not referred to dietitians. However, when nutritional counseling is provided in the prenatal care setting as was investigated in a quasi-experimental study among 27 pregnant women, participants’ nutrition knowledge and awareness improve 27 and their nutrition knowledge scores significantly increase after receiving nutrition education according to a cross-sectional study that sampled 743 pregnant women in Istanbul. 28
In a study that examined the nutrition knowledge of 252 pregnant women and their consumption of iron-rich foods, only 16.3% of the respondents were able to identify foods that help the body to absorb and use iron. 29 In another review article that evaluated the current recommendations for the intake of the most common micronutrients and omega-3 fatty acids during pregnancy and lactation in the United States, Canada, and Europe, many pregnant women were advised by health experts to avoid certain types of fish and seafood, which are rich in omega-3 fatty acids and iodine, respectively, because of concerns about contamination with parasites, germs, toxins, and mercury. 30 Therefore, healthcare providers need to ensure that pregnant women obtain 200–300 mg of omega-3 fatty acids as they play a role in the cognitive and visual development of the fetus. 31
Minor discomforts of pregnancy are viewed by pregnant women and healthcare providers as a normal occurrence in a healthy pregnancy, yet the challenge is in finding the best strategies to manage these discomforts. 32 Among the dietary guidelines that were developed to help clinicians share when counseling women on the management of nausea and vomiting include avoiding large meals and fatty food, avoiding strong tasting foods, having small frequent meals, and eating simple dry carbohydrates, such as, crackers and biscuits, prior to getting out of bed in the morning. 33 In our study, the knowledge of pregnant women regarding diet and lifestyle in relieving the minor discomforts of heartburn, constipation, and nausea and vomiting was high.
According to the WHO, iodine deficiency is the most frequent avoidable cause of brain damage 34 and severe iodine deficiency leads to major adverse health effects in pregnant women and their offspring. 35 In our study, most of the women were not capable of recognizing iodine as the nutrient essential for healthy development of a fetus’s brain. Similar to our study, a cross-sectional study that was conducted on 804 pregnant women in Norway found that 74% of pregnant women had none to low iodine knowledge scores and only 16% of pregnant women properly classified iodine as vital for normal child growth and development. 36 Because a shortage of knowledge about iodine may be a possible factor for iodine deficiency in pregnant women, 36 being aware of iodine significance during pregnancy may result in adequate iodine status. 37
During pregnancy omega-3 polyunsaturated fatty acids (n-3 PUFAs), particularly docosahexaenoic acid (DHA), are vital for appropriate neural, visual, and cognitive growth of the fetus. 38 A main obstacle to adequate n-3 PUFA intake among pregnant women may be their unfamiliarity with the “right” foods. 39 In our study, only 30.9% of pregnant women were able to identify that n-3 PUFA is the nutrient that can aid with a baby’s eyes, brain, and nervous development. Similar to the findings of our study, Sinikovic et al. aimed to assess the knowledge of 190 women regarding the importance of n-3 PUFAs during pregnancy and found that women’s awareness of n-3 PUFA requirements was limited, which could be because healthcare services did not provide pregnant women with sufficient material on the significance of ingesting foods high in n-3 PUFA during pregnancy. 38
Food safety practices are important to prevent food-borne illnesses, particularly during pregnancy since they could lead to adverse effects such as stillbirth and fetal blindness. 40 Our findings are similar to the findings of Jevšnik et al., who explored the food safety knowledge and practices of 145 pregnant women and 90 postpartum mothers in Slovenia using an online questionnaire and showed that women have basic knowledge of proper food handling but had some specific gaps concerning microbiological risks, particularly regarding Listeria. 41 One explanation could be that pregnant women rely on media as a source of food safety information, whereas the credible resource should be trained health professionals in prenatal parenting classes or gynecology clinics. 41
Pregnant women who are aware of healthy eating behaviors, such as being able to identify food groups that help prevent too much weight gain and changes in energy requirements during pregnancy, are able to manage GWG. 42 In our study, pregnant women’s knowledge assessment of those eating behaviors revealed a high degree of knowledge of foods that consumption has to be adjusted to avoid excessive GWG and of the changes in energy requirements during the trimesters of pregnancy. Similar to the findings of our study, a formative research that was conducted and included semi-structured individual interviews and focus group interviews among pregnant women in Pennsylvania showed that 42% pregnant women had no knowledge of how much GWG they should gain. 42 Moreover, the women who had some knowledge of the GWG and healthy eating guidelines were receiving this information from a non-healthcare provider resource. 42
There are some limitations of our study. First, its cross-sectional design was able to provide valuable information about the current status of nutrition knowledge among pregnant women in Lebanon, but was not able to capture changes over time or establish reliable relationships between variables. This makes the generalization of results hindered and the results should be interpreted with caution. Moreover, there might be other variables that could have played a role in influencing nutrition knowledge during pregnancy such as, access to healthcare services and cultural beliefs but they were not measured in our questionnaire. The questionnaire used in the study was not validated but was somehow controlled because an internal validity was performed and the questionnaire was based on an existing survey that was validated. Women who participated in filling out the survey might have been more interested and thus more knowledgeable about nutrition than women who chose not to participate. The study relied on self-administered and self-reported questionnaire; thus, the findings could be influenced by response bias.
Conclusion
This study revealed a generally good level of nutrition knowledge among pregnant women; yet significant gaps exist in critical areas of maternal nutrition. The primary source of health information for pregnant women should be their prenatal healthcare providers. These professionals play a vital role in imparting general nutrition information and should proactively refer expectant mothers to registered dietitians for tailored dietary guidance. Collaboration between healthcare providers and dietitians is essential to ensure that pregnant women receive comprehensive and accurate nutritional advice throughout their pregnancy journey.
Furthermore, the development of targeted nutrition education programs by community dietitians, specifically aimed at women of childbearing age, holds immense potential. These programs can effectively raise nutrition awareness, enhance knowledge, and contribute to improved health outcomes for both mothers and newborns.
In conclusion, addressing the gaps in maternal nutrition knowledge is a critical step toward promoting healthier pregnancies and better long-term health for both mothers and their offspring. It requires a concerted effort from healthcare providers, dietitians, and community initiatives to empower pregnant women with the knowledge they need to make informed and nutritious choices for themselves and their babies.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241272216 – Supplemental material for Nutrition knowledge among pregnant women in Lebanon: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057241272216 for Nutrition knowledge among pregnant women in Lebanon: A cross-sectional study by Jessy Rizk, Eleni Andreou, Dona Hileti, Ali Ghaddar and Antonis Zampelas in Women’s Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057241272216 – Supplemental material for Nutrition knowledge among pregnant women in Lebanon: A cross-sectional study
Supplemental material, sj-pdf-2-whe-10.1177_17455057241272216 for Nutrition knowledge among pregnant women in Lebanon: A cross-sectional study by Jessy Rizk, Eleni Andreou, Dona Hileti, Ali Ghaddar and Antonis Zampelas in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.