
Abstract
Background:
Many adults in the United States do not reach the recommended levels of activity needed for health benefits. Single-female caregivers present a unique and vulnerable population that is often less active than their partnered peers or single-male caregivers.
Objective:
The primary objective of this cross-sectional investigation was to identify the prevalence of physical inactivity in single-family, female-led households and determine differences in personal factors and social characteristics between physically active and not physically active single-female caregivers. A secondary objective was to examine associations among the social characteristic variables and physical inactivity in single-female caregiver households. Finally, we examined the odds single-female caregivers who are physically inactive reported chronic health conditions.
Design:
Cross-sectional survey design.
Methods:
We used the 2020 Behavioral Risk Factor Surveillance System (BRFSS) data. Participants were selected based on pre-determined criteria for inclusion.
Results:
There was a 39.3% prevalence of physical inactivity among single-female caregivers in the sample. Single-female caregivers who were physically inactive had greater odds of having a history of multiple chronic health conditions.
Conclusion:
Healthcare providers and other community stakeholders should explore existing physical activity promotion strategies to increase physical activity in single-female caregivers. Future research should employ more rigorous, prospective research designs to determine if these chronic conditions and various social characteristics are caused by physical inactivity.
Introduction
The current physical activity (PA) guidelines in the United States recommend adults include a minimum of 150 minutes of moderate-intensity aerobic activity or a minimum of 75 minutes of vigorous-intensity aerobic activity and 2-days per week of muscle-strengthening activities to reduce the risk of negative health outcomes and chronic disease development. 1 PA is also associated with life satisfaction and happiness. 2 Even though there are known benefits to PA, the U.S. Department of Health and Human Services estimates that almost 80% of adults in the United States do not meet both the aerobic and strength training recommendations, and 50% do not meet the aerobic guidelines. 1 Intrapersonal barriers negatively associated with PA included lack of time, negative emotions, and decreased health, while increased motivation, enjoyment with activity, and positive beliefs about being active were positively associated. 3 Social support and support from family members and friends were also positively associated with PA, 3 along with demographic variables such as male gender, white ethnicity, education, and income. 4
Given the barriers and facilitators discussed above and the known barriers for single-female caregivers such as lack of support, family responsibilities, not enough time, and childcare responsibilities, 5 it should be of no surprise that single-female caregivers are physically inactive. Single mothers are more likely to be physically inactive than their peers, self-reporting less PA, and objectively participating in less moderate-vigorous PA compared to non-mothers and married mothers. 6 This inactivity may be causing serious long-term health outcomes. A review of the National Health and Nutrition Examination Survey (NHANES) data identified an increased odds of poorer cardiovascular health compared to partnered mothers. 7 Additional analysis of NHANES data (1988–1994) identified single mothers were more likely to have diabetes and cardiovascular disease such as hypertension and hyperlipidemia. 8 It has been estimated that there are approximately 15 million single-female caregiver households in the United States, 9 resulting in a large number of women at risk for physical inactivity and the negative health outcomes associated with inactivity. It is important to understand the incidence of physical inactivity and to determine whether PA participation is associated with reduced risk for chronic health diseases.
It is important to explore physical inactivity rates for single-female caregivers by personal and social characteristics that are often related to physical inactivity such as race, income, and education. Non-Hispanic Black, Asian, and Hispanic adults are less likely to meet the recommended PA guidelines compared to White adults. 10 Adults in the United States that had higher income and higher education levels were more likely to be physical active. 11 Identifying subpopulations of single-female caregivers who are at the greatest risk of physical inactivity is essential for developing specific intervention strategies to increase PA. In order to explore effective intervention strategies, or develop and champion health promotion and PA promotion strategies among single-female caregivers, additional analysis are needed.
The primary purpose of this cross-sectional investigation was to identify the prevalence of physical inactivity for single-female caregivers who participated in the 2020 Behavioral Risk Factor Surveillance System (BRFSS). The association between various personal factors and social characteristics and physical inactivity were also explored. It was hypothesized there would be an association between personal factors and social characteristics and physical inactivity in a sample of single-female caregivers. A secondary purpose was to examine the odds those who were physically inactive reported chronic conditions compared to those who were considered activity. It is hypothesized single-female caregivers who were inactive would have higher odds of reporting various chronic conditions that were assessed in the BRFSS database.
Methods
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement was utilized in the reporting of this cross-sectional analysis.
Data source
Data from the 2020 BRFSS was used for this study. The BRFSS is a health-related survey that is administered via telephone each year in the United States across all 50 states, the District of Columbia, and three territories. 12 The BRFSS collects over 400,000 adult responses each year in the United States. 12 The BRFSS database includes a set of “core questions” that are asked to all adult participants with topics that range from health status, health care access, exercise, chronic health conditions, tobacco use, alcohol use, etc. 13 There are also optional modules and questions that are administered on a state-by-state basis. 13 All variables selected for inclusion in this analysis are a part of the core questions asked of all participants. All surveys were administered in 2020.
Participant selection
We included females who lived alone (single-female) and reported having children (caregivers) who participated in the 2020 BRFSS. 14 The participants were selected from the 2020 BRFSS 14 if they reported female for the sex variable and responded only one adult living in the household. Next, only participants who responded that 1 or more children lived in the household were included when asked the question, “How many children less than 18 years of age lived in your household?.” Appendix 1 includes all 2020 BRFSS variables used to select participants.
Participants were excluded if they indicated they were of male sex or were females who did not report living alone and did not report having children under the age of 18. The University of Kentucky Institutional Review Board (IRB) determined that the analysis did not require IRB review as it involved using publicly available data from the Centers for Disease Control.
Variables of interest
Dependent variable
The dependent variable of interest was whether or not the single mother was physically active. The variable was a dichotomous response (yes/no) for adults who reported doing PA or exercise during the past 30 days outside of their job duties. This is a calculated variable from the question “During the past month, other than your regular job, did you participate in any physical activities or exercise such as running, calisthenics, golf, gardening, or walking for exercise?” For the purposes of this analysis, participants who responded no were categorized as physically inactivity and participants who responded yes were categorized as physically active.
Independent variables
Personal factors and social characteristic variables
The personal factors and social characteristic variables that were summarized and explored across groups and as potential associations with physical inactivity included race and ethnicity, level of education completed, income, urban/rural status of the respondents, their overall health, insurance status, and whether or not the participant has a personal doctor. Additional variables also explored included age, body mass index, and number of children. These variables were selected to represent social determinants of health that are known to influence PA participation and/or have a relationship with health outcomes.
Health-related variables
Additional analyses were performed to determine the relationship between chronic health conditions assessed in the 2020 BRFSS 14 and physical inactivity. The following variables to represent chronic health conditions were included: whether or not participants have ever reported having coronary artery disease or myocardial infarction, whether or not they have been told they asthma, whether or not they had diabetes, have had kidney disease, history of cancer (non-skin), and history of stroke. A variable associated with mental health, which categorized the number of good mental health days into three categories, was also included. Appendix 2 includes all 2020 BRFSS 14 dependent and independent variables, their associated questions, and labels. These variables were selected based on the review of the 2020 BRFSS database, which captured the chronic health conditions of all participants.
Statistical analysis
All variables were summarized as counts for each variable, for those single-female caregivers who participated in PA outside of their job-related duties and for those single-female caregivers who do not participate in PA outside of their job-related duties. Those participants with missing data specific to the exercise variable were excluded. Those participants who responded “did not know” for any of the variables were removed from all analyses. To determine the prevalence of physical inactivity for single-female caregivers, the number of single-female caregivers who were physically inactive was divided by the total number of single-female caregivers in the sample. Contingency tables were created to calculate the total number of participants in each category (physically active versus physically inactive) associated with the variables of interest. Chi-square tests of independence were performed to determine if an association exists between the dependent variables and physical inactivity. Odd ratios and associated 95% confidence intervals (95% CI) were calculated to determine the association between the health-related variables and physical inactivity. All statistical analyses were performed in R Studio version 2022.07.01. All statistical analyses were significant at the p < 0.05 level.
Results
There were a total of 1,922 single-female caregivers in the dataset. After participants were removed due to missing data, a total of 1,541 single-female caregivers who responded to whether or not they participated in PA in the last 30 days outside of their job duties and had data for all of the demographic and personal characteristic variables were included in the analyses. There was a 39.3% (n = 435) prevalence of physical inactivity among this sample. Summaries (count and frequencies) for the personal characteristics and demographic variables for both groups for the entire sample of single-female caregivers in the 2020 BRFSS can be found in Table 1. Summaries (count and frequencies) for the health-related variables for both groups for the entire sample of single-female caregivers in 2020 can be found in Table 2.
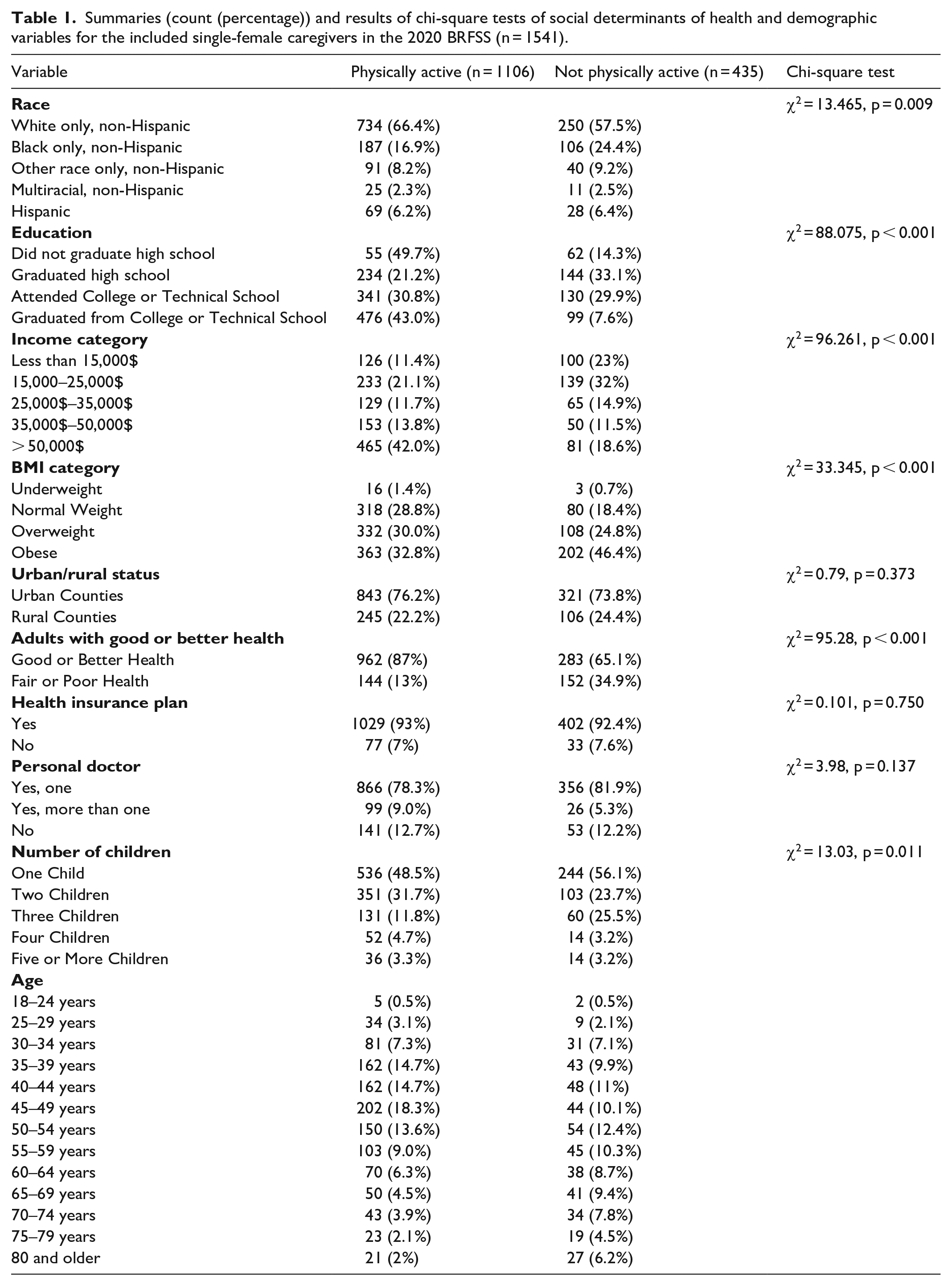
Summaries (count (percentage)) and results of chi-square tests of social determinants of health and demographic variables for the included single-female caregivers in the 2020 BRFSS (n = 1541).
Summaries (count) of health-related variables for the included single-female caregivers in the 2020 BRFSS.

There was no significant association between urban/rural status, whether or not the women had a health insurance plan or whether or not the women had a personal doctor (Table 1) with activity status. There was a significant association between race with a higher percentage of White single-female caregivers who were physically active and a higher percentage of Black single-female caregivers who were physically inactive (Table 1). Single-female caregivers who were physically active were significantly more likely to have post-high school education while those who were not physically active were more likely to have at most a high school diploma (Table 1). Similarly, over 40% of single-female caregivers who are physically active reported being in the highest income bracket while almost 25% of those who were physically inactive reported incomes of less than $15,000 (Table 1). There was a significant association between BMI category and PA group, with 46% of single-female caregivers who were physically inactive categorized as obese while more that were physically active were in the normal weight and overweight category (Table 1). PA status and overall health were significantly associated, with 87% of single-female caregivers who were physically active describing themselves as in good or better health as compared to only 65% of those who were physically inactive. (Table 1). Finally, there was a significant association between number of children and PA status. A higher percentage of single-female caregivers in the physically inactive group reported having only one child (Table 1).
Single-female caregivers who were physically inactive had 3.11 greater odds (95% CI (2.06–4.70)) of reporting a history of coronary artery disease or myocardial infarction, 0.94 odds (95% CI (0.71–1.26)) of reporting having asthma and 2.62 greater odds (95% CI (1.42–4.85)) of having been told they had a kidney disease compared to those that were physically active (Table 2). Finally, physically inactive single-female caregivers had 1.78 greater odds (95% CI (1.2–2.63)) of disclosing a history of cancer other than skin cancer and 3.16 greater odds (95% CI (1.89–5.30)) of reporting a history of stroke compared to those that were physically active (Table 2).
Discussion
The primary purpose of this cross-sectional study was to identify the prevalence of physical inactivity in single-female caregivers who participated in the 2020 BRFSS. Secondary purposes were to examine differences in demographic variables and social characteristic variables between physically active and physically inactive single-female caregivers, to explore the relationship among the social characteristic variables and physical inactivity in this population, and to determine the odds single-female caregivers who were physically inactive reported chronic conditions assessed in the 2020 BRFSS database.
The U.S. Department of Health and Human Services summarized the benefits of PA for adults to include: lower risk of all-cause mortality, lower risk of cardiovascular disease mortality, weight loss, lower risk for additional chronic diseases such as diabetes, cancer, and hypertension, improved sleep, improved bone health, and decreased risk for falls. 1 The results of this analysis indicated the prevalence of physical inactivity in single-female caregivers who participated in the 2020 BRFSS was 39.3%. The additional analyses revealed there were significant relationships between multiple social characteristic variables and physical inactivity. The results of these analyses revealed that women who were highly educated, who had higher incomes, and who reported better overall health were more likely to be physically active.
While the prevalence of physical inactivity is of concern in this population, of even more concern is the relationship between physical inactivity and chronic diseases among these women. Single-female caregivers who were physically inactive had greater odds of reporting having had coronary artery disease or myocardial infarction, kidney disease, cancer other than skin cancer, and a history of stroke compared to the single-female caregivers who were physically active. These results are similar to that of a recent systematic review that summarized PA and cardiovascular disease in middle-aged and elderly women. 15 The authors reported decreased relative risks of cardiovascular disease (0.74, 95% CI (0.67-0.80),) decreased risk for stroke (0.77, 95% CI (0.70-0.85)) and decreased risk for all-cause mortality (0.70, 95% CI (0.65-0.78)) for those that were physically active. 15 Given the high rates of chronic diseases and low rates of PA among single-female caregivers, there is a desperate need to improve PA participation for single-female caregivers. Two factors included in the analyses to identify potential mechanisms to address physical inactivity and overall health, that we believe are strengths to this investigation, were whether or not these women had insurance, and whether or not they had a personal doctor. Interestingly enough, there were no significant relationships between either of these factors. Similar percentages of women in the physically active group and physically inactive group reported having health insurance and also reported having at least one or more personal doctors. Therefore, the mechanism to address physical inactivity in these women may be through PA promotion through their primary care providers with the support of community health workers and public health policies to support these efforts. However, caution must be utilized when interpreting these results. These results are derived from a cross-sectional analysis, and only relationships and associations can be made. Given that these results are correlational in nature only, future research studies should include prospective research designs to determine the prospective nature of this relationship and the potential for causation in this population.
Previous evidence identified racial disparities in PA among women. 16 Of the total sample, 52.7% of the participants were classified as inactive, 16 and the racial-ethnic groups with the largest percentage of physically inactive women were Black (56.5%) and American Indian Alaskan-Native (58.7%). 16 These overall results are similar to the results identified in this current investigation: Black women had a higher prevalence of physical inactivity compared to those of White race. While this investigation did not compare race and ethnicity across other social characteristics, previous research has identified that these differences in race exist across education, family income, occupation, employment, poverty, and marital status. 17
The racial, educational, and income disparity associated with PA in women must be taken into consideration when developing specific health policies or health promotion activities to improve PA in single-female caregivers. It is important that healthcare providers, public health departments and community initiatives develop focused interventions that have targeted women of significant personal and social characteristics identified to be significantly associated with physical inactivity. Previous investigations have identified mechanisms to increase PA for women, some of which have specifically targeted the known barriers associated with single-female caregiver's inactivity.
A scoping review summarized 79 studies that investigated the effectiveness of PA assessment and promotion interventions in the clinical setting. 18 A majority of the clinical trials to improve PA participation were conducted in primary care or family medicine clinics (48%), but also 23% in community clinics and hospitals. 18 These interventions represent promising opportunities for PA promotion as a large majority of the single-female caregiver participants in the 2020 BRFSS indicated they had at least one personal doctor. One study included in the review was a randomized controlled trial that explored the effectiveness of a primary care, phone, and Internet-based intervention to improve diet, PA, and depressive symptoms in overweight women. 19 The intervention included a computerized assessment of overall diet and exercise, which provided the female participants with a personal stage-based action plan. 19 The women then completed an in-person meeting with a healthcare provider to review their personal plan, and were then instructed to log in once a month to complete online educational modules on topics related to PA and nutrition. 19 The women set monthly goals, and trained providers communicated monthly with the women via email and quarterly via telephone. 19 The women randomized into the control group received standard-of-care information from their provider regarding changing PA and eating habits, as well as materials that made exercise and eating habit recommendations. 19 The results indicated that there was a greater decrease in self-reported depression scores in the women who completed the intervention compared to the control group; however, the authors did not report the results for PA or BMI. 19 A summary of previous evidence identified lack of social support, inadequate time, and lack of childcare as barriers for PA, specifically for parents. 20 It is possible that an intervention such as the one described by Kerr et al. 19 may address these barriers associated with physical inactivity and meet the needs of the single-female caregivers as the participants were identified through physicians clinics, the social support was provided through trained individuals by quarterly phone calls, and the online interventions could be done at a time convenient for the participants. 19 However, it must be noted that a large percentage of the women who participated in the Kerr et al. 19 trial were of White race, were college graduates, and were married. Therefore, additional research into the implications of this intervention on single females with children, and specifically those women of lower income and less education, is warranted.
A recent randomized controlled trial explored the effectiveness, feasibility and acceptability of a PA intervention that included group activity delivered via videoconferencing and included multiple mobile apps of the participant’s choice. 21 The participants in the exercise group were assigned to a video exercise group at a time of convenience and were provided an 8-week exercise prescription. 21 The 8-week intervention included participation in five video exercise sessions of the participant’s choice per week, and the participants were asked to meet daily with their social support group for 30 minutes. 21 The results revealed mothers in the PA group increased their mean weekly moderate to vigorous PA by 42.4 minutes, which was more than the mothers in the control group. The mothers who were inactive at baseline saw a significant increase of 50 minutes of moderate to vigorous activity. 21 Additional outcomes included significant weight loss in the intervention arm for those women who were inactive at baseline and also a significant improvement in social support for PA for the women in the intervention group. 21 Finally, the majority of the participants indicated that they were extremely or somewhat satisfied with the intervention, and all women reported feeling a benefit from participating in the intervention. 21 This intervention may be an acceptable intervention for single-female caregivers and appears to benefit most of those mothers who are physically inactive. Healthcare providers and community health practitioners should explore the implementation of this intervention for single-female caregivers who are physically inactive in their local communities.
Limitations
This is a cross-sectional investigation that used a national survey to identify the single-female caregivers for this analysis. There was only a small sample of single-female caregivers who met the inclusion criteria, and no power analysis was performed to justify the sample size. It is possible that these findings are not representative of the entire population of single-female caregivers. The BRFSS did not collect the age of the children, which limits any association between physical inactivity and the age of the children that the females care for. In addition, the BRFSS survey did not identify barriers to PA among these single-female caregivers. It is possible that the barriers described in the previous literature and the health promotion interventions that were described would not be sufficient to meet the needs of the single-female caregivers included in this population. Finally, the variable used to determine if women were physically active or not did not account for types of activity, extent of activity, and did not determine if the women met the recommended levels of activity as recommended for adults in the United States. The variable of interest also excluded activity associated with occupation, which may have miscategorized some women who may have physically demanding.
Conclusion
Black, lower income, less educated, and higher BMI single-female caregivers were more likely to be physically inactive outside of their job responsibilities. Healthcare providers and community partners should be conscius of this dispareity and make efforts to explore PA promotion activities that consider reported barriers with their clients, especially black women. In addition, single-female caregivers who were inactive were more likely to report they had been diagnosed with chronic health conditions compared to active single-female caregivers. Future research should consider the implementation of PA promotion activities that consider the reported barriers identified by single-women with children. More specifically, this research should explore the implementation of these programs with single-female caregivers of non-White race, who have less education, who are of lower income, and who have a higher BMI. Additional support from community health partners should be explored for the implementation of these efforts. Finally, more rigorous prospective research designs should be implemented to determine if there are significant causal relationships among these populations.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241265082 – Supplemental material for Physical inactivity among American single-female caregivers: An analysis of the 2020 behavioral risk factor surveillance system
Supplemental material, sj-docx-1-whe-10.1177_17455057241265082 for Physical inactivity among American single-female caregivers: An analysis of the 2020 behavioral risk factor surveillance system by Johanna M Hoch, Deirdre Dlugonski, Stacey Slone, Rachel Hogg-Graham and Maureen Jones in Women's Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.